
TITF1 Screening in Human Congenital Diaphragmatic Hernia (CDH)

 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
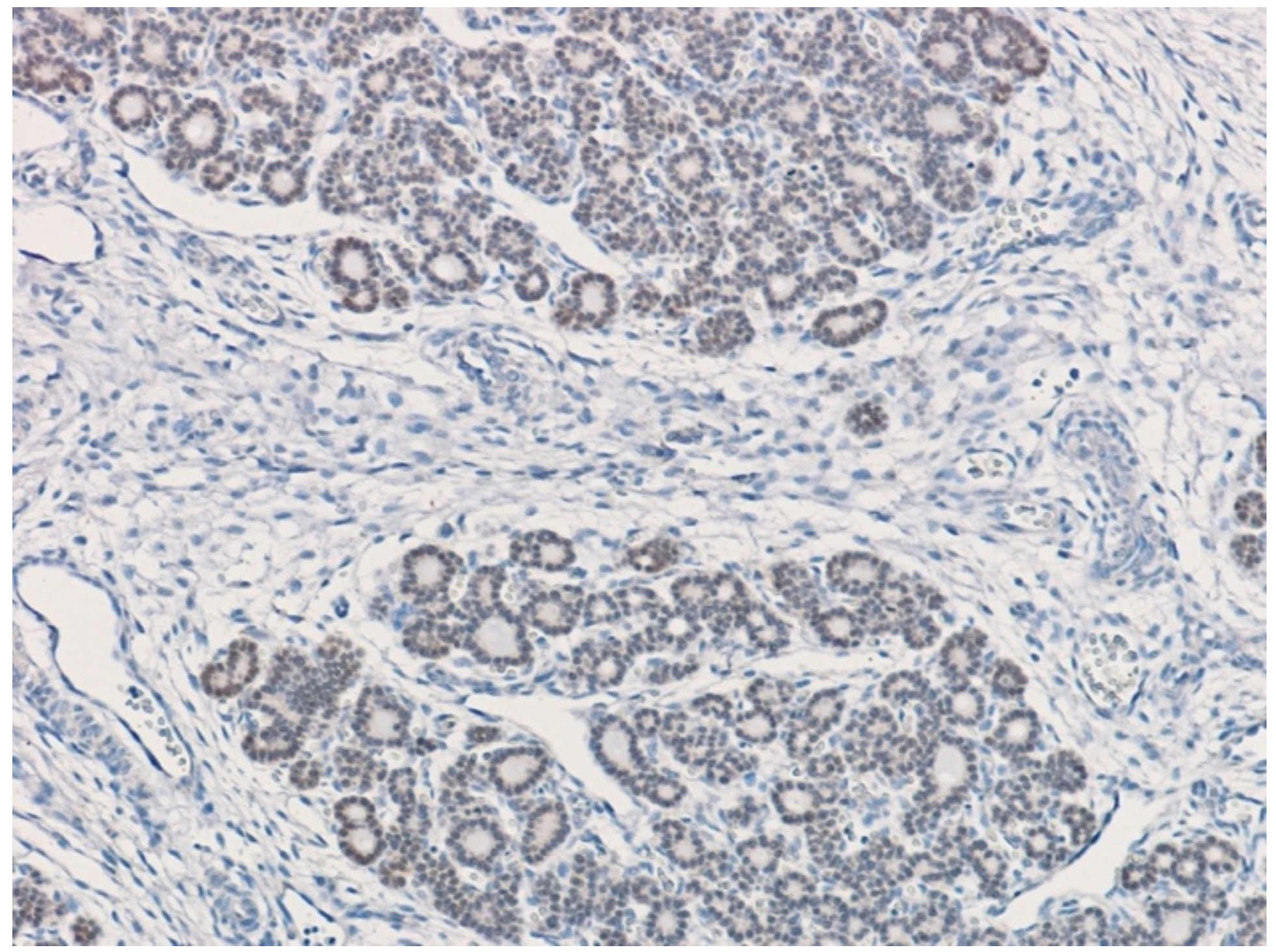
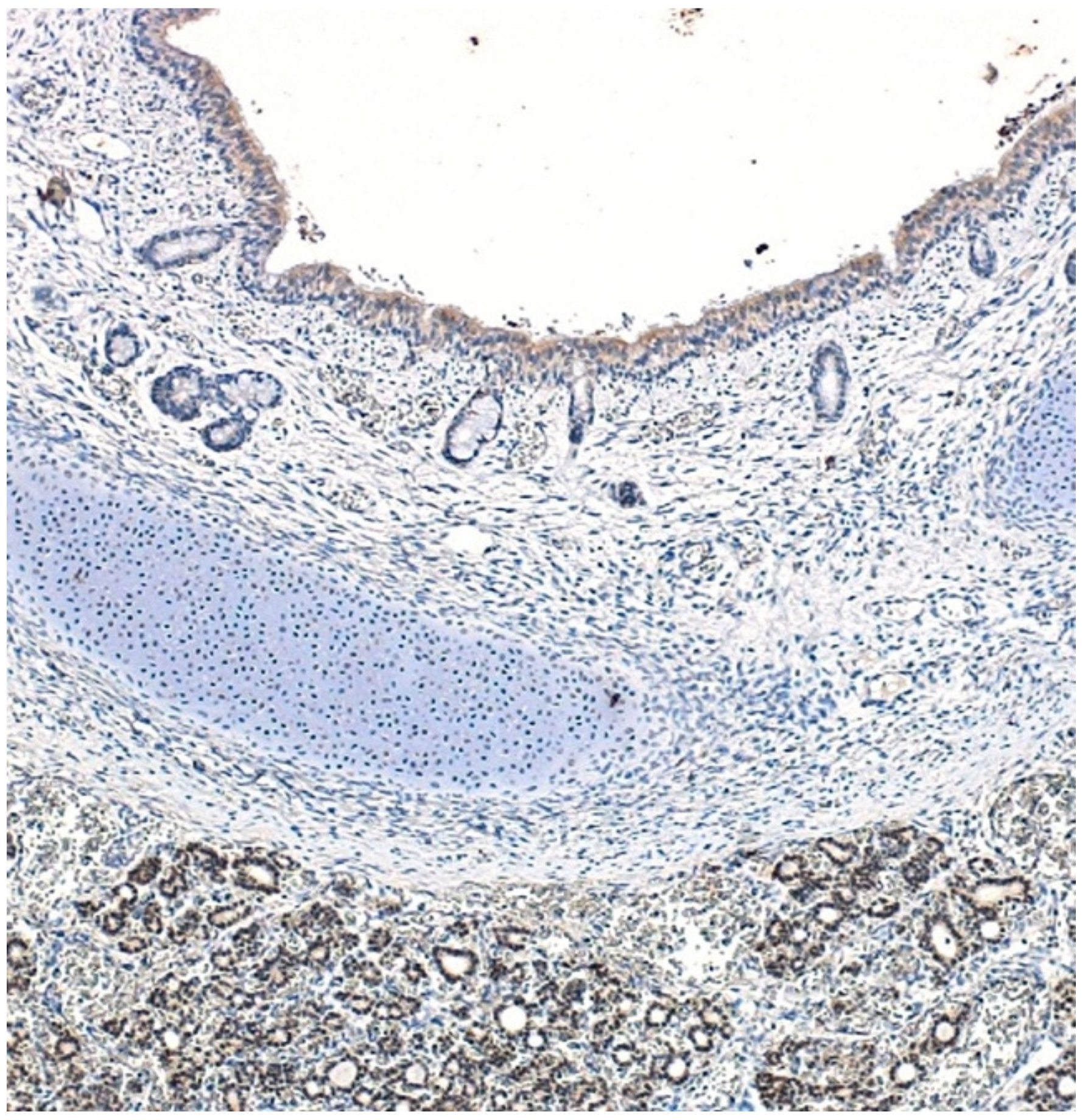
2.1. Immunohistochemistry: Fetuses
2.2. Molecular Genetics: CDH Patients
3. Results
3.1. Fetuses
3.2. CDH Patients
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Torfs, C.P.; Curry, C.J.R.; Bateson, T.F.; Honoré, L.H. A population-based study of congenital diaphragmatic hernia. Teratology 1992, 46, 555–565. [Google Scholar] [CrossRef]
- McGivern, M.R.; Best, K.; Rankin, J.; Wellesley, D.; Greenlees, R.; Addor, M.-C.; Arriola, L.; De Walle, H.; Barisic, I.; Beres, J.; et al. Epidemiology of congenital diaphragmatic hernia in Europe: A register-based study. Arch. Dis. Child.-Fetal Neonatal Ed. 2015, 100, F137–F144. [Google Scholar] [CrossRef]
- Yang, W.; Carmichael, S.L.; Harris, J.A.; Shaw, G.M. Epidemiologic characteristics of congenital diaphragmatic hernia among 2.5 million California births, 1989–1997. Birth Defects Res. Part A Clin. Mol. Teratol. 2006, 76, 170–174. [Google Scholar] [CrossRef]
- Gallot, D.; Boda, C.; Ughetto, S.; Perthus, I.; Robert-Gnansia, E.; Francannet, C.; Laurichesse-Delmas, H.; Jani, J.; Coste, K.; Deprest, J.; et al. Prenatal detection and outcome of congenital diaphragmatic hernia: A French registry-based study. Ultrasound Obstet. Gynecol. 2007, 29, 276–283. [Google Scholar] [CrossRef]
- Colvin, J.; Bower, C.; Dickinson, J.E.; Sokol, J. Outcomes of congenital diaphragmatic hernia: A population-based study in Western Australia. Pediatrics 2005, 116, e356–e363. [Google Scholar] [CrossRef] [Green Version]
- Chandrasekharan, P.K.; Rawat, M.; Madappa, R.; Rothstein, D.H.; Lakshminrusimha, S. Congenital Diaphragmatic hernia—A review. Matern. Health Neonatol. Perinatol. 2017, 3, 6. [Google Scholar] [CrossRef] [Green Version]
- Nakamura, Y.; Yamamoto, I.; Fukuda, S.; Hashimoto, T. Pulmonary acinar development in diaphragmatic hernia. Arch. Pathol. Lab. Med. 1991, 115, 372–376. [Google Scholar]
- Morini, F.; Lally, K.P.; Lally, P.A.; Crisafulli, R.M.; Capolupo, I.; Bagolan, P. Treatment Strategies for Congenital Diaphragmatic Hernia: Change Sometimes Comes Bearing Gifts. Front. Pediatr. 2017, 5, 195. [Google Scholar] [CrossRef] [Green Version]
- Deprest, J.; Brady, P.; Nicolaides, K.; Benachi, A.; Berg, C.; Vermeesch, J.; Gardener, G.; Gratacos, E. Prenatal management of the fetus with isolated congenital diaphragmatic hernia in the era of the TOTAL trial. Semin. Fetal Neonatal Med. 2014, 19, 338–348. [Google Scholar] [CrossRef]
- Coughlin, M.A.; Werner, N.L.; Gajarski, R.; Gadepalli, S.; Hirschl, R.; Barks, J.; Treadwell, M.C.; Ladino-Torres, M.; Kreutzman, J.; Mychaliska, G. Prenatally diagnosed severe CDH: Mortality and morbidity remain high. J. Pediatr. Surg. 2016, 51, 1091–1095. [Google Scholar] [CrossRef]
- Wells, L.J. A study of closure of the pleuropericardial and pleuroperitoneal canals in the human embryo. Anat. Rec. 1947, 97, 428. [Google Scholar] [CrossRef]
- Harrison, M.R.; Jester, J.A.; Ross, N.A. Correction of congenital diaphragmatic hernia in utero. I. The model: Intrathoracic balloon produces fatal pulmonary hypoplasia. Surgery 1980, 88, 174–182. [Google Scholar]
- Iritani, I. Experimental study on embryogenesis of congenital diaphragmatic hernia. Anat. Embryol. 1984, 169, 133–139. [Google Scholar] [CrossRef]
- Guilbert, T.W.; Gebb, S.A.; Shannon, J.M. Lung hypoplasia in the nitrofen model of congenital diaphragmatic hernia occurs early in development. Am. J. Physiol. Cell. Mol. Physiol. 2000, 279, L1159–L1171. [Google Scholar] [CrossRef]
- Jesudason, E.C.; Connell, M.; Fernig, D.G.; Lloyd, D.A.; Losty, P.D. Early lung malformations in congenital diaphragmatic hernia. J. Pediatr. Surg. 2000, 35, 124–127, discussion 128. [Google Scholar] [CrossRef]
- Keijzer, R.; Liu, J.; Deimling, J.; Tibboel, D.; Post, M. Dual-hit hypotesis explains pulmonary hypoplasia in the nitrofen model of congenital diapragmatic hernia. Am. J. Pathol. 2000, 156, 1299–1306. [Google Scholar] [CrossRef]
- Kunisaki, S.M.; Jiang, G.; Biancotti, J.C.; Ho, K.K.Y.; Dye, B.R.; Liu, A.P.; Spence, J.R. Human induced pluripotent stem cell-derived lung organoids in an ex vivo model of the congenital diaphragmatic hernia fetal lung. Stem Cells Transl. Med. 2021, 10, 98–114. [Google Scholar] [CrossRef]
- Kardon, G.; Ackerman, K.G.; McCulley, D.J.; Shen, Y.; Wynn, J.; Shang, L.; Bogenschutz, E.; Sun, X.; Chung, W.K. Congenital diaphragmatic hernias: From genes to mechanisms to therapies. Dis. Model. Mech. 2017, 10, 955–970. [Google Scholar] [CrossRef] [Green Version]
- Yu, L.; Sawle, A.D.; Wynn, J.; Aspelund, G.; Stolar, C.J.; Arkovitz, M.S.; Potoka, D.; Azarow, K.S.; Mychaliska, G.B.; Shen, Y.; et al. Increased burden of de novo predicted deleterious variants in complex congenital diaphragmatic hernia. Hum. Mol. Genet. 2015, 24, 4764–4773. [Google Scholar] [CrossRef] [Green Version]
- Beurskens, L.W.J.E.; Tibboel, D.; Lindemans, J.; Duvekot, J.J.; Cohen-Overbeek, T.E.; Veenma, D.C.M.; de Klein, A.; Greer, J.J.; Steegers-Theunissen, R.P.M. Retinol status of newborn infants is associated with congenital diaphragmatic hernia. Pediatrics 2010, 126, 712–720. [Google Scholar] [CrossRef]
- Beurskens, L.W.; Tibboel, D.; Steegers-Theunissen, R.P. Role of nutrition, lifestyle factors, and genes in the pathogenesis of congenital diaphragmatic hernia: Human and animal studies. Nutr. Rev. 2009, 67, 719–730. [Google Scholar] [CrossRef]
- Lazzaro, D.; Price, M.; de Felice, M.; Di Lauro, R. The transcription factor TTF-1 is expressed at the onset of thyroid and lung morphogenesis and in restricted regions of the foetal brain. Development 1991, 113, 1093–1104. [Google Scholar] [CrossRef]
- Kimura, S.; Hara, Y.; Pineau, T.; Fernandez-Salguero, P.; Fox, C.H.; Ward, J.M.; Gonzalez, F.J. The T/ebp null mouse: Thyroid-specific enhancer-binding protein is essential for the organogenesis of the thyroid, lung, ventral forebrain, and pituitary. Genes Dev. 1996, 10, 60–69. [Google Scholar] [CrossRef] [Green Version]
- Kimura, S.; Ward, J.M.; Minoo, P. Thyroid-specific enhancer-binding protein/thyroid transcription factor 1 is not required for the initial specification of the thyroid and lung primordia. Biochimie 1999, 81, 321–327. [Google Scholar] [CrossRef]
- Minoo, P.; Hamdan, H.; Bu, D.; Warburton, D.; Stepanik, P.; deLemos, R. TTF-1 regulates lung epithelial morphogenesis. Dev. Biol. 1995, 172, 694–698. [Google Scholar] [CrossRef] [Green Version]
- Minoo, P.; Li, C.; Liu, H.B.; Hamdan, H.; DeLemos, R. TTF-1 is an epithelial morphoregulatory transcriptional factor. Chest 1997, 111, 135S–137S. [Google Scholar] [CrossRef]
- Minoo, P.; Su, G.; Drum, H.; Bringas, P.; Kimura, S. Defects in tracheoesophageal and lung morphogenesis in Nkx2.1(-/-) mouse embryos. Dev. Biol. 1999, 209, 60–71. [Google Scholar] [CrossRef] [Green Version]
- Snyder, E.L.; Watanabe, H.; Magendantz, M.; Hoersch, S.; Chen, T.A.; Wang, D.G.; Crowley, D.; Whittaker, C.A.; Meyerson, M.; Kimura, S.; et al. Nkx2-1 represses a latent gastric differentiation program in lung adenocarcinoma. Mol. Cell 2013, 50, 185–199. [Google Scholar] [CrossRef] [Green Version]
- Little, D.R.; Gerner-Mauro, K.N.; Flodby, P.; Crandall, E.D.; Borok, Z.; Akiyama, H.; Kimura, S.; Ostrin, E.J.; Chen, J. Transcriptional control of lung alveolar type 1 cell development and maintenance by NK homeobox 2-1. Proc. Natl. Acad. Sci. USA 2019, 116, 20545–20555. [Google Scholar] [CrossRef] [Green Version]
- Stahlman, M.T.; Gray, M.E.; Whitsett, J.A. Expression of thyroid transcription factor-1(TTF-1) in fetal and neonatal human lung. J. Histochem. Cytochem. 1996, 44, 673–678. [Google Scholar] [CrossRef] [Green Version]
- Paris, N.D.; Coles, G.L.; Ackerman, K.G. Wt1 and β-catenin cooperatively regulate diaphragm development in the mouse. Dev. Biol. 2015, 407, 40–56. [Google Scholar] [CrossRef] [Green Version]
- Schwab, M.E.; Dong, S.; Lianoglou, B.R.; Lucero, A.F.A.; Schwartz, G.B.; Norton, M.E.; MacKenzie, T.C.; Sanders, S.J. Exome sequencing of fetuses with congenital diaphragmatic hernia supports a causal role for NR2F2, PTPN11, and WT1 variants. Am. J. Surg. 2022, 223, 182–186. [Google Scholar] [CrossRef]
- Wat, M.J.; Veenma, D.; Hogue, J.; Holder, A.; Yu, Z.; Wat, J.J.; Hanchard, N.; Shchelochkov, O.A.; Fernandes, C.; Johnson, A.; et al. Genomic alterations that contribute to the development of isolated and non-isolated congenital diaphragmatic hernia. J. Med. Genet. 2011, 48, 299–307. [Google Scholar] [CrossRef]
- Wilson, J.G.; Roth, C.B.; Warkany, J. An analysis of the syndrome of malformations induced by maternal vitamin A deficiency. Effects of restoration of vitamin A at various times during gestation. Am. J. Anat. 1953, 92, 189–217. [Google Scholar] [CrossRef]
- Mendelsohn, C.; Lohnes, D.; Décimo, D.; Lufkin, T.; LeMeur, M.; Chambon, P.; Mark, M. Function of the retinoic acid receptors (RARs) during development (II). Multiple abnormalities at various stages of organogenesis in RAR double mutants. Development 1994, 120, 2749–2771. [Google Scholar] [CrossRef]
- Kelly, M.; von Lintig, J. STRA6: Role in cellular retinol uptake and efflux. Hepatobiliary Surg. Nutr. 2015, 4, 229–242. [Google Scholar] [CrossRef]
- Pasutto, F.; Sticht, H.; Hammersen, G.; Gillessen-Kaesbach, G.; FitzPatrick, D.R.; Nürnberg, G.; Brasch, F.; Schirmer-Zimmermann, H.; Tolmie, J.L.; Chitayat, D.; et al. Mutations in STRA6 cause a broad spectrum of malformations including anophthalmia, congenital heart defects, diaphragmatic hernia, alveolar capillary dysplasia, lung hypoplasia, and mental retardation. Am. J. Hum. Genet. 2007, 80, 550–560. [Google Scholar] [CrossRef] [Green Version]
- Van Esch, H.; Backx, L.; Pijkels, E.; Fryns, J.P. Congenital diaphragmatic hernia is part of the new 15q24 microdeletion syndrome. Eur. J. Med. Genet. 2009, 52, 153–156. [Google Scholar] [CrossRef]
- Steiner, M.B.; Vengoechea, J.; Collins, R.T. Duplication of the ALDH1A2 gene in association with pentalogy of Cantrell: A case report. J. Med. Case Rep. 2013, 7, 287. [Google Scholar] [CrossRef] [Green Version]
- Henriques-Coelho, T.; Oliva-Teles, N.; Fonseca-Silva, M.L.; Tibboel, D.; Guimarães, H.; Correia-Pinto, J. Congenital diaphragmatic hernia in a patient with tetrasomy 9p. Pediatr. Surg. 2005, 40, e29–e31. [Google Scholar] [CrossRef] [Green Version]
- Klaassens, M.; van Dooren, M.; Eussen, H.; Douben, H.; Dekker, A.D.; Lee, C.; Donahoe, P.; Galjaard, R.; Goemaere, N.; de Krijger, R.; et al. Congenital diaphragmatic hernia and chromosome 15q26: Determination of a candidate region by use of fluorescent in situ hybridization and array-based comparative genomic hybridization. Am. J. Hum. Genet. 2005, 76, 877–882. [Google Scholar] [CrossRef] [Green Version]
- You, L.-R.; Takamoto, N.; Yu, C.-T.; Tanaka, T.; Kodama, T.; DeMayo, F.J.; Tsai, S.Y.; Tsai, M.-J. Mouse lacking COUP-TFII as an animal model of Bochdalek-type congenital diaphragmatic hernia. Proc. Natl. Acad. Sci. USA 2005, 102, 16351–16356. [Google Scholar] [CrossRef] [Green Version]
- Cooney, A.J.; Tsai, S.Y.; O’Malley, B.W.; Tsai, M.J. Chicken ovalbumin upstream promoter transcription factor (COUP-TF) dimers bind to different GGTCA response elements, allowing COUP-TF to repress hormonal induction of the vitamin D3, thyroid hormone, and retinoic acid receptors. Mol. Cell. Biol. 1992, 12, 4153–4163. [Google Scholar] [CrossRef]
- Brady, P.D.; DeKoninck, P.; Fryns, J.P.; Devriendt, K.; Deprest, J.A.; Vermeesch, J.R. Identification of dosage-sensitive genes in fetuses referred with severe isolated congenital diaphragmatic hernia. Prenat. Diagn. 2013, 33, 1283–1292. [Google Scholar] [CrossRef]
- Schreiner, Y.; Schaible, T.; Rafat, N. Genetics of diaphragmatic hernia. Eur. J. Hum. Genet. 2021, 29, 1729–1733. [Google Scholar] [CrossRef]
- Chapin, C.J.; Ertsey, R.; Yoshizawa, J.; Hara, A.; Sbragia, L.; Greer, J.J.; Kitterman, J.A. Congenital diaphragmatic hernia, tracheal occlusion, thyroid transcription factor-1, and fetal pulmonary epithelial maturation. Am. J. Physiol. Cell. Mol. Physiol. 2005, 289, L44–L52. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Male/Female | Sporadic/Familial | Disease during Pregnancy | Left/Right Broad | Pulmonary Hypoplasia | Associated Anomalies | Survivor | |
|---|---|---|---|---|---|---|---|
| CDH01 | M | Familial | - | Right | Severe | - | not |
| CDH02 | M | Sporadic | - | Right | Severe | Pectus excavatum | yes |
| CDH03 | F | Familial | - | Left | Mild | - | |
| CDH04 | M | Familial | - | Left | Mild | - | - |
| CDH05 | F | Familial | - | Left | Mild | Tricuspid regurgitation | yes |
| CDH06 | M | Sporadic | - | Left | Mild | - | yes |
| CDH07 | F | Sporadic | - | Left | Mild | - | yes |
| CDH08 | F | Sporadic | - | Left | Mild | - | yes |
| CDH09 | F | Sporadic | - | Left | Mild | - | yes |
| CDH10 | M | Sporadic | - | Left | Mild | ||
| CDH11 | M | Sporadic | - | Right | Mild | - | yes |
| CDH12 | F | Sporadic | - | Left | Mild | - | - |
| CDH13 | M | Sporadic | - | Left | Mild | - | yes |
| CDH14 | M | Sporadic | - | Left | Mild | yes | |
| CDH15 | F | Sporadic | - | Right | Severe | Pectus excavatum | yes |
| CDH16 | M | Sporadic | - | Left | Mild | yes |
| Name | Type | Sequence 5′→3′ |
|---|---|---|
| hTiTF1 exIIF | Exon II PCR/Seq Forward | TGG CTG CCT AAA ACC TG |
| hTiTF1 exIIR | Exon II PCR/Seq Reverse | GCC GCC CTC CCT GAT GC |
| hTiTF1 exIIF2 | Exon II Seq Forward | GGA AAG CTA CAA GAA AGT GGG |
| hTiTF1 exIIR2 | Exon II Seq Reverse | CTG TTC CTC ATG GTG TCC TGG |
| hTiTF1 exIIPCRUP | Exon II PCR/Seq Forward | GAG GAC TCG GTC CAC TCC GTT AC |
| hTiTF1 exIIPCRDw | Exon II PCR/Seq Reverse | AGC GCT ACC AAG TGC CTG TTC TTG |
| hTiTF1 exIIIF | Exon III PCR/Seq Forward | AGG GTT GGG GCT GTG AG |
| hTiTF1 exIIIR | Exon III PCR/Seq Reverse | GGA TGG TGG TCT GTG TGG |
| hTiTF1 exIIIF2 | Exon III Seq Forward | ATG GCG CGG AAA ACA GG |
| hTiTF1 exIIIR2 | Exon III Seq Reverse | GCG GTG GAT GGT GGT CA |
| hTiTF1 exIIIF3 | Exon III Seq Forward | GCT TCA AGC AAC AGA AGT ACC |
| hTiTF1 exIIIR3 | Exon III Seq Reverse | ACG GTT TGC CGT CTT TCA CC |
| hTiTF1 exIIIF4 | Exon III Seq Forward | AAC AGG CTC AGC AGC AGT CG |
| hTiTF1 exIIIR4 | Exon III Seq Reverse | GTC AGG TGG ATC ATG CTG G |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gulino, M.E.; Martucciello, G.; Biffali, E.; Morbini, P.; Patti, R.; Borra, M.; Scuderi, M.G. TITF1 Screening in Human Congenital Diaphragmatic Hernia (CDH). Children 2022, 9, 1108. https://0-doi-org.brum.beds.ac.uk/10.3390/children9081108
Gulino ME, Martucciello G, Biffali E, Morbini P, Patti R, Borra M, Scuderi MG. TITF1 Screening in Human Congenital Diaphragmatic Hernia (CDH). Children. 2022; 9(8):1108. https://0-doi-org.brum.beds.ac.uk/10.3390/children9081108
Chicago/Turabian StyleGulino, Maria Eugenia, Giuseppe Martucciello, Elio Biffali, Patrizia Morbini, Roberta Patti, Marco Borra, and Maria Grazia Scuderi. 2022. "TITF1 Screening in Human Congenital Diaphragmatic Hernia (CDH)" Children 9, no. 8: 1108. https://0-doi-org.brum.beds.ac.uk/10.3390/children9081108