
Family Dysfunctional Interactive Patterns and Alexithymia in Adolescent Patients with Restrictive Eating Disorders


 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
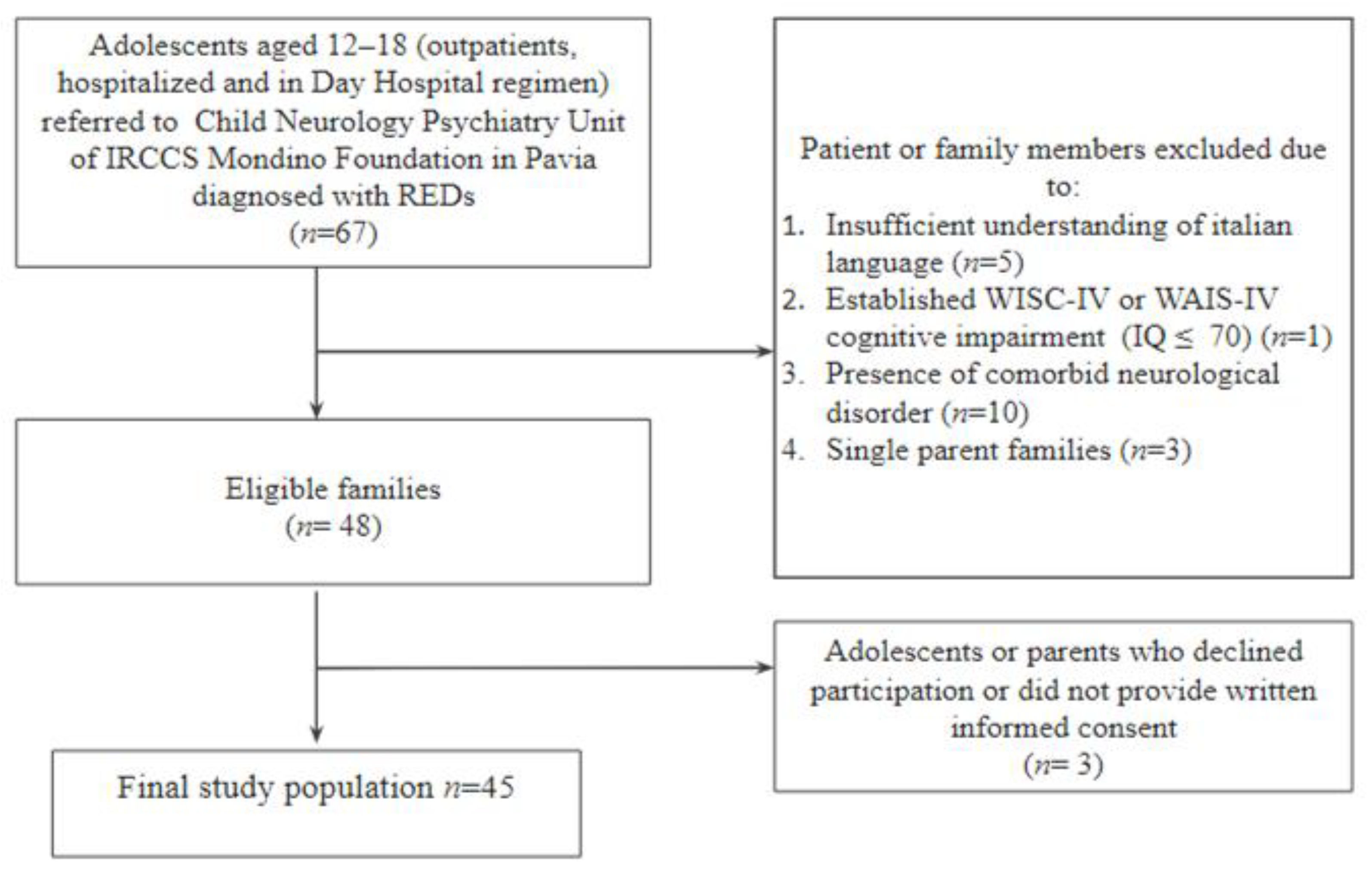
2.1. Participants
2.2. Procedures
2.3. Measures
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hay, P.; Mitchison, D.; Collado, A.E.L.; González-Chica, D.A.; Stocks, N.; Touyz, S. Burden and Health-Related Quality of Life of Eating Disorders, Including Avoidant/Restrictive Food Intake Disorder (ARFID), in the Australian Population. J. Eat. Disord. 2017, 5, 21. [Google Scholar] [CrossRef] [PubMed]
- Mensi, M.M.; Orlandi, M.; Rogantini, C.; Provenzi, L.; Chiappedi, M.; Criscuolo, M.; Castiglioni, M.C.; Zanna, V.; Borgatti, R. Assessing Family Functioning Before and After an Integrated Multidisciplinary Family Treatment for Adolescents With Restrictive Eating Disorders. Front. Psychiatry 2021, 12, 653047. [Google Scholar] [CrossRef] [PubMed]
- Dell’Osso, L.; Abelli, M.; Carpita, B.; Pini, S.; Castellini, G.; Carmassi, C.; Ricca, V. Historical Evolution of the Concept of Anorexia Nervosa and Relationships with Orthorexia Nervosa, Autism, and Obsessive-Compulsive Spectrum. Neuropsychiatr. Dis. Treat. 2016, 12, 1651–1660. [Google Scholar]
- Gutiérrez, T.; Espinoza, P.; Penelo, E.; Mora, M.; González, M.L.; Rosés, R.; Raich, R.M. Association of Biological, Psychological and Lifestyle Risk Factors for Eating Disturbances in Adolescents. J. Health Psychol. 2015, 20, 839–849. [Google Scholar] [CrossRef]
- Lock, J.; La Via, M.C. Practice Parameter for the Assessment and Treatment of Children and Adolescents with Eating Disorders. J. Am. Acad. Child Adolesc. Psychiatry 2015, 54, 412–425. [Google Scholar] [CrossRef]
- National Collaborating Centre for Mental Health (UK). Eating Disorders: Core Interventions in the Treatment and Management of Anorexia Nervosa, Bulimia Nervosa and Related Eating Disorders; British Psychological Society: Leicester, UK, 2004. [Google Scholar]
- Rikani, A.A.; Choudhry, Z.; Choudhry, A.M.; Ikram, H.; Asghar, M.W.; Kajal, D.; Waheed, A.; Mobassarah, N.J. A Critique of the Literature on Etiology of Eating Disorders. Ann. Neurosci. 2013, 20, 157–161. [Google Scholar] [CrossRef] [Green Version]
- Hatch, A.; Madden, S.; Kohn, M.; Clarke, S.; Touyz, S.; Williams, L.M. Anorexia Nervosa: Towards an Integrative Neuroscience Model. Eur. Eat. Disord. Rev. 2010, 18, 165–179. [Google Scholar] [CrossRef]
- Oldershaw, A.; Treasure, J.; Hambrook, D.; Tchanturia, K.; Schmidt, U. Is Anorexia Nervosa a Version of Autism Spectrum Disorders? Eur. Eat. Disord. Rev. 2011, 19, 462–474. [Google Scholar] [CrossRef]
- Westwood, H.; Tchanturia, K. Autism Spectrum Disorder in Anorexia Nervosa: An Updated Literature Review. Curr. Psychiatry Rep. 2017, 19, 41. [Google Scholar] [CrossRef] [Green Version]
- Gaggero, G.; Bonassi, A.; Dellantonio, S.; Pastore, L.; Aryadoust, V.; Esposito, G. A Scientometric Review of Alexithymia: Mapping Thematic and Disciplinary Shifts in Half a Century of Research. Front. Psychiatry 2020, 11, 611489. [Google Scholar] [CrossRef]
- Nowakowski, M.E.; McFarlane, T.; Cassin, S. Alexithymia and Eating Disorders: A Critical Review of the Literature. J. Eat. Disord. 2013, 1, 21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taylor, G.J.; Bagby, R.M.; Parker, J.D.A.; Grotstein, J. Disorders of Affect Regulation; Cambridge University Press: Cambridge, UK, 1997. [Google Scholar]
- Taylor, G.J.; Michael Bagby, R. New Trends in Alexithymia Research. Psychother. Psychosom. 2004, 73, 68–77. [Google Scholar] [CrossRef] [PubMed]
- Treasure, J.; Schmidt, U. The Cognitive-Interpersonal Maintenance Model of Anorexia Nervosa Revisited: A Summary of the Evidence for Cognitive, Socio-Emotional and Interpersonal Predisposing and Perpetuating Factors. J. Eat. Disord. 2013, 1, 13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pinna, F.; Sanna, L.; Carpiniello, B. Alexithymia in Eating Disorders: Therapeutic Implications. Psychol. Res. Behav. Manag. 2015, 8, 1–15. [Google Scholar] [CrossRef] [Green Version]
- Anastasiadou, D.; Medina-Pradas, C.; Sepulveda, A.R.; Treasure, J. A Systematic Review of Family Caregiving in Eating Disorders. Eat. Behav. 2014, 15, 464–477. [Google Scholar] [CrossRef] [PubMed]
- Lyke, J.; Matsen, J. Family Functioning and Risk Factors for Disordered Eating. Eat. Behav. 2013, 14, 497–499. [Google Scholar] [CrossRef] [PubMed]
- Hibbs, R.; Rhind, C.; Leppanen, J.; Treasure, J. Interventions for Caregivers of Someone with an Eating Disorder: A Meta-Analysis. Int. J. Eat. Disord. 2015, 48, 349–361. [Google Scholar] [CrossRef]
- Malagoli Togliatti, M.; Mazzoni, S. Osservare, Valutare, e Sostenere La Relazione Genitori-Figli. Il Lausanne Trilogue Play Clinico [Observe, Evaluate, and Support the Parent-Child Relationship. The Clinical Lausanne Trilogue Play]; Raffaello Cortina Editore: Milano, Italy, 2006. [Google Scholar]
- Balottin, L.; Mannarini, S.; Mensi, M.M.; Chiappedi, M.; Gatta, M. Triadic Interactions in Families of Adolescents with Anorexia Nervosa and Families of Adolescents with Internalizing Disorders. Front. Psychol. 2017, 7, 2046. [Google Scholar] [CrossRef] [Green Version]
- Mensi, M.M.; Balottin, L.; Rogantini, C.; Orlandi, M.; Galvani, M.; Figini, S.; Chiappedi, M.; Balottin, U. Focus on Family Functioning in Anorexia Nervosa: New Perspectives Using the Lausanne Trilogue Play. Psychiatry Res. 2020, 288, 112968. [Google Scholar] [CrossRef]
- Balottin, L.; Mannarini, S.; Mensi, M.M.; Chiappedi, M.; Balottin, U. Are Family Relations Connected to the Quality of the Outcome in Adolescent Anorexia Nervosa? An Observational Study with the Lausanne Trilogue Play. Clin. Psychol. Psychother. 2018, 25, 785–796. [Google Scholar] [CrossRef]
- Criscuolo, M.; Laghi, F.; Mazzoni, S.; Castiglioni, M.C.; Vicari, S.; Zanna, V. How Do Families of Adolescents with Anorexia Nervosa Coordinate Parenting? J. Child Fam. Stud. 2020, 29, 2542–2551. [Google Scholar] [CrossRef]
- Fivaz-Depeursinge, E.; Corboz-Warnery, A. The Primary Triangle: A Developmental Systems View of Mothers, Fathers and Infants; Basic Books: New York, NY, USA, 1999. [Google Scholar]
- Mannarini, S.; Balottin, L.; Palmieri, A.; Carotenuto, F. Emotion Regulation and Parental Bonding in Families of Adolescents with Internalizing and Externalizing Symptoms. Front. Psychol. 2018, 9, 1493. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mannarini, S.; Kleinbub, J.R. Parental-Bonding and Alexithymia in Adolescents with Anorexia Nervosa, Their Parents, and Siblings. Behav. Sci. 2022, 12, 123. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar]
- Kaufman, J.; Birmaher, B.; Rao, U.; Ryan, N. K-SADS-PL DSM-5. Intervista Diagnostica per La Valutazione Dei Disturbi Psicopatologici in Bambini e Adolescenti. [Schedule for Affective Disorders and Schizophrenia for School-Aged Children: Present and Lifetime Version (K-SADS-PL) DSM-5]; di Sogos, C., Di Noia, S.P., Fioriello, F., Picchiotti, G., Eds.; Erickson: Trento, Italy, 2019. [Google Scholar]
- First, M.B.; Williams, J.B.W.; Janet, S.B.; Spitzer, R.L. Structured Clinical Interview for DSM-5. Personality Disorders (SCID-5-PD); American Psychiatric Association: Washington, DC, USA, 2017. [Google Scholar]
- Wechsler, D. Wechsler Adult Intelligence Scale (WAIS-IV), 4th ed.; Giunti Organizzazioni Speciali: Firenze, Italy, 2008. [Google Scholar]
- Wechsler, D. Wechsler Intelligence Scale for Children (WISC-IV), 4th ed.; Giunti Organizzazioni Speciali: Firenze, Italy, 2003. [Google Scholar]
- Bagby, R.M.; Parker, J.D.A.; Taylor, G.J. The Twenty-Item Toronto Alexithymia Scale-I. Item Selection and Cross-Validation of the Factor Structure. J. Psychosom. Res. 1994, 38, 23–32. [Google Scholar] [CrossRef]
- Bressi, C.; Taylor, G.; Parker, J.; Bressi, S.; Brambilla, V.; Aguglia, E.; Allegranti, I.; Bongiorno, A.; Giberti, F.; Bucca, M.; et al. Cross Validation of the Factor Structure of the 20-Item Toronto Alexithymia Scale: An Italian Multicenter Study. J. Psychosom. Res. 1996, 41, 551–559. [Google Scholar] [CrossRef]
- La Barbera, D.; Caretti, V.; Craparo, G. La Toronto Alexithymia Scale (TAS-20). In Alessitimia. Valutazione e Trattamento; Astrolabio Ubaldini: Roma, Italy, 2005; pp. 17–23. [Google Scholar]
- Taylor, G.J.; Bagby, R.M.; Parker, J.D.A. The 20-Item Toronto Alexithymia Scale: IV. Reliability and Factorial Validity in Different Languages and Cultures. J. Psychosom. Res. 2003, 55, 277–283. [Google Scholar] [CrossRef]
- Espina Eizaguirre, A.; Ortego Saenz de Cabezón, A.; Ochoa de Alda, I.; Joaristi Olariaga, L.; Juaniz, M. Alexithymia and Its Relationships with Anxiety and Depression in Eating Disorders. Pers. Individ. Dif. 2004, 36, 321–331. [Google Scholar] [CrossRef]
- Gramaglia, C.; Ressico, F.; Gambaro, E.; Palazzolo, A.; Mazzarino, M.; Bert, F.; Siliquini, R.; Zeppegno, P. Alexithymia, Empathy, Emotion Identification and Social Inference in Anorexia Nervosa: A Case-Control Study. Eat. Behav. 2016, 22, 46–50. [Google Scholar] [CrossRef]
- Montebarocci, O.; Codispoti, M.; Surcinelli, P.; Franzoni, E.; Baldaro, B.; Rossi, N. Alexithymia in Female Patients with Eating Disorders. Eat. Weight Disord. 2006, 11, 14–21. [Google Scholar] [CrossRef]
- Torres, S.; Guerra, M.P.; Lencastre, L.; Roma-Torres, A.; Brandão, I.; Queirós, C.; Vieira, F. Cognitive Processing of Emotions in Anorexia Nervosa. Eur. Eat. Disord. Rev. 2011, 19, 100–111. [Google Scholar] [CrossRef]
- Rogantini, C.; Provenzi, L.; Mensi, M.M. Prioritizing Family-Centered Mental Health Care for Pediatric Patients with Eating Disorders. JAMA Pediatr. 2020, 175, 324. [Google Scholar] [CrossRef] [PubMed]
- Erriu, M.; Cimino, S.; Cerniglia, L. The Role of Family Relationships in Eating Disorders in Adolescents: A Narrative Review. Behav. Sci. 2020, 10, 71. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Collusive Alliance | |||||||
|---|---|---|---|---|---|---|---|
| All (N = 45) | Yes (N = 18) | No (N = 27) | |||||
| N | % | N | % | N | % | ||
| Sex | Males | 9 | 20.0 | 3 | 16.7 | 6 | 22.2 |
| Females | 36 | 80.0 | 15 | 83.3 | 21 | 77.8 | |
| Socially withdrawn | No | 40 | 88.9 | 16 | 88.9 | 24 | 88.9 |
| Yes | 5 | 11.9 | 2 | 11.9 | 3 | 11.9 | |
| Academic retreat | No | 37 | 82.2 | 12 | 66.7 | 25 | 92.6 |
| Yes | 8 | 17.8 | 6 | 33.3 | 2 | 7.4 | |
| Self-harm behaviors | No | 36 | 80.0 | 13 | 72.2 | 23 | 85.2 |
| Yes | 9 | 20.0 | 5 | 27.8 | 4 | 14.8 | |
| Comorbid affective symptoms | No | 24 | 53.3 | 8 | 44.4 | 16 | 59.3 |
| Yes | 21 | 46.7 | 10 | 55.6 | 11 | 40.7 | |
| Mean | SD | Mean | SD | Mean | SD | ||
| Demographic characteristics | Patients’ age (years) | 14.91 | 1.59 | 14.78 | 1.63 | 15.11 | 1.57 |
| Patients’ weight (kg) | 40.20 | 7.35 | 39.53 | 7.37 | 31.22 | 7.40 | |
| Patients’ BMI (kg/m2) | 15.88 | 2.50 | 16.52 | 2.33 | 15.45 | 2.57 | |
| Fathers’ age (years) | 51.00 | 5.53 | 51.91 | 5.78 | 49.76 | 5.08 | |
| Mothers’ age (years) | 48.25 | 5.41 | 48.43 | 5.69 | 48.00 | 5.16 | |
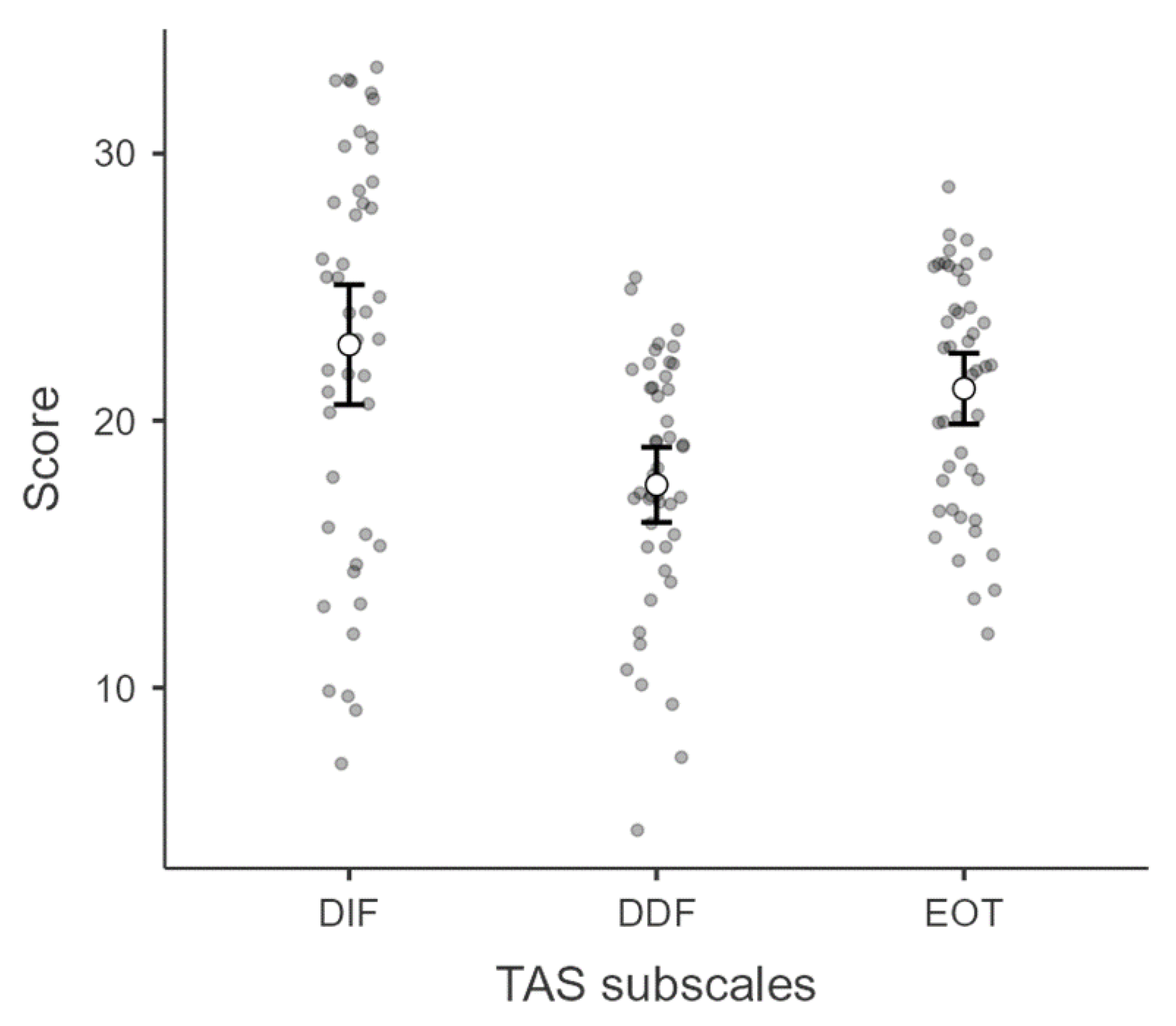
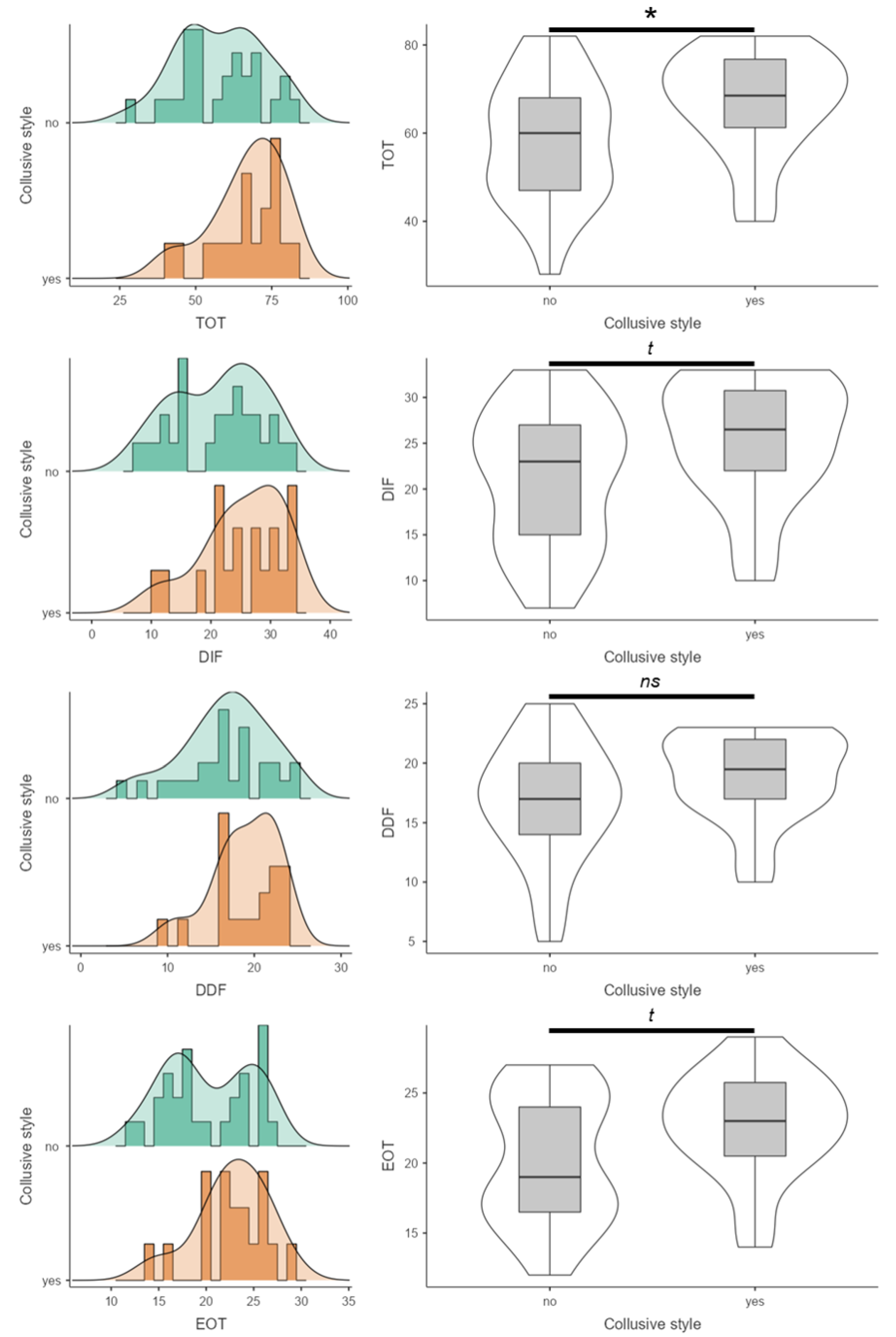
| TAS scores | DIF | 22.84 | 7.47 | 25.33 | 6.82 | 21.19 | 7.54 |
| DDF | 17.60 | 4.68 | 18.89 | 3.76 | 16.74 | 5.08 | |
| EOT | 21.20 | 4.41 | 22.72 | 3.79 | 20.19 | 4.57 | |
| TOT | 61.64 | 13.74 | 66.94 | 11.91 | 58.11 | 13.94 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Coci, C.; Provenzi, L.; De Giorgis, V.; Borgatti, R.; Chiappedi, M.; Mensi, M.M.; on behalf of the Mondino Foundation Eating Disorders Clinical and Research Group. Family Dysfunctional Interactive Patterns and Alexithymia in Adolescent Patients with Restrictive Eating Disorders. Children 2022, 9, 1038. https://0-doi-org.brum.beds.ac.uk/10.3390/children9071038
Coci C, Provenzi L, De Giorgis V, Borgatti R, Chiappedi M, Mensi MM, on behalf of the Mondino Foundation Eating Disorders Clinical and Research Group. Family Dysfunctional Interactive Patterns and Alexithymia in Adolescent Patients with Restrictive Eating Disorders. Children. 2022; 9(7):1038. https://0-doi-org.brum.beds.ac.uk/10.3390/children9071038
Chicago/Turabian StyleCoci, Chiara, Livio Provenzi, Valentina De Giorgis, Renato Borgatti, Matteo Chiappedi, Martina Maria Mensi, and on behalf of the Mondino Foundation Eating Disorders Clinical and Research Group. 2022. "Family Dysfunctional Interactive Patterns and Alexithymia in Adolescent Patients with Restrictive Eating Disorders" Children 9, no. 7: 1038. https://0-doi-org.brum.beds.ac.uk/10.3390/children9071038