
Impact of Bullying—Victimization and Gender over Psychological Distress, Suicidal Ideation, and Family Functioning of Mexican Adolescents


 ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Instruments
2.3. Procedure
2.4. Data Analysis
3. Results
3.1. Correlations
3.2. Cluster Analyses
3.3. MANOVAS
3.3.1. Main effect: victimization
3.3.2. Main effect: gender
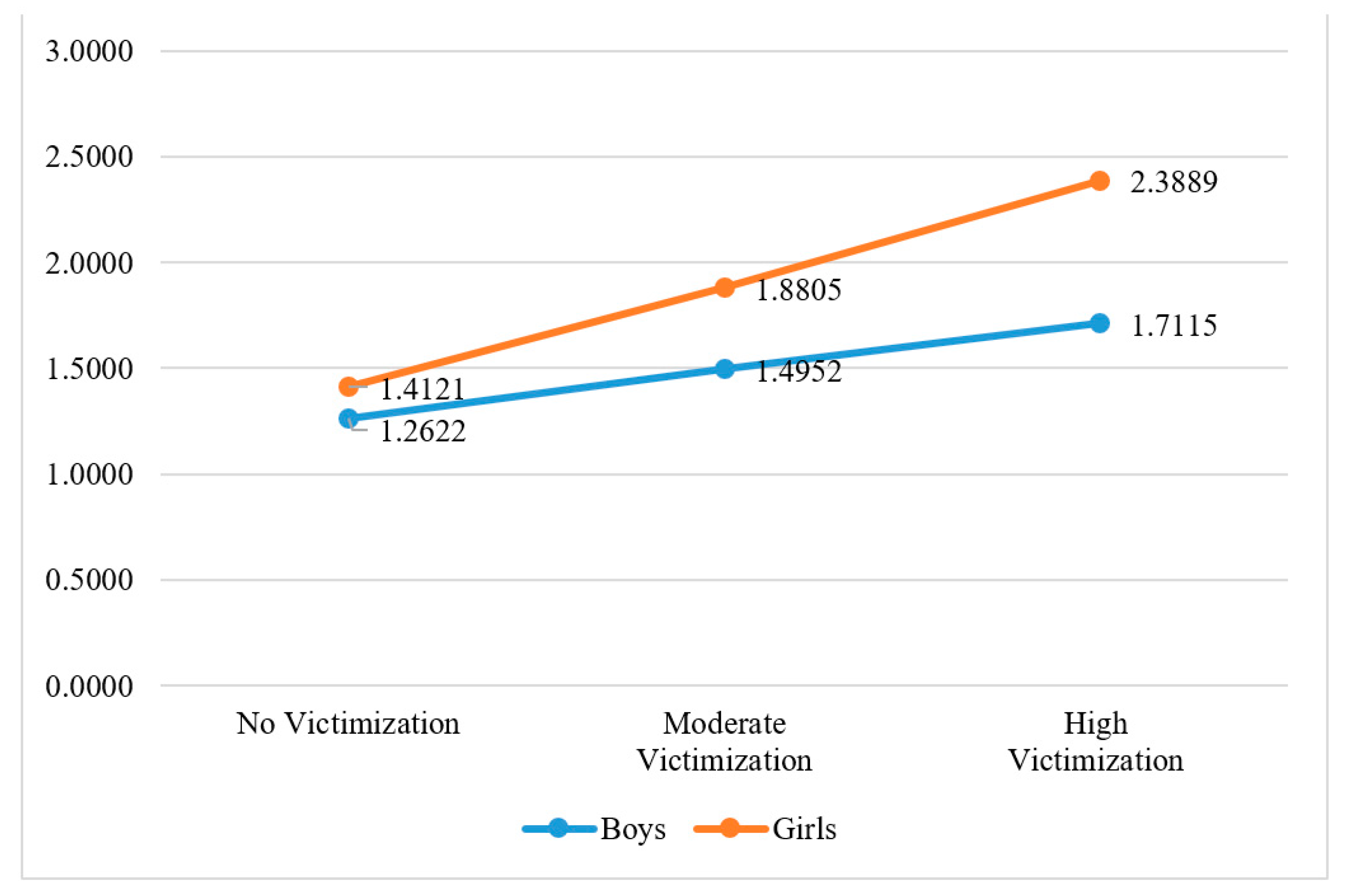
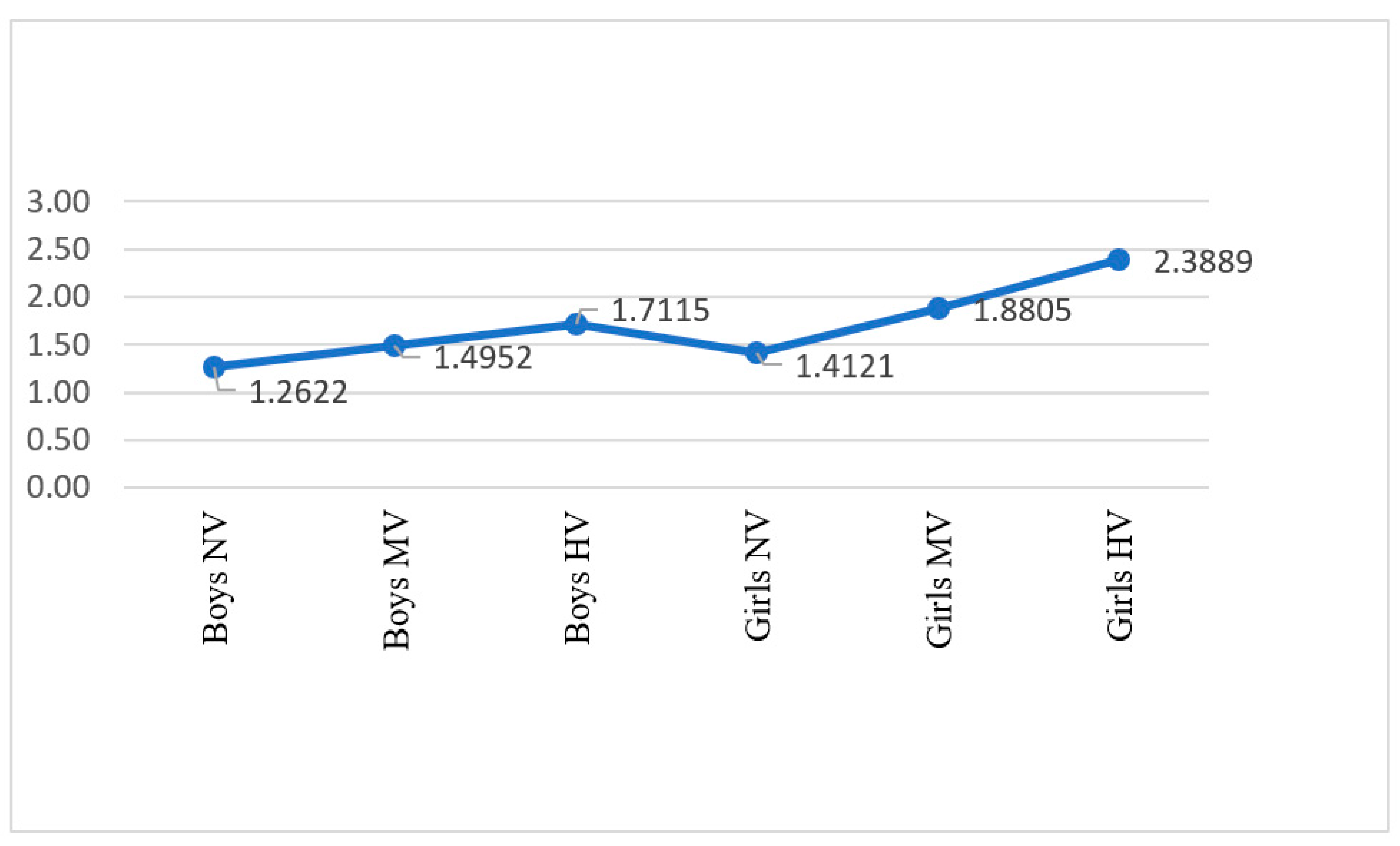
3.3.3. Interaction
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Olweus, D. School Bullying: Development and Some Important Challenges. Annu. Rev. Clin. Psychol. 2013, 9, 751–780. [Google Scholar] [CrossRef] [PubMed]
- Salmivalli, C. Bullying and the Peer Group: A Review. Aggress. Violent Behav. 2010, 15, 112–120. [Google Scholar] [CrossRef]
- Martínez-Ferrer, B.; Moreno Ruiz, D. Dependencia de las Redes Sociales Virtuales Y Violencia Escolar en Adolescentes. Int. J. Dev. Educ. Psychol. Rev. INFAD Psicol. 2017, 2, 105. [Google Scholar] [CrossRef] [Green Version]
- Bronfenbrenner, U.; Ceci, S.J. Nature-Nurture Reconceptualized in Developmental Perspective: A Bioecological Model. Psychol. Rev. 1994, 101, 568–586. [Google Scholar] [CrossRef]
- Campbell, O.L.K.; Bann, D.; Patalay, P. The Gender Gap in Adolescent Mental Health: A Cross-National Investigation of 566,829 Adolescents across 73 Countries. SSM-Popul. Health 2021, 13, 100742. [Google Scholar] [CrossRef]
- Tang, J.J.; Yu, Y.; Wilcox, H.C.; Kang, C.; Wang, K.; Wang, C.; Wu, Y.; Chen, R. Global Risks of Suicidal Behaviours and Being Bullied and Their Association in Adolescents: School-Based Health Survey in 83 Countries. EClinicalMedicine 2020, 19, 100253. [Google Scholar] [CrossRef] [Green Version]
- Smith, P.K.; López-Castro, L.; Robinson, S.; Görzig, A. Consistency of Gender Differences in Bullying in Cross-Cultural Surveys. Aggress. Violent Behav. 2019, 45, 33–40. [Google Scholar] [CrossRef]
- Asad, N.; Karmaliani, R.; McFarlane, J.; Bhamani, S.S.; Somani, Y.; Chirwa, E.; Jewkes, R. The Intersection of Adolescent Depression and Peer Violence: Baseline Results from a Randomized Controlled Trial of 1752 Youth in Pakistan. J. Child Adolesc. Ment. Health 2017, 22, 232–241. [Google Scholar] [CrossRef]
- Ramos-Jiménez, A.; Hernández-Torres, R.P.; Murguía-Romero, M.; Villalobos-Molina, R. Prevalence of Bullying by Gender and Education in a City with High Violence and Migration in Mexico. Rev. Panam. Salud Publica/Pan Am. J. Public Health 2017, 41, e37. [Google Scholar] [CrossRef]
- Wen, Y.; Zhu, X.; Haegele, J.A.; Yu, F. Mental Heath, Bulying, and Victimization among Chinese Adolescents. Children 2022, 9, 240. [Google Scholar] [CrossRef]
- Panjwani, N.; Chaplin, T.M.; Sinha, R.; Mayes, L.C. Gender Differences in Emotion Expression in Low-Income Adolescents Under Stress. J. Nonverbal Behav. 2016, 40, 117–132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barzilay, S.; Brunstein Klomek, A.; Apter, A.; Carli, V.; Wasserman, C.; Hadlaczky, G.; Hoven, C.W.; Sarchiapone, M.; Balazs, J.; Kereszteny, A.; et al. Bullying Victimization and Suicide Ideation and Behavior Among Adolescents in Europe: A 10-Country Study. J. Adolesc. Health 2017, 61, 179–186. [Google Scholar] [CrossRef] [PubMed]
- Cha, C.B.; Franz, P.J.; Guzmán, E.M.; Glenn, C.R.; Kleiman, E.M.; Nock, M.K. Annual Research Review: Suicide among Youth—Epidemiology, (Potential) Etiology, and Treatment. J. Child Psychol. Psychiatry Allied Discip. 2018, 59, 460–482. [Google Scholar] [CrossRef] [Green Version]
- Brunstein Klomek, A.; Barzilay, S.; Apter, A.; Carli, V.; Hoven, C.W.; Sarchiapone, M.; Hadlaczky, G.; Balazs, J.; Kereszteny, A.; Brunner, R.; et al. Bi-Directional Longitudinal Associations between Different Types of Bullying Victimization, Suicide Ideation/Attempts, and Depression among a Large Sample of European Adolescents. Psychiatry J. Child Psychol. 2019, 60, 209–215. [Google Scholar] [CrossRef] [PubMed]
- Arseneault, L. Annual Research Review: The Persistent and Pervasive Impact of Being Bullied in Childhood and Adolescence: Implications for Policy and Practice. J. Child Psychol. Psychiatry Allied Discip. 2018, 59, 405–421. [Google Scholar] [CrossRef] [Green Version]
- Hill, R.M.; Mellick, W.; Temple, J.R.; Sharp, C. The Role of Bullying in Depressive Symptoms from Adolescence to Emerging Adulthood: A Growth Mixture Model. J. Affect. Disord. 2017, 207, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Eastman, M.; Foshee, V.; Ennett, S.; Sotres-Alvarez, D.; Reyes, H.L.M.N.; Faris, R.; North, K. Profiles of Internalizing and Externalizing Symptoms Associated with Bullying Victimization. J. Adolesc. 2018, 65, 101–110. [Google Scholar] [CrossRef]
- Brunstein Klomek, A.; Sourander, A.; Elonheimo, H. Bullying by Peers in Childhood and Effects on Psychopathology, Suicidality, and Criminality in Adulthood. Lancet Psychiatry 2015, 2, 930–941. [Google Scholar] [CrossRef]
- Arvidsdotter, T.; Marklund, B.; Kylen, S.; Taft, C.; Ekman, I. Understanding Persons with Psychological Distress in Primary Health Care. Scand. J. Caring Sci. 2016, 30, 687–694. [Google Scholar] [CrossRef]
- Alonso, J.; Herdman, M.; Pinto, A.; Vilagut, G. Desarrollo de Un Instrumento de Evaluación de Trastornos Depresivos y de Ansiedad Para Encuestas de Salud; Institute Hospital del Mar d’Investigacions Mediques: Barcelona, Spain, 2010. [Google Scholar]
- Kessler, R.C.; Andrews, G.; Colpe, L.J.; Hiripi, E.; Mroczek, D.K.; Normand, S.-L.T.; Walters, E.E.; Zaslavsky, A.M. Short Screening Scales to Monitor Population Prevalences and Trends in Non-Specific Psychological Distress. Psychol. Med. 2002, 32, 959–976. [Google Scholar] [CrossRef]
- World Health Organization. Suicide. Available online: https://www.who.int/news-room/fact-sheets/detail/suicide (accessed on 6 July 2020).
- Instituto Nacional de Estadística y Geografía INEGI Estadísticas a Propósito Del Día Mundial Para La Prevención Del Suicidio (10 de Setiembre). Datos Nacionales. Available online: https://www.inegi.org.mx/contenidos/saladeprensa/aproposito/2019/suicidios2019_Nal.pdf (accessed on 6 July 2020).
- Turecki, G.; Brent, D.; Turecki, G.; Brent, D.A. Suicide and Suicidal Behaviour. Lancet 2016, 387, 1227–1239. [Google Scholar] [CrossRef]
- Barzilay, S.; Apter, A.; Snir, A.; Carli, V.; Hoven, C.W.; Sarchiapone, M.; Hadlaczky, G.; Balazs, J.; Kereszteny, A.; Brunner, R.; et al. A Longitudinal Examination of the Interpersonal Theory of Suicide and Effects of School-Based Suicide Prevention Interventions in a Multinational Study of Adolescents. J. Child Psychol. Psychiatry Allied Discip. 2019, 60, 1104–1111. [Google Scholar] [CrossRef] [PubMed]
- Miranda, R.; Ortin, A.; Scott, M.; Shaffer, D. Characteristics of Suicidal Ideation That Predict the Transition to Future Suicide Attempts in Adolescents. J. Child Psychol. Psychiatry Allied Discip. 2014, 55, 1288–1296. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Suicide Rates. Available online: https://www.who.int/data/gho/data/themes/mental-health/suicide-rates (accessed on 23 March 2022).
- Romo, M.L.; Kelvin, E.A. Impact of Bullying Victimization on Suicide and Negative Health Behaviors among Adolescents in Latin America. Rev. Panam. Salud Publica 2016, 40, 347–355. [Google Scholar]
- Hong, J.S.; Kral, M.J.; Sterzing, P.R. Pathways From Bullying Perpetration, Victimization, and Bully Victimization to Suicidality Among School-Aged Youth: A Review of the Potential Mediators and a Call for Further Investigation. Trauma Violence Abus. 2015, 16, 379–390. [Google Scholar] [CrossRef]
- Chang, E.C.; Wan, L.; Li, P.; Guo, Y.; He, J.; Gu, Y.; Wang, Y.; Li, X.; Zhang, Z.; Sun, Y.; et al. Loneliness and Suicidal Risk in Young Adults: Does Believing in a Changeable Future Help Minimize Suicidal Risk Among the Lonely? J. Psychol. 2017, 151, 453–463. [Google Scholar] [CrossRef]
- Endo, K.; Ando, S.; Shimodera, S.; Yamasaki, S.; Usami, S.; Okazaki, Y.; Sasaki, T.; Richards, M.; Hatch, S.; Nishida, A. Preference for Solitude, Social Isolation, Suicidal Ideation, and Self-Harm in Adolescents. J. Adolesc. Health 2017, 61, 187–191. [Google Scholar] [CrossRef] [Green Version]
- Sánchez-Sosa, J.C.; Villarreal-González, M.E.; Musitu, G.; Martínez Ferrer, B. Ideación Suicida En Adolescentes: Un Análisis Psicosocial. Psychosoc. Interv. 2010, 19, 279–287. [Google Scholar] [CrossRef] [Green Version]
- Musitu, G.; Callejas, J.E. El Modelo De Estrés Familiar En La Adolescencia: Mefad. Int. J. Dev. Educ. Psychol. Rev. INFAD Psicol. 2017, 1, 11. [Google Scholar] [CrossRef] [Green Version]
- Cerezo, F.; Ruiz-Esteban, C.; Lacasa, C.S.; Arense Gonzalo, J.J. Dimensions of Parenting Styles, Social Climate, and Bullying Victims in Primary and Secondary Education. Psicothema 2018, 30, 59–65. [Google Scholar] [CrossRef]
- Bonilla Castillón, C.E.; Nuñez Fadda, S.M.; Domínguez Mora, R.; Callejas Jerónimo, J.E. Conducta Violenta En Adolescentes Escolarizados: Un Modelo Estructural Predictivo. Univ. Psychol. 2017, 16, 1. [Google Scholar] [CrossRef] [Green Version]
- Castro Castañeda, R.; Nuñez Fadda, S.M.; Musitu Ochoa, G.; Callejas Jerónimo, J.E. Comunicación Con Los Padres, Malestar Psicológico y Actitud Hacia La Autoridad En Adolescentes Mexicanos: Su Influencia En La Victimización Escolar. Estud. Sobre Educ. 2019, 36, 113–134. [Google Scholar] [CrossRef]
- Nuñez-Fadda, S.M.; Castro-Castañeda, R.; Vargas-Jiménez, E.; Musitu-Ochoa, G.; Callejas-Jerónimo, J.E. Bullying Victimization among Mexican Adolescents: Psychosocial Differences from an Ecological Approach. Int. J. Environ. Res. Public Health 2020, 17, 4831. [Google Scholar] [CrossRef] [PubMed]
- Oppenheimer, C.W.; Ladouceur, C.D.; Waller, J.M.; Ryan, N.D.; Benoit Allen, K.; Sheeber, L.; Forbes, E.E.; Dahl, R.E.; Silk, J.S. Emotion Socialization in Anxious Youth: Parenting Buffers Emotional Reactivity to Peer Negative Events. J. Abnorm. Child Psychol. 2016, 44, 1267–1278. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Plexousakis, S.S.; Kourkoutas, E.; Giovazolias, T.; Kalliopi, C.; Nikolopoulos, D. School Bullying and Post-Traumatic Stress Disorder Symptoms: The Role of Parental Bonding. Front. Public Health 1 2019, 7, 75. [Google Scholar] [CrossRef] [PubMed]
- Cruz-Manrique, Y.; Herrero Olaizola, J.; Cortés-Ayala, L.; Malvaceda-Espinoza, E. Effect of Violence and SchoolVictimization on Suicidal Ideationin Mexican Adolescents. Int. J. Psychol. Res. 2021, 14, 30–36. [Google Scholar] [CrossRef]
- Crespo-Ramos, S.; Romero-Abrio, A.; Martínez-Ferrer, B.; Musitu, G. Variables Psicosociales y Violencia Escolar En La Adolescencia. Psychosoc. Interv. 2017, 26, 125–130. [Google Scholar] [CrossRef] [Green Version]
- Hong, J.S.; Espelage, D.L.; Grogan-Kaylor, A.; Allen-Meares, P. Identifying Potential Mediators and Moderators of the Association between Child Maltreatment and Bullying Perpetration and Victimization in School. Educ. Psychol. Rev. 2012, 24, 167–186. [Google Scholar] [CrossRef] [Green Version]
- Hadiwijaya, H.; Klimstra, T.A.; Vermunt, J.K.; Branje, S.J.T.; Meeus, W.H.J. On the Development of Harmony, Turbulence, and Independence in Parent–Adolescent Relationships: A Five-Wave Longitudinal Study. J. Youth Adolesc. 2017, 46, 1772–1788. [Google Scholar] [CrossRef] [Green Version]
- Luijten, C.C.; van de Bongardt, D.; Jongerling, J.; Nieboer, A.P. Associations between Adolescents’ Internalizing Problems and Well-Being: Is There a Buffering Role of Boys’ and Girls’ Relationships with Their Mothers and Fathers? BMC Public Health 2021, 21, 1871. [Google Scholar] [CrossRef]
- Fuentes-Balderrama, J.; del Castillo, C.C.; Parra-Cardona, J.R.; Plaza, B.T.; García, A.O.; Díaz-Loving, R. Parental Practices and Maternal Warmth as Protective Factors for Problem Behaviors in Mexican Preadolescents. J. Sociol. Soc. Welf. 2020, 47, 59–81. [Google Scholar]
- Santos Peñas, J.; Muñoz Alamillos, Á.; Juez Martel, P.; Cortiñas Vázquez, P. Diseño de Encuestas de Estudio de Mercado. Técnicas de Muestreo y Análisis Multivariante; Fundación Ramón Areces: Madrid, Spain, 2003. [Google Scholar]
- Buelga, S.; Cava, M.J.; Musitu, G. Reputacion Social, Ajuste Psicosocial y Victimizacion Entre Adolescentes En El Contexto Escolar. An. Psicol. 2012, 28, 180–187. [Google Scholar]
- Mariño, M.C.; Medina, M.E.; Chaparro, J.J.; González-Forteza, C. Confiabilidad y Estructura Factorial del CES-D En Adolescentes Mexicanos. Rev. Mex. Psicol. 1993, 10, 141–145. [Google Scholar]
- Smilkstein, G. The Family APGAR: A Proposal for a Family Function Test and Its Use by Physician. J. Fam. Pract. 1978, 6, 1231–1239. [Google Scholar] [PubMed]
- Bellón Saameño, J.A.; Delgado Sánchez, A.; Luna del Castillo, J.d.D.; Lardelli Claret, P. Validez y Fiabilidad del Cuestionario de Función Familiar Apgar-Familiar. Aten Primaria 1996, 18, 289–296. [Google Scholar]
- World Medical Association Declaration of Helsinki. Ethical Principles for Medical Research Involving Human Subjects. J. Am. Med. Assoc. 2013, 310, 2191–2194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Useche Castro, L.M.; Mesa Ávila, D.M. Una Introducción a La Imputación de Valores Perdidos. Terra Nueva Etapa 2006, XXII, 127–151. [Google Scholar] [CrossRef]
- Hair, J.F., Jr.; Black, W.C.; Babin, B.J.; Anderson, R.E.; Tatham, R.L. Multivariate Data Analysis; Dorling Kindersley, Pvt. Ltd.: New Delhi, India, 2008. [Google Scholar]
- Zimmer-Gembeck, M.J. Peer Rejection, Victimization, and Relational Self-System Processes in Adolescence: Toward a Transactional Model of Stress, Coping, and Developing Sensitivities. Child Dev. Perspect. 2016, 10, 122–127. [Google Scholar] [CrossRef]
- Cheek, S.M.; Reiter-Lavery, T.; Goldston, D.B. Social Rejection, Popularity, Peer Victimization, and Self-Injurious Thoughts and Behaviors among Adolescents: A Systematic Review and Meta-Analysis. Clin. Psychol. Rev. 2020, 82, 101936. [Google Scholar] [CrossRef]
- Sullivan, L.; Camic, P.M.; Brown, J.S. Masculinity, Alexithymia, and Fear of Intimacy as Predictors of UK Men’s Attitudes towards Seeking Professional Psychological Help. Br. J. Health Psychol. 2015, 20, 194–211. [Google Scholar] [CrossRef]
- River, J. Diverse and Dynamic Interactions: A Model of Suicidal Men’s Help Seeking as It Relates to Health Services. Am. J. Mens. Health 2018, 12, 150–159. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lynch, L.; Long, M.; Moorhead, A. Young Men, Help-Seeking, and Mental Health Services: Exploring Barriers and Solutions. Am. J. Mens. Health 2018, 12, 138–149. [Google Scholar] [CrossRef] [PubMed]
- Shamah-Levy, T.; Vielma-Orozco, E.; Heredia-Hernández, O.; Romero-Martínez, M.; Mojica-Cuevas, J.; Cuevas-Nasu, L.; Santaella-Castell, J.A.; Rivera-Dommarco, J. Encuesta Nacional de Salud y Nutrición 2018–19: Resultados Nacionales; Instituto Nacional de Salud Pública: Cuernavaca, Mexico, 2020. [Google Scholar]
- Instituto Nacional de Estadística y Geografía. Estadísticas a Propósito Del … Día De La Familia Mexicana (5 De Marzo); INEGI: Aguascalientes, Mexico, 2017. [Google Scholar]
- Garcia, R.; Tomlinson, J. Rethinking the Domestic Division of Labour: Exploring Change and Continuity in the Context of Redundancy. Sociology 2021, 55, 300–318. [Google Scholar] [CrossRef]
- Luna Bernaly, A.C.; Cruz Abundis, C. Frecuencia e Intensidad de Conflictos Con Los Padres En Adolescentes Bachilleres. Altern. Psicol. 2014, 30, 8–21. [Google Scholar]
- Lugo-Candelas, C.; Harvey, E.A.; Breaux, R.P. Emotion Socialization Practices in Latina and European American Mothers of Preschoolers with Behavior Problems. J. Fam. Stud. 2015, 21, 144–162. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ybarra, M.L.; Espelage, D.L.; Mitchell, K.J. Differentiating Youth Who Are Bullied from Other Victims of Peer-Aggression: The Importance of Differential Power and Repetition. J. Adolesc. Health 2014, 55, 293–300. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mascayano, F.; Irrazabal, M.; Emilia, W.D.; Shah, B.; Vaner, S.J.; Sapag, J.C.; Alvarado, R.; Yang, L.H. Suicide in Latin America: A Growing Public Health Issue. Rev. Fac. Cienc. Med. 2015, 73, 295–303. [Google Scholar]



{kind=link}
{kind=link}
| 1 | 2 | 3 | 4 | 5 | 6 | |
|---|---|---|---|---|---|---|
| 1. Relational Victimization | 1 | |||||
| 2. Direct Physical Victimization | 0.709 ** | 1 | ||||
| 3. Direct Verbal Victimization | 0.838 ** | 0.720 ** | 1 | |||
| 4. Psychological Distress | 0.377 ** | 0.244 ** | 0.365 ** | 1 | ||
| 5. Suicidal Ideation | 0.316 ** | 0.236 ** | 0.315 ** | 0.534 ** | 1 | |
| 6. Family Functioning | −0.186 ** | −0.168 ** | −0.184 ** | −0.396 ** | −0.389 ** | 1 |
| Means | 1.66 | 1.46 | 1.73 | 2.29 | 1.47 | 3.61 |
| Standard Deviation | 0.78 | 0.63 | 0.78 | 0.84 | 0.71 | 1.09 |
| Gender | HV (N y%) | MV (N y%) | NV (N y%) | Totals by Gender |
|---|---|---|---|---|
| Boys | 52 (3.1%) | 208 (12.4%) | 514 (30.63%) | 774 (45.88%) |
| Girls | 45 (2.68%) | 196 (11.68%) | 663 (39.51%) | 904 (53.58%) |
| Total | 97 (5.78%) | 404 (24.07%) | 1177 (69.76%) | 1678 (100%) |
| Variation Source | Variables | |||||
|---|---|---|---|---|---|---|
| Λ A | F | dfentre | dferror | p | η2 | |
| (A) Victimization a1,a2,a3 | 0.858 | 44.453 | 6 | 3340 | <0.001 *** | 0.074 |
| (B) Gender b1,b2 | 0.952 | 27.796 | 6 | 1670 | <0.001 *** | 0.059 |
| A × B | 0.987 | 3.760 | 6 | 3340 | <0.001 *** | 0.007 |
| Source of Variation | Bullying Victimization | ||||
|---|---|---|---|---|---|
| NV | MV | HV | F | η2 | |
| Psychological Distress | 2.12 (0.77) | 2.62 (0.85) | 3.00 (0.89) | 97.872 *** | 0.104 |
| Suicidal Ideation | 1.35 (0.61) | 1.68 (0.79) | 2.02 (0.96) | 70.125 *** | 0.077 |
| Family Functioning | 3.73 (1.05) | 3.40 (1.10) | 3.13 (1.29) | 24.179 *** | 0.028 |
| Source of Variation | Gender | |||
|---|---|---|---|---|
| Boys | Girls | F | η2 | |
| Psychological Distress | 2.10 (0.76) | 2.46 (0.88) | 76.250 *** | 0.043 |
| Suicidal Ideation | 1.36 (0.58) | 1.56 (0.78) | 37.271 *** | 0.813 |
| Family Functioning | 3.78 (0.99) | 3.47 (1.15) | 35.876 *** | 0.021 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nuñez-Fadda, S.M.; Castro-Castañeda, R.; Vargas-Jiménez, E.; Musitu-Ochoa, G.; Callejas-Jerónimo, J.E. Impact of Bullying—Victimization and Gender over Psychological Distress, Suicidal Ideation, and Family Functioning of Mexican Adolescents. Children 2022, 9, 747. https://0-doi-org.brum.beds.ac.uk/10.3390/children9050747
Nuñez-Fadda SM, Castro-Castañeda R, Vargas-Jiménez E, Musitu-Ochoa G, Callejas-Jerónimo JE. Impact of Bullying—Victimization and Gender over Psychological Distress, Suicidal Ideation, and Family Functioning of Mexican Adolescents. Children. 2022; 9(5):747. https://0-doi-org.brum.beds.ac.uk/10.3390/children9050747
Chicago/Turabian StyleNuñez-Fadda, Silvana Mabel, Remberto Castro-Castañeda, Esperanza Vargas-Jiménez, Gonzalo Musitu-Ochoa, and Juan Evaristo Callejas-Jerónimo. 2022. "Impact of Bullying—Victimization and Gender over Psychological Distress, Suicidal Ideation, and Family Functioning of Mexican Adolescents" Children 9, no. 5: 747. https://0-doi-org.brum.beds.ac.uk/10.3390/children9050747