
Relationship between Physiological Resorption of Primary Molars with Its Permanent Successors, Dental Age and Chronological Age

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
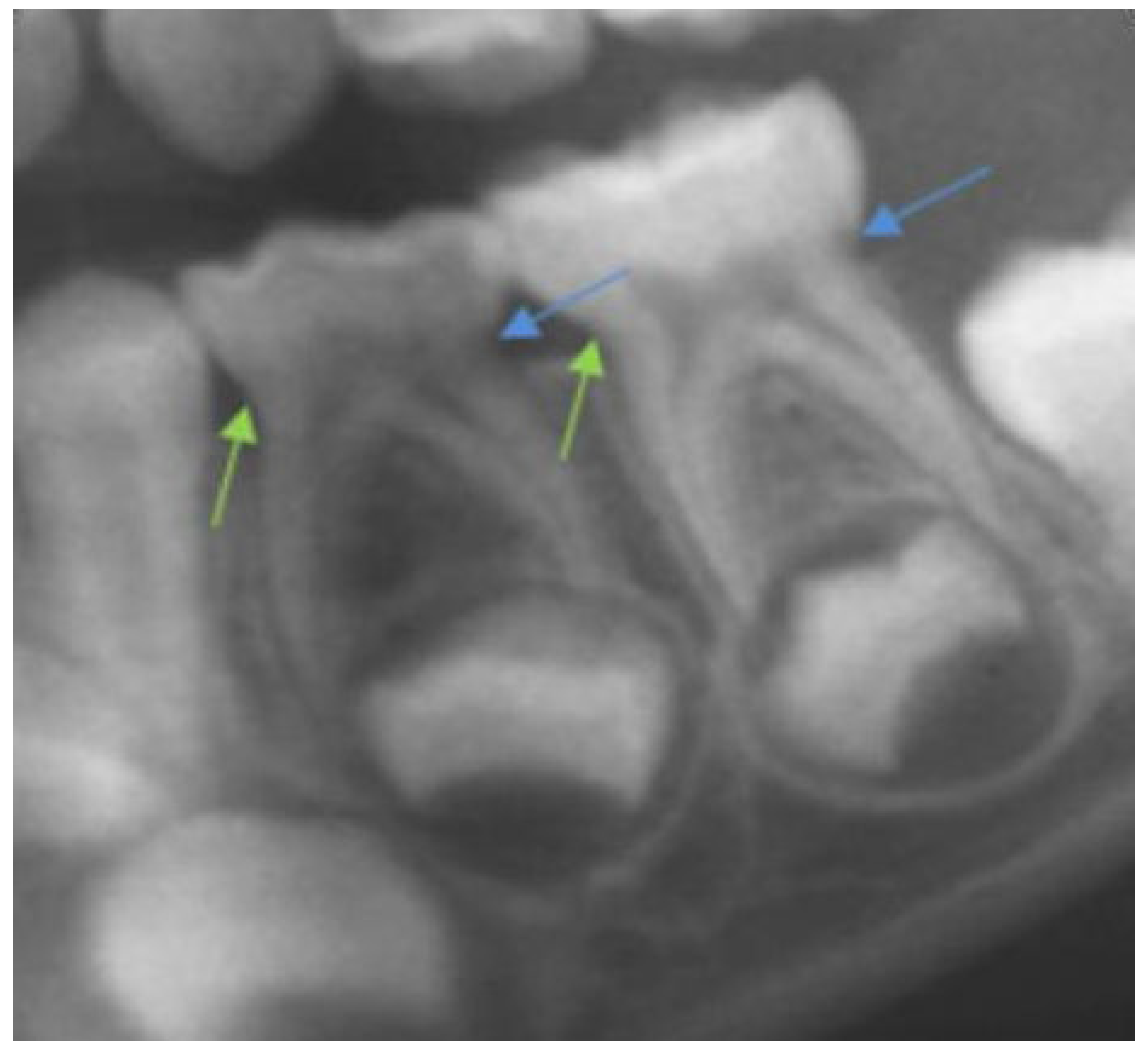
- Crown height was calculated as the distance between the line that links the mesial and distal cemento-enamel junctions and the highest point of the occlusal surface of the molar (Figure 1).
- Mesial root length was calculated as the distance between the mesial cemento-enamel junction and the most apical point of the mesial root.
- Distal radicular length was calculated in the same way as mesial root length, but in the distal molar area (Figure 1).
- Mesial and distal crown-to-root ratios (CRR-m and CRR-d, respectively) were calculated by dividing the length of each root by its coronal height.
3. Results
- -
- The developmental stage of #34 was greater in girls than in boys of 5 years old (p < 0.05)
- -
- The length of the mesial and distal roots, and the CRR-m and CRR-d of #74, was greater in boys of 7 years old than in girls (p < 0.05)
- -
- The length of the distal root of #75 was greater in boys of 8 years old than in girls (p = 0.02)
- -
- The length of the mesial root and the CRR- m of #74 was greater in 9-year-old boys than in girls (p < 0.05)
- -
- The developmental stage of #34 was greater in boys than in 9-year-old girls (p = 0.006)
- -
- The distal root length of #75 was greater in 10-year-old boys than in girls (p = 0.02).
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
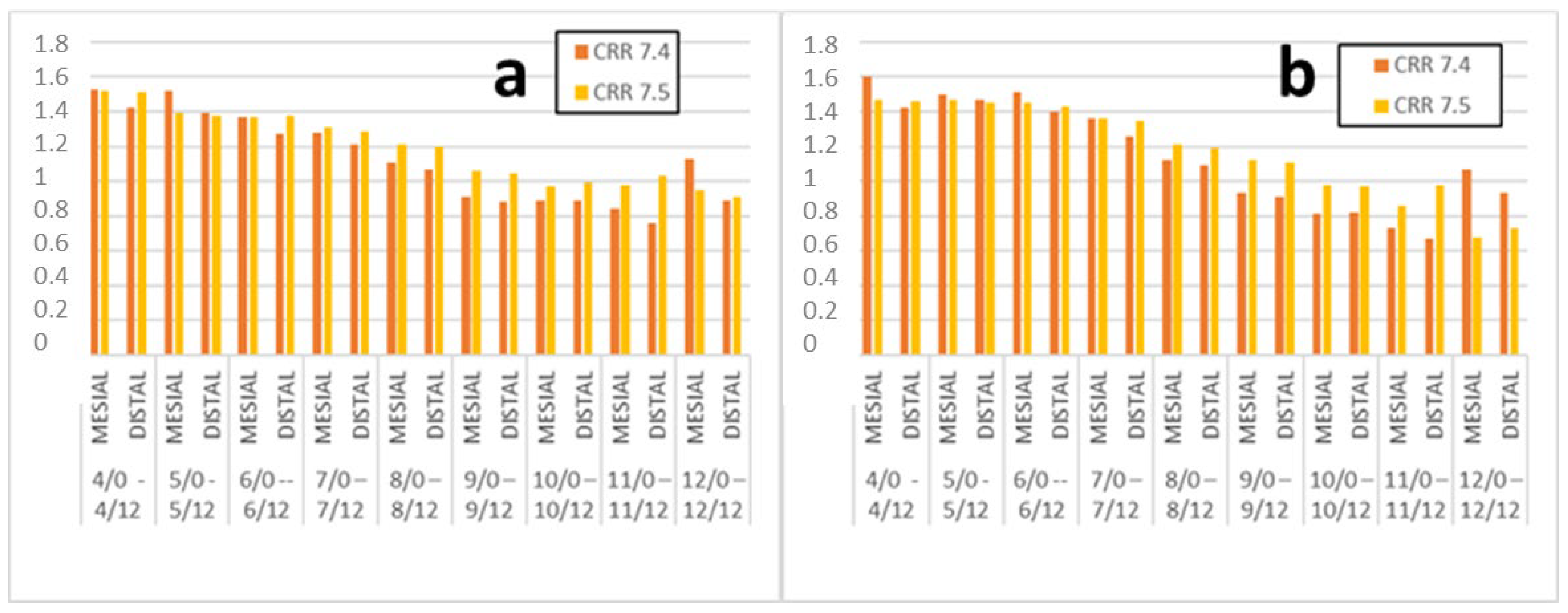
| Chronological Age Range | Root | n | CRR #74 ± S.D. + | n | CRR #75 ± S.D. |
|---|---|---|---|---|---|
| 4/0–4/12 | Mesial | 23 | 1.53 ± 0.15 | 23 | 1.52 ± 0.16 |
| Distal | 1.42 ± 0.21 | 1.51 ± 0.18 | |||
| 5/0–5/12 | Mesial | 20 | 1.52 ± 0.31 | 24 | 1.39 ± 0.17 |
| Distal | 1.39 ± 0.25 | 1.38 ± 0.17 | |||
| 6/0–6/12 | Mesial | 45 | 1.37 ± 0.23 | 52 | 1.37 ± 0.16 |
| Distal | 1.27 ± 0.213 | 1.38 ± 0.17 | |||
| 7/0–7/12 | Mesial | 81 | 1.28 ± 0.29 | 95 | 1.31 ± 0.22 |
| Distal | 1.21 ± 0.25 | 1.29 ± 0.20 | |||
| 8/0–8/12 | Mesial | 65 | 1.11 ± 0.27 | 81 | 1.21 ± 0.22 |
| Distal | 1.07 ± 0.26 | 1.20 ± 0.20 | |||
| 9/0–9/12 | Mesial | 62 | 0.91 ± 0.30 | 82 | 1.06 ± 0.27 |
| Distal | 0.88 ± 0.28 | 1.05 ± 0.26 | |||
| 10/0–10/12 | Mesial | 21 | 0.89 ± 0.39 | 33 | 0.97 ± 0.30 |
| Distal | 0.89 ± 0.39 | 0.99 ± 0.29 | |||
| 11/0–11/12 | Mesial | 4 | 0.84 ± 0.37 | 8 | 0.98 ± 0.30 |
| Distal | 0.76 ± 0.47 | 1.03 ± 0.33 | |||
| 12/0–12/12 | Mesial | 1 | 1.13 * | 3 | 0.95 ± 0.26 |
| Distal | 0.89 * | 0.91 ± 0.20 |
| Dental Age Range | Root | n | CRR #74 ± S.D. + | n | CRR #75 ± S.D. |
|---|---|---|---|---|---|
| 4/0–4/12 | Mesial | 8 | 1.60 ± 0.14 | 8 | 1.47 ± 0.12 |
| Distal | 1.42 ± 0.20 | 1.46 ± 0.13 | |||
| 5/0–5/12 | Mesial | 14 | 1.50 ± 0.21 | 15 | 1.47 ± 0.21 |
| Distal | 1.47 ± 0.25 | 1.45 ± 0.18 | |||
| 6/0–6/12 | Mesial | 16 | 1.51 ± 0.19 | 20 | 1.45 ± 0.16 |
| Distal | 1.40 ± 0.2 | 1.43 ± 0.20 | |||
| 7/0–7/12 | Mesial | 108 | 1.36 ± 0.26 | 130 | 1.36 ± 0.17 |
| Distal | 1.26 ± 0.22 | 1.35 ± 0.16 | |||
| 8/0–8/12 | Mesial | 94 | 1.12 ± 0.26 | 108 | 1.21 ± 0.19 |
| Distal | 1.09 ± 0.24 | 1.19 ± 0.19 | |||
| 9/0–9/12 | Mesial | 46 | 0.93 ± 0.29 | 62 | 1.12 ± 0.30 |
| Distal | 0.91 ± 0.31 | 1.11 ± 0.28 | |||
| 10/0–10/12 | Mesial | 23 | 0.81 ± 0.41 | 30 | 0.98 ± 0.28 |
| Distal | 0.82 ± 0.36 | 0.97 ± 0.31 | |||
| 11/0–11/12 | Mesial | 11 | 0.73 ± 0.33 | 19 | 0.86 ± 0.19 |
| Distal | 0.67 ± 0.32 | 0.98 ± 0.24 | |||
| 12/0–12/12 | Mesial | 2 | 1.07 ± 0.15 | 8 | 0.68 ± 0.19 |
| Distal | 0.93 ± 0.04 | 0.73 ± 0.20 |
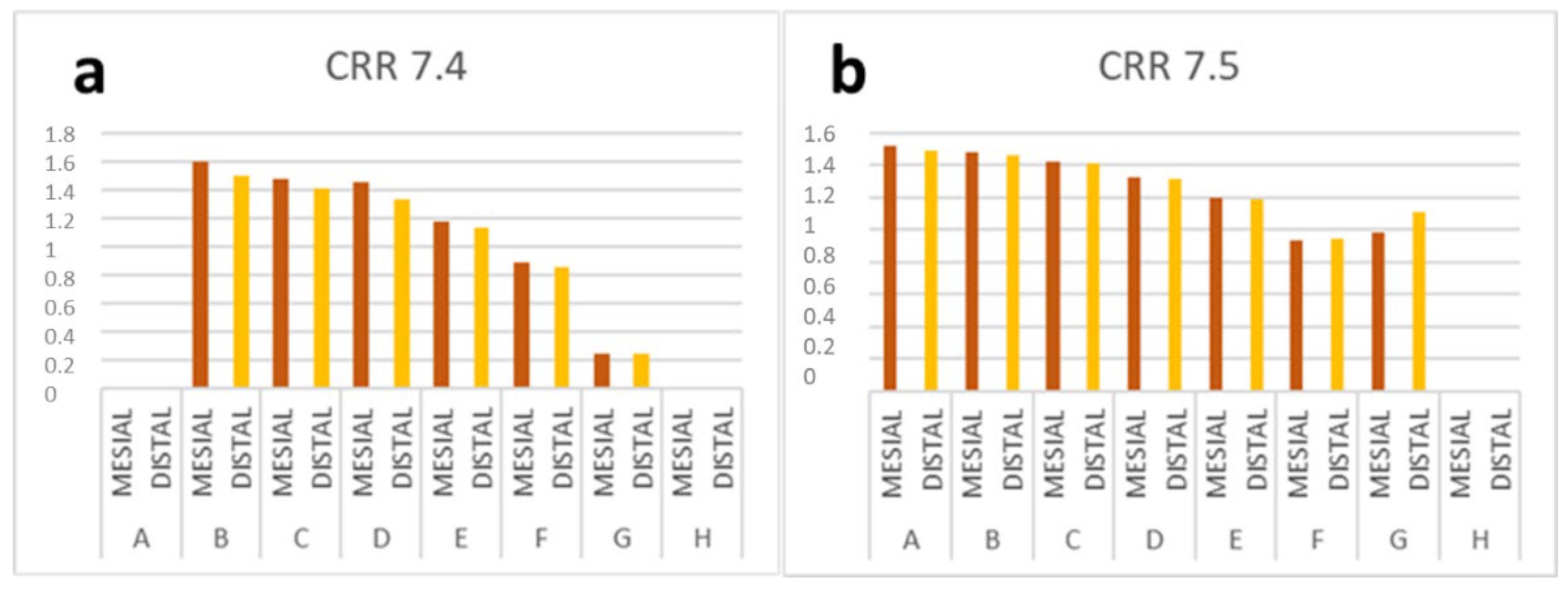
| Stages of Development of #34 | Root | N | CRR #74 ± S.D. + | Stages of Development of #35 | ROOT | n | CRR #75 ± S.D. |
|---|---|---|---|---|---|---|---|
| A | Mesial | 0 | - | A | MESIAL | 0 | 1.52 ± 0.20 |
| Distal | - | DISTAL | 1.49 ± 0.22 | ||||
| B | Mesial | 5 | 1.60 ± 0.21 | B | MESIAL | 22 | 1.48 ± 0.19 |
| Distal | 1.50 ± 0.17 | DISTAL | 1.46 ± 0.16 | ||||
| C | Mesial | 28 | 1.48 ± 0.20 | C | MESIAL | 32 | 1.42 ± 0.14 |
| Distal | 1.41 ± 0.23 | DISTAL | 1.41 ± 0.18 | ||||
| D | Mesial | 61 | 1.45 ± 0.26 | D | MESIAL | 139 | 1.32 ± 0.18 |
| Distal | 1.33 ± 0.20 | DISTAL | 1.31 ± 0.17 | ||||
| E | Mesial | 147 | 1.18 ± 0.25 | E | MESIAL | 5 | 1.20 ± 0.23 |
| Distal | 1.13 ± 0.25 | DISTAL | 1.19 ± 0.21 | ||||
| F | Mesial | 79 | 0.89 ± 0.33 | F | MESIAL | 70 | 0.93 ± 0.28 |
| Distal | 0.86 ± 0.31 | DISTAL | 0.94 ± 0.27 | ||||
| G | Mesial | 2 | 0.25 ± 0.28 | G | MESIAL | 2 | 0.98 ± 0.12 |
| Distal | 0.25 ± 0.28 | DISTAL | 1.11 ± 0.07 | ||||
| H | Mesial | 0 | - | H | MESIAL | 0 | - |
| Distal | - | DISTAL | - |
References
- Bolan, M.; Rocha, M.J. Histopathologic study of physiological and pathological resorptions in human primary teeth. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2007, 104, 680–685. [Google Scholar] [CrossRef] [PubMed]
- Prove, S.A.; Symons, A.L.; Meyers, I.A. Physiological root resorption of primary molars. J. Clin. Pediatr. Dent. 1992, 16, 202. [Google Scholar] [PubMed]
- Harokopakis-Hajishengallis, E. Physiologic root resorption in primary teeth: Molecular and Histological events. J. Oral Sci. 2007, 49, 1–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, P.H.; Heffez, L.B. Multiple idiopathic resorption in the primary dentition. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 1999, 88, 501–505. [Google Scholar] [CrossRef]
- Monteiro, J.; Day, P.; Duggal, M.; Morgan, C.; Rodd, H. Pulpal status of human primary teeth with physiological root resorption. Int. J. Paediatr. Dent. 2009, 19, 16–25. [Google Scholar] [CrossRef]
- Haralabakis, N.; Yiagtzis, S.C.; Tountoutzakis, N. Premature o delayed exfoliation of deciduos teeh and root resorption and formation. Angle Orthod. 1994, 64, 151–157. [Google Scholar]
- Obersztyn, A. Experimental Investigation of Factor Causing Resorption of Deciduos Teeth. J. Dent. Res. 1963, 42, 660–674. [Google Scholar] [CrossRef]
- Sahara, N.; Ozawa, H. Cementum-Like Tissue Deposition on the Resorbed Enamel Surface of Human Deciduous Teeth Prior to Shedding. Anat. Rec. 2004, 279, 779–791. [Google Scholar] [CrossRef]
- Bjerklin, K.; Al-Naijjar, M.; Kárestedt, H.; Andren, A. Agenesis of mandibular second premolars with retained primary molars. A longitudinal radiographic study of 99 subjects from 12 years of age to adulthood. Eur. J. Orthod. 2008, 30, 254–261. [Google Scholar] [CrossRef]
- Cardoso Silva, C.; Maroto Edo, M.; Álvaro Llorente, M.A.; Barbería Leache, E. Primary molar infraocclusion: Frequency, magnitude, root resorption and premolar agenesis in a Spanish sample. Eur. J. Paediatr. Dent. 2014, 15, 258–264. [Google Scholar]
- Fanning, E. A longitudinal study of tooth formation and root resorption. N. Z. Dent. J. 1961, 57, 202–217. [Google Scholar]
- Dos Santos, C.C.O.; Melo, D.L.; da Silva, P.P.; Normando, D. What is the survival rate of deciduous molars in cases with agenesis of premolar successors? A systematic review. Angle Orthod. 2022, 92, 110–117. [Google Scholar] [CrossRef] [PubMed]
- Haavikko, K. The physiological resorption of the roots of deciduous teeth in Helsinki children. Proc. Finn. Dent. 1973, 69, 93–98. [Google Scholar]
- Rose, J.S. Variations in the developmental position of unerupted premolar. Dent. Pract. Dent. Rec. 1962, 12, 212–217. [Google Scholar]
- Wasserstein, A.; Brezniak, N.; Shalis, M.; Heller, M.; Rakocz, M. Angular changes and their rates in concurrence to developmental stages of the mandibular second premolar. Angle Orthod. 2004, 74, 332–336. [Google Scholar]
- Black, G.V. Descriptive Anatomy of Human Teeth; White Dental Company: Philadelphia, PA, USA, 1890. [Google Scholar]
- Ash, N. Anatomía, Fisiología y Oclusión Dental, 9th ed.; Elsevier: Barcelona, Spain, 2010. [Google Scholar]
- Demirjian, A.; Goldstein, H. New system for dental maturity based on seven and four teeth. Ann. Hum. Biol. 1976, 3, 411–421. [Google Scholar] [CrossRef]
- Demirjian, A.; Goldstein, H.; Tanner, J.M. A new system of dental age assessment. Hum. Biol. 1973, 45, 211–227. [Google Scholar]
- Moorrees, C.F.A.; Fanning, E.A.; Hunt, E.E. Formation and resorption of three deciduos teeth in children. Am. J. Phys. Anthtop. 1963, 21, 205–213. [Google Scholar] [CrossRef]
- Daito, M.; Kawahara, S.; Kato, M.; Okamoto, K.; Imai, G.; Hieda, T. Radiographic observations on root resorption in primary dentition. J. Osaka Dent. Univ. 1991, 25, 1–23. [Google Scholar] [CrossRef]
- Haavikko, K. Correlation between the root resorption of decidous teeth and the formation of the corresponding permanent teeth. Proc. Finn. Dent. Soc. 1973, 69, 191–201. [Google Scholar]
- Feijóo, G.; Barbería, E.; De Nova, J.; Prieto, J.L. Permanent teeth development in a Spanish sample. Application to dental age estimation. Forensic Sci. Int. 2012, 214, 213.e1–213.e6. [Google Scholar] [CrossRef] [PubMed]
- Haavikko, K. Tooth formation age estimated on a few selected teeth. A simple method for clinical use. Proc. Finn. Dent. Soc. 1974, 70, 15–19. [Google Scholar] [PubMed]
- Harris, E.F. Technical Note: Primary tooth mineralization and exfoliation ages calculated from the Moorrees-Fanning-Hunt study. Dent. Anthropol. 2010, 23, 61–65. [Google Scholar] [CrossRef] [Green Version]
- White, S.C.; Pharoah, M.J. Radiología Oral. Principios e Interpretación, 4th ed.; Ediciones Harcout: Madrid, Spain, 2001. [Google Scholar]
- González-Salazar, F.; Márquez-Preciado, R.; Nava-Zárate, N.; Torre-Martínez, H.N. Comparison of tripe image area using panoramic radiography of child and adult dry skull. Eur. J. Paediatric. Dent. 2008, 9, 59–64. [Google Scholar]
- Puricelli, E. Panorametry: Suggestion of a method for mandibular measurements on panoramic radiographs. Head Face Med. 2009, 5, 19. [Google Scholar] [CrossRef] [Green Version]
- Laster, W.S.; Ludlow, J.B.; Bailey, L.J.; Hershey, H.G. Accuracy of measurements of mandibular anatomy and prediction of asymetry in panoramic radiographic images. Dentomaxillofac. Radiol. 2005, 34, 343. [Google Scholar] [CrossRef]
- Haavikko, K.; Mattila, K. The reliability of Orthopantomograms in determining the stage of resorption of deciduos teeth. Proc. Finn. Dent. Soc. 1973, 69, 88–91. [Google Scholar]
- Kim, Y.K.; Park, J.Y.; Kim, J.S.; Kim, J.D. Magnification rate of digital panoramic radiographs and its effectiveness for pre-operative assessment of dental implants. Dentomaxillofac. Radiol. 2011, 40, 76–83. [Google Scholar] [CrossRef]
- Gher, M.E.; Richardson, A.C. The accuracy of dental radiographic techniques used for evaluation of implant fixture placement. Int. Periodontics Restorative Dent. 1995, 15, 268–283. [Google Scholar]
- Schmeling, A.; Olze, A.; Reisinger, W. Age estimation of living people undergoing criminal proceedings. Lancet 2001, 358, 89–90. [Google Scholar] [CrossRef]
- Philip, R.G.; Hurst, R.V. The Cant of the oclusal plane and distortion in the panoramic radiograph. Angle Orthod. 1978, 48, 317–323. [Google Scholar]
- Yitschaky, M.; Haviv, Y.; Aframian, D.J.; Abed, Y.; Redlich, M. Prediction of premolar tooth lengths based on their panoramic radiographic lengths. Dentomaxillofac. Radiol. 2004, 33, 370–372. [Google Scholar] [CrossRef] [PubMed]
- Thanyakarn, C.; Hansen, K.; Rohlin, M. Measurements of tooth length in panoramic radiographs. 2: Observer performance. Dentomaxillofac. Radiol. 1992, 21, 31–35. [Google Scholar] [CrossRef] [PubMed]
- Rejebian, G.P. A statistical correlation of individual tooth size distortions on the orthopantomographic radiograph. Am. J. Orthod. 1979, 75, 525–534. [Google Scholar] [CrossRef]
- Warren, J.J.; Yonezu, T.; Bishara, S.E. Tooth wear patterns in the deciduous dentition. Am. J. Orthod. Dentofacial Orthop. 2002, 122, 614–618. [Google Scholar] [CrossRef]
- Caleya Zambrano, A.M. Tamaños Radiculares y Coronales de Molares Temporales en una Muestra de Niños Españoles. Master’s Thesis, Universidad Complutense de Madrid, Servicio de Publicaciones, Madrid, Spain, 2011. [Google Scholar]
- Chandrappa, R.; Kamath, V.V.; Srikanth, N.; Sharada, C. Comparative evaluation of vertical crown length of deciduous and permanent teeth as a predictor of an individual height by linear stepwise regression analysis. Int. J. Forensic Odontol. 2017, 2, 2. [Google Scholar] [CrossRef]
- Brace, C.L.; Mahler, P.E. Post-Pleistocene changes in the human dentition. Am. J. Phys. Anthr. 1971, 34, 191–203. [Google Scholar] [CrossRef] [Green Version]
- Axelsson, G.; Kirveskari, P. Crown size of deciduous teeth in Icelanders. Acta Odontol. Scand. 1984, 42, 339–343. [Google Scholar] [CrossRef]
- Anderson, A.A. Dentition and occlusion development in African American children: Mesiodistal crown diameters and tooth-ize ratios of primary teeth. Pediatr. Dent. 2005, 27, 121–128. [Google Scholar]
- Marseillier, E. Les Dents Humaines. Morphologie, 9th ed.; Gauthier-Villars: Paris, France, 1975. [Google Scholar]
- Kramer, W.S.; Ireland, R.L. Measurements of the primary teeth. J. Dent. Child. 1959, 26, 252–261. [Google Scholar]
- Liversidge, H.M.; Dean, M.C.; Molleson, T.I. Increasing human tooth length between birth and 5,4 years. Am. J. Phys. Anthr. 1993, 90, 307–313. [Google Scholar] [CrossRef] [PubMed]
- Sujitha, P.; Bhavyaa, R.; Muthu, S.; Latha, N.; Sneha, P. Crown dimensions of primary teeth—A systematic review and meta-analysis. J. Forensic Sci. 2022. [Google Scholar] [CrossRef]
- Rowlands, P.; Poling, R.; Slater, D.; Hobson, R.; Steen, N. Can crown-root ratio predict premolar eruption? Am. J. Orthod. Dentofac. Orthop. 2006, 129, 331–336. [Google Scholar] [CrossRef]
- Alansary, M.; Drummond, B.; Coates, D. Immunocytochemical characterization of primary teeth pulp stem cells from three stages of resorption in serum-free medium. Dent. Traumatol. 2021, 37, 90–102. [Google Scholar] [CrossRef] [PubMed]
- Murthy, P.; Bhojraj, N.; Hegde, U. Ultrastructural morphologic pattern in the roots of deciduous teeth in different stages of physiologic resorption. Pediatr. Dent. J. 2020, 30, 215–223. [Google Scholar] [CrossRef]



| Stage of Develpment #34 | CRR-M #74 | CRR-D #74 | Differences | t Test p | ||
|---|---|---|---|---|---|---|
| Mean ± S.D. + | Mean ± S.D. | Mean Difference | Confidence Interval 95% | |||
| Higher | Lower | |||||
| Stage B | 1.596 ± 0.113 | 1.502 ± 0.167 | 0.094 | −0.018 | 0.206 | 0.081 |
| Stage C | 1.481 ± 0.203 | 1.406 ± 0.225 | 0.075 | −0.009 | 0.158 | 0.078 |
| Stage D | 1.454 ± 0.262 | 1.326 ± 0.204 | 0.128 | 0.787 | 0.177 | 0.000 * |
| Stage E | 1.178 ± 0.254 | 1.132 ± 0.246 | 0.046 | −0.167 | 0.076 | 0.002 * |
| Stage F | 0.890 ± 0.333 | 0.863 ± 0.308 | 0.027 | −0.015 | 0.069 | 0.211 |
| BOYS (N = 177) | ||||||
| Stage B | 1.557 ± 0.140 | 1.467 ± 0.196 | 0.090 | −0.107 | 0.287 | 0.188 |
| Stage C | 1.470 ± 0.236 | 1.441 ± 0.264 | 0.028 | −0.091 | 0.149 | 0.617 |
| Stage D | 1.470 ± 0.256 | 1.333 ± 0.200 | 0.057 | 0.014 | 0.101 | 0.001 * |
| Stage E | 1.179 ± 0.260 | 1.121 ± 0.249 | −0.009 | −0.296 | 0.278 | 0.010 * |
| Stage F | 0.924 ± 0.289 | 0.894 ± 0.273 | 0.030 | −0.030 | 0.090 | 0.321 |
| GIRLS (N = 145) | ||||||
| Stage B | 1.655 ± 0.21 | 1.555 ± 0.162 | 0.100 | −1.170 | 1.371 | 0.500 |
| Stage C | 1.495 ± 0.157 | 1.360 ± 0.158 | 0.135 | 0.013 | 0.259 | 0.033 * |
| Stage D | 1.435 ± 0.273 | 1.318 ± 0.211 | 0.117 | 0.054 | 0.179 | 0.001 * |
| Stage E | 1.178 ± 0.247 | 1.145 ± 0.242 | 0.032 | −0.007 | 0.728 | 0.106 |
| Stage F | 0.842 ± 0.387 | 0.820 ± 0.350 | 0.022 | −0.038 | 0.082 | 0.455 |
| Stage of Development #35 | CRR-m 75 | CRR-d 75 | Differences | t Test p | ||
|---|---|---|---|---|---|---|
| Mean ± S.D. + | Mean ± S.D. | Mean Difference | Confidence Interval 95% | |||
| Higher | Lower | |||||
| Stage A | 1.520 ± 0.197 | 1.490 ± 0.214 | 0.030 | −0.026 | 0.086 | 0.208 |
| Stage B | 1.476 ± 0.185 | 1.464 ± 0.161 | 0.011 | −0.022 | 0.044 | 0.484 |
| Stage C | 1.420 ± 0.140 | 1.414 ± 0.179 | 0.006 | −0.055 | 0.068 | 0.846 |
| Stage D | 1.320 ± 0.177 | 1.306 ± 0.172 | 0.013 | −0.008 | 0.035 | 0.229 |
| Stage E | 1.201 ± 0.230 | 1.190 ± 0.216 | 0.011 | −0.018 | 0.039 | 0.467 |
| Stage F | 0.931 ± 0.276 | 0.940 ± 0.267 | −0.009 | −0.04 | 0.030 | 0.642 |
| BOYS (N = 221) | ||||||
| Stage B | 1.432 ± 0.187 | 1.409 ± 0.168 | 0.023 | −0.014 | 0.059 | 0.195 |
| Stage C | 1.423 ± 0.137 | 1.469 ± 0.205 | −0.046 | −0.148 | 0.055 | 0.433 |
| Stage D | 1.305 ± 0.170 | 1.274 ± 0.152 | 0.032 | 0.001 | 0.062 | 0.043 * |
| Stage E | 1.205 ± 0.239 | 1.207 ± 0.234 | −0.002 | −0.040 | 0.036 | 0.916 |
| Stage F | 0.953 ± 0.280 | 0.986 ± 0.283 | −0.033 | −0.083 | 0.016 | 0.180 |
| GIRLS (N = 180) | ||||||
| Stage A | 1.490 ± 0.170 | 1.415 ± 0.205 | 0.075 | −0.243 | 0.392 | 0.205 |
| Stage B | 1.519 ± 0.182 | 1.519 ± 0.141 | 0.000 | −0.062 | 0.062 | 1.000 |
| Stage C | 1.417 ± 0.148 | 1.371 ± 0.148 | 0.047 | −0.033 | 0.126 | 0.234 |
| Stage D | 1.335 ± 0.183 | 1.342 ± 0.185 | −0.007 | −0.038 | 0.023 | 0.633 |
| Stage E | 1.195 ± 0.217 | 1.165 ± 0.186 | 0.030 | −0.014 | 0.075 | 0.173 |
| Stage F | 0.902 ± 0.271 | 0.879 ± 0.235 | 0.023 | −0.042 | 0.088 | 0.474 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Caleya, A.M.; Gallardo, N.E.; Feijoo, G.; Mourelle-Martínez, M.R.; Martín-Vacas, A.; Maroto, M. Relationship between Physiological Resorption of Primary Molars with Its Permanent Successors, Dental Age and Chronological Age. Children 2022, 9, 941. https://0-doi-org.brum.beds.ac.uk/10.3390/children9070941
Caleya AM, Gallardo NE, Feijoo G, Mourelle-Martínez MR, Martín-Vacas A, Maroto M. Relationship between Physiological Resorption of Primary Molars with Its Permanent Successors, Dental Age and Chronological Age. Children. 2022; 9(7):941. https://0-doi-org.brum.beds.ac.uk/10.3390/children9070941
Chicago/Turabian StyleCaleya, Antonia M., Nuria E. Gallardo, Gonzalo Feijoo, M. Rosa Mourelle-Martínez, Andrea Martín-Vacas, and Myriam Maroto. 2022. "Relationship between Physiological Resorption of Primary Molars with Its Permanent Successors, Dental Age and Chronological Age" Children 9, no. 7: 941. https://0-doi-org.brum.beds.ac.uk/10.3390/children9070941