

Transdermal Patches Containing Opioids in the Treatment of Patients with Chronic Pain


1
Department of Industrial Engineering, University of Salerno, Via Giovanni Paolo II, 132, 84084 Fisciano, SA, Italy
2
Research Centre for Biomaterials BIONAM, University of Salerno, Via Giovanni Paolo II, 132, 84084 Fisciano, SA, Italy
Processes 2023, 11(9), 2673; https://0-doi-org.brum.beds.ac.uk/10.3390/pr11092673
Submission received: 4 July 2023
/
Revised: 17 August 2023
/
Accepted: 5 September 2023
/
Published: 6 September 2023
(This article belongs to the Special Issue Drug Carriers Production Processes for Innovative Human Applications)
Abstract
:Transdermal delivery is a non-invasive route, used as an alternative to the oral route, to administer drugs through the skin surface. One of the fields in which they are particularly used is that of pain therapy. In this treatment, transdermal patches, particularly those containing opioids, are used to complement or replace orally administered drugs. First-generation patches are constituted by reservoir systems, where the drug is dissolved in a solvent and gelled with a polymer. In contrast, the active principle is incorporated into the polymer adhesive in more recent matrix patches. In this review, the main papers related to the production and employment of transdermal patches containing the two most used opioids, i.e., fentanyl and buprenorphine, have been critically analyzed. From the analysis of the literature, it is possible to deduce that the type of drug and the amount of drug present in the patch must be chosen not according to the origin of the pain but to the age of the patient, the area where the patch is applied, and the frequency at which the patch is replaced.
1. Introduction
The International Association for the Study of Pain (IASP), which is the central organization concerned with the study of pain and possible strategies to alleviate it, currently defines pain as “an unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage” [1]. Pain can be categorized regarding its time frame and pathophysiology [2]. Concerning the former classification, pain can be acute and chronic. It is defined as “acute” if it lasts for less than three months and chronic if it restricts daily activities for more than three months [3]. Sometimes an intermediate category, called subacute pain, is considered [4]. As for the pathophysiology, pain can be divided into nociceptive, neuropathic, and nociplastic. Nociceptive pain (somatic, visceral), which is the most common form of chronic pain, is associated with damage to organs and tissues with an intact nervous system. Neuropathic pain is associated with damage or disease of the nervous system, and nociplastic pain is due to abnormal processing of pain signals without clearly identifying tissue damage or diagnosing pathologies concerning the somatosensory system [5]. It can be of somatic origin (bone fractures, muscle spasms, osteoarthritis, and postoperative pain) or visceral (peptic ulcer, cancer, liver cirrhosis, and ischemia). Neuropathic pain can affect central nerves, such as from spinal injuries, Parkinson’s disease, multiple sclerosis or transverse myelitis, or peripherally, such as with carpal tunnel syndrome, or local pain of a traumatic nature, nutritional deficiencies, and acute herpes zoster [6]. Nociplastic pain can have various causes, such as fibromyalgia, irritable bowel syndrome, or bladder pain [7]. Chronic pain, which lasts over time, is sometimes considered a real disease, with the need for pharmacological treatment (for example, to be operational although the pain) and psychological implications (for example, accepting pain) [7]. In some cases, a distinction is made according to whether the chronic pain originates from cancer or not; chronic cancer pain (CCP) and chronic non-cancer pain (CNCP) treatments are therefore considered. However, regardless of the origin, pain treatments are often common [8].
In 1986, the World Health Organization (WHO) proposed a three-step analgesic ladder (sketched in Figure 1) to provide adequate pain relief in the treatment of CCP [9], which, nowadays, is also used in the treatment of CNCP. The WHO analgesic ladder requires analgesic therapy to be established based on pain intensity:
- Mild pain can be treated with non-steroidal anti-inflammatory drugs (NSAIDs) or non-opioid analgesics such as acetaminophen or paracetamol and/or adjuvants such as antidepressants or anticonvulsants;
- Moderate pain requires the use of weak opioid analgesics, such as codeine, dihydrocodeine, tramadol, and/or adjuvants;
It is, therefore, evident that opioids are the most potent analgesics and are well-established drugs for the treatment of severe acute [13], surgical [14], and chronic pain [15].
It is important to underline that in defining analgesic therapy, it is not only necessary to consider the choice between the different active ingredients [16] but also the different administration routes, such as oral, sublingual, inhaled, intravenous, intramuscular, rectal, transdermal and topical [17]. The oral route is preferred except when oral intake is not possible because of severe vomiting, problems with swallowing, constipation, and poor compliance. To overcome these drawbacks, transdermal drug delivery (TDD) is a good choice; in addition, opioid transdermal delivery results in a lower risk of addiction than oral and parenteral routes [2]. Different research articles and reviews have been published regarding treating chronic pain using opioids; they are generally focused on the mechanism of action of the different drugs in the case of CCP and CNCP. Less frequent is the publication of reviews focused on preparing and producing patches containing opioids [2,7,16,18,19,20,21,22].
Therefore, this review aims to underlie the aspects related to the production of opioid-based patches; in particular, this study is focused on two of the most frequently administered opioids via transdermal delivery: fentanyl and buprenorphine.
2. Transdermal Drug Delivery
TDD is a non-invasive and painless way to administer active ingredients at a predetermined rate across the dermis to achieve a local or systemic effect; it consists of the application of a pharmacological formulation (generally a transdermal patch containing the active ingredients) on intact skin [23,24,25,26,27]. On the other hand, the treatment of damaged skin is different; in this case, we speak of wound healing [28,29,30,31]. TDD has different advantages over both oral and parenteral administration. Compared to the first, there is no passage of the active principle through the gastrointestinal tract; therefore, there is no loss of efficacy due to first-pass hepatic metabolism, and drugs can be administered without pH changes, enzymes, and intestinal bacteria interference [32]. The dosing frequency is also reduced, and the adverse effects arising from peak plasma drug concentrations are minimized; in addition, this method improves patient compliance and is also advisable for patients who are unconscious or who have vomiting as a symptom of their pathology or as a side effect related to the medications taken. TDD is also suitable for patients who self-administer the drugs. Compared to the parenteral route, transdermal administration does not carry any risk of infection and overcomes problems related to poor acceptance of needles by the patients [33]. On the other hand, the drawbacks of TDD are linked to skin irritation, difficulties in delivering hydrophilic drugs, delayed absorption, and high costs [34].
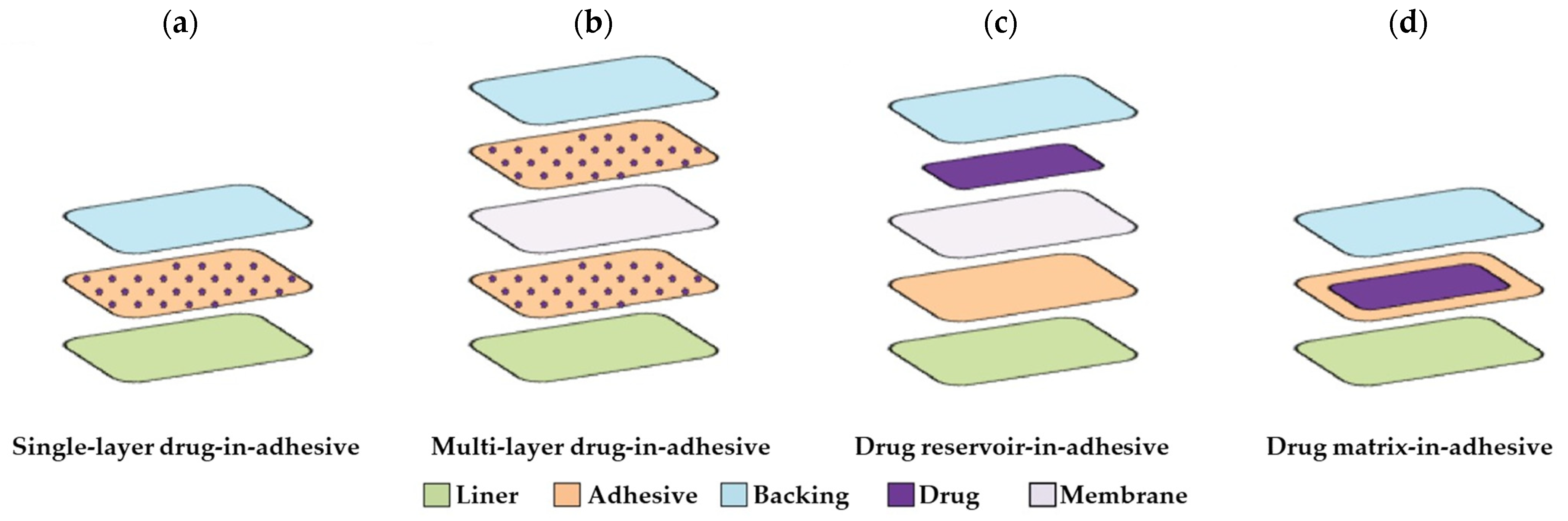
Transdermal patches are constituted of different components [35]: (a) an impermeable backing layer (represented in light blue in Figure 2), constituted of elastomers, which has the aim of protecting the patch from the external environment and confers flexibility to the patch; (b) a membrane (represented in light pink in Figure 2), which controls the drug release; (c) an adhesive part (represented in light orange in Figure 2), which binds the components of the patch together and the patch to the skin; and (d) a liner (in light green in Figure 2), which serves to protect the patch during storage and is removed before application to the skin.
Provided that the backing and the liner constitute the two external layers of the patch, different solutions are obtained depending on how the active ingredient is distributed into the adhesive layer, as represented in Figure 2 [36]. In particular, if the drug is confined directly into the adhesive layer, a drug-in-adhesive system is proposed; when it is dispersed in a unique layer, a “single-layer drug-in-adhesive” (Figure 2a) is prepared, whereas when the drug is dispersed into two adhesive layers parted by a membrane, a “multi-layer drug-in-adhesive” (Figure 2b) is arranged. The latter solution allows the administration of different drugs within the same patch or the possibility of having both an immediate drug release from one of the two layers and a controlled release from the other. In the “drug reservoir-in-adhesive” patch (Figure 2c), the drug is dissolved or dispersed in a liquid phase which, thanks to a semi-permeable membrane, is separated from the adhesive layer. Finally, the drug can be dissolved or dispersed in a hydrophilic or lipophilic polymer matrix, concentric with respect to the adhesive layer, which is positioned between the backing and the liner, forming a “drug matrix-in-adhesive” (Figure 2d).
Other types of transdermal patches based on the use of microneedles have also been proposed [37,38,39]. Such systems are used to administer drugs such as naltrexone [40], lidocaine [41], and insulin [42], but there are no papers involving the administration of opioids.
In the following subsections, the articles dedicated to producing devices containing the most transdermally administered opioids are critically and systematically analyzed. The classification has been made considering the different administered opioids.
2.1. Fentanyl
Fentanyl is an analgesic with a potency of at least 80 times higher than that of morphine, which is widely used as a surgical anesthetic and for the control of chronic pain. Depending on the application, it is administered by intravenous injection, transdermal patches, oral transmucosal tablets, and vestibular tabs. Transdermal administration of fentanyl is associated with ease of dosing and a significantly extended duration of analgesic effect compared to parenteral administration [43]. It is an excellent option for the long-term treatment of cancer pain and chronic non-cancer pain [44]. Moreover, fentanyl’s characteristics, such as high potency, low molecular weight, lipid solubility, and excellent skin flux properties (approximately 1000 times greater than morphine), make it suitable for delivery via the transdermal therapeutic system [45,46]. The first generation of fentanyl-based patches consists of reservoir delivery systems that provide continuous, systemic delivery of fentanyl for 72 h in a constant amount per unit time, while second-generation patches have a matrix-type design. Reservoir systems are constituted of an occlusive backing (polyester/ethylene or polyester film), a drug reservoir (fentanyl base dissolved in ethyl alcohol and gelled with hydroxyethyl cellulose), a rate-controlling membrane (generally constituted of ethylene-vinyl acetate copolymer film) and a silicone adhesive layer. In matrix-designed systems, fentanyl is incorporated directly into the adhesive, which can be constituted by polyacrylate or acrylate vinyl acetate; sometimes, dypropylene glycol droplets are dispersed in a silicone matrix.
In Table 1, a summary of fentanyl-based patches obtained with the different technologies is reported.
In the reservoir systems, patches containing 1.25–10 mg fentanyl are available to provide 12.5–100 µg/h of fentanyl, respectively, for up to three days (72 h). It is, therefore, evident that more than 25% of fentanyl present in the patch is not released. For example, considering the 100 µg/h patch, 7.2 mg of the 10 mg present will have been released after three days [57].
Observing the data inserted in Table 1, it is clear that the matrix systems are the ones mainly used at this point in time. The transition from the first type of patches to the second occurred due to better skin compatibility, adhesive properties, wearability/comfort, and patients’ general satisfaction, which improved significantly with the new matrix technology. Another reason why the second type of patch has supplanted the first is that, in reservoir patches, a significant amount of opioids remain in the patch after removal and, therefore, the patches must be discarded according to opioid disposal guidelines to prevent misuse [58]; in addition, it has been experienced that defects in such patches can cause the patch reservoir to leak onto patients skin and result in overdose [59] and that the gel can be eliminated from the patch and the content unintentionally taken by the patient, leading to a fatal outcome [60]. Conversely, the matrix systems distinctly reduce the risk of drug leakage and abuse. From the point of view of the dimensions of the patch, the matrix patches are thinner (because no reservoir is present) and smaller (for equal strengths, the matrix patch is at least one-third smaller). Considering the pharmacokinetic profiles of reservoir and matrix patches, they are very similar; in Figure 3, the results obtained by Marier et al. indicate that the mean serum concentrations are superimposable [54].
Many papers are devoted to comparing two types of systems from different perspectives. For example, Moore et al. [61] studied the effects of a heating pad on serum fentanyl concentrations with the two types of patches; for both systems, an increase in systemic exposure to fentanyl was observed when a direct external heat source was applied for 10 h; the authors concluded that heat-associated devices, such as saunas, hot tubs, tanning beds, and electric blankets should be avoided during treatment with transdermal fentanyl systems.
Other comparative studies have been published considering different kinds of matrix systems. Zecca et al. [62] proposed a bilayer matrix fentanyl patch compared to a standard monolayer patch to improve the efficiency and reliability of delivery systems. The novel patch provides a constant fentanyl delivery over 72 h.
Considering the results in terms of fentanyl release, it is possible to observe that:
- In the case of reservoir formulations, the drug release rate from the reservoir layer is dependent on the choice of polymer and membrane layer thickness;
- In drug-in-adhesive systems and matrix patches, the control of the drug administered is diffusive, and the amount dispensed is directly proportional to the surface of the patch in contact with the skin.
A recent study by Defraeye et al. [63] aimed to verify the effect of the patient’s age and the site of application of the patch on the amount of the active ingredient absorbed. The adsorption of the drug is strongly related to the different body locations because of different thicknesses of the stratum corneum or the presence of hair follicles. Indeed, the difference in fentanyl uptake between applying the patch on the shoulder and the forearm was 36% after 72 h. To evaluate the impact of the patient’s age on fentanyl uptake kinetics, the authors divided the volunteers by age into six different groups. They observed that the total amount of a drug taken after 72 h differed by 26% between an 18-year-old and a 70-year-old patient, as reported in Figure 4. Furthermore, the time necessary to reach the drug’s minimum effective concentration (MEC) depends on the patient’s age. Considering the 18- and 70-year-old patients, the MEC was reached after 23 h in the former case and after 32 h in the latter.
In any case, fentanyl-based patches must be used with particular caution. For example, the patch has is to be used in association with any heat exposure or in cases of fever [64]. Furthermore, the patches must be applied to intact skin and must not be damaged. Unfortunately, there have been many cases of death in patients taking fentanyl. In some cases, the causes of death have been associated with using the active substance and in others not. Indeed, it is possible that manufacturing defects present in the reservoir patches favor the leakage of the reservoir on the patient’s skin, resulting in an overdose [65].
2.2. Buprenorphine
Buprenorphine is a semisynthetic, low molecular weight, lipophilic opioid analgesic with peculiar pharmacodynamic and pharmacokinetic properties mainly used in patients who require joint administration of various drugs, the elderly, and patients who have renal or hepatic insufficiency [66,67]. It has demonstrated promising efficacy cases of moderate to severe CCP and severe CNCP unresponsive to nonopioid analgesics (for example, in the case of patients with osteoarthritis, low back pain, and other permanent pain syndromes) [68,69]. In some cases, it is preferred to other opioids because the intensity of several classic opioid-related side effects, such as respiratory depression and abuse liability, is reduced [70]. Its therapeutic effect may be correlated to the “binding affinity”, which is the ability of an active principle to bind to a receptor; more molecular interactions between the buprenorphine molecule and μ-opioid receptor are present, leading to an excellent binding affinity (corresponding to a low equilibrium dissociation constant, Ki value) in comparison with that of other opioids [66]. Figure 5 compares the different binding affinities of some of the most prescribed opioids.
As in the case of fentanyl, the use of reservoir systems appears to be overcome. Those systems were applied until the end of the last century; ethanol- or aqueous-based reservoirs produced sustained plasma levels of buprenorphine [71]. Buprenorphine transdermal patches (BTPs) are preferably applied to the upper outer arm, upper back, sub clavicular region, or chest; they are, in general, better tolerated than transdermal fentanyl, as evidenced by a reduced need for dosage increases [72]. Different from fentanyl transdermal patches that are always worn for 72 h, BTPs can be applied (a) for 3–4 days, considering a dosage equal to 35, 52.5, and 70 μg/h [73] or (b) for more days at lower doses (5–20 μg/h) [74]. For both cases, a rotation of the application site is recommended, and a new patch must be applied to a different skin site for the following 3 or 4 weeks. Likar et al. [75] compared two durations of buprenorphine patch wearing in terms of analgesic efficacy and skin tolerability, a transdermal patch containing a buprenorphine dose of 50 μg/h in a 4-day regimen vs. a standard 3-day regimen. The tests were performed on 49 white patients of both sexes, which asserted that the quality of treatment did not differ significantly between regimens.
Patches containing a low dose of buprenorphine are commonly used in postoperative pain management or in the case of clinically diagnosed osteoarthritis or rheumatoid arthritis or for less invasive pathologies such as low back pain and joint/muscle pain. Mythili et al. [76] proposed using 10 μg/h patches in the management of postoperative pain in oral and maxillofacial surgery, including in the study of 100 people of both sexes in the age group of 18–60 years. The patches were effective because buprenorphine showed high analgesic potential and was well tolerated by the patients. Breivik et al. [77] tested low-dose (5–20 μg/h) BTPs in elderly patients with pain due to osteoarthritis. The selected patients had opioid-sensitive pain and were unable to undergo surgery. In addition, the administration of paracetamol was ineffective, and NSAIDs were not recommended. Tests were performed with 200 patients of both sexes: 100 of them were treated with 7-day BTPs and 100 with placebo patches. The patients’ global impression in terms of pain reduction after a 6-month treatment period was significantly better in patients treated with BTPs than in the patients treated with a placebo. Yoon et al. [78] evaluated the effectiveness and tolerability of 5–20 μg/h BTPs in Asian patients with moderate to severe chronic musculoskeletal non-malignant pain. Treatment with BTPs resulted in effective and sustained pain relief and improved daily functioning and quality of life.
Apart from transdermal patches, Buprenorphine is sometimes administered via buccal films or tablets. Compared with the oral route, the transdermal administration avoids losses in bioavailability due to first-pass hepatic metabolism [79]. James et al. [80] compared the efficacy and tolerability of 7-day low-dose buprenorphine transdermal patches (BTPs) with buprenorphine sublingual tablets to treat osteoarthritis pain. Tests were performed on 110 patients, and the authors concluded that low-dose BTPs are as effective as sublingual buprenorphine, with a better tolerability profile. Low-dose BTPs were compared to tablets containing other opioids, such as tramadol. For example, Karlsson et al. [81] compared 5, 10, and 20 μg/h 7-day BTPs with prolonged-release of 75, 100, 150, and 200 mg tramadol tablets in patients affected by chronic osteoarthritis pain (at a level from moderate to severe). The efficacy of BTPs was non-inferior to that of tramadol tablets, and the incidence of adverse effects was similar in the two therapy groups. Consequently, most patients reported that, in case of future treatment, they would prefer the 7-day transdermal patch to the twice-daily tablet. Similar conclusions were drawn when comparing the efficacy of the same type of BTP (7-day 5–20 μg/h) with higher doses (150–300 mg) of prolonged-release tramadol tablets for the treatment of postoperative pain after single-level spinal fusion surgery [82]. Plosker and Lyseng-Williamson [83], in a review paper, analyzed the analgesic efficacy of low-dose BTPs, observing that they are equivalent to sublingual buprenorphine, non-inferior to prolonged-release tramadol, and generally superior to a matching transdermal placebo patch.
3. Conclusions and Perspectives
This review focused on using transdermal patches containing opioids (fentanyl and buprenorphine) to treat chronic cancer and non-cancer pain. The different kinds of patches can be classified into two main categories: reservoir and matrix systems. The second one has replaced the first kind of patch, as it has better skin compatibility, adhesive properties, and wearability/comfort, coupled with the identical pharmacokinetics of the active ingredient. Furthermore, in the matrix system patches, the active ingredient is almost wholly released so that no abuse phenomena have been observed in using the device; instead, abuse phenomena have been frequently noted using the reservoir systems.
This review also focused on comparing patches containing fentanyl and those containing buprenorphine, underscoring for both the priority areas of use, advantages, and disadvantages. Without a doubt, the challenges to be faced in the field of drug administration are many. The challenges include having to improve the bioavailability of poorly water-soluble drugs to having to control the release of some active ingredients. Regarding transdermal administration, research should focus on developing patches to be applied as infrequently as possible. In this way, the patient could have an important psychological advantage with the same pain-relieving effect. An interesting way to pursue this could be to couple the opioid with another active ingredient, such as a different type of analgesic or a drug that assists the therapy the patient is following.
Funding
This research received no external funding.
Data Availability Statement
Not applicable.
Conflicts of Interest
The author declares no conflict of interest.
References
- Raja, S.N.; Carr, D.B.; Cohen, M.; Finnerup, N.B.; Flor, H.; Gibson, S.; Keefe, F.J.; Mogil, J.S.; Ringkamp, M.; Sluka, K.A.; et al. The revised International Association for the Study of Pain definition of pain: Concepts, challenges, and compromises. Pain 2020, 161, 1976–1982. [Google Scholar] [CrossRef] [PubMed]
- Leppert, W.; Malec-Milewska, M.; Zajaczkowska, R.; Wordliczek, J. Transdermal and Topical Drug Administration in the Treatment of Pain. Molecules 2018, 23, 681. [Google Scholar] [PubMed]
- Bussières, A.E.; Stewart, G.; Al-Zoubi, F.; Decina, P.; Descarreaux, M.; Hayden, J.; Hendrickson, B.; Hincapié, C.; Pagé, I.; Passmore, S.; et al. The Treatment of Neck Pain-Associated Disorders and Whiplash-Associated Disorders: A Clinical Practice Guideline. J. Manip. Physiol. Ther. 2016, 39, 523–564.e527. [Google Scholar] [CrossRef]
- Banerjee, S.; Argáez, C. Multidisciplinary Treatment Programs for Patients with Acute or Subacute Pain: A Review of Clinical Effectiveness, Cost-Effectiveness, and Guidelines. Ottawa (ON): Canadian Agency for Drugs and Technologies in Health. Available online: https://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/books/NBK546002/ (accessed on 7 May 2023).
- Fitzcharles, M.A.; Cohen, S.P.; Clauw, D.J.; Littlejohn, G.; Usui, C.; Häuser, W. Nociplastic pain: Towards an understanding of prevalent pain conditions. Lancet 2021, 397, 2098–2110. [Google Scholar] [CrossRef] [PubMed]
- Devers, A.; Galer, B.S. Topical Lidocaine Patch Relieves a Variety of Neuropathic Pain Conditions: An Open-Label Study. Clin. J. Pain 2000, 16, 205–208. [Google Scholar] [CrossRef]
- Cohen, S.P.; Vase, L.; Hooten, W.M. Chronic pain: An update on burden, best practices, and new advances. Lancet 2021, 397, 2082–2097. [Google Scholar] [CrossRef]
- Ripamonti, C.I.; Bandieri, E.; Roila, F. Management of cancer pain: ESMO clinical practice guidelines. Ann. Oncol. 2011, 22, vi69–vi77. [Google Scholar] [CrossRef]
- Ventafridda, V.; Saita, L.; Ripamonti, C.; De Conno, F. WHO guidelines for the use of analgesics in cancer pain. Int. J. Tissue React. 1985, 7, 93–96. [Google Scholar]
- Carr, D.B.; Goudas, L.C. Acute pain. Lancet 1999, 353, 2051–2058. [Google Scholar] [CrossRef]
- Franco, P.; De Marco, I. Supercritical CO2 adsorption of non-steroidal anti-inflammatory drugs into biopolymer aerogels. J. CO2 Util. 2020, 36, 40–53. [Google Scholar] [CrossRef]
- Upton, R.N.; Semple, T.J.; Macintyre, P.E. Pharmacokinetic Optimisation of Opioid Treatment in Acute Pain Therapy. Clin. Pharmacokinet. 1997, 33, 225–244. [Google Scholar] [CrossRef] [PubMed]
- Gordon, D.B.; Dahl, J.; Phillips, P.; Frandsen, J.; Cowley, C.; Foster, R.L.; Fine, P.G.; Miaskowski, C.; Fishman, S.; Finley, R.S. The use of “as-needed” range orders for opioid analgesics in the management of acute pain: A consensus statement of the American Society for Pain Management Nursing and the American Pain Society. Pain Manag. Nurs. 2004, 5, 53–58. [Google Scholar] [CrossRef] [PubMed]
- Walder, B.; Schafer, M.; Henzi, I.; Tramer, M. Efficacy and safety of patient-controlled opioid analgesia for acute postoperative pain: A quantitative systematic review. Acta Anaesthesiol. Scand. 2001, 45, 795–804. [Google Scholar] [CrossRef] [PubMed]
- Furlan, A.D.; Sandoval, J.A.; Mailis-Gagnon, A.; Tunks, E. Opioids for chronic noncancer pain: A meta-analysis of effectiveness and side effects. CMAJ 2006, 174, 1589–1594. [Google Scholar] [CrossRef]
- Sarzi-Puttini, P.; Vellucci, R.; Zuccaro, S.M.; Cherubino, P.; Labianca, R.; Fornasari, D. The appropriate treatment of chronic pain. Clin. Drug Investig. 2012, 32, 21–33. [Google Scholar] [CrossRef]
- McCleane, G.J. Pain Management: Expanding the Pharmacological Options; Wiley-Blackwell: Hoboken, NJ, USA, 2009; pp. 1–192. ISBN 978140517823. [Google Scholar] [CrossRef]
- Manchikanti, L.; Singh, V.; Caraway, D.L.; Benyamin, R.M. Breakthrough pain in chronic non-cancer pain: Fact, fiction, or abuse. Pain Phys. 2011, 14, E103–E117. [Google Scholar] [CrossRef]
- Leonardi, C.; Vellucci, R.; Mammucari, M.; Fanelli, G. Opioid risk addiction in the management of chronic pain in primary care: The addition risk questionnaire. Eur. Rev. Med. Pharmacol. Sci. 2015, 19, 4898–4905. [Google Scholar]
- Fallon, M.; Giusti, R.; Aielli, F.; Hoskin, P.; Rolke, R.; Sharma, M.; Ripamonti, C.I. Management of cancer pain in adult patients: ESMO Clinical Practice Guidelines. Ann. Oncol. 2018, 29, iv166–iv191. [Google Scholar] [CrossRef]
- Volkow, N.; Benveniste, H.; McLellan, A.T. Use and Misuse of Opioids in Chronic Pain. In Annual Review of Medicine; Annual Reviews Inc.: San Mateo, CA, USA, 2018; Volume 69, pp. 451–465. [Google Scholar]
- Latina, R.; Varrassi, G.; Di Biagio, E.; Giannarelli, D.; Gravante, F.; Paladini, A.; D’Angelo, D.; Iacorossi, L.; Martella, C.; Alvaro, R.; et al. Chronic Non-cancer Pain Management in a Tertiary Pain Clinic Network: A Retrospective Study. Pain Ther. 2023, 12, 151–164. [Google Scholar] [CrossRef]
- Alkilani, A.Z.; McCrudden, M.T.; Donnelly, R.F. Transdermal Drug Delivery: Innovative Pharmaceutical Developments Based on Disruption of the Barrier Properties of the stratum corneum. Pharmaceutics 2015, 7, 438–470. [Google Scholar] [CrossRef]
- Schoellhammer, C.M.; Blankschtein, D.; Langer, R. Skin permeabilization for transdermal drug delivery: Recent advances and future prospects. Expert Opin. Drug Deliv. 2014, 11, 393–407. [Google Scholar] [CrossRef] [PubMed]
- Mathews, L.M.; Roy, A. Management of pain using transdermal patches—A review. Asian J. Pharm. Clin. Res. 2016, 9, 32–35. [Google Scholar] [CrossRef]
- Ciurba, A.; Antonoaea, P.; Todoran, N.; Rédai, E.; Vlad, R.A.; Tătaru, A.; Muntean, D.L.; Bîrsan, M. Polymeric films containing tenoxicam as prospective transdermal drug delivery systems: Design and characterization. Processes 2021, 9, 136. [Google Scholar] [CrossRef]
- Tsai, J.H.; Liu, I.T.; Su, P.F.; Huang, Y.T.; Chiu, G.L.; Chen, Y.Y.; Lai, W.S.; Lin, P.C. Lidocaine transdermal patches reduced pain intensity in neuropathic cancer patients already receiving opioid treatment. BMC Palliat. Care 2023, 22, 4. [Google Scholar] [CrossRef] [PubMed]
- Franco, P.; Pessolano, E.; Belvedere, R.; Petrella, A.; De Marco, I. Supercritical impregnation of mesoglycan into calcium alginate aerogel for wound healing. J. Supercrit. Fluids 2020, 157, 104711. [Google Scholar] [CrossRef]
- Belvedere, R.; Novizio, N.; Morello, S.; Petrella, A. The combination of mesoglycan and VEGF promotes skin wound repair by enhancing the activation of endothelial cells and fibroblasts and their cross-talk. Sci. Rep. 2022, 12, 11041. [Google Scholar] [CrossRef]
- Khandaker, M.; Alkadhem, N.; Progri, H.; Nikfarjam, S.; Jeon, J.; Kotturi, H.; Vaughan, M.B. Glutathione Immobilized Polycaprolactone Nanofiber Mesh as a Dermal Drug Delivery Mechanism for Wound Healing in a Diabetic Patient. Processes 2022, 10, 512. [Google Scholar] [CrossRef]
- Tyeb, S.; Verma, V.; Kumar, N. Polysaccharide based transdermal patches for chronic wound healing: Recent advances and clinical perspective. Carbohydr. Polym. 2023, 316, 121038. [Google Scholar] [CrossRef]
- Jeong, W.Y.; Kwon, M.; Choi, H.E.; Kim, K.S. Recent advances in transdermal drug delivery systems: A review. Biomater. Res. 2021, 25, 24. [Google Scholar] [CrossRef]
- Kaestli, L.Z.; Wasilewski-Rasca, A.F.; Bonnabry, P.; Vogt-Ferrier, N. Use of transdermal drug formulations in the elderly. Drugs Aging 2008, 25, 269–280. [Google Scholar] [CrossRef]
- Tanner, T.; Marks, R. Delivering drugs by the transdermal route: Review and comment. Ski Res. Technol. 2008, 14, 249–260. [Google Scholar] [CrossRef] [PubMed]
- Bird, D.; Ravindra, N.M. Transdermal drug delivery and patches—An overview. Med. Devices Sens. 2020, 3, e10069. [Google Scholar] [CrossRef]
- Sozio, P.; Cerasa, L.S.; Marinelli, L.; Di Stefano, A. Transdermal donepezil on the treatment of Alzheimer’s disease. Neuropsychiatr. Dis. Treat. 2012, 8, 361–368. [Google Scholar] [CrossRef] [PubMed]
- He, J.; Zhang, Y.; Yu, X.; Xu, C. Wearable patches for transdermal drug delivery. Acta Pharm. Sin. B 2023, 13, 2298–2309. [Google Scholar] [CrossRef] [PubMed]
- McKenna, P.E.; Abbate, M.T.A.; Vora, L.K.; Sabri, A.H.; Peng, K.; Volpe-Zanutto, F.; Tekko, I.A.; Permana, A.D.; Maguire, C.; Dineen, D.; et al. Polymeric Microarray Patches for Enhanced Transdermal Delivery of the Poorly Soluble Drug Olanzapine. ACS Appl. Mater. Interfaces 2023, 15, 31300–31319. [Google Scholar] [CrossRef]
- Naser, Y.A.; Tekko, I.A.; Vora, L.K.; Peng, K.; Anjani, Q.K.; Greer, B.; Elliott, C.; McCarthy, H.O.; Donnelly, R.F. Hydrogel-forming microarray patches with solid dispersion reservoirs for transdermal long-acting microdepot delivery of a hydrophobic drug. J. Control. Release 2023, 356, 416–433. [Google Scholar] [CrossRef]
- Wermeling, D.P.; Banks, S.L.; Hudson, D.A.; Gill, H.S.; Gupta, J.; Prausnitz, M.R.; Stinchcomb, A.L. Microneedles permit transdermal delivery of a skin-impermeant medication to humans. Proc. Natl. Acad. Sci. USA 2008, 105, 2058–2063. [Google Scholar] [CrossRef]
- Kochhar, J.S.; Lim, W.X.S.; Zou, S.; Foo, W.Y.; Pan, J.; Kang, L. Microneedle integrated transdermal patch for fast onset and sustained delivery of lidocaine. Mol. Pharm. 2013, 10, 4272–4280. [Google Scholar] [CrossRef]
- Gupta, J.; Felner, E.I.; Prausnitz, M.R. Rapid pharmacokinetics of intradermal insulin administered using microneedles in type 1 diabetes subjects. Diabetes Technol. Ther. 2011, 13, 451–456. [Google Scholar] [CrossRef]
- Freynhagen, R.; Von Giesen, H.J.; Busche, P.; Sabatowski, R.; Konrad, C.; Grond, S. Switching from reservoir to matrix systems for the transdermal delivery of fentanyl: A prospective, multicenter pilot study in outpatients with chronic pain. J. Pain Symptom Manag. 2005, 30, 289–297. [Google Scholar] [CrossRef]
- Grape, S.; Schug, S.A.; Lauer, S.; Schug, B.S. Formulations of fentanyl for the management of pain. Drugs 2010, 70, 57–72. [Google Scholar] [CrossRef] [PubMed]
- Jeal, W.; Benfield, P. Transdermal fentanyl—A review of its pharmacological properties and therapeutic efficacy in pain control. Drugs 1997, 53, 109–138. [Google Scholar] [CrossRef]
- Roy, S.D.; Flynn, G.L. Transdermal Delivery of Narcotic Analgesics: pH, Anatomical, and Subject Influences on Cutaneous Permeability of Fentanyl and Sufentanil. Pharm. Res. Off. J. Am. Assoc. Pharm. Sci. 1990, 7, 842–847. [Google Scholar] [CrossRef]
- Gupta, S.K.; Southam, M.; Gale, R.; Hwang, S.S. System functionality and physicochemical model of fentanyl transdermal system. J. Pain Symptom Manag. 1992, 7, S17–S26. [Google Scholar] [CrossRef] [PubMed]
- Takashina, Y.; Naito, T.; Mino, Y.; Yagi, T.; Ohnishi, K.; Kawakami, J. Impact of CYP3A5 and ABCB1 gene polymorphisms on fentanyl pharmacokinetics and clinical responses in cancer patients undergoing conversion to a transdermal system. Drug Metab. Pharmacokinet. 2012, 27, 414–421. [Google Scholar] [CrossRef]
- Prodduturi, S.; Smith, G.J.; Wokovich, A.M.; Doub, W.H.; Westenberger, B.J.; Buhse, L. Reservoir based fentanyl transdermal drug delivery systems: Effect of patch age on drug release and skin permeation. Pharm. Res. 2009, 26, 1344–1352. [Google Scholar] [CrossRef]
- Kim, T.S.; Jin, S.E.; Sun, B.; Kim, M.S.; Hwang, S.J. Comparison of adhesion and dissolution of fentanyl patches: Fentadur® and Durogesic DTrans®. J. Pharm. Investig. 2015, 45, 475–480. [Google Scholar] [CrossRef]
- Miyazaki, T.; Hanaoka, K.; Namiki, A.; Ogawa, S.; Kitajima, T.; Hosokawa, T.; Ishida, T.; Nogami, S.; Mashimo, S. Efficacy, safety and pharmacokinetic study of a novel fentanyl-containing matrix transdermal patch system in Japanese patients with cancer pain. Clin. Drug Investig. 2008, 28, 313–325. [Google Scholar] [CrossRef]
- Prodduturi, S.; Sadrieh, N.; Wokovich, A.M.; Doub, W.H.; Westenberger, B.J.; Buhse, L. Transdermal delivery of fentanyl from matrix and reservoir systems: Effect of heat and compromised skin. J. Pharm. Sci. 2010, 99, 2357–2366. [Google Scholar] [CrossRef]
- Marier, J.F.; Lor, M.; Morin, J.; Roux, L.; Di Marco, M.; Morelli, G.; Sædder, E.A. Comparative bioequivalence study between a novel matrix transdermal delivery system of fentanyl and a commercially available reservoir formulation. Br. J. Clin. Pharmacol. 2007, 63, 121–124. [Google Scholar] [CrossRef]
- Marier, J.F.; Lor, M.; Potvin, D.; DiMarco, M.; Morelli, G.; Sædder, E.A. Pharmacokinetics, tolerability, and performance of a novel matrix transdermal delivery system of fentanyl relative to the commercially available reservoir formulation in healthy subjects. J. Clin. Pharmacol. 2006, 46, 642–653. [Google Scholar] [CrossRef] [PubMed]
- Hoy, S.M.; Keating, G.M. Fentanyl Transdermal Matrix Patch (Durotep® MT Patch; Durogesic® DTrans®; Durogesic® SMAT). Drugs 2008, 68, 1711–1721. [Google Scholar] [CrossRef] [PubMed]
- Hair, P.I.; Keating, G.M.; McKeage, K. Transdermal matrix fentanyl membrane patch (Matrifen®): In severe cancer-related chronic pain. Drugs 2008, 68, 2001–2009. [Google Scholar] [CrossRef] [PubMed]
- Lane, M.E. The transdermal delivery of fentanyl. Eur. J. Pharm. Biopharm. 2013, 84, 449–455. [Google Scholar] [CrossRef]
- Marquardt, K.A.; Tharratt, R.S.; Musallam, N.A. Fentanyl remaining in a transdermal system following three days of continuous use. Ann. Pharmacother. 1995, 29, 969–971. [Google Scholar] [CrossRef]
- Oliveira, G.; Hadgraft, J.; Lane, M.E. Toxicological implications of the delivery of fentanyl from gel extracted from a commercial transdermal reservoir patch. Toxicol. In Vitro 2012, 26, 645–648. [Google Scholar] [CrossRef]
- Kuhlman, J.J., Jr.; McCaulley, R.; Valouch, T.J.; Behonick, G.S. Fentanyl use, misuse, and abuse: A summary of 23 postmortem cases. J. Anal. Toxicol. 2003, 27, 499–504. [Google Scholar] [CrossRef] [PubMed]
- Moore, K.T.; Sathyan, G.; Richarz, U.; Natarajan, J.; Vandenbossche, J. Randomized 5-treatment crossover study to assess the effects of external heat on serum fentanyl concentrations during treatment with transdermal fentanyl systems. J. Clin. Pharmacol. 2012, 52, 1174–1185. [Google Scholar] [CrossRef]
- Zecca, E.; Manzoni, A.; Centurioni, F.; Farina, A.; Bonizzoni, E.; Seiler, D.; Perrone, T.; Caraceni, A. Pharmacokinetic study between a bilayer matrix fentalyl patch and a monolayer matrix fentanyl patch: Single dose administration in healthy volunteers. Br. J. Clin. Pharmacol. 2015, 80, 110–115. [Google Scholar] [CrossRef]
- Defraeye, T.; Bahrami, F.; Ding, L.; Malini, R.I.; Terrier, A.; Rossi, R.M. Predicting Transdermal Fentanyl Delivery Using Mechanistic Simulations for Tailored Therapy. Front. Pharmacol. 2020, 11, 585393. [Google Scholar] [CrossRef]
- Shomaker, T.S.; Zhang, J.; Ashburn, M.A. Assessing the impact of heat on the systemic delivery of fentanyl through the transdermal fentanyl delivery system. Pain Med. 2000, 1, 225–230. [Google Scholar] [CrossRef]
- Luckenbill, K.; Thompson, J.; Middleton, O.; Kloss, J.; Apple, F. Fentanyl postmortem redistribution: Preliminary findings regarding the relationship among femoral blood and liver and heart tissue concentrations. J. Anal. Toxicol. 2008, 32, 639–643. [Google Scholar] [CrossRef] [PubMed]
- Gudin, J.; Fudin, J. A Narrative Pharmacological Review of Buprenorphine: A Unique Opioid for the Treatment of Chronic Pain. Pain Ther. 2020, 9, 41–54. [Google Scholar] [CrossRef] [PubMed]
- Al-Tawil, N.; Odar-Cederlöf, I.; Berggren, A.C.; Johnson, H.E.; Persson, J. Pharmacokinetics of transdermal buprenorphine patch in the elderly. Eur. J. Clin. Pharmacol. 2013, 69, 143–149. [Google Scholar] [CrossRef]
- Plosker, G.L. Buprenorphine 5, 10 and 20 μg/h Transdermal Patch. Drugs 2011, 71, 2491–2509. [Google Scholar] [CrossRef]
- Böhme, K. Buprenorphine in a transdermal therapeutic system—A new option. Clin. Rheumatol. 2002, 21, S13–S16. [Google Scholar] [CrossRef] [PubMed]
- Ehrlich, A.T.; Darcq, E. Recommending buprenorphine for pain management. Pain Manag. 2019, 9, 13–16. [Google Scholar] [CrossRef]
- Wilding, I.R.; Davis, S.S.; Rimoy, G.H.; Rubin, P.; Kurihara-Bergstrom, T.; Tipnis, V.; Berner, B.; Nightingale, J. Pharmacokinetic evaluation of transdermal buprenorphine in man. Int. J. Pharm. 1996, 132, 81–87. [Google Scholar] [CrossRef]
- Sittl, R.; Nuijten, M.; Nautrup, B.P. Changes in the prescribed daily doses of transdermal fentanyl and transdermal buprenorphine during treatment of patients with cancer and noncancer pain in Germany: Results of a retrospective cohort study. Clin. Ther. 2005, 27, 1022–1031. [Google Scholar] [CrossRef]
- Ahn, J.S.; Lin, J.; Ogawa, S.; Yuan, C.; O’Brien, T.; Le, B.H.; Bothwell, A.M.; Moon, H.; Hadjiat, Y.; Ganapathi, A. Transdermal buprenorphine and fentanyl patches in cancer pain: A network systematic review. J. Pain Res. 2017, 10, 1963–1972. [Google Scholar] [CrossRef]
- Evans, H.C.; Easthope, S.E. Transdermal buprenorphine. Drugs 2003, 63, 1999–2010. [Google Scholar] [CrossRef] [PubMed]
- Likar, R.; Lorenz, V.; Korak-Leiter, M.; Kager, I.; Sittl, R. Transdermal Buprenorphine Patches Applied in a 4-Day Regimen Versus a 3-Day Regimen: A Single-Site, Phase III, Randomized, Open-Label, Crossover Comparison. Clin. Ther. 2007, 29, 1591–1606. [Google Scholar] [CrossRef] [PubMed]
- Mythili, N.; Navaneetham, R.; Sham, M.E.; Menon, S.; Kumar, V.; Archana, S. Efficacy of Transdermal Buprenorphine Patch in Postoperative Pain Management in Oral and Maxillofacial Surgery. J. Maxillofac. Oral Surg. 2022, 1–6. [Google Scholar] [CrossRef]
- Breivik, H.; Ljosaa, T.M.; Stengaard-Pedersen, K.; Persson, J.; Aro, H.; Villumsen, J.; Tvinnemose, D. A 6-months, randomised, placebo-controlled evaluation of efficacy and tolerability of a low-dose 7-day buprenorphine transdermal patch in osteoarthritis patients naïve to potent opioids. Scand. J. Pain 2010, 1, 122–141. [Google Scholar] [CrossRef] [PubMed]
- Yoon, D.H.; Bin, S.-I.; Chan, S.K.-C.; Chung, C.K.; In, Y.; Kim, H.; Lichauco, J.J.; Mok, C.C.; Moon, Y.-W.; Ng, T.K.-T.; et al. Effectiveness and tolerability of transdermal buprenorphine patches: A multicenter, prospective, open-label study in Asian patients with moderate to severe chronic musculoskeletal pain. BMC Musculoskelet. Disord. 2017, 18, 337. [Google Scholar] [CrossRef]
- Brown, L.; Langer, R. Transdermal delivery of drugs. Annu. Rev. Med. 1988, 39, 221–229. [Google Scholar] [CrossRef]
- James, I.G.; O’Brien, C.M.; McDonald, C.J. A randomized, double-blind, double-dummy comparison of the efficacy and tolerability of low-dose transdermal buprenorphine (BuTrans seven-day patches) with buprenorphine sublingual tablets (Temgesic) in patients with osteoarthritis pain. J. Pain Symptom Manag. 2010, 40, 266–278. [Google Scholar] [CrossRef]
- Karlsson, M.; Berggren, A.C. Efficacy and safety of low-dose transdermal buprenorphine patches (5, 10, and 20 microg/h) versus prolonged-release tramadol tablets (75, 100, 150, and 200 mg) in patients with chronic osteoarthritis pain: A 12-week, randomized, open-label, controlled, parallel-group noninferiority study. Clin. Ther. 2009, 31, 503–513. [Google Scholar] [CrossRef]
- Kim, H.J.; Ahn, H.S.; Nam, Y.; Chang, B.S.; Lee, C.K.; Yeom, J.S. Comparative study of the efficacy of transdermal buprenorphine patches and prolonged-release tramadol tablets for postoperative pain control after spinal fusion surgery: A prospective, randomized controlled non-inferiority trial. Eur. Spine J. 2017, 26, 2961–2968. [Google Scholar] [CrossRef]
- Plosker, G.L.; Lyseng-Williamson, K.A. Buprenorphine 5, 10 and 20 μg/h transdermal patch: A guide to its use in chronic non-malignant pain. CNS Drugs 2012, 26, 367–373. [Google Scholar] [CrossRef]
Figure 1.
Adapted WHO three-step analgesic ladder.

Figure 2.
Different types of transdermal delivery patches. (a) single-layer drug-in-adhesive; (b) multi-layer drug-in-adhesive; (c) drug reservoir-in-adhesive; (d) drug matrix-in-adhesive. Adapted from [36].
Figure 2.
Different types of transdermal delivery patches. (a) single-layer drug-in-adhesive; (b) multi-layer drug-in-adhesive; (c) drug reservoir-in-adhesive; (d) drug matrix-in-adhesive. Adapted from [36].

Figure 3.
Mean serum concentration profiles of fentanyl after 72 h application of the reservoir and novel matrix systems (50 μg/h). Adapted with permission from [54]. Copyright © 2006 John Wiley and Sons.
Figure 3.
Mean serum concentration profiles of fentanyl after 72 h application of the reservoir and novel matrix systems (50 μg/h). Adapted with permission from [54]. Copyright © 2006 John Wiley and Sons.

Figure 4.
Cumulative amount of fentanyl taken up in the blood as a function of time for different age categories. Adapted from [63]. Copyright © 2020 Frontiers in Pharmacology.
Figure 4.
Cumulative amount of fentanyl taken up in the blood as a function of time for different age categories. Adapted from [63]. Copyright © 2020 Frontiers in Pharmacology.

Figure 5.
Binding affinity for different opioids. Adapted from [66]. Copyright © 2020 Pain and Therapy, Springer Link.
Figure 5.
Binding affinity for different opioids. Adapted from [66]. Copyright © 2020 Pain and Therapy, Springer Link.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
Transdermal patches containing fentanyl.
| Type of Patch | Amount of Drug [μg/h] | Main Results | Reference |
|---|---|---|---|
| Reservoir | 25–100 | Comparison with fentanyl infusion; the drug half-life after patch removal was significantly longer than the half-life after infusion | [47] |
| 25–50 | Use of Durotep® commercial patches on 60 Japanese cancer patients that previously used oral morphine or oxycodone; evaluation of the influence of two biomarkers on fentanyl pharmacokinetics | [48] | |
| 25 | Use of Duragesic® commercial patches to evaluate stability and skin permeation profiles as a function of the age of the patch | [49] | |
| Matrix | 12–100 | Comparison with a reservoir system; tests on 46 patients with CCP and CNCP; 91% of patients preferred the matrix system | [43] |
| 12–100 | Comparison between Fentadur®, a reservoir system, and Durogesic Dtrans®, a matrix system, in terms of adhesion and dissolution properties; both were acceptable for skin attachment, although higher adhesion forces were expressed by the matrix system; from the point of view of the dissolution study, the release of the reservoir system was lower than that of the matrix system. | [50] | |
| 12.5 | Comparison with Durotep®, a commercial reservoir system; tests on 87 patients of both sexes with a confirmed diagnosis of cancer; successful replacement of morphine, oral oxycodone, or fentanyl injection formulations | [51] | |
| 25 | Comparison with Duragesic® commercial patches to evaluate the effect of elevated temperatures and compromised skin on drug release and skin permeation; the patches are comparable when applied to intact skin at normal skin temperature, whereas, in the case of compromised skin, the matrix patch has a more significant permeation enhancement effect than the reservoir system | [52] | |
| 50 | Comparison with Durogesic®, a commercial reservoir system; adherence and skin irritability results were similar, but the matrix formulation is more convenient because of the smaller size | [53] | |
| 50 | Comparison with a reservoir system; tests on 24 male patients; enhanced adherence compared to the reservoir formulation; constant fentanyl delivery rate over three days | [54] | |
| 12.5–50 | Use of Durotep® MT patch, Durogesic® Dtrans®, and Durogesic® SMAT commercial patches; comparison with a reservoir system; patients preferred the transdermal matrix patch over the transdermal reservoir patch | [55] | |
| 12–300 | Equivalent to a reservoir system in terms of TDD and analgesic efficacy in patients with CCP | [56] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
De Marco, I. Transdermal Patches Containing Opioids in the Treatment of Patients with Chronic Pain. Processes 2023, 11, 2673. https://0-doi-org.brum.beds.ac.uk/10.3390/pr11092673
AMA Style
De Marco I. Transdermal Patches Containing Opioids in the Treatment of Patients with Chronic Pain. Processes. 2023; 11(9):2673. https://0-doi-org.brum.beds.ac.uk/10.3390/pr11092673
Chicago/Turabian StyleDe Marco, Iolanda. 2023. "Transdermal Patches Containing Opioids in the Treatment of Patients with Chronic Pain" Processes 11, no. 9: 2673. https://0-doi-org.brum.beds.ac.uk/10.3390/pr11092673
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.