Computational Fluid Dynamic Analysis of the Pharyngeal Airway after Bimaxillary Orthognathic Surgery in Patients with Mandibular Prognathism


Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
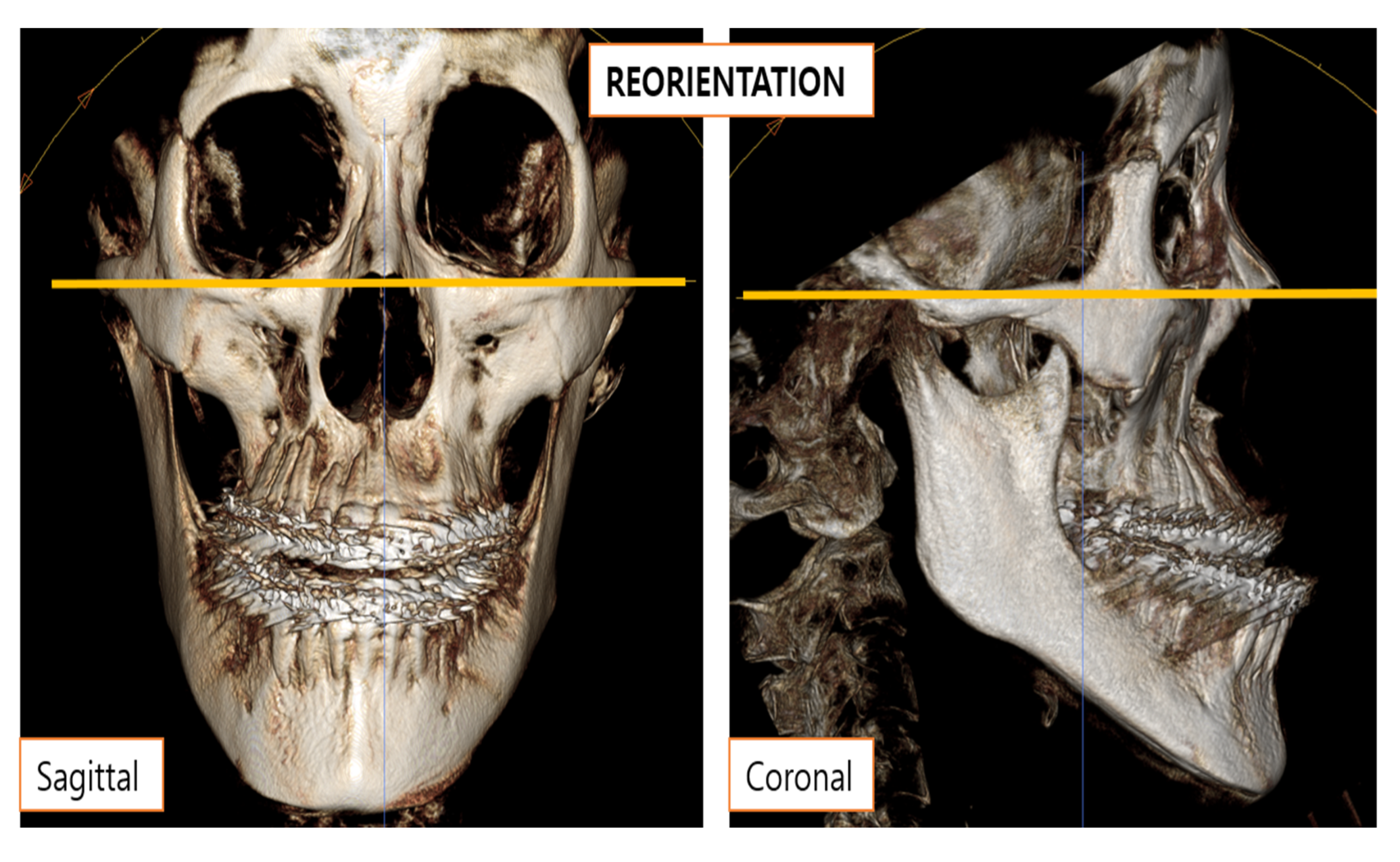
2.2. Skeletal Measurements
2.3. Reconstruction of the Model and Mesh Generation
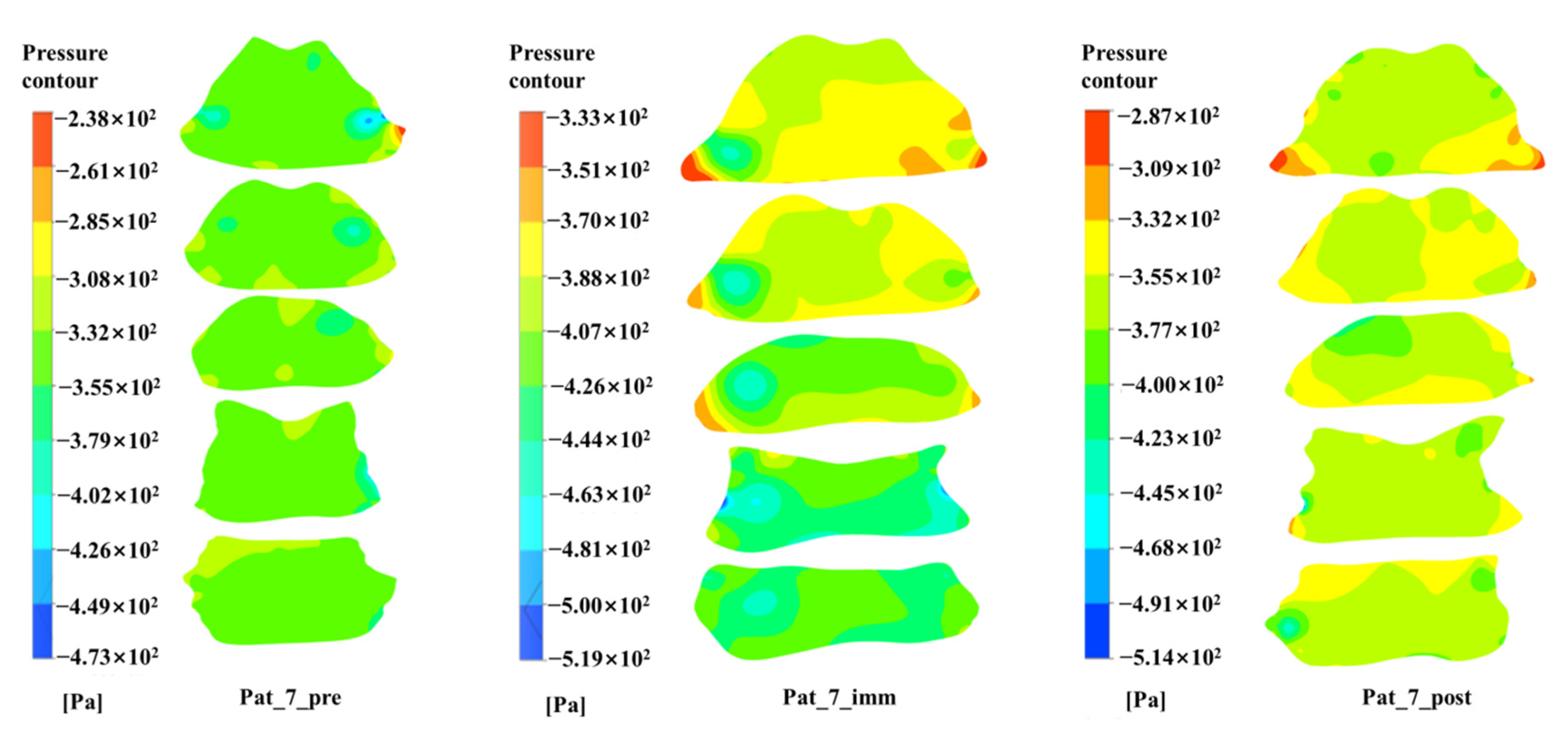
2.4. Computational Fluid Dynamics
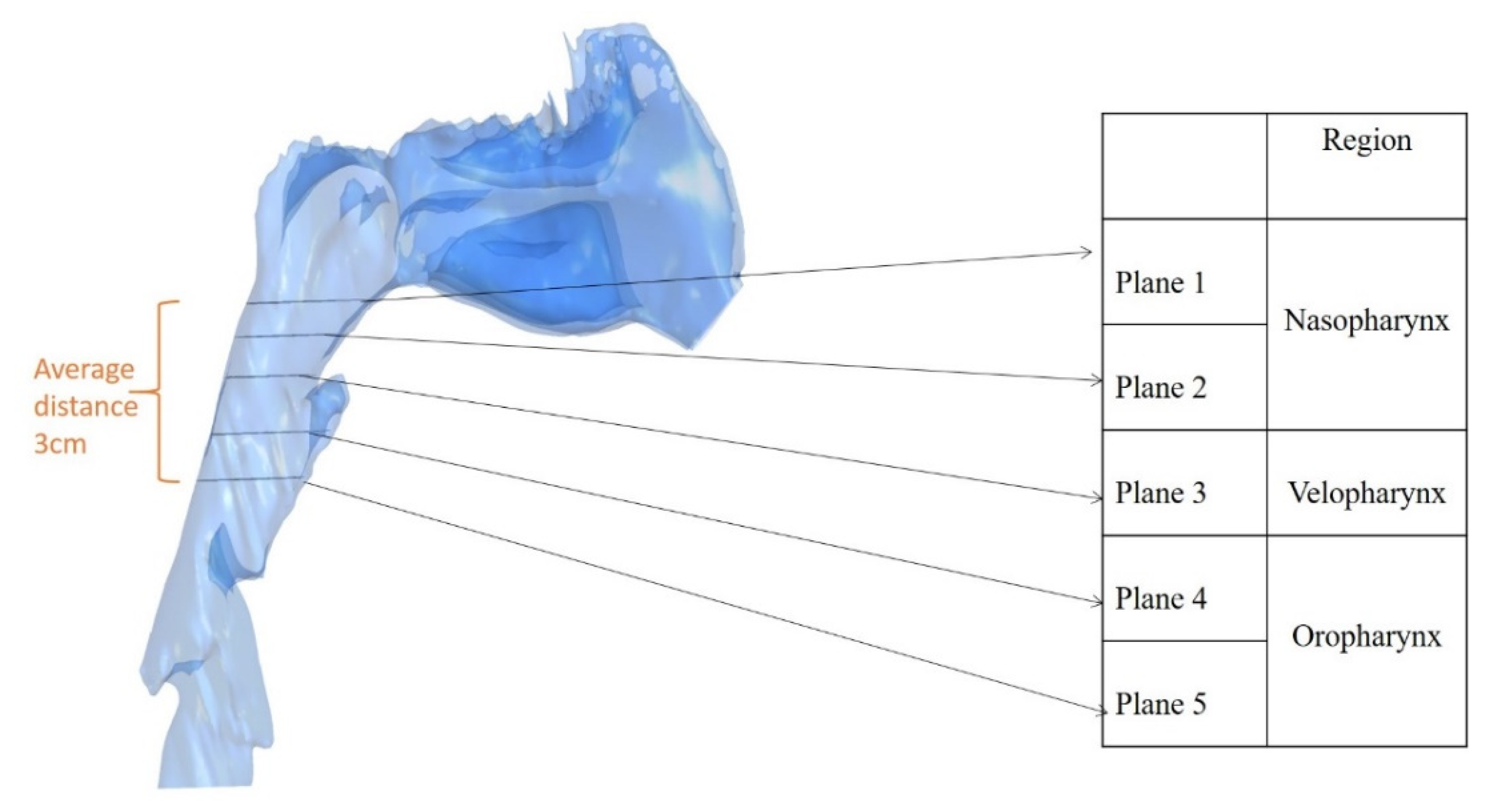
2.5. Outcome Parameters
2.6. Statistical Analysis
3. Results
3.1. Comparison of the Pre- and Post-Operative Measurements
3.2. Correlation between the Surgical Changes and Outcome Parameters
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
References
- Croce, C.; Fodil, R.; Durand, M.; Sbirlea-Apiou, G.; Caillibotte, G.; Papon, J.-F.; Blondeau, J.-R.; Coste, A.; Isabey, D.; Louis, B. In Vitro Experiments and Numerical Simulations of Airflow in Realistic Nasal Airway Geometry. Ann. Biomed. Eng. 2006, 34, 997–1007. [Google Scholar] [CrossRef] [PubMed]
- Ferziger, J.H.; Peric, M. Computational Methods for Fluid Dynamics, 3rd ed.; Springer: Berlin/Heidelberg, Germany, 2002; p. 426. [Google Scholar]
- Gokce, S.M.; Görgülü, S.; Gokce, H.S.; Bengi, A.O.; Karacayli, U.; Ors, F. Evaluation of pharyngeal airway space changes after bimaxillary orthognathic surgery with a 3-dimensional simulation and modeling program. Am. J. Orthod. Dentofac. Orthop. 2014, 146, 477–492. [Google Scholar] [CrossRef] [PubMed]
- Gonçales, E.S.; Rocha, J.F.; Gonçales, A.G.; Yaedú, R.Y.; Sant’Ana, E. Computerized cephalometric study of the pharyngeal airway space in patients submitted to orthognathic surgery. J. Maxillofac. Oral Surg. 2013, 13, 253–258. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gottsauner-Wolf, S.; Laimer, J.; Bruckmoser, E. Posterior Airway Changes Following Orthognathic Surgery in Obstructive Sleep Apnea. J. Oral Maxillofac. Surg. 2018, 76, 1093.e1–1093.e21. [Google Scholar] [CrossRef]
- Jakobsone, G.; Neimane, L.; Krumina, G. Two- and three-dimensional evaluation of the upper airway after bimaxillary correction of Class III malocclusion. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2010, 110, 234–242. [Google Scholar] [CrossRef]
- Jang, S.-I.; Ahn, J.; Paeng, J.-Y.; Hong, J. Three-dimensional analysis of changes in airway space after bimaxillary orthognathic surgery with maxillomandibular setback and their association with obstructive sleep apnea. Maxillofac. Plast. Reconstr. Surg. 2018, 40, 33. [Google Scholar] [CrossRef]
- Jeong, S.; Sung, J.; Kim, Y.-D.; Shin, S.; Kim, S.-S. Upper airway morphologic changes after mandibular setback surgery in skeletal class III malocclusion patients measured using cone beam computed tomography superimposition. Int. J. Oral Maxillofac. Surg. 2018, 47, 1405–1410. [Google Scholar] [CrossRef]
- Katiyar, R.; Singh, G.K.; Mehrotra, D.; Singh, A. Surgical–orthodontic treatment of a skeletal class III malocclusion. Natl. J. Maxillofac. Surg. 2010, 1, 143–149. [Google Scholar] [CrossRef] [Green Version]
- Kim, H.Y.; Bok, K.H.; Dhong, H.-J.; Chung, S.-K. The correlation between pharyngeal narrowing and the severity of sleep-disordered breathing. Otolaryngol. Head Neck Surg. 2008, 138, 289–293. [Google Scholar] [CrossRef]
- Kim, M.A.; Kim, B.R.; Choi, J.Y.; Youn, J.K.; Kim, Y.J.; Park, Y.H. Three-dimensional changes of the hyoid bone and airway volumes related to its relationship with horizontal anatomic planes after bimaxillary surgery in skeletal Class III patients. Angle Orthod. 2013, 83, 623–629. [Google Scholar] [CrossRef] [Green Version]
- Lee, Y.; Chun, Y.S.; Kang, N.; Kim, M. Volumetric changes in the upper airway after bimaxillary surgery for skeletal class III malocclusions: A case series study using 3-dimensional cone-beam computed tomography. J. Oral Maxillofac. Surg. 2012, 70, 2867–2875. [Google Scholar] [CrossRef] [PubMed]
- Lu, M.Z.; Liu, Y.; Ye, J.Y.; Luo, H.Y. Large Eddy Simulation of Flow in Realistic Human Upper Airways with Obstructive Sleep. Procedia Comput. Sci. 2014, 29, 557–564. [Google Scholar] [CrossRef] [Green Version]
- Menter, F.R. Two-equation eddy-viscosity turbulence models for engineering applications. AIAA J. 1994, 32, 1598–1605. [Google Scholar] [CrossRef] [Green Version]
- Mihaescu, M.; Murugappan, S.; Kalra, M.; Khosla, S.; Gutmark, E. Large Eddy Simulation and Reynolds-Averaged Navier-Stokes modeling of flow in a realistic pharyngeal airway model: An investigation of obstructive sleep apnea. J. Biomech. 2008, 41, 2279–2288. [Google Scholar] [CrossRef]
- Mihaescu, M.; Mylavarapu, G.; Farbos de Luzan, C.; Gutmark, E.; Powell, N. Large Eddy Simulation for Estimating Flow Instabilities Associated with Obstructive Sleep Apnea in a Pharyngeal Airway. In Proceedings of the International Conference on Jets, Wakes and Separated Flows, ICJWSF-2010, Cincinnati, OH, USA, 27–30 September 2010. [Google Scholar]
- Na, J.S.; Jung, H.D.; Cho, H.J.; Choi, Y.J.; Lee, J.S. Computational analysis of airflow dynamics for predicting collapsible sites in the upper airways: A preliminary study. J. Appl. Physiol. 2019, 126, 330–340. [Google Scholar] [CrossRef]
- Piao, Y.; Kim, S.J.; Yu, H.S.; Cha, J.Y.; Baik, H.S. Five-year investigation of a large orthodontic patient population at a dental hospital in South Korea. Korean J. Orthod. 2016, 46, 137–145. [Google Scholar] [CrossRef] [Green Version]
- Borojeni, A.A.T.; Garcia, G.J.M.; Moghaddam, M.G.; Frank-Ito, D.O.; Kimbell, J.S.; Laud, P.W.; Koenig, L.J.; Rhee, J.S. Normative ranges of nasal airflow variables in healthy adults. Int. J. Comput. Assist. Radiol. Surg. 2020, 15, 87–98. [Google Scholar] [CrossRef]
- Borojeni, A.A.T.; Frank-Ito, D.O.; Kimbell, J.S.; Rhee, J.S.; Garcia, G.J. Creation of an idealized nasopharynx geometry for accurate computational fluid dynamics simulations of nasal airflow in patient-specific models lacking the nasopharynx anatomy. Int. J. Numer. Methods Biomed. Eng. 2016, 33, e2825. [Google Scholar] [CrossRef] [Green Version]
- Rama, A.N.; Tekwani, S.H.; Kushida, C.A. Sites of obstruction in obstructive sleep apnea. Chest 2002, 122, 1139–1147. [Google Scholar] [CrossRef] [Green Version]
- Sascău, R.; Zota, I.M.; Stătescu, C.; Boișteanu, D.; Roca, M.; Maștaleru, A.; Constantin, M.M.L.; Vasilcu, T.F.; Gavril, R.S.; Mitu, F. Review of Echocardiographic Findings in Patients with Obstructive Sleep Apnea. Can. Respir. J. 2018, 2018, 1206217. [Google Scholar] [CrossRef] [Green Version]
- Shin, J.H.; Kim, M.A.; Park, I.Y.; Park, Y.H. A 2-year follow-up of changes after bimaxillary surgery in patients with mandibular prognathism: 3-dimensional analysis of pharyngeal airway volume and hyoid bone position. J. Oral Maxillofac. Surg. 2015, 73, 340.e1–340.e9. [Google Scholar] [CrossRef] [PubMed]
- Shivalkar, B.; Van de Heyning, C.; Kerremans, M.; Rinkevich, D.; Verbraecken, J.; De Backer, W.; Vrints, C. Obstructive sleep apnea syndrome: More insights on structural and functional cardiac alterations, and the effects of treatment with continuous positive airway pressure. J. Am. Coll. Cardiol. 2006, 47, 1433–1439. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taherian, S.; Rahai, H.; Gomez, B.; Waddington, T.; Mazdisnian, F. Computational fluid dynamics evaluation of excessive dynamic airway collapse. Clin. Biomech. 2017, 50, 145–153. [Google Scholar] [CrossRef] [PubMed]
- Taherian, S.; Rahai, H.; Lopez, S.; Shin, J.; Jafari, B. Evaluation of human obstructive sleep apnea using computational fluid dynamics. Commun. Biol. 2019, 2, 423. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taherian, S.; Rahai, H.R.; Bonifacio, J.; Gomez, B.Z.; Waddington, T. Particulate Deposition in a Patient with Tracheal Stenosis. J. Eng. Sci. Med. Diagn. Ther. 2017, 1, 011005. [Google Scholar] [CrossRef] [Green Version]
- Tan, S.K.; Tang, A.T.H.; Leung, W.K.; Zwahlen, R.A. Three-Dimensional Pharyngeal Airway Changes After 2-Jaw Orthognathic Surgery with Segmentation in Dento-Skeletal Class III Patients. J. Craniofacial Surg. 2019, 30, 1533–1538. [Google Scholar] [CrossRef]
- Tepecik, T.; Ertaş, Ü.; Akgün, M. Effects of bimaxillary orthognathic surgery on pharyngeal airway and respiratory function at sleep in patients with class III skeletal relationship. J. Cranio-Maxillofac. Surg. 2018, 46, 645–653. [Google Scholar] [CrossRef]
- Vos, W.; De Backer, J.; Devolder, A.; Vanderveken, O.M.; Verhulst, S.; Salgado, R.; Germonpre, P.; Partoens, B.; Wuyts, F.; Parizel, P.; et al. Correlation between severity of sleep apnea and upper airway morphology based on advanced anatomical and functional imaging. J. Biomech. 2007, 40, 2207–2213. [Google Scholar] [CrossRef]
- Wiedemeyer, V.; Berger, M.; Martini, M.; Kramer, F.J.; Heim, N. Predictability of pharyngeal airway space dimension changes after orthognathic surgery in class II patients: A mathematical approach. J. Cranio-Maxillofac. Surg. 2019, 47, 1504–1509. [Google Scholar] [CrossRef]
- Wilcox, D.C. Turbulence Modeling for CFD. In Turbulence Modeling for CFD, 1st ed.; DCW Industries, Inc.: La Cañada Flintridge, CA, USA, 1994. [Google Scholar]
- Wootton, D.M.; Luo, H.; Persak, S.C.; Sin, S.; McDonough, J.M.; Isasi, C.R.; Arens, R. Computational fluid dynamics endpoints to characterize obstructive sleep apnea syndrome in children. J. Appl. Physiol. 2014, 116, 104–112. [Google Scholar] [CrossRef]
- Xu, C.; Sin, S.; McDonough, J.M.; Udupa, J.K.; Guez, A.; Arens, R.; Wootton, D.M. Computational fluid dynamics modeling of the upper airway of children with obstructive sleep apnea syndrome in steady flow. J. Biomech. 2006, 39, 2043–2054. [Google Scholar] [CrossRef] [PubMed]
- Zhao, M.; Barber, T.; Cistulli, P.; Sutherland, K.; Rosengarten, G. Computational fluid dynamics for the assessment of upper airway response to oral appliance treatment in obstructive sleep apnea. J. Biomech. 2013, 46, 142–150. [Google Scholar] [CrossRef] [PubMed]
- Zheng, Z.; Liu, H.; Xu, Q.; Wu, W.; Du, L.; Chen, H.; Zhang, Y.; Liu, D. Computational fluid dynamics simulation of the upper airway response to large incisor retraction in adult class I bimaxillary protrusion patients. Sci. Rep. 2017, 7, 45706. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fan, Y.; Dong, J.; Tian, L.; Inthavong, K.; Tu, J. Numerical and Experimental Analysis of Inhalation Airflow Dynamics in a Human Pharyngeal Airway. Int. J. Environ. Res. Public Health 2020, 17, 1556. [Google Scholar] [CrossRef] [PubMed] [Green Version]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Original Patient Number | Age/Sex | BMI (kg/m2) | Pre-Operative (T0) Immediate Post-Operative (T1) 6 Months Post-Operative (T2) |
|---|---|---|---|
| Patient 1 | 23/M | 22.7 | T0, T2 |
| Patient 2 | 19/M | 20.5 | T0, T2 |
| Patient 3 | 19/M | 25.9 | T0, T1, T2 |
| Patient 4 | 19/F | 18.9 | T0, T2 |
| Patient 5 | 20/F | 24.3 | T0, T2 |
| Patient 6 | 20/F | 22.7 | T0, T1, T2 |
| Patient 7 | 21/M | 24.9 | T0, T1, T2 |
| Patient 8 | 22/F | 19.1 | T0, T2 |
| Patient 9 | 26/F | 19.2 | T0, T2 |
| Patient 10 | 18/F | 19.9 | T0, T2 |
| Patient 11 | 33/M | 23.5 | T0, T1, T2 |
| Landmarks | |
|---|---|
| PNS | The most posterior point of the hard palate. |
| B Point | The deepest anterior point in the concavity of the anterior mandible. |
| A Point | Most concave point of anterior maxilla |
| Reference planes | |
| FH Plane | Constructed on both sides of Po and to the right of the orbitale. |
| Vertical Reference Plane | Perpendicular to the FH plane passing through sella turcica. |
| T-y Plane | Parallel to the vertical reference plane and 20 mm in front. |
| T-x Plane | Parallel to the FH plane and passing through the most anterior inferior point of the body of the second cervical vertebra. |
| T0 | T1 | p-Value | T2 | p-Value | ||
|---|---|---|---|---|---|---|
| Nasopharynx | Plane 1 | 4.61 ± 1.71 | 2.82 ± 1.10 | 0.144 | 4.05 ± 1.72 | 0.066 |
| Plane 2 | 3.77 ± 1.62 | 2.7 ± 0.77 | 0.068 | 3.53 ± 1.69 | 0.441 | |
| Velopharynx | Plane 3 | 2.96 ± 1.64 | 1.9 ± 0.75 | 0.068 | 2.83 ± 1.71 | 0.173 |
| Oropharynx | Plane 4 | 3.76 ± 1.74 | 2.32 ± 1.06 | 0.144 | 3.28 ± 1.70 | 0.051 |
| Plane 5 | 3.47 ± 1.82 | 2.13 ± 0.40 | 0.068 | 3.32 ± 1.83 | 0.314 |
| T0 | T1 | p-Value | T2 | p-Value | |
|---|---|---|---|---|---|
| Total volume | 62.04 ± 19.7 | 47.88 ± 9.06 | 0.465 | 57.25 ± 11.6 | 0.534 |
| Pressure Drop (Pa) | Adjusted Pressure Coefficient | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| T0 | T1 | p-Value | T2 | p-Value | T0 | T1 | p-Value | T2 | p-Value | |
| 1.25 s I.P. | −54.68 ± 103.66 | −101.5 ± 140.2 | 0.144 | −119.18 ± 154.9 | 0.075 | 0.48 ± 0.12 | 0.44 ± 0.17 | 1 | 0.59 ± 0.24 | 0.139 |
| 2.5 s R.P. | −48.17 ± 92.30 | −86.34 ± 114.3 | 0.144 | −207.21 ± 379.8 | 0.075 | 0.47 ± 0.18 | 0.45 ± 0.16 | 0.715 | 0.57 ± 0.24 | 0.050 |
| 3.75 s E.P. | −40.40 ± 78.47 | −72.68 ± 93.90 | 0.144 | −160.71 ± 288.59 | 0.075 | 0.46 ± 0.18 | 0.61 ± 0.08 | 0.175 | 0.55 ± 0.25 | 0.212 |
| Δ Pressure Drop | Δ Adjusted Pressure Coefficient | ||||||
|---|---|---|---|---|---|---|---|
| 1.25 s I.P. | 2.5 s R.P. | 3.75 s E.P. | 1.25 s I.P. | 2.5 s R.P. | 3.75 s E.P. | ||
| Tongue x | r | 0.638 | 0.615 | 0.597 | −0.565 | −0.553 | −0.534 |
| p-value | 0.035 * | 0.044 * | 0.053 | 0.070 | 0.078 | 0.091 | |
| Δ Plane 2 | r | 0.655 | 0.655 | 0.618 | −0.355 | −0.560 | −0.433 |
| p-value | 0.029 * | 0.029 * | 0.043 * | 0.285 | 0.073 | 0.183 | |
| Δ Volume | Hyoid (y-Axis) | Tongue (x-Axis) | |
|---|---|---|---|
| Δ Plane 1 | r = 0.8 p = 0.000 | - | r = 0.7 p = 0.023 |
| Δ Plane 2 | - | - | |
| Δ Plane 3 | r = 0.7 p = 0.004 | - | - |
| Δ Plane 4 | r = 0.8 p = 0.003 | - | - |
| Δ Plane 5 | - | r = 0.68 p = 0.042 | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wadhwa, P.; Jang, H.-S.; Park, S.-H.; Kim, H.-H.; Lee, E.-S. Computational Fluid Dynamic Analysis of the Pharyngeal Airway after Bimaxillary Orthognathic Surgery in Patients with Mandibular Prognathism. Processes 2021, 9, 152. https://0-doi-org.brum.beds.ac.uk/10.3390/pr9010152
Wadhwa P, Jang H-S, Park S-H, Kim H-H, Lee E-S. Computational Fluid Dynamic Analysis of the Pharyngeal Airway after Bimaxillary Orthognathic Surgery in Patients with Mandibular Prognathism. Processes. 2021; 9(1):152. https://0-doi-org.brum.beds.ac.uk/10.3390/pr9010152
Chicago/Turabian StyleWadhwa, Puneet, Hyon-Seok Jang, Se-Hyun Park, Hyoung-Ho Kim, and Eui-Seok Lee. 2021. "Computational Fluid Dynamic Analysis of the Pharyngeal Airway after Bimaxillary Orthognathic Surgery in Patients with Mandibular Prognathism" Processes 9, no. 1: 152. https://0-doi-org.brum.beds.ac.uk/10.3390/pr9010152