
Is Gutta-Percha Still the “Gold Standard” among Filling Materials in Endodontic Treatment?

 , and
, and
Abstract
:1. Introduction on the Modern Stage of Sustainable Development of Dentistry
2. Main Goals of the Paper and Justification of Its Structure
3. Principles of Tooth Qualification for Endodontic Treatment
- Preliminary analysis and diagnostic evaluation of teeth to qualify for endodontic treatment;
- Removal of the pulp chamber roof;
- Identification of the pulp chamber mouth and the bottom of the root canal opening; and
- Root canal instrumentation.
4. Importance of the Selection of Filling Material for Endodontic Treatment
5. Methods and Tools of Root Canal Preparation in Endodontic Treatment
6. Importance of Sterilization of Endodontic Instruments and Lubricants for the Effectiveness of Root Canal Preparation
7. Review of Root Canal Obturation Methods
8. Selection and Description of the Scope and Methodology of Experimental Research
- Clinical—how to choose the conditions for the development and obturation of root canals;
- Technological—which of the methods used for the development and obturation of root canals ensures the best tightness of the filling;
- Methodological—what research methods are most useful for the assessment of the effectiveness of endodontic treatment; and
- Scientific—why there is a difference in the tightness of the filling between the root canal wall and the filling material, depending on the adopted root canal preparation and obturation method.
9. Results of Experimental Research and Their Discussion
10. Strengths, Weaknesses, Opportunities, and Threats Analysis of Filling Material Based on Gutta-Percha
11. Summary and General Conclusions
- It has been fully confirmed that the material based on gutta-percha is still the “gold standard” among endodontic filling materials;
- It has been shown that the cause of differentiation in the effectiveness of endodontic treatment, measured by the tightness between the root canal wall and the filling, is the formation of a tight three-layer connection between the dentin of the root canal; the sealant usually in a relatively small proportion, which is a favorable tendency; and the filling material in the form of a monoblock, ensuring a homogeneous structure; and filling with plasticized material of the lateral canals, especially using the THC method, and in the apical zone partly with a sealant, root delta with plasticized material as well as a sealant, dentinal tubules mainly with a sealant, which occurs only in the case of heat obturation with filling material based on gutta-percha using the THC method with Obtura III and System B devices, when in other cases there is no close connection of structural components, which determines the relatively lower quality of the connection and lower suitability of these methods for use in endodontics;
- The method of root canal preparation, including the extensive use of tools made of a nickel–titanium alloy of the nitinol type, and the method of obturation, where the thermo-hydraulic condensation (THC) technique plays the most important role, while the correct selection of sealants is also of major importance;
- The best efficiency of root canal filling among the analyzed and empirically tested in this study was ensured by the technology consisting of the preparation of dental canals with K3 rotary tools and filling the teeth with the THC thermoplastic method using System B and Obtura III devices with studs and pellets made of material based on gutta-percha after covering the walls root canal with a thin layer of AH Plus sealant;
- It has been shown that visualization methods with the use of materialographic microscopes, especially the scanning electron microscope (SEM) and the light stereoscopic microscope (LSM), due to the possibility of obtaining a sufficiently high resolution with which to observe the tested specimens, and the possibility of unequivocally determining the details of the tested material, are most useful for evaluation of the effectiveness of methods and techniques of endodontic treatment in vitro and ex post, where it is recommended to make preparations by breaking them after cooling them in liquid nitrogen along the tooth axis, because the use of specimens prepared differently is much lower, especially as materialographic samples.
Author Contributions
Funding
Conflicts of Interest
Notice
References
- Dobrzański, L.A.; Dobrzański, L.B.; Dobrzańska-Danikiewicz, A.D.; Dobrzańska, J. The Concept of Sustainable Development of Modern Dentistry. Processes 2020, 8, 1605. [Google Scholar] [CrossRef]
- Caldas, A.F., Jr. Reason for tooth extraction in a Brazilian population. Int. Dent. J. 2000, 50, 267–273. [Google Scholar] [CrossRef]
- Chestnutt, I.G.; Binnie, V.I.; Taylor, M.M. Reason for tooth extraction in Scotland. J. Dent. 2000, 28, 295–297. [Google Scholar] [CrossRef]
- Morita, M.; Kimura, T.; Kanegae, M.; Ishikawa, A.; Watanobe, T. Reasons for extraction of permanent teeth in Japan. Community Dent. Oral. Epidemiol. 1994, 22, 303–306. [Google Scholar] [CrossRef] [PubMed]
- Angelillo, I.F.; Nobile, C.G.A.; Pavia, M. Survey of reasons for extraction of permanent teeth in Italy. Community Dent. Oral. Epidemiol. 1996, 24, 336–340. [Google Scholar] [CrossRef] [PubMed]
- Al-Shammari, K.F.; Al-Arsari, J.M.; Al-Melh, M.A.; Al-Khabhaz, A.K. Reasons for tooth extraction in Kuwait. Med. Princ. Pract. 2006, 15, 417–422. [Google Scholar] [CrossRef]
- Fejerskov, O. Concepts of dental caries and their consequences for understanding the disease. Community Dent. Oral Epidemiol. 1997, 25, 5–12. [Google Scholar] [CrossRef] [PubMed]
- Reisine, S.; Litt, M. Social and psychological theories and their use for dental practice. Int. Dent. J. 1993, 43, 279–287. [Google Scholar]
- Selwitz, R.H.; Ismail, A.I.; Pitts, N.B. Dental caries. Lancet 2007, 369, 51–59. [Google Scholar] [CrossRef]
- Costerton, J.W. Introduction to biofilm. Int. J. Antimicrob. Agents 1999, 11, 217–221. [Google Scholar] [CrossRef]
- Svensater, G.; Bergenholtz, G. Biofilms in endodontic infections. Endod. Top. 2004, 9, 27–36. [Google Scholar] [CrossRef]
- Zero, D.T. Dental caries process. Dent. Clin. N. Am. 1999, 43, 635–664. [Google Scholar]
- Featherstone, J.D. The continuum of dental caries—evidence for a dynamic disease process. J. Dent. Res. 2004, 83, C39–C42. [Google Scholar] [CrossRef] [PubMed]
- Pitts, N.B. A review of the current knowledge of the progress of approximal lesions. In Proceedings of the 10th Asian Pacific Dental Scientific Congress, Singapore, 26–31 March 1981; Singapore Dental Association: Singapore, 1983; pp. 31–36. [Google Scholar]
- Amaechi, B.T. Remineralization therapies for initial caries lesions. Curr. Oral Health Rep. 2015, 2, 95–101. [Google Scholar] [CrossRef]
- Zero, D.T. Dentifrices, mouthwashes, and remineralization/caries arrestment strategies. BMC Oral Health 2006, 6, S9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Holmgren, C.; Gaucher, N.; Decerle, N.; Doméjean, S. Minimal intervention dentistry II: Part 3. Management of non-cavitated (initial) occlusal caries lesions—Non-invasive approaches through remineralization and therapeutic sealants. Br. Dent. J. 2014, 216, 237–243. [Google Scholar] [CrossRef] [Green Version]
- Takahashi, N.; Nyvad, B. Caries ecology revisited: Microbial dynamics and the caries process. Caries Res. 2008, 42, 409–418. [Google Scholar] [CrossRef]
- Margolis, H.C.; Moreno, E.C. Composition and cariogenic potential of dental plaque fluid. Crit. Rev. Oral Biol. Med. 1994, 5, 1–25. [Google Scholar] [CrossRef]
- Margolis, H.C.; Moreno, E.C. Kinetics of hydroxyapatite dissolution in acetic, lactic, and phosphoric acid solutions. Calcif. Tissue Int. 1992, 50, 137–143. [Google Scholar] [CrossRef]
- Vogel, G.L.; Carey, C.M.; Chow, L.C.; Gregory, T.M.; Brown, W.E. Micro-analysis of mineral saturation within enamel during lactic acid demineralization. J. Dent. Res. 1988, 67, 1172–1180. [Google Scholar] [CrossRef]
- Reynolds, E.C.; Cai, F.; Shen, P.; Walker, G.D. Retention in plaque and remineralization of enamel lesions by various forms of calcium in a mouthrinse or sugar-free chewing gum. J. Dent. Res. 2003, 82, 206–211. [Google Scholar] [CrossRef]
- Kitasako, Y.; Sadr, A.; Hamba, H.; Ikeda, M.; Tagami, J. Gum containing calcium fluoride reinforces enamel subsurface lesions in situ. J. Dent. Res. 2012, 91, 370–375. [Google Scholar] [CrossRef] [PubMed]
- Hamba, H.; Nikaido, T.; Inoue, G.; Sadr, A.; Tagami, J. Effects of CPP-ACP with sodium fluoride on inhibition of bovine enamel demineralization: A quantitative assessment using micro-computed tomography. J. Dent. 2011, 39, 405–413. [Google Scholar] [CrossRef]
- ten Cate, J.M.; Featherstone, J.D. Mechanistic aspects of the interactions between fluoride and dental enamel. Crit. Rev. Oral Biol. Med. 1991, 2, 283–296. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.E.; Baek, H.J.; Choi, Y.H.; Jeong, S.H.; Park, Y.D.; Song, K.B. Comparison of remineralization effect of three topical fluoride regimens on enamel initial carious lesions. J. Dent. 2010, 38, 166–171. [Google Scholar] [CrossRef] [PubMed]
- Amaechi, B.T.; van Loveren, C. Fluorides and non-fluoride remineralization systems. Monogr. Oral Sci. 2013, 23, 15–26. [Google Scholar] [CrossRef]
- Featherstone, J.D. Prevention and reversal of dental caries: Role of low level fluoride. Community Dent. Oral Epidemiol. 1999, 27, 31–40. [Google Scholar] [CrossRef]
- Iheozor-Ejiofor, Z.; Worthington, H.V.; Walsh, T.; O’Malley, L.; Clarkson, J.E.; Macey, R.; Alam, R.; Tugwell, P.; Welch, V.; Glenny, AM. Water fluoridation for the prevention of dental caries. Cochrane Database Syst. Rev. 2015, 6, CD010856. [Google Scholar] [CrossRef]
- Pitts, N.B.; Zero, D.T.; White Paper on Dental Caries Prevention and Management. FDI World Dental Federation. Available online: https://www.fdiworlddental.org/sites/default/files/2020-11/2016-fdi_cpp-white_paper.pdf (accessed on 19 May 2021).
- Kidd, E.A.M.; Fejerskov, O. What constitutes dental caries? Histopathology of carious enamel and dentin related to the action of cariogenic biofilms. J. Dent. Res. 2004, 83, C35–C38. [Google Scholar] [CrossRef] [PubMed]
- Yu, C.; Abbott, P.V. An overview of the dental pulp: Its functions and responses to injury. Aust. Dent. J. 2007, 52, S4–S16. [Google Scholar] [CrossRef]
- Harumi Miyagi, S.P.; Kerkis, I.; da Costa Maranduba, C.M.; Gomes, C.M.; Martinis, M.D.; Marques, M.M. Expression of extracellular matrix proteins in human dental pulp stem cells depends on the donor tooth conditions. J. Endod. 2010, 36, 826–831. [Google Scholar] [CrossRef] [PubMed]
- Dobrzańska, J. Analiza Szczelności Wypełnień Kanałów Korzeniowych. Ph.D. Thesis, Śląski Uniwersytet Medyczny w Katowicach, Zabrze, Poland, 2011. [Google Scholar]
- Seltzer, S.; Farber, P.A. Microbiologic factors in endodontology. Oral Surg. Oral Med. Oral Pathol. 1994, 78, 634–645. [Google Scholar] [CrossRef]
- Aas, J.A.; Griffen, A.L.; Dardis, S.R.; Lee, A.M.; Olsen, I.; Dewhirst, F.E.; Leys, E.J.; Paster, B.J. Bacteria of dental caries in primary and permanent teeth in children and young adults. J. Clin. Microbiol. 2008, 46, 1407–1417. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spratt, D.A.; Pratten, J.; Wilson, M.; Gulabivala, K. An in vitro evaluation of the antimicrobial efficacy of irrigants on biofilms of root canal isolates. Int. Endod. J. 2001, 34, 300–307. [Google Scholar] [CrossRef] [Green Version]
- Vieira, C.L.Z.; Caramelli, B. The history of dentistry and medicine relationship: Could the mounth finally return to the body? Oral Dis. 2009, 15, 538–546. [Google Scholar] [CrossRef]
- Paju, S.; Scannapieco, F.A. Oral biofilms, periodontitis and pulmonary infections. Oral Dis. 2007, 13, 508–512. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al-Nawas, B.; Maeurer, M. Severe versus local odontogenic bacterial infections: Comparision of microbial isolates. Eur. Surg. Res. 2008, 40, 220–224. [Google Scholar] [CrossRef]
- Stanley, H.R. Dental iatrogenesis. Int. Dent. J. 1994, 44, 3–18. [Google Scholar] [PubMed]
- Love, R.M. Effects of dental trauma on the pulp. Pract. Periodontics Aesthert. Dent. 1997, 9, 427–436. [Google Scholar]
- Mueller, A.A.; Saldami, B.; Stübinger, S.; Walter, C.; Flückiger, U.; Merlo, A.; Schwenzer-Zimmerer, K.; Zeilhofer, H.F.; Zimmerer, S. Oral bacterial cultures in nontraumatic brain abscesses: Results of a first line study. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2009, 107, 469–476. [Google Scholar] [CrossRef]
- Pallasch, T.J.; Wahl, M.J. Focal infection: New age or ancient history? Endod. Top. 2003, 4, 32–45. [Google Scholar] [CrossRef] [Green Version]
- Buset, S.L.; Walter, C.; Friedmann, A.; Weiger, R.; Borgnakke, W.S.; Zitzmann, N.U. Are periodontal diseases really silent? A systematic review of their effect on quality of life. J. Clin. Periodontol. 2016, 43, 333–344. [Google Scholar] [CrossRef] [PubMed]
- Sierpinska, T.; Golebiewska, M.; Dlugosz, J.W.; Kemona, A.; Laszewicz, W. Connection between masticatory efficiency and pathomorphologic changes in gastric mucosa. Quintessence Int. 2007, 38, 31–37. [Google Scholar]
- De Pablo, P.; Dietrich, T.; McAlindon, T.E. Association of periodontal disease and tooth loss with rheumatoid arthritis in the US population. J. Rheumatol. 2008, 35, 70–76. [Google Scholar]
- Felton, D.A. Edentualism and comorbid factors. J. Prosthodont. 2009, 18, 88–96. [Google Scholar] [CrossRef]
- Volzke, H.; Schwahn, C.; Hummel, A.; Wolff, B.; Kleine, V.; Robinson, D.M.; Dahm, J.B.; Felix, S.B.; John, U.; Kocher, T. Tooth loss is independently associated with the risk of acquired aortic valve sclerosis. Am. Heart J. 2005, 150, 1198–1203. [Google Scholar] [CrossRef]
- Bagchi, S.; Tripathi, A.; Tripathi, S.; Kar, S.; Tiwari, S.C.; Singh, J. Obstructive sleep apnea and neurocognitive dysfunction in edentulous patients. J. Prosthodont. 2019, 28, e837–e842. [Google Scholar] [CrossRef] [PubMed]
- Nagpal, R.; Yamashiro, Y.; Izumi, Y. The two-way association of periodontal infection with systemic disorders: An overview. Mediat. Inflamm. 2015, 2015, 793898. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abnet, C.C.; Qiao, Y.L.; Dawsey, S.M.; Dong, Z.W.; Taylor, P.R.; Mark, S.D. Tooth loss is associated with increased risk of total death and death from upper gastrointestinal cancer, heart disease, and stroke in a Chinese population-based cohort. Int. J. Epidemiol. 2005, 34, 467–474. [Google Scholar] [CrossRef] [PubMed]
- Burzyńska, B.; Mierzwińska-Nastalska, E. Rehabilitacja protetyczna pacjentów bezzębnych. Nowa Stomatol. 2011, 4, 167–199. [Google Scholar]
- Bui, F.Q.; Almeida-da-Silva, C.L.C.; Huynh, B.; Trinh, A.; Liu, J.; Woodward, J.; Asadi, H.; Ojcius, D.M. Association between periodontal pathogens and systemic disease. Biomed. J. 2019, 42, 27–35. [Google Scholar] [CrossRef] [PubMed]
- Holmlund, A.; Holm, G.; Lind, L. Number of teeth as a predictor of cardiovascular mortality in a cohort of 7674 subjects followed for 12 years. J. Periodontol. 2010, 81, 870–876. [Google Scholar] [CrossRef]
- Takata, Y.; Ansai, T.; Matsumura, K.; Awano, S.; Hamasaki, T.; Sonoki, K.; Kusaba, A.; Akifusa, S.; Takehara, T. Relationship between tooth loss and electrocardiographic abnormalities in octogenarians. J. Dent. Res. 2001, 80, 1648–1652. [Google Scholar] [CrossRef]
- Felton, D.A. Complete edentulism and comorbid diseases: An update. J. Prosthodont. 2016, 25, 5–20. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Iinuma, M.; Onozuka, M.; Kubo, K.-Y. Chewing maintains hippocampus-dependent cognitive. Int. J. Med. Sci. 2015, 12, 502–509. [Google Scholar] [CrossRef] [Green Version]
- Stein, P.S.; Desrosiers, M.; Donegan, S.J.; Yepes, J.F.; Kryscio, R.J. Tooth loss, dementia and neuropathology in the Nun study. J. Am. Dent. Assoc. 2007, 138, 1314–1322. [Google Scholar] [CrossRef] [PubMed]
- Henke, K. A model for memory systems based on processing modes rather than consciousness. Nat. Rev. Neurosci. 2010, 11, 523–532. [Google Scholar] [CrossRef] [PubMed]
- Lexomboon, D.; Trulsson, M.; Wårdh, I.; Parker, W.G. Chewing ability and tooth loss: Association with cognitive impairment in an elderly population study. J. Am. Geriatr. Soc. 2012, 60, 1951–1956. [Google Scholar] [CrossRef]
- Hirano, Y.; Obata, T.; Takahashi, H.; Tachibana, A.; Kuroiwa, D.; Takahashi, T.; Ikehira, H.; Onozuka, M. Effects of chewing on cognitive processing speed. Brain Cognit. 2013, 81, 376–381. [Google Scholar] [CrossRef]
- Onishi, M.; Iinuma, M.; Tamura, Y.; Kubo, K.Y. Learning deficits and suppression of the cell proliferation in the hippocampal dentate gyrus of offspring are attenuated by maternal chewing during prenatal stress. Neurosci. Lett. 2014, 560, 77–80. [Google Scholar] [CrossRef]
- Kawahata, M.; Ono, Y.; Ohno, A.; Kawamoto, S.; Kimoto, K.; Onozuka, M. Loss of molars early in life develops behavioral lateralization and impairs hippocampus-dependent recognition memory. BMC Neurosci. 2014, 15, 4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, X.; Tornstad, L.; Olsen, I. Brain abscesses caused by oral infection. Dent. Traumatol. 1999, 15, 95–101. [Google Scholar] [CrossRef] [PubMed]
- Scannapieco, F.A.; Bush, R.B.; Paju, S. Associations between periodontal disease and risk for nosocomial bacterial pneumonia and chronic obstructive pulmonary disease. A systemic review. Ann. Periodontol. 2003, 8, 54–69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dobrzański, L.A.; Dobrzański, L.B.; Dobrzańska-Danikiewicz, A.D.; Dobrzańska, J.; Rudziarczyk, K.; Achtelik-Franczak, A. Non-antagonistic contradictoriness of the progress of advanced digitized production with SARS-CoV-2 virus transmission in the area of dental engineering. Processes 2020, 8, 1097. [Google Scholar] [CrossRef]
- Aleksander, M.; Krishnan, B.; Shenoy, N. Diabetes mellitus and odontogenic infections-an exaggerated risk? Oral Maxillofac. Surg. 2008, 12, 129–130. [Google Scholar] [CrossRef] [PubMed]
- Scannapieco, F.A. Role of oral bacteria in respiratory infection. J. Periodontol. 1999, 70, 793–802. [Google Scholar] [CrossRef]
- Dobrzańska, J.; Dobrzański, L.B.; Gołombek, K.; Dobrzański, L.A.; Dobrzańska-Danikiewicz, A.D. Virtual approach to the comparative analysis of biomaterials used in endodontic treatment. Processes 2021, 9, 926. [Google Scholar] [CrossRef]
- Castellucci, A. Endodontics Vol. 1; Il Tridente Edizioni Odontolatriche: Bologna, Italy, 2005. [Google Scholar]
- Alwadani, M.; Mashyakhy, M.H.; Jali, A.; Hakami, A.O.; Areshi, A.; Daghriri, A.A.; Shaabi, F.I.; Al Moaleem, M.M. Dentists and Dental Intern’s Preferences of Root Canal Treatment with Restoration Versus Extraction then Implant-Supported Crown Treatment Plan. Open Dent. J. 2019, 13, 93–100. [Google Scholar] [CrossRef]
- Estrela, C.; Holland, R.; Estrela, C.R.; Alencar, A.H.; Sousa-Neto, M.D.; Pécora, J.D. Characterization of successful root canal treatment. Braz. Dent. J. 2014, 25, 3–11. [Google Scholar] [CrossRef]
- Marthaler, T.M. A standardized system of recording dental conditions. Helv. Odontol. Acta 1966, 10, 1–18. [Google Scholar]
- Dirks, O.B.; van Amerongen, J.; Winkler, K.C. A reproducible method for caries evaluation. J. Dent. Res. 1951, 30, 346–359. [Google Scholar] [CrossRef]
- Black, G.V. A Work on Operative Dentistry: The Technical Procedures in Filling Teeth; Medico-Dental Publishing: Chicago, IL, USA, 1917; p. 5. [Google Scholar]
- Pitts, N. “ICDAS”—An international system for caries detection and assessment being developed to facilitate caries epidemiology, research and appropriate clinical management. Community Dent. Health 2004, 21, 193–198. [Google Scholar] [PubMed]
- ICDAS Website. Available online: https://www.icdas.org/ (accessed on 6 April 2021).
- Ismail, A.I.; Sohn, W.; Tellez, M.; Amaya, A.; Sen, A.; Hasson, H.; Pitts, N.B. The International Caries Detection and Assessment System (ICDAS): An integrated system for measuring dental caries. Community Dent. Oral Epidemiol. 2007, 35, 170–178. [Google Scholar] [CrossRef] [Green Version]
- Ismail, A.; Tellez, M.; Pitts, N.B.; Ekstrand, K.R.; Ricketts, D.; Longbottom, C.; Eggertsson, H.; Deery, C.; Fisher, J.; Young, D.A.; et al. Caries management pathways preserve dental tissues and promote oral health. Community Dent. Oral Epidemiol. 2013, 41, e12–e40. [Google Scholar] [CrossRef] [Green Version]
- Pitts, N.B.; Ekstrand, K.R. International Caries Detection and Assessment System (ICDAS) and its International Caries Classification and Management System (ICCMS)—Methods for staging of the caries process and enabling dentists to manage caries. Community Dent. Oral Epidemiol. 2013, 41, e41–e52. [Google Scholar] [CrossRef]
- Ormond, C.; Douglas, G.; Pitts, N. The use of the International Caries Detection and Assessment System (ICDAS) in a National Health Service general dental practice as part of an oral health assessment. Prim. Dent. Care 2010, 17, 153–159. [Google Scholar] [CrossRef]
- Ismail, A.; Pitts, N.B.; Tellez, M. The international caries classification and management system (ICCMSTM) an example of a caries management pathway. BMC Oral Health 2015, 15, S9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clarkson, B.H.; Exterkate, R.A.M. Noninvasive dentistry: A dream or reality? Caries Res. 2015, 49 (Suppl. 1), 11–17. [Google Scholar] [CrossRef] [PubMed]
- Wierichs, R.J.; Meyer-Lueckel, H. Systematic review on noninvasive treatment of root caries lesions. J. Dent. Res. 2015, 94, 261–271. [Google Scholar] [CrossRef] [PubMed]
- Marsh, P.D.; Head, D.A.; Devine, D.A. Prospects of oral disease control in the future—An opinion. J. Oral Microbiol. 2014, 6, 261–276. [Google Scholar] [CrossRef]
- Edwards Deming, W. Out of the Crisis; Massachusetts Institute of Technology, Center for Advanced Engineering Study: Cambridge, MA, USA, 1986. [Google Scholar]
- Cohen, S.; Hargreaves, K. Pathways of the Pulp, 9th ed.; Mosby: St. Louis, MO, USA, 2006. [Google Scholar]
- Krasner, P.; Rankow, H.J.; Abrams, E.S. Endodontics. Colleagues for Excellence. Access Opening and Canal Location; American Association of Endodontists: Chicago, IL, USA, 2010. [Google Scholar]
- Krasner, P.; Rankow, H.J. Anatomy of the pulp-chamber floor. J. Endod. 2004, 30, 5–16. [Google Scholar] [CrossRef] [Green Version]
- Moreinis, S.A. Avoiding perforation during endodontic access. J. Am. Dent. Assoc. 1979, 98, 707–712. [Google Scholar] [CrossRef]
- Weller, R.N.; Hartwell, G.R. The impact of improved access and searching techniques on detection of the mesiolingual canal in maxillary molars. J. Endod. 1989, 15, 82–83. [Google Scholar] [CrossRef]
- Dental Consumables Market by Product [Dental Implants (Root Form Dental Implants and Plate Form Dental Implants), Dental Prosthetics (Crowns, Bridges, Dentures, Abutments, Veneers, and Inlays & Onlays), Endodontics (Endodontic Files, Obturators, and Permanent Endodontic Sealers), Orthodontics (Brackets, Archwires, Anchorage Appliances, and Ligatures), Periodontics (Dental Sutures and Dental Hemostats), Retail Dental Care Essentials (Specialized Dental Pastes, Dental Brushes, Dental Wash Solutions, Whitening Agents, and Dental Floss), and Other Dental Consumables (Dental Splints, Dental Sealants, Dental Burs, Dental Impression Materials, Dental Disposables, Bonding Agents, Patient Bibs, and Aspirator Tubes & Saliva Ejectors)]—Global Opportunity Analysis and Industry Forecast, 2017–2023. Available online: https://www.alliedmarketresearch.com/dental-consumables-market (accessed on 7 May 2021).
- Endodontic Devices Market Size, Share & Trends Analysis Report by Type (Instruments, Consumables), by End Use (Hospitals, Clinics, Dental Academic & Research Institutes), And Segment Forecasts, 2019–2026. Available online: https://www.grandviewresearch.com/industry-analysis/endodontic-devices-market (accessed on 7 May 2021).
- Dental Endodontics Market (Product—Instruments (Endodontic Scalers & Lasers, Motors, Apex Locators, and Machine Assisted Obturation Systems) and Consumables (Obturation, Shaping and Cleaning, and Access Cavity Preparation); End User: Dental Hospitals, Dental Clinics, and Dental Academic & Research Institutes)—Global Industry Analysis, Size, Share, Growth, Trends, and Forecast 2017–2025. Available online: https://www.transparencymarketresearch.com/dental-endodontics-market.html (accessed on 7 May 2021).
- Wang, Z.; Pan, J.; Wright, J.T.; Bencharit, S.; Zhang, S.; Everett, E.T.; Teixeira, F.B.; Preisser, J.S. Putative stem cells in human dental pulp with irreversible pulpitis: An exploratory study. J. Endod. 2010, 36, 820–825. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krupiński, J. Endodoncja Praktyczna; Wyd. Kwintesencja: Warszawa, Poland, 2008; pp. 30–44. [Google Scholar]
- Siqueira, J.F.; Rocas, I.N.; Lopes, H.P.; de Uzeda, M. Coronal leakage of two root canal sealers containing calcium hydroxide after exposure to human saliva. J. Endod. 1999, 25, 14–16. [Google Scholar] [CrossRef]
- Hirsch, J.M.; Ahlstrom, U.; Henrikson, P.A.; Peterson, LE. Periapical surgery. Int. J. Oral Surg. 1979, 8, 173–185. [Google Scholar] [CrossRef]
- Sundqvist, G.; Figdor, D.; Persson, S.; Sjörgren, U. Microbiological analysis of teeth with failed endodontic treatment and the outcome of conservative re-treatment. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 1998, 85, 86–93. [Google Scholar] [CrossRef]
- Carrotte, P. Endodontics: Part 1. The modern concept of root canal treatment. Br. Dent. J. 2004, 197, 181–183. [Google Scholar] [CrossRef] [Green Version]
- Stabholz, A.; Sahar-Helft, S.; Moshonov, J. Lasers in endodontics. Dent. Clin. N. Am. 2004, 48, 809–832. [Google Scholar] [CrossRef]
- Kimura, Y.; Wilder-Smith, P.; Matsumoto, K. Lasers in endodontics: A review. Int. Endod. J. 2000, 33, 173–185. [Google Scholar] [CrossRef]
- Van der Sluis, L.W.M.; Versluis, M.; Wu, M.K.; Wasserlink, P.R. Passive ultrasonic irrigation of the root canal: A review of the literature. Int. Endod. J. 2007, 40, 415–426. [Google Scholar] [CrossRef]
- Roy, R.A.; Ahmad, M.; Crum, L.A. Physical mechanisms governing the hydrodynamic response of an oscillating ultrasonic file. Int. Endod. J. 1994, 27, 197–207. [Google Scholar] [CrossRef] [PubMed]
- Huque, J.; Kota, K.; Yamaga, M.; Iwaku, M.; Hoshino, E. Bacterial eradication from root dentine by ultrasonic irrigation with sodium hypochloride. Int. Endod. J. 1998, 31, 242–250. [Google Scholar] [CrossRef]
- Asgary, S.; Shadman, B.; Ghalamkarpour, Z.; Shahravan, A.; Ghoddusi, J.; Bagherpour, A.; Akbarzadeh Baghban, A.; Hashemipour, M.; Ghasemian Pour, M. Periapical status and quality of root canal filling and coronal restoration in Iranian population. Iran. Endod. J. 2010, 5, 74–82. [Google Scholar]
- Ǿstravik, D. Materials used for root canal obturation: Technical, biological and clinical testing. Endod. Top. 2005, 12, 25–38. [Google Scholar] [CrossRef]
- Teoh, Y.-Y.; Walsh, L.J. Residual Endodontic Filling Material after Post Space Preparation: A Confocal Microscopic Study. Materials 2017, 10, 1333. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferreira, C.M.; Silva, J.B.A., Jr.; de Paula, R.C.M.; Andrade Feitosa, J.P.; Negreiros Cortez, D.G.; Zaia, A.A.; de Souza-Filho, F.J. Brazilian gutta-percha points. Part I: Chemical composition and X-ray diffraction analysis. Braz. Oral Res. 2005, 19, 193–197. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dobrzańska, J.; Gołombek, K.; Dobrzański, L.B. Polymer materials used in endodontic treatment—in vitro testing. AMSE 2012, 58, 110–115. [Google Scholar]
- Chauhan, A.; Makkar, S.; Garg, N.; Khade, A.; Bhagat, S.; Agarwal, R. Comparison of the apical sealing ability of gutta-percha by three different obturation techniques: Lateral Condensation technique, Single cone root canal obturation technique and Injectable thermoplasticized gutta-percha technique (System B). Ann. RSCB 2021, 25, 873–879. [Google Scholar]
- Schilder, H.; Goodman, A.; Winthrop, A. The termomechanical properties of gutta-percha. Determination of phase transition temperatures for gutta-percha. Oral Surg. Oral Med. Oral Pathol. 1974, 38, 109–114. [Google Scholar] [CrossRef]
- Ferreira, C.M.; Gurgel-Filho, E.D.; Silva, J.B.A., Jr.; de Paula, R.C.M.; Pessoa Andrade Feitosa, J.; de Almeida Gomes, B.P.F.; de Souza-Filho, F.J. Brazilian gutta-percha points. Part II: Thermal properties. Braz. Oral Res. 2007, 21, 29–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Combe, E.C.; Cohen, B.D.; Cumming, K. Alpha- and beta-forms of gutta-percha in products for root canal filling. Int. Endodon. J. 2001, 34, 447–451. [Google Scholar] [CrossRef]
- Ribeiro, M.A.; Queiroz, A.C.F.S.; Silva, P.G.; Yoshinari, G.H.; Guerisoli, D.M.Z.; Pereira, K.F.S. Comparative study of the area filled with gutta-percha in the TC, Thermafil and Lateral Condensation techniques. Rev. Odontol. UNESP 2009, 38, 65–71. [Google Scholar]
- Li, G.H.; Niu, L.N.; Selem, L.C.; Eid, A.A.; Bergeron, B.E.; Chen, J.H.; Pashley, D.H.; Tay, F.R. Quality of obturation achieved by an endodontic core-carrier system with crosslinked gutta-percha carrier in single-rooted canals. J. Dent. 2014, 42, 1124–1134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shin, S.J.; Jee, S.W.; Song, J.S.; Jung, I.Y.; Cha, J.H.; Kim, E. Comparison of regrowth of Enterococcus faecalis in dentinal tubules after sealing with gutta-percha or Resilon. J. Endod. 2008, 34, 445–448. [Google Scholar] [CrossRef]
- Jack, R.M.; Goodell, G.G. In vitro comparison of coronal microleakage between Resilon alone and gutta-percha with a glass ionomer intraorifice barrier using a fluid filtration model. J. Endod. 2008, 34, 718–720. [Google Scholar] [CrossRef]
- Santos, J.; Tjäderhane, L.; Ferraz, C.; Zaia, A.; Alves, M.; De Goes, M.; Carrilho, M. Long-term sealing ability of resin-based root canal fillings. Int. Endod. J. 2010, 43, 455–460. [Google Scholar] [CrossRef]
- Shemesh, H.; Wu, M.K.; Wesselink, P.R. Leakage along the apical root fillings with and without smear layer using two different leakage models: A two month longitudinal ex vivo study. Int. Endod. J. 2006, 39, 968–976. [Google Scholar] [CrossRef]
- De Bruyne, M.A.; De Moor, R.J. Long-term sealing ability of Resilon apical root-end fillings. Int. Endod. J. 2009, 42, 884–892. [Google Scholar] [CrossRef]
- Deus, G.A.D.; Fábio, M.; Rocha, L.A.C.M.; Gurgel-Filho, E.D.; Maniglia, C.F.; Coutinho-Filho, T. Analysis of the film thickness of a root canal sealer following three obturation techniques. Pesqui Odontol. Bras. 2003, 17, 119–125. [Google Scholar] [CrossRef] [Green Version]
- Paqué, F.; Sirtes, G. Apical sealing ability of Resilon/Epiphany versus gutta-percha/AH Plus: Immediate and 16 month leakage. Int. Endod. J. 2007, 40, 722–729. [Google Scholar] [CrossRef]
- Pasqualini, D.; Scotti, N.; Mollo, L.; Berutti, E.; Angelini, E.; Migliaretti, G.; Cuffini, A.; Adlerstein, D. Microbial leakage of Gutta-Percha and Resilon root canal filling material: A comparative study using a new homogeneous assay for sequence detection. J. Biomater. Appl. 2008, 22, 337–352. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shemesh, H.; Souza, E.M.; Wu, M.K.; Wesselink, P.R. Glucose reactivity with filling materials as a limitation for using the glucose leakage model. Int. Endod. J. 2008, 41, 869–872. [Google Scholar] [CrossRef]
- Kokorikos, I.; Kolokouris, I.; Economides, N.; Gogos, C.; Helvatjoglu-Antoniades, M. Long-term evaluation of the sealing ability of two root canal sealers in combination with self-etching bonding agents. J. Adhes. Dent. 2009, 11, 239–246. [Google Scholar] [PubMed]
- Onay, E.O.; Ungor, M.; Orucoglu, H. An in vitro evaluation of the apical sealing ability of a new resin based root canal obturation system. J. Endod. 2006, 32, 976–978. [Google Scholar] [CrossRef] [PubMed]
- Hirai, V.H.; da Silva Neto, U.X.; Westphalen, V.P.D.; Perin, C.P.; Carneiro, E.; Fariniuk, L.F. Comparative analysis of leakage in root canal filling performed with gutta-percha and Resilon cones with AH Plus and Epiphany sealers. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2010, 109, 131–135. [Google Scholar] [CrossRef] [PubMed]
- Saleh, I.M.; Ruyter, I.E.; Haapasalo, M.; Ørstavik, D. Bacterial penetration along different root canal filling materials in the presence or absence of smear layer. Int. Endod. J. 2008, 41, 32–40. [Google Scholar] [CrossRef] [PubMed]
- De-Deus, G.; Namen, F.; Galan, J. Reduced long-term sealing ability of adhesive root fillings after water-storage stress. J. Endod. 2008, 34, 322–325. [Google Scholar] [CrossRef] [PubMed]
- Pandey, P.; Aggarwal, H.; Tikku, A.P.; Singh, A.; Bains, R.; Mishra, S. Comparative evaluation of sealing ability of gutta percha and resilon as root canal filling materials- a systematic review. J. Oral Biol. Craniofac. Res. 2020, 10, 220–226. [Google Scholar] [CrossRef] [PubMed]
- Barborka, B.J.; Woodmansey, K.F.; Glickman, G.N.; Schneiderman, E.; He, J. Long-term Clinical Outcome of Teeth Obturated with Resilon. J. Endod. 2017, 43, 556–560. [Google Scholar] [CrossRef]
- Teixeira, F.B.; Teixeira, E.C.; Thompson, J.Y.; Trope, M. Fracture resistance of roots endodontically treated with a new resin filling material. J. Am. Dent. Assoc. 2004, 135, 646–652. [Google Scholar] [CrossRef]
- Donnermeyer, D.; Bürklein, S.; Dammaschke, T.; Schäfer, E. Endodontic sealers based on calcium silicates: A systematic review. Odontol. 2019, 107, 421–436. [Google Scholar] [CrossRef] [PubMed]
- Gandolfi, M.G.; Siboni, F.; Prati, C. Properties of a novel polysiloxane-guttapercha calcium silicate-bioglass-containing root canal sealer. Dent. Mater. 2016, 32, e113–e126. [Google Scholar] [CrossRef]
- Zoufan, K.; Jiang, J.; Komabayashi, T.; Wang, Y.-H.; Safavi, K.E.; Zhu, Q. Cytotoxicity evaluation of Gutta Flow and Endo Sequence BC sealers. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2011, 112, 657–661. [Google Scholar] [CrossRef] [PubMed]
- Shipper, G.; Ørstavik, D.; Teixeira, F.B.; Trope, M. An evaluation of microbial leakage in roots filled with a thermoplastic synthetic polymer-based root canal filling material (Resilon). J. Endod. 2004, 30, 342–347. [Google Scholar] [CrossRef] [PubMed]
- Shipper, G.; Teixeira, F.B.; Arnold, R.R.; Trope, M. Periapical inflammation after coronal microbial inoculation of dog roots filled with gutta-percha or resilon. J. Endod. 2005, 31, 91–96. [Google Scholar] [CrossRef] [PubMed]
- Kqiku, L.; Miletic, I.; Gruber, H.J.; Anic, I.; Städtler, P. Dichtigkeit von Wurzelkanalfüllungen mit GuttaFlow und Resilon im Vergleich zur lateralen Kondensation. Wien. Med. Wochenschr. 2010, 160, 230–234. [Google Scholar] [CrossRef] [PubMed]
- Silveira, F.F.; Soares, J.A.; Nunes, E.; Mordente, V.L. Negative influence of continuous wave technique on apical sealing of the root canal system with Resilon. J. Oral Sci. 2007, 49, 121–128. [Google Scholar] [CrossRef] [Green Version]
- Kocak, M.M.; Er, O.; Saglam, B.C.; Yaman, S. Apical leakage of epiphany root canal sealer combined with different master cones. Eur. J. Dent. 2008, 2, 91–95. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bodrumlu, E.; Tunga, U. The apical sealing ability of a new root canal filling material. Am. J. Dent. 2007, 20, 295–298. [Google Scholar] [PubMed]
- Bodrumlu, E.; Tunga, U. Coronal sealing ability of a new root canal filling material. J. Can. Dent. Assoc. 2007, 73, 623. [Google Scholar] [PubMed]
- Bodrumlu, E.; Tunga, U. Apical leakage of Resilon obturation material. J. Contemp. Dent. Pract. 2006, 7, 45–52. [Google Scholar] [CrossRef] [PubMed]
- Verissimo, D.M.; do Vale, M.S.; Monteiro, A.J. Comparison of apical leakage between canals filled with gutta-percha/AH-plus and Resilon/Epiphany System, when submitted to two filling techniques. J. Endod. 2007, 33, 291–294. [Google Scholar] [CrossRef]
- Moura-Netto, C.; Pinto, T.; Davidowicz, H.; de Moura, A.A.M. Apical leakage of three resin-based endodontic sealers after 810-nm-diode laser irradiation. Photomed. Laser Surg. 2009, 27, 891–894. [Google Scholar] [CrossRef]
- Wedding, J.R.; Brown, C.E.; Legan, J.J.; Moore, B.K.; Vail, M.M. An in vitro comparison of micro leakage between Resilon and gutta-percha with a fluid filtration model. J. Endod. 2007, 33, 1447–1449. [Google Scholar] [CrossRef]
- Ishimura, H.; Yoshioka, T.; Suda, H. Sealing ability of new adhesive root canal filling materials measured by new dye penetration method. Dent. Mater. J. 2007, 26, 290–295. [Google Scholar] [CrossRef] [Green Version]
- Nawal, R.R.; Parande, M.; Sehgal, R.; Rao, N.R.; Naik, A. A comparative evaluation of 3 root canal filling systems. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2011, 111, 387–393. [Google Scholar] [CrossRef]
- Punia, S.K.; Nadig, P.; Punia, V. An in vitro assessment of apical microleakage in root canals obturated with guttaflow, Resilon, thermafil and lateral condensation: A stereomicroscopic study. J. Conserv. Dent. 2011, 14, 173–177. [Google Scholar] [CrossRef] [Green Version]
- Tunga, U.; Bodrumlu, E. Assessment of the sealing ability of a new root canal obturation material. J. Endod. 2006, 32, 876–878. [Google Scholar] [CrossRef] [PubMed]
- Shashidhar, C.; Shivanna, V.; Shivamurthy, G.; Shashidhar, J. The comparison of microbial leakage in roots filled with resilon and gutta-percha: An in vitro study. J. Conserv. Dent. 2011, 14, 21–27. [Google Scholar] [CrossRef] [PubMed]
- Sagsen, B.; Er, O.; Kahraman, Y.; Orucoglu, H. Evaluation of micro leakage of roots filled with different techniques with a computerized fluid filtration technique. J. Endod. 2006, 32, 1168–1170. [Google Scholar] [CrossRef] [PubMed]
- Kqiku, L.; Städtler, P.; Gruber, H.J.; Baraba, A.; Anic, I.; Miletic, I. Active versus passive microleakage of Resilon/Epiphany and gutta-percha/AH Plus. Aust. Endod. J. 2011, 37, 141–146. [Google Scholar] [CrossRef]
- Aptekar, A.; Ginnan, K. Comparative analysis of microleakage and seal for two obturation materials: Resilon/Epiphany and gutta-percha. J. Can. Dent. Assoc. 2006, 72, 245. [Google Scholar] [PubMed]
- Stratton, R.K.; Apicella, M.J.; Mines, P. A fluid filtration comparison of gutta-percha versus Resilon, a new soft resin endodontic obturation system. J. Endod. 2006, 32, 642–645. [Google Scholar] [CrossRef] [PubMed]
- Kurtzman, G.M. Resilon Update. Inside Dent. 2007, 3, 1–5. [Google Scholar]
- Siqueira, J.F.; Roças, I.N.; Favieri, A.; Abad, E.C.; Castro, A.J.; Gahyva, S.M. Bacterial leakage in coronally unsealed root canals obturated with 3 different techniques. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2000, 90, 647–650. [Google Scholar] [CrossRef]
- Limkangwalmongkol, S.; Burtscher, P.; Abbot, P.; Sandler, A.; Bishop, B. A comparative study of the apical leakage of four root canals sealers and laterally condensed gutta percha. J. Endod. 1991, 17, 495–499. [Google Scholar] [CrossRef]
- Swanson, K.; Madison, S. An evaluation of coronal microleakage in endodontically treated teeth. Part 1. Time periods. J. Endod. 1987, 13, 56–59. [Google Scholar] [CrossRef]
- Friedman, S.; Torneck, C.; Komorowsji, R.; Ouzounian, Z.; Syrtash, P.; Kaufman, A. In vivo model for assessing the functional efficacy of endodontic materials and techniques. J. Endod. 1997, 23, 557–561. [Google Scholar] [CrossRef]
- Torabinejad, M.; Ung, B.; Kettering, J. In vitro bacterial penetration of coronally unsealed endodontically treated teeth. J. Endod. 1990, 16, 566–569. [Google Scholar] [CrossRef]
- Shipper, G.; Trope, M. In vitro microbial leakage of endodontically treated teeth using new and standard obturation techniques. J. Endod. 2004, 30, 154–158. [Google Scholar] [CrossRef]
- Magura, M.E.; Kafrawy, A.H.; Brown, C.E.; Newton, C.W. Human saliva coronal microleakeage in obturated root canals: An in vitro study. J. Endod. 1991, 17, 324–331. [Google Scholar] [CrossRef]
- Oliver, C.; Abbott, P. An in vitro study of apical and coronal micro leakage of laterally condensed gutta-percha with Ketac-Endo and AH-26. Aust. Dent. J. 1998, 43, 262–268. [Google Scholar] [CrossRef]
- Madison, S.; Wilcox, L. An evaluation of coronal microleakge in endodontically treated teeth. Part III. In vivo study. J. Endod. 1988, 14, 455–458. [Google Scholar] [CrossRef]
- Khayat, A.; Lee, S.J.; Torabinejad, M. Human saliva penetration of coronally unsealed obturated root canals. J. Endod. 1993, 19, 458–461. [Google Scholar] [CrossRef]
- Schilder, H. Filling root canals in three dimensions. Dent. Clin. N. Am. 1967, 723–744. [Google Scholar] [CrossRef]
- Buchanan, L.S. The continuous wave of condensation technique: A convergence of conceptual and procedural advances in obturation. Dent. Today 1994, 13, 80, 82, 84–85. [Google Scholar]
- Hand, R.E.; Huget, E.F.; Tsakinis, P.J. Effects of a warm gutta-percha technique on the lateral periodontium. Oral Surg. Oral Med. Oral Pathol. 1976, 42, 395–401. [Google Scholar] [CrossRef]
- Nahmias, Y.; Mab, T.; Dovgan, J.S. The Thermo Hydraulic Condensation Technique. Oral Health 2001, 91, 11–18. [Google Scholar]
- Nahmias, Y.; Serota, K.S.; Watson, W.R., Jr. Predictable Endodontic Success: Part II—Microstructural Replication. Available online: http://www.ecoweek.ca/issues/PrinterFriendly.asp?aid=1000156065&RType=&PC=&issue=12012003 (accessed on 7 May 2021).
- Barattolo, R.; Santarcangelo, F. Otturazione del sistema dei canali radicolari con guttaperca termoplasticizzata: Principi, materiali e tecniche. G. Ital. Endod. 2011, 25, 112–124. [Google Scholar] [CrossRef] [Green Version]
- Nahmias, Y.; Mab, T.; Dovgan, J.S. La tecnica di condensazione termoidraulica. L’infor. Endod. 2002, 5, 28–33. [Google Scholar]
- Nahmias, Y.; Bery, P. Due radici palatine nei primi molari superiori. L’infor. Endod. 2007, 10, 48–51. [Google Scholar]
- Carvalho-Sousa, B.; Almeida-Gomes, F.; Carvalho, P.R.; Maníglia-Ferreira, C.; Gurgel-Filho, E.D.; Albuquerque, D.S. Filling lateral canals: Evaluation of different filling techniques. Eur. J. Dent. 2010, 4, 251–256. [Google Scholar] [CrossRef]
- Kim, S.; Kim, S.; Park, J.-W.; Jung, I.-Y.; Shin, S.-J. Comparison of the Percentage of Voids in the Canal Filling of a Calcium Silicate-Based Sealer and Gutta Percha Cones Using Two Obturation Techniques. Materials 2017, 10, 1170. [Google Scholar] [CrossRef] [Green Version]
- Chenxi, N.; Xia, L. Research progress on the effect of root canal sealers on root fracture resistance. Int. J. Stomatol. 2020, 47, 711–716. [Google Scholar] [CrossRef]
- Hryniewicz, T.; Rokosz, K. On the wear inspection and endurance recovery of Nitinol endodontic files. Pomiary Autom. Kontrola 2009, 55, 247–250. [Google Scholar]
- Hülsmann, M.; Paters, O.A.; Dummer, P.M.H. Mechanical preparation of root canals: Shaping goals, techniques and means. Endod. Top. 2005, 10, 30–76. [Google Scholar] [CrossRef]
- Hülsmann, M.; Hahn, W. Complications during root canal irrigation-literature review and case reports. Int. Endod. J. 2000, 33, 186–193. [Google Scholar] [CrossRef] [PubMed]
- Gu, Y.; Kum, K.-Y.; Perinpanayagam, H.; Kim, C.; Kum, D.J.; Lim, S.-M.; Chang, S.-W.; Baek, S.-H.; Zhu, Q.; Yoo, Y.-J. Various heat-treated nickel–titanium rotary instruments evaluated in S-shaped simulated resin canals. J. Dent. Sci. 2017, 12, 14–20. [Google Scholar] [CrossRef] [Green Version]
- Walia, H.M.; Brantley, W.A.; Gerstein, H. An initial investigation of the bending and torsional properties of Nitinol root canal files. J. Endod. 1988, 14, 346–351. [Google Scholar] [CrossRef]
- Anderson, M.E.; Price, J.H.W.; Parashos, P. Fracture resistance of electropolished rotary Nickel-Titanium endodontic instruments. J. Endod. 2007, 33, 1212–1216. [Google Scholar] [CrossRef]
- Duerig, T.; Pelton, A.; Stöckel, D. An overview of nitinol medical applications. Mater. Sci. Eng. A 1999, 273–275, 149–160. [Google Scholar] [CrossRef]
- Buehler, W.J.; Gilfrich, J.W.; Wiley, R.C. Effects of Low-Temperature Phase Changes on the Mechanical Properties of Alloys Near Composition TiNi. J. App. Phys. 1963, 34, 1475–1477. [Google Scholar] [CrossRef]
- Wang, F.E.; Buehler, W.J.; Pickart, S.J. Crystal Structure and a Unique Martensitic Transition of TiNi. J. App. Phys. 1965, 36, 3232–3239. [Google Scholar] [CrossRef]
- Metallurgy: The Alloy That Remembers. Available online: http://content.time.com/time/subscriber/article/0,33009,838687,00.html (accessed on 17 August 2021).
- Kauffman, G.B.; Mayo, I. The Story of Nitinol: The Serendipitous Discovery of the Memory Metal and Its Applications. Chem. Edu. 1997, 2, 1–21. [Google Scholar] [CrossRef]
- Withers, N. Nitinol. Available online: https://www.chemistryworld.com/podcasts/nitinol/6710article (accessed on 10 May 2021).
- Hryniewicz, T.; Rokosz, K.; Rokicki, R. Magnetoelectropolishing process improves characteristics of finished metal surfaces: Intensity of externally applied magnetic field, plus oxygen control, manipulates rate of dissolution in electropolishing. Met. Finish. 2006, 104, 26–33. [Google Scholar] [CrossRef]
- Hryniewicz, T. Wstęp do Obróbki Powierzchniowej Biomateriałów Metalowych; Wyd. Politechniki Koszalińskiej: Koszalin, Poland, 2007; pp. 1–155. [Google Scholar]
- Rokicki, R.; Hryniewicz, T. Nitinol Surface Finishing by Magnetoelectropolishing. Trans. Inst. Met. Finish. 2008, 86, 280–285. [Google Scholar] [CrossRef]
- Hryniewicz, T.; Rokicki, R.; Rokosz, K. Modifying Metallic Implants with Magnetoelectropolishing. Med. Dev. Diagn. Indust. 2008, 30, 102–111. [Google Scholar]
- Civjan, S.; Huget, E.F.; DeSimon, L.B. Potential applications of certain nickel-titanium (nitinol) alloys. J. Dent. Res. 1975, 54, 89–96. [Google Scholar] [CrossRef]
- Pawlicka, H.; Ebert, J.; Prociów, A. Systematyka rotacyjnych narzędzi niklowo-tytanowych. Czas. Stomatol. 2005, 58, 709–713. [Google Scholar]
- Product Catalog Dentsply Maillefer. Available online: https://www.maillefer.com/wp-content/uploads/2016/10/2016-Maillefer-Catalog.pdf (accessed on 31 May 2021).
- Schrader, C.; Ackermann, M.; Barbakow, F. Step-by-step description of a rotary root canals preparation technique. Int. Endod. J. 1999, 32, 312–320. [Google Scholar] [CrossRef]
- Guelzow, A.; Stamm, O.; Martus, P.; Kielbassa, A.M. Comparative study of six rotary nickel-titanium systems and hand instrumentation for root canal preparation. Int. Endod. J. 2005, 38, 743–752. [Google Scholar] [CrossRef]
- Bergmans, L.; van Cleynenbreugel, J.; Wevers, M.; Lambrechts, P. Mechanical root canal preparation with NiTi rotary instruments: Rationale, performance and safety. Status report for the American Journal of Dentistry. Am. J. Dent. 2001, 14, 324–333. [Google Scholar] [PubMed]
- Bechelli, C.; Orlandini, S.Z.; Colafranceschi, M. Scanning electron microscope study on the efficacy of root canal wall debridement of hand versus Lightspeed instrumentation. Int. Endod. J. 1999, 32, 484–493. [Google Scholar] [CrossRef] [PubMed]
- Tucker, D.M.; Wenckus, C.S.; Bentkover, S.K. Canal wall planning by engine-driven nickel-titanium instruments, compared with stainless steel hand instrumentation. J. Endod. 1997, 23, 170–173. [Google Scholar] [CrossRef]
- Zuolo, M.L.; Walton, R.E. Instrument deterioration with usage: Nickel-titanium versus stainless steel. Quint. Int. 1997, 28, 397–402. [Google Scholar]
- Tanalp, J.; Kaplan, F.; Sert, S.; Kayahan, B.; Bayirl, G. Quantitative evaluation of the amount of apically extruded debris using 3 different rotary instrumentation systems. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2006, 101, 250–257. [Google Scholar] [CrossRef]
- GT Rotary Files 20/.06 Yellow 25 mm. Available online: https://www.dentsplysirona.com/en-ca/products/endodontics/glide-path-shaping.html/Endodontics/Glide-Path-%26-Shaping/Rotary-%26-Reciprocating-Files/Shaping/GT-Rotary-Files/p/TUL-GTR0602025/c/1000671.html (accessed on 7 May 2021).
- ASTM 2063 Shape Memory Ni Ti Alloy Nitinol 55 Nitinol 60 Wire. Available online: https://www.nitinolcn.com/showroom/astm-2063-shape-memory-ni-ti-alloy-nitinol-55-nitinol-60-wire.html (accessed on 7 May 2021).
- Massalski, T.B.; Okamoto, H.; Subramanian, P.R.; Kacprzak, L. (Eds.) Binary Alloys Phase Diagrams, 2nd ed.; ASM International: Materials Park, OH, USA, 1990; Volume 3, pp. 1–2875. [Google Scholar]
- Honma, T.; Matsumoto, T.; Shugo, Y.; Nishida, M. Annual Research Report. Res. Rep. Nucl. Sci. Lab. Tohoku Univ. 1979, 12, 183–190. [Google Scholar]
- Nishida, M.; Wayman, C.M.; Honma, T. Electron microscopy studies of the Ti11Ni14 phase in an aged Ti-52.0at%Ni shape memory alloy. Scr. Metall. 1985, 19, 983–987. [Google Scholar] [CrossRef]
- Tadaki, T.; Nakata, Y.; Shimizu, K.; Otsuka, K. Crystal Structure, Composition and Morphology of a Precipitate in an Aged Ti-51 at%Ni Shape Memory Alloy. Trans. JIM 1986, 27, 731–740. [Google Scholar] [CrossRef] [Green Version]
- Saburi, T.; Nenno, S.; Fukuda, T. Crystal structure and morphology of the metastable X phase in shape memory Ti-Ni alloys. J. Less Com. Met. 1986, 125, 157–166. [Google Scholar] [CrossRef]
- Kai, W.-Y.; Chang, K.-C.; Wu, H.-F.; Chen, S.-W.; Yeh, A.-C. Formation mechanism of Ni2Ti4Ox in NITI shape memory alloy. Materialia 2019, 5, 100194. [Google Scholar] [CrossRef]
- ASTM F2063-18. Standard Specification for Wrought Nickel-Titanium Shape Memory Alloys for Medical Devices and Surgical Implants; ASTM International: West Conshohocken, PA, USA, 2018. [Google Scholar]
- Bojarski, Z.; Morawiec, H. Metale z Pamięcią Kształtu; PWN: Warszawa, Poland, 1989. [Google Scholar]
- Hanlon, J.E.; Butler, S.R.; Wasilewski, R.J. Effect of martensitic transformation on the electrical and magnetic properties of NiTi. Trans. Metall. Soc. AIME 1967, 239, 1323–1327. [Google Scholar]
- Harrison, J.D.; Hodgson, D.E. Use of TiNi in Mechanical and Electrical Connectors. In Shape Memory Effects in Alloys; Perkins, J., Ed.; Plenum Press: New York, NY, USA, 1975; pp. 517–523. [Google Scholar] [CrossRef]
- Dobrzański, L.A.; Dobrzański, L.B.; Dobrzańska, J.; Dobrzański, J.; Jung, T. Application of nitinol type alloys in teeth endodontic treatment. Processes 2021, 9, 926. [Google Scholar]
- Lin, Z.; Pike, K.; Schlun, M.; Zipse, A.; Draper, J. Nitinol Fatigue Life for Variable Strain Amplitude Fatigue. J. Mater. Eng. Perform. 2012, 21, 2628–2632. [Google Scholar] [CrossRef]
- Thompson, S.A.; Dummer, P.M. Shaping ability of Quantec Series 2000 rotary nickel-titanium instruments in simulated root canals: Part 2. Int. Endod. J. 1998, 31, 268–274. [Google Scholar] [CrossRef] [PubMed]
- Lin, Z.; Pike, K.; Zipse, A.; Schlun, M. Nitinol Fatigue Investigation on Stent-Finish Specimens Using Tension-Tension Method. J. Mater. Eng. Perform. 2011, 20, 591–596. [Google Scholar] [CrossRef]
- Rahim, M.; Frenzel, J.; Frotscher, M.; Pfetzing-Micklich, J.; Steegmüller, R.; Wohlschlögel, M.; Mughrabi, H.; Eggeler, G. Impurity levels and fatigue lives of pseudoelastic NiTi shape memory alloys. Acta Mater. 2013, 61, 3667–3686. [Google Scholar] [CrossRef]
- Urbano, M.F.; Coda, A.; Beretta, S.; Cadelli, A.; Sczerzenie, F. The Effect of Inclusions on Fatigue Properties for Nitinol. In Fatigue and Fracture Metallic Medical Materials and Devices; Mitchell, M., Smith, S., Woods, T., Berg, B., Eds.; ASTM International: West Conshohocken, PA, USA, 2013; pp. 18–34. [Google Scholar] [CrossRef]
- Robertson, S.W.; Launey, M.; Shelley, O.; Ong, I.; Vien, L.; Senthilnathan, K.; Saffari, P.; Schlegel, S.; Pelton, A.R. A statistical approach to understand the role of inclusions on the fatigue resistance of superelastic Nitinol wire and tubing. J. Mech. Behav. Biomed. Mater. 2015, 51, 119–131. [Google Scholar] [CrossRef]
- Launey, M.; Robertson, S.W.; Vien, L.; Senthilnathan, K.; Chintapalli, P.; Pelton, A.R. Influence of microstructural purity on the bending fatigue behavior of VAR-melted superelastic Nitinol. J. Mech. Behav. Biomed. Mater. 2014, 34, 181–186. [Google Scholar] [CrossRef]
- Yoneyama, T.; Doi, H.; Hamanaka, H.; Okamoto, Y.; Mogi, M.; Miura, F. Super-elasticity and thermal behavior of Ni-Ti alloy orthodontic arch wires. Dent. Mater. J. 1992, 11, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Wang, F.E.; Pickart, S.J.; Alperin, H.A. Mechanism of the TiNi martensitic transformation and the crystal structures of TiNi-II and TiNi-III phases. J. Appl. Phys. 1972, 43, 97–112. [Google Scholar] [CrossRef]
- Schäfer, E. Root canal instruments for manual use: A review. Dent. Traumatol. 1997, 13, 51–64. [Google Scholar] [CrossRef] [PubMed]
- Pelton, A.R.; Russell, S.M.; DiCello, J. The physical metallurgy of nitinol for medical applications. JOM 2003, 55, 33–37. [Google Scholar] [CrossRef]
- Hryniewicz, T.; Rokicki, R. Improved surface properties of nitinol after magnetoelectropolishing. In Proceedings of the 16th Annual International Conference on Composites/Nano-Engineering “ICCE-16”, Kunming, China, 20‒26 July 2008. [Google Scholar]
- Hryniewicz, T. Biomaterials surface improvement by magnetoelectropolishing. In Proceedings of the BIT Life Sciences’ 1st Annual World Congress of IBIO2008, New Starting Line for Decision Makers in Bioeconomy Era, Hangzhou, China, 18‒22 May 2008. [Google Scholar]
- Chekotu, J.C.; Groarke, R.; O’Toole, K.; Brabazon, D. Advances in Selective Laser Melting of Nitinol Shape Memory Alloy Part Production. Materials 2019, 12, 809. [Google Scholar] [CrossRef] [Green Version]
- Zhang, X.; Qian, M.; Zhu, X.; Shang, C.; Geng, L. Elastocaloric effects in ultra-fine grained NiTi microwires processed by cold-drawing. APL Mater. 2018, 6, 036102. [Google Scholar] [CrossRef] [Green Version]
- Świec, P.; Zubko, M.; Lekston, Z.; Stróż, D. Structure and properties of NiTi shape memory alloy after cold rolling in martensitic state. Acta Phys. Pol. A 2016, 130, 1081–1084. [Google Scholar] [CrossRef]
- Burow, J.; Frenzel, J.; Somsen, C.; Prokofiev, E.; Valiev, R.; Eggeler, G. Grain nucleation and growth in deformed NiTi shape memory alloys: An in situ TEM study. Shap. Mem. Superelast. 2017, 3, 347–360. [Google Scholar] [CrossRef]
- Tong, Y.X.; Hu, K.P.; Chen, F.; Tian, B.; Li, L.; Zheng, Y.F. Multiple-stage transformation behavior of Ti49.2Ni50.8 alloy with different initial microstructure processed by equal channel angular pressing. Intermetallics 2017, 85, 163–169. [Google Scholar] [CrossRef]
- Wang, X.; Kustov, S.; Verlinden, B.; Van Humbeeck, J. Fundamental development on utilizing the R-phase transformation in NiTi shape memory alloys. Shap. Mem. Superelast. 2015, 1, 231–239. [Google Scholar] [CrossRef] [Green Version]
- Shamimi, A.; Amin-Ahmadi, B.; Stebner, A.; Duerig, T. The effect of low temperature aging and the evolution of R-phase in Ni-rich NiTi. Shap. Mem. Superelast. 2018, 4, 417–427. [Google Scholar] [CrossRef]
- Wang, Z.; Everaerts, J.; Salvati, E.; Korsunsky, A.M. Evolution of thermal and mechanical properties of Nitinol wire as a function of ageing treatment conditions. J. Alloys Compd. 2020, 819, 153024. [Google Scholar] [CrossRef]
- Chad Hornbuckle, B.; Yu, X.X.; Noebe, R.D.; Martens, R.; Weaver, M.L.; Thompson, G.B. Hardening behavior and phase decomposition in very Ni-rich Nitinol alloys. Mater. Sci. Eng. A 2015, 639, 336–344. [Google Scholar] [CrossRef]
- Velmurugan, C.; Senthilkumar, V.; Dinesh, S.; Arulkirubakaran, D. Review on phase transformation behavior of NiTi shape memory alloys. Mater. Today Proc. 2018, 5, 14597–14606. [Google Scholar] [CrossRef]
- Liang, X.; Xiao, F.; Chen, H.; Li, Z.; Li, Z.; Jin, X.; Fukuda, T. Internal friction of the R-phase in single crystalline Ti-50.8Ni (at.%) alloy containing controlled precipitate of Ti3Ni4. Scr. Mater. 2019, 166, 44–47. [Google Scholar] [CrossRef]
- Pourbabak, S.; Orekhov, A.; Samaee, V.; Verlinden, B.; Van Humbeeck, J.; Schryvers, D. In-Situ TEM stress induced martensitic transformation in Ni50.8Ti49.2 microwires. Shap. Mem. Superelast. 2019, 5, 154–162. [Google Scholar] [CrossRef]
- Gurley, A.; Lambert, T.R.; Beale, D.; Broughton, R. Dual measurement self-sensing technique of NiTi actuators for use in robust control. Smart Mater. Struct. 2017, 26, 105050. [Google Scholar] [CrossRef]
- Dilibal, S.; Sahin, H.; Dursun, E.; Engeberg, E.D. Nickel–titanium shape memory alloy-actuated thermal overload relay system design. Electr. Eng. 2017, 99, 923–930. [Google Scholar] [CrossRef]
- Mehrpouya, M.; Gisario, A.; Broggiato, G.B.; Puopolo, M.; Vesco, S.; Barletta, M. Effect of welding parameters on functionality of dissimilar laser-welded NiTi superelastic (SE) to shape memory effect (SME) wires. Int. J. Adv. Manuf. Technol. 2019, 103, 1593–1601. [Google Scholar] [CrossRef]
- Casati, R.; Saghafi, F.; Biffi, C.A.; Vedani, M.; Tuissi, A. Improved functional properties and efficiencies of nitinol wires under high-performance shape memory effect (HP-SME). J. Mater. Eng. Perform. 2017, 26, 4964–4969. [Google Scholar] [CrossRef]
- Dobrzański, L.A. Metale i ich Stopy. In Open Access Library VII(2); Dobrzański, L.A., Ed.; International OCSCO World Press: Gliwice, Poland, 2017; pp. 1–982. [Google Scholar]
- Fan, G.; Chen, W.; Yang, S.; Zhu, J.; Ren, X.; Otsuka, K. Origin of abnormal multi-stage martensitic transformation behavior in aged Ni-rich Ti–Ni shape memory alloys. Acta Mater. 2004, 52, 4351–4362. [Google Scholar] [CrossRef]
- Otsuka, K.; Ren, X. Physical Metallurgy of Ti-Ni-based Shape Memory Alloys. Prog. Mater. Sci. 2005, 50, 511–678. [Google Scholar] [CrossRef]
- Chluba, C.; Ge, W.; Lima de Miranda, R.; Strobel, J.; Kienle, L.; Quandt, E.; Wuttig, M. Shape memory alloys. Ultralow-fatigue shape memory alloy films. Science 2015, 348, 1004–1007. [Google Scholar] [CrossRef]
- Spini, T.S.; Valarelli, F.P.; Cançado, R.H.; Freitas, K.M.; Villarinho, D.J. Transition temperature range of thermally activated nickel-titanium archwires. J. Appl. Oral. Sci. 2014, 22, 109–117. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Funakubo, H. Shape Memory Alloys; University of Tokyo: Tokyo, Japan, 1984; p. 7. [Google Scholar]
- Sadiq, H.; Wong, M.B.; Al-Mahaidi, R.; Zhao, X.L. The effects of heat treatment on the recovery stresses of shape memory alloys. Smart Mater. Struct. 2010, 19, 035021. [Google Scholar] [CrossRef]
- ASTM E8/E8M-21. Standard Test. Methods for Tension Testing of Metallic Materials; ASTM International: West Conshohocken, PA, USA, 2021. [Google Scholar]
- Ren, X.; Miura, N.; Taniwaki, K.; Otsuka, K.; Suzuki, T.; Tanaka, K.; Chumlyakov, Yu.I.; Asai, M. Understanding the martensitic transformations in TiNi-based alloys by elastic constants measurement. Mater. Sci. Eng. A 1999, 273–275, 190–194. [Google Scholar] [CrossRef]
- Wang, X.; VerlinDen, B.; Kustov, S. Multi-stage martensitic transformation in Ni-rich NiTi shape memory alloys. Funct. Mater. Lett. 2017, 10, 1–8. [Google Scholar] [CrossRef]
- Fan, G.; Zhou, Y.; Chen, W.; Yang, S.; Ren, X.; Otsuka, K. Precipitation kinetics of Ti3Ni4 in polycrystalline Ni-rich TiNi alloys and its relation to abnormal multi-stage transformation behavior. Mater. Sci. Eng. A 2006, 438–440, 622–626. [Google Scholar] [CrossRef]
- Nishida, M.; Wayman, C.M.; Kainuma, R.; Honma, T. Further electron microscopy studies of the Ti11Ni14 phase in an aged Ti-52at%Ni shape memory alloy. Scr. Metall. 1986, 20, 899–904. [Google Scholar] [CrossRef]
- Nishida, M.; Wayman, C.M.; Honma, T. Precipitation processes in near-equiatomic TiNi shape memory alloys. Metall. Mater. Trans. A 1986, 17, 1505–1515. [Google Scholar] [CrossRef]
- Khalil-Allafi, J.; Eggeler, G.; Dlouhy, A.; Schmahl, WW.; Somsen, C.H. On the influence of heterogeneous precipitation on martensitic transformations in a Ni-rich NiTi shape memory alloy. Mater. Sci. Eng. A 2004, 378, 148–151. [Google Scholar] [CrossRef]
- Liu, S.; Zhu, J.; Lin, X.; Wang, X.; Wang, G. Coupling effect of stretch-bending deformation and electric pulse treatment on phase transformation behavior and superelasticity of a Ti-50.8 at.% Ni alloy. Mater. Sci. Eng. A 2021, 799, 140164. [Google Scholar] [CrossRef]
- Hirsch, P.; Howie, A.; Nicholson, R.B.; Pashley, D.W.; Whelan, M.J. Electron Microscopy of Thin Crystals, 2nd ed.; Krieger Publishing Company: Malabar, FL, USA, 1977; pp. 169, 317. [Google Scholar]
- Honma, T. The effect of aging, on the spontaneous shape change and the all-round shape memory effect in Ni-rich TiNi alloy. In Proceedings of the International Conference on Martensitic Transformations ICOMAT-86, Nara, Japan, 26–30 August 1986; pp. 709–716. [Google Scholar]
- Kainuma, R.; Matsumoto, M.; Honma, T. The mechanism of the all-round shape memory effect in a Ni-rich TiNi alloy. In Proceedings of the International Conference on Martensitic Transformations ICOMAT-86, Nara, Japan, 26–30 August 1986; pp. 717–722. [Google Scholar]
- Koskimaki, D.; Marcinkowski, M.J.; Sastri, A.S. Solid State Diffusional Transformations in the Near Equiatomic Ni-Ti Alloys. Trans. Metall. Soc. AIME 1969, 245, 1883–1890. [Google Scholar]
- Chen, Q.; Wu, X.F.; Ko, T. The effects of Ti3Ni4 precipitates on the R-phase transformation. Scr. Metall. Mater. 1993, 29, 49–53. [Google Scholar] [CrossRef]
- Xie, C.Y.; Zhao, L.C.; Lei, T.C. Effect of precipitates on the electrical resistivity-temperature curves in an aged Ti-51.8 at % Ni shape memory alloy. Scr. Metall. 1989, 23, 2131–2136. [Google Scholar] [CrossRef]
- Xie, C.Y.; Zhao, L.C.; Lei, T.C. Effect of Ti3Ni4 precipitates on the phase transitions in an aged Ti-51.8at% Ni shape memory alloy. Scr. Metall. Mater. 1990, 24, 1753–1758. [Google Scholar] [CrossRef]
- Khalil-Allafi, J.; Ren, X.; Eggeler, G. The mechanism of multistage martensitic transformations in aged Ni-rich NiTi shape memory alloys. Acta Mater. 2002, 50, 793–803. [Google Scholar] [CrossRef]
- Zou, W.H.; Han, X.D.; Wang, R.; Zhang, Z.; Zhang, W.-Z.; Lai, J.K.L. TEM and HREM study of the interphase interface structure of Ti3Ni4 precipitates and parent phase in an aged TiNi shape memory alloy. Mater. Sci. Eng. A 1996, 219, 142–147. [Google Scholar] [CrossRef]
- Van Humbeeck, J. Non-medical applications of shape memory alloys. Mater. Sci. Eng. A 1999, 273–275, 134–148. [Google Scholar] [CrossRef]
- Wang, X.; Li, K.; Schryvers, D.; Verlinden, B.; Van Humbeeck, J. R-phase transition and related mechanical properties controlled by low-temperature aging treatment in a Ti–50.8at.% Ni thin wire. Scr. Mater. 2014, 72‒73, 21–24. [Google Scholar] [CrossRef]
- Dautovich, D.P.; Purdy, G.R. Phase Transformations in TiNi. Canad. Metall. Quart. 1965, 4, 129–143. [Google Scholar] [CrossRef]
- Miyazaki, S.; Otsuka, K. Deformation and transition behavior associated with the R-phase in Ti-Ni alloys. Metall. Mater. Trans. A 1986, 17, 53–63. [Google Scholar] [CrossRef]
- Miyazaki, S.; Kimura, S.; Otsuka, K. Shape-memory effect and pseudoelasticity associated with the R-phase transition in Ti-50·5 at.% Ni single crystals. Philos. Mag. A 1988, 57, 467–478. [Google Scholar] [CrossRef]
- Hara, T.; Ohba, T.; Okunishi, E.; Otsuka, K. Structural Study of R-Phase in Ti-50.23 at.%Ni and Ti-47.75 at.%Ni-1.50 at.%Fe Alloys. Mater. Trans. JIM 1997, 38, 11–17. [Google Scholar] [CrossRef] [Green Version]
- Tirry, W.; Schryvers, D. Quantitative determination of strain fields around Ni4Ti3 precipitates in NiTi. Acta Mater. 2005, 53, 1041–1049. [Google Scholar] [CrossRef]
- Karaca, H.E.; Kaya, I.; Tobe, H.; Basaran, B.; Nagasako, M.; Kainuma, R.; Chumlyakov, Y. Shape memory behavior of high strength Ni54Ti46 alloys. Mater. Sci. Eng. A 2013, 580, 66–70. [Google Scholar] [CrossRef]
- Wang, X.; Li, C.; Verlinden, B.; Van Humbeeck, J. Effect of grain size on aging microstructure as reflected in the transformation behavior of a low-temperature aged Ti–50.8 at.% Ni alloy. Scr. Mater. 2013, 69, 545–548. [Google Scholar] [CrossRef]
- Šittner, P.; Landa, M.; Lukáš, P.; Novák, V. R-phase transformation phenomena in thermomechanically loaded NiTi polycrystals. Mech. Mater. 2006, 38, 475–492. [Google Scholar] [CrossRef]
- Ha, J.H.; Kim, S.K.; Cohenca, N.; Kim, H.C. Effect of R-phase heat treatment on torsional resistance and cyclic fatigue fracture. J. Endod. 2013, 39, 389–393. [Google Scholar] [CrossRef]
- Pelton, A.R.; Huang, G.H.; Moine, P.; Sinclair, R. Effects of thermal cycling on microstructure and properties in Nitinol. Mater. Sci. Eng. A 2012, 532, 130–138. [Google Scholar] [CrossRef]
- Tobushi, H.; Yamada, S.; Hachisuka, T.; Ikai, A.; Tanaka, K. Thermomechanical properties due to martensitic and R-phase transformations of TiNi shape memory alloy subjected to cyclic loadings. Smart Mater. Struct. 1996, 5, 788. [Google Scholar] [CrossRef]
- Uchil, J.; Kumara, K.G.; Mahesh, K.K. Effect of thermal cycling on R-phase stability in a NiTi shape memory alloy. Mater. Sci. Eng. A 2002, 332, 25–28. [Google Scholar] [CrossRef]
- Miyazaki, S.; Igo, Y.; Otsuka, K. Effect of thermal cycling on the transformation temperatures of Ti-Ni alloys. Acta Metall. 1986, 34, 2045–2051. [Google Scholar] [CrossRef]
- Tobushi, H.; Kimura, K.; Sawada, T.; Hattori, T.; Lin, P.H. Recovery Stress Associated with R-Phase Transformation in TiNi Shape Memory Alloy: Properties under Constant Residual Strain. JSME Int. J. A 1994, 37, 138–142. [Google Scholar] [CrossRef] [Green Version]
- Miyazaki, S.; Otsuka, K. Mechanical behaviour associated with the premartensitic rhombohedral-phase transition in a Ti50Ni47Fe3 alloy. Philos. Mag. A 1985, 50, 393–408. [Google Scholar] [CrossRef]
- Huang, X.; Liu, Y. Effect of annealing on the transformation behavior and superelasticity of NiTi shape memory alloy. Scr. Mater. 2001, 45, 153–160. [Google Scholar] [CrossRef]
- Gall, K.; Tyber, J.; Wilkesanders, G.; Robertson, S.W.; Ritchie, R.O.; Maier, H.J. Effect of microstructure on the fatigue of hot-rolled and cold-drawn NiTi shape memory alloys. Mater. Sci. Eng. A 2008, 486, 389–403. [Google Scholar] [CrossRef]
- Nishida, M.; Wayman, C.M. Electron microscopy studies of the “Premartensitic” transformations in an aged Ti-51 at%Ni shape memory alloy. Metallography 1988, 21, 255–273. [Google Scholar] [CrossRef]
- Favier, D.; Liu, Y.; McCormick, P.G. Three stage transformation behaviour in aged NiTi. Scr. Metall. Mater. 1993, 28, 669–672. [Google Scholar] [CrossRef]
- Liu, X.; Wang, Y.; Yang, D.; Qi, M. The effect of ageing treatment on shape-setting and superelasticity of a nitinol stent. Mater. Charact. 2008, 59, 402–406. [Google Scholar] [CrossRef]
- Matsumoto, H. Appearance of an intermediate phase with thermal cycling on the transformation of NiTi. J. Mater. Sci. Lett. 1991, 10, 408–410. [Google Scholar] [CrossRef]
- Matsumoto, H. Transformation behaviour with thermal cycling in NiTi alloys. J. Alloys Compd. 2003, 350, 213–217. [Google Scholar] [CrossRef]
- Dilibal, S.; Hamilton, R.F.; Lanba, A. The effect of employed loading mode on the mechanical cyclic stabilization of NiTi shape memory alloys. Intermetallics 2017, 89, 1–9. [Google Scholar] [CrossRef]
- Piekielny, M.; Jarmołowicz, M.; Dobrzyński, M. Odporność na cykliczne zmęczenie wybranych endodontycznych narzędzi maszynowych w świetle piśmiennictwa. Inż. Fiz. Med. 2020, 9, 143–144. [Google Scholar]
- Cao, S.; Nishida, M.; Schryvers, D. Quantitative three-dimensional analysis of Ni4Ti3 precipitate morphology and distribution in polycrystalline Ni-Ti. Acta Mater. 2011, 59, 1780–1789. [Google Scholar] [CrossRef]
- Xue, D.; Zhou, Y.; Ren, X. The effect of ageing on the B2-R transformation behaviors in Ti-51at%Ni alloy. Intermetallics 2011, 19, 1752–1758. [Google Scholar] [CrossRef]
- Jordan, L.; Chandrasekaran, M.; Masse, M.M.; Bouquet, G. Study of the phase transformation in Ni-Ti based shape memory alloys. J. Phys. IV Fr. 1995, 5, C2-489–C2-494. [Google Scholar] [CrossRef] [Green Version]
- Khalil-Allafi, J.; Eggeler, G.; Schmahl, W.W. Quantitative phase analysis in microstructures which display multiple step martensitic transformations in Ni-rich NiTi shape memory alloys. Mater. Sci. Eng. A 2006, 438‒440, 593–596. [Google Scholar] [CrossRef]
- Pushin, V.G.; Stolyarov, V.V.; Valiev, R.Z.; Lowe, T.C.; Zhu, Y.T. Nanostructured TiNi based shape memory alloys processed by severe plastic deformation. Mater. Sci. Eng. 2005, 410–411, 386–389. [Google Scholar] [CrossRef]
- Moon, H.-J.; Chun, S.-J.; Liu, Y.; Yang, H.; Kim, Y.-W.; Nam, T.-H. Effect of alloy composition on the B2–R transformation in rapidly solidified Ti–Ni alloys. J. Alloys Compd. 2013, 577, S259–S264. [Google Scholar] [CrossRef]
- Kim, J.I.; Liu, Y.; Miyazaki, S. Ageing-induced two-stage R-phase transformation in Ti—50.9at.%Ni. Acta Mater. 2004, 52, 487–499. [Google Scholar] [CrossRef]
- Rapisarda, E.; Bonaccorso, A.; Tripi, T.R.; Condorelli, G.G. Effect of sterilization on the cutting efficiency of rotary nickel-titanium endodontic files. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 1999, 88, 343–347. [Google Scholar] [CrossRef]
- Plotino, G.; Costanzo, A.; Grande, N.M.; Petrovic, R.; Testarelli, L.; Gambarini, G. Experimental Evaluation on the Influence of Autoclave Sterilization on the Cyclic Fatigue of New Nickel-Titanium Rotary Instruments. J. Endod. 2012, 38, 222–225. [Google Scholar] [CrossRef]
- la Chapelle, C.F.; Veersema, S.; Brölmann, H.A.M.; Jansen, F.W. Effectiveness and feasibility of hysteroscopic sterilization techniques: A systematic review and meta-analysis. Fertil. Steril. 2015, 103, 1516–1525.e3. [Google Scholar] [CrossRef]
- Dioguardi, M.; Laneve, E.; Di Cosola, M.; Cazzolla, A.P.; Sovereto, D.; Aiuto, R.; Laino, L.; Leanza, T.; Alovisi, M.; Troiano, G.; et al. The Effects of Sterilization Procedures on the Cutting Efficiency of Endodontic Instruments: A Systematic Review and Network Meta-Analysis. Materials 2021, 14, 1559. [Google Scholar] [CrossRef] [PubMed]
- Schafer, E. Effect of sterilization on the cutting efficiency of PVD-coated nickel-titanium endodontic instruments. Int. Endod. J. 2002, 35, 867–872. [Google Scholar] [CrossRef] [PubMed]
- Seago, S.T.; Bergeron, B.E.; Kirkpatrick, T.C.; Roberts, M.D.; Roberts, H.W.; Himel, V.T.; Sabey, K.A. Effect of Repeated Simulated Clinical Use and Sterilization on the Cutting Efficiency and Flexibility of Hyflex CM Nickel-Titanium Rotary Files. J. Endod. 2015, 41, 725–728. [Google Scholar] [CrossRef] [PubMed]
- Haïkel, Y.; Serfaty, R.; Wilson, P.; Speisser, J.M.; Allemann, C. Cutting efficiency of nickel-titanium endodontic instruments and the effect of sodium hypochlorite treatment. J. Endod. 1998, 24, 736–739. [Google Scholar] [CrossRef]
- Neal, R.G.; Craig, R.G.; Powers, J.M. Effect of sterilization and irrigants on the cutting ability of stainless steel files. J. Endod. 1983, 9, 93–96. [Google Scholar] [CrossRef]
- Morrison, S.W.; Newton, C.W.; Brown, C.E. The effects of steam sterilization and usage on cutting efficiency of endodontic instruments. J. Endod. 1989, 15, 427–431. [Google Scholar] [CrossRef]
- Haïkel, Y.; Serfaty, R.; Lwin, T.T.; Allemann, C. Measurement of the cutting efficiency of endodontic instruments: A new concept. J. Endod. 1996, 22, 651–656. [Google Scholar] [CrossRef]
- Webber, J.; Moser, J.B.; Heuer, M.A. A method to determine the cutting efficiency of root canal instruments in linear motion. J. Endod. 1980, 6, 829–834. [Google Scholar] [CrossRef]
- Villalobos, R.L.; Moser, J.B.; Heuer, M.A. A method to determine the cutting efficiency of root canal instruments in rotary motion. J. Endod. 1980, 6, 667–671. [Google Scholar] [CrossRef]
- Molven, O. A comparison of the dentin-removing ability of five root canal instruments. Scand. J. Dent. Res. 1970, 78, 500–511. [Google Scholar] [CrossRef] [PubMed]
- Oliet, S.; Sorin, S.M. Cutting efficiency of endodontic reamers. Oral Surg. Oral Med. Oral Pathol. 1973, 36, 243–252. [Google Scholar] [CrossRef]
- Fromme, H.G.; Riedel, H. Treatment of Dental Root Canals and the Marginal Contact between Filling Material and Tooth, studied by Scanning Electronic Microscopy. Int. Endod. J. 1972, 6, 17–20. [Google Scholar] [CrossRef] [PubMed]
- Stefanescu, T.; Popovici, R.A.; Antoniac, I.V.; Galuscan, A.; Tirca, T. Ni-Ti Rotary Instrument Fracture Analysis after Clinical Use. Structure Changes in Used Instruments. Environ. Eng. Manag. J. 2016, 15, 981–988. [Google Scholar] [CrossRef]
- Matei, A.; Pencea, I.; Stanciu, S.; Hristu, R.; Antoniac, I.; Coman, E.C.; Sfat, C.; Stanciu, G. Structural characterization and adhesion appraisal of TiN and TiCN coatings deposited by CAE-PVD technique on a new carbide composite cutting tool. J. Adhes. Sci. Technol. 2015, 29, 2576–2589. [Google Scholar] [CrossRef]
- Inan, U.; Keskin, C. Torsional Resistance of ProGlider, Hyflex EDM, and One G Glide Path Instruments. J. Endod. 2019, 45, 1253–1257. [Google Scholar] [CrossRef]
- Spagnuolo, G.; Ametrano, G.; d’Antò, V.; Rengo, C.; Simeone, M.; Riccitiello, F.; Amato, M. Effect of autoclaving on the surfaces of TiN-coated and conventional nickel-titanium rotary instruments. Int. Endod. J. 2012, 45, 1148–1155. [Google Scholar] [CrossRef]
- Razavian, H.; Iranmanesh, P.; Mojtahedi, H.; Nazeri, R. Effect of Autoclave Cycles on Surface Characteristics of S-File Evaluated by Scanning Electron Microscopy. Iran. Endod. J. 2015, 11, 29–32. [Google Scholar] [CrossRef]
- Nair, A.S.; Tilakchand, M.; Naik, B.D. The effect of multiple autoclave cycles on the surface of rotary nickel-titanium endodontic files: An in vitro atomic force microscopy investigation. J. Conserv. Dent. 2015, 18, 218–222. [Google Scholar]
- Fayyad, D.M.; Elgendy, A.A.E. Cutting Efficiency of Twisted versus Machined Nickel-Titanium Endodontic Files. J. Endod. 2011, 37, 1143–1146. [Google Scholar] [CrossRef]
- Hilt, B.R.; Cunningham, C.J.; Shen, C.; Richards, N. Torsional Properties of Stainless-Steel and Nickel-Titanium Files After Multiple Autoclave Sterilizations. J. Endod. 2000, 26, 76–80. [Google Scholar] [CrossRef] [PubMed]
- Siqueira, J.F.; Rôcas, I.N.; Favieri, A.; Lima, K.C. Chemomechanical reduction of the bacterial population in the root canal instrumentation and irrigation with 1%,2,5% and 5,25% sodium hypochlorite. J. Endod. 2000, 26, 331–334. [Google Scholar] [CrossRef] [PubMed]
- Saleh, A.A.; Ettaman, W.M. Effect of endodontic irrigation solutions on microhardness of root canal dentine. J. Dent. 1999, 27, 43–46. [Google Scholar] [CrossRef]
- Walsh, L.J.; George, R. Activation of Alkaline Irrigation Fluids in Endodontics. Materials 2017, 10, 1214. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sim, T.P.; Knowles, J.C.; Ng, Y.L.; Shelton, J.; Gulabivala, K. Effect of sodium hypochlorite on mechanical properties of dentine and tooth surface strain. Int. Endod. J. 2001, 34, 120–132. [Google Scholar] [CrossRef]
- Hart, J.R. Ethylenediaminetetraacetic Acid and Related Chelating Agents. In Ullmann’s Encyclopedia of Industrial Chemistry; Ullmann, F., Ed.; Wiley-VCH: Weinheim, Germany, 2000. [Google Scholar] [CrossRef]
- Wujec, P.; Pawlicka, H. Standardowe środki płuczące polecane w leczeniu endodontycznym—Przegląd piśmiennictwa. Dent. Med. Probl. 2008, 45, 466–472. [Google Scholar]
- Heling, I.; Irani, E.; Karni, S.; Steinberg, D. In vitro antimicrobial effect of RC-Prep within dentinal tubules. J. Endod. 1999, 25, 782–785. [Google Scholar] [CrossRef]
- Morris, M.D.; Lee, K.W.; Bouillaguet, S.; Pashley, D.H. Effects of sodium hypochlorite and RC-Prep on bond strenghts of resin cement to endodontic surfaces. J. Endod. 2001, 27, 753–757. [Google Scholar] [CrossRef] [PubMed]
- Wu, M.K.; Wesselink, P.R. A primary observation on the preparation and obturation of oval canals. Int. Endod. J. 2001, 34, 137–141. [Google Scholar] [CrossRef] [Green Version]
- Peters, L.B.; Wesselink, P.R.; Moorer, W.R. The fate and the role of bacteria left in root dentinal tubules. Int. Endod. J. 1995, 28, 95–99. [Google Scholar] [CrossRef] [PubMed]
- Shahi, S.; Zand, V.; Oskoee, S.S.; Abdolrahimi, M.; Rahnema, A.H. An in vitro study of the effect of spreader penetration depth and apical microleakage. J. Oral Sci. 2007, 49, 283–286. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Silva, D.; Endal, U.; Reynaud, A.; Portenier, I.; Ǿstravik, D.; Haapasalo, M. A comparative study of lateral condensation, heat-softened gutta-percha and modified master cone heat-softened backfilling technique. Int. Endod. J. 2002, 35, 1005–1111. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, B.A.; Baumgartner, J.C. Spreader penetration during lateral compaction of resilon and gutta-percha. J. Endod. 2006, 32, 52–54. [Google Scholar] [CrossRef] [PubMed]
- Johnson, W.B. A new gutta-percha technique. J. Endod. 1978, 4, 184–188. [Google Scholar] [CrossRef]
- Tani-Ishii, N.; Teranka, T. Clinical and radiographic evaluation of root-canal obturation with Obtura II. J. Endod. 2003, 29, 739–742. [Google Scholar] [CrossRef]
- Goldberg, F.; Artaza, L.P.; De Silvio, A. Effectiveness of different obturation techniques in the filling of simulated lateral canals. J. Endod. 2001, 27, 362–364. [Google Scholar] [CrossRef] [PubMed]
- De Deus, G.; Gurgel-Filho, E.D.; Magalhaes, K.M.; Countinho-Filho, T. A laboratory of gutta-percha filled area obtained using Thermafil, System B and Lateral condensation. Int. Endod. J. 2006, 39, 378–383. [Google Scholar] [CrossRef] [PubMed]
- Pawińska, M.; Kierklo, A. Ocena jakości wypełnień kanałowych w aspekcie przylegania i szczelności na podstawie obrazów mikroskopowych SEM. Czas. Stomatol. 2009, 62, 5–13. [Google Scholar]
- Buchanan, S.L. The continuous wave of obturation technique: “Centered” condensation of warm gutta-percha in 12 seconds. Dent. Today 1996, 15, 60–67. [Google Scholar]
- Bugea, C. Continuous Wave of Condensation. Available online: http://endodontics.styleitaliano.org/continuous-wave-of-condensation/ (accessed on 17 May 2021).
- Barbosa, F.O.G.; Gusman, H.; Pimenta de Araujo, M.C. A comparative study on the frequency location and direction of accessory canals filled with the hydraulic vertical condensation and continuous wave of condensation techniques. J. Endod. 2009, 35, 397–400. [Google Scholar] [CrossRef]
- Nahmias, Y.; Mab, T.; Dovgan, J.S. The Thermo-Hydraulic Condensation Technique. Available online: https://www.endoexperience.com/documents/YTHTTechnique2001.pdf (accessed on 17 May 2021).
- DuLac, K.A.; Nielsen, C.J.; Tomazic, T.J.; Ferrillo, P.J.; Hatton, J.F. Comparison of the obturation of lateral canals by six techniques. J. Endod. 1999, 25, 376–380. [Google Scholar] [CrossRef]
- Cassai, E. THERMAFIL: The Technique Step by Step. Available online: http://endodontics.styleitaliano.org/thermafil-the-technique-step-by-step/ (accessed on 17 May 2021).
- Faus-Llácer, V.; Pérez, R.L.; Faus-Matoses, I.; Ruiz-Sánchez, C.; Zubizarreta-Macho, Á.; Sauro, S.; Faus-Matoses, V. Efficacy of Removing Thermafil and GuttaCore from Straight Root Canal Systems Using a Novel Non-Surgical Root Canal Re-Treatment System: A Micro-Computed Tomography Analysis. J. Clin. Med. 2021, 10, 1266. [Google Scholar] [CrossRef]
- Lipski, M.; Lichota, D.; Woźniak, K. Evaluation of the controlled placement of Thermafil obturators. In Proceedings of the 9th Biennial Congress of the European Society of Endodontology, Zagreb, Croatia, 7–9 October 1999. [Google Scholar]
- Namazikhah, S.; Shirani, R.; Mohseni, A.; Farsio, F. Dye leakage study: Comparing conventional and new techniques. J. Calif. Dent. Assoc. 2000, 28, 435–442. [Google Scholar] [PubMed]
- Juhlin, J.J.; Walton, R.E.; Dorgan, J.S. Adaptation of Thermafil components to canal walls. J. Endod. 1993, 19, 130–135. [Google Scholar] [CrossRef]
- Gutman, J.L.; Sounders, W.P.; Saunders, E.M.; Nguyen, L. An assessment of the plastic Thermafil obturation technique Part I, Radiographic evaluation of adaptation and placement. Int. Endod. J. 1993, 26, 173–178. [Google Scholar] [CrossRef]
- Dobrzański, L.A.; Dobrzański, L.B.; Dobrzańska-Danikiewicz, A.D. Overview of conventional technologies using the powders of metals, their alloys and ceramics in Industry 4.0 stage. J. Achiev. Mater. Manuf. Eng. 2020, 98, 56–85. [Google Scholar] [CrossRef]
- Dobrzański, L.A. Role of materials design in maintenance engineering in the context of industry 4.0 idea. J. Achiev. Mater. Manuf. Eng. 2019, 96, 12–49. [Google Scholar] [CrossRef]
- Dobrzański, L.A.; Dobrzańska-Danikiewicz, A.D. Applications of Laser Processing of Materials in Surface Engineering in the Industry 4.0 Stage of the Industrial Revolution. Mater. Perform. Charact. 2019, 8, 1091–1129. [Google Scholar] [CrossRef]
- Dobrzański, L.A.; Dobrzańska-Danikiewicz, A.D. Why Are Carbon-Based Materials Important in Civilization Progress and Especially in the Industry 4.0 Stage of the Industrial Revolution. Mater. Perform. Charact. 2019, 8, 337–370. [Google Scholar] [CrossRef]
- Dobrzański, L.A.; Dobrzański, L.B.; Dobrzańska-Danikiewicz, A.D.; Kraszewska, M. Manufacturing powders of metals, their alloys and ceramics and the importance of conventional and additive technologies for products manufacturing in Industry 4.0 stage. Arch. Mater. Sci. Eng. 2020, 102, 13–41. [Google Scholar] [CrossRef]
- Hermann, M.; Pentek, T.; Otto, B. Design Principles for Industrie 4.0 Scenarios: A Literature Review; Technische Universität Dortmund: Dortmund, Germany, 2015. [Google Scholar]
- Kagermann, H.; Wahlster, W.; Helbig, J. Recommendations for Implementing the Strategic Initiative INDUSTRIE 4.0: Final Report of the Industrie 4.0 Working Group; Federal Ministry of Education and Research: Bonn, Germany, 2013.
- Rüßmann, M.; Lorenz, M.; Gerbert, P.; Waldner, M.; Justus, J.; Engel, P.; Harnisch, M. Industry 4.0: The Future of Productivity and Growth in Manufacturing Industries; Boston Consulting Group: Boston, MA, USA, 2015. [Google Scholar]
- Kagermann, H. Chancen von Industrie 4.0 Nutzen. In: Industrie 4.0 in Produktion, Automatisierung und Logistik; Springer Fachmedien Wiesbaden: Wiesbaden, Germany, 2014; pp. 603–614. [Google Scholar]
- Lee, J.; Kao, H.-A.; Yang, S. Service Innovation and Smart Analytics for Industry 4.0 and Big Data Environment. Proc. CIRP 2014, 16, 3–8. [Google Scholar] [CrossRef] [Green Version]
- Jose, R.; Ramakrishna, S. Materials 4.0: Materials Big Data Enabled Materials Discovery. Appl. Mat. Today 2018, 10, 127–132. [Google Scholar] [CrossRef]
- Brettel, M.; Friederichsen, N.; Keller, M.; Rosenberg, M. How Virtualization, Decentralization, and Network-Building Change the Manufacturing Landscape: An Industry 4.0 Perspective. Int. J. Mech. Aerospac. Indust. Mechatron. Manuf. Eng. 2014, 8, 37–44. [Google Scholar]
- Tay, S.I.; Lee, T.C.; Hamid, N.A.A.; Ahmad, A.N.A. An Overview of Industry 4.0: Definition, Components, and Government Initiatives. J. Adv. Res. Dynamic Control Syst. 2018, 10, 1379–1387. [Google Scholar]
- Xu, X. Machine Tool 4.0 for the New Era of Manufacturing. Int. J. Adv. Manuf. Techn. 2017, 92, 1893–1900. [Google Scholar] [CrossRef]
- Sipsas, K.; Alexopoulos, K.; Xanthakis, V.; Chryssolouris, G. Collaborative Maintenance in Flow-Line Manufacturing Environments: An Industry 4.0 Approach. Proc. CIRP 2016, 55, 236–241. [Google Scholar] [CrossRef] [Green Version]
- Hozdic, E. Smart Factory for Industry 4.0: A Review. Int. J. Modern Manuf. Tech. 2015, 7, 28–35. [Google Scholar]
- Zhong, R.Y.; Xu, X.; Klotz, E.; Newman, S.T. Intelligent Manufacturing in the Context of Industry 4.0: A Review. Engineering 2017, 3, 616–630. [Google Scholar] [CrossRef]
- Bahrin, M.A.K.; Othman, M.F.; Azli, N.H.N.; Talib, M.F. Industry 4.0: A Review on Industrial Automation and Robotic. J. Tekno 2016, 78, 137–143. [Google Scholar] [CrossRef] [Green Version]
- Vaidya, S.; Ambad, P.; Bhosle, S. Industry 4.0—A Glimpse. Proc. Manuf. 2018, 20, 233–238. [Google Scholar] [CrossRef]
- Lee, J.; Bagheri, B.; Kao, H.-A. A Cyber-Physical Systems Architecture for Industry 4.0-Based Manufacturing Systems. Manuf. Lett. 2015, 3, 18–23. [Google Scholar] [CrossRef]
- Stock, T.; Seliger, G. Opportunities of Sustainable Manufacturing in Industry 4.0. Proc. CIRP 2016, 40, 536–541. [Google Scholar] [CrossRef] [Green Version]
- Schumacher, A.; Erol, S.; Sihn, W. A Maturity Model for Assessing Industry 4.0 Readiness and Maturity of Manufacturing Enterprises. Proc. CIRP 2016, 52, 161–166. [Google Scholar] [CrossRef]
- Kumar, K.; Zindani, D.; Davim, J.P. Industry 4.0: Developments towards the Fourth Industrial Revolution; Springer Nature: Singapore, 2019. [Google Scholar]
- Wang, S.; Wan, J.; Zhang, D.; Li, D.; Zhang, C. Towards Smart Factory for Industry 4.0: A Self-Organized Multi-Agent System with Big Data Based Feedback and Coordination. Comp. Netw. 2016, 101, 158–168. [Google Scholar] [CrossRef] [Green Version]
- Mosterman, P.J.; Zander, J. Industry 4.0 as a Cyber-Physical System Study. Softw. Syst. Model. 2016, 15, 17–29. [Google Scholar] [CrossRef]
- Almada-Lobo, F. The Industry 4.0 Revolution and the Future of Manufacturing Execution Systems (MES). J. Innov. Manag. 2015, 3, 16–21. [Google Scholar] [CrossRef]
- Qin, J.; Liu, Y.; Grosvenor, R. A Categorical Framework of Manufacturing for Industry 4.0 and Beyond. Proc. CIRP 2016, 52, 173–178. [Google Scholar] [CrossRef] [Green Version]
- Dobrzański, L.A.; Dobrzański, L.B. Approach to the Design and Manufacturing of Prosthetic Dental Restorations According to the Rules of Industry 4.0. Mater. Perform. Charact. 2020, 9, 394–476. [Google Scholar] [CrossRef]
- Dobrzański, L.A.; Dobrzański, L.B. Dentistry 4.0 Concept in the Design and Manufacturing of Prosthetic Dental Restorations. Processes 2020, 8, 525. [Google Scholar] [CrossRef]
- Dobrzański, L.A.; Dobrzański, L.B.; Achtelik-Franczak, A.; Dobrzańska, J. Application Solid Laser-Sintered or Machined Ti6Al4V Alloy in Manufacturing of Dental Implants and Dental Prosthetic Restorations According to Dentistry 4.0 Concept. Processes 2020, 8, 664. [Google Scholar] [CrossRef]
- Dobrzański, L.A.; Dobrzański, L.B.; Dobrzańska-Danikiewicz, A.D. Manufacturing technologies thick-layer coatings on various substrates and manufacturing gradient materials using powders of metals, their alloys and ceramics. J. Achiev. Mater. Manuf. Eng. 2020, 99, 14–41. [Google Scholar] [CrossRef]
- Dobrzańska-Danikiewicz, A.D.; Dobrzański, L.A.; Szindler, M.; Achtelik-Franczak, A.; Dobrzański, L.B. Obróbka powierzchni materiałów mikroporowatych wytworzonych metodą selektywnego spiekania laserowego w celu uefektywnienia proliferacji żywych komórek. In Metalowe Materiały Mikroporowate i Lite do Zastosowań Medycznych i Stomatologicznych; Open Access Library VII(1); Dobrzański, L.A., Dobrzańska-Danikiewicz, A.D., Eds.; International OCSCO World Press: Gliwice, Poland, 2017; pp. 289–375. [Google Scholar]
- Dobrzańska-Danikiewicz, A. The methodological fundaments of development state analysis of surface engineering technologies. J. Achiev. Mater. Manuf. Eng. 2010, 40, 203–210. [Google Scholar]
- Dobrzańska-Danikiewicz, A.D.; Hajduczek, E.; Polok-Rubiniec, M.; Przybył, M.; Adamaszek, K. Evaluation of selected steel thermochemical treatment technologies using foresight methods. J. Achiev. Mater. Manuf. Eng. 2011, 46, 115–146. [Google Scholar]
- Dobrzańska-Danikiewicz, A.D. The development perspectives of Physical Vapour Deposition technologies. J. Achiev. Mater. Manuf. Eng. 2012, 54, 103–109. [Google Scholar]
- Dobrzańska-Danikiewicz, A.D. Metodologia Komputerowo Zintegrowanego Prognozowania Rozwoju Inżynierii Powierzchni Materiałów; In Open Access Library 1(7); Dobrzański, L.A., Ed.; International OCSCO World Press: Gliwice, Poland, 2012; pp. 1–289. [Google Scholar]
- Dobrzańska-Danikiewicz, A.D. Księga Technologii Krytycznych Kształtowania Struktury i Własności Powierzchni Materiałów Inżynierskich; In Open Access Library 8(26); Dobrzański, L.A., Ed.; International OCSCO World Press: Gliwice, Poland, 2013; p. 1823. [Google Scholar]
- Dobrzańska-Danikiewicz, A.D. (Ed.) Materials Surface Engineering Development Trends; Open Access Library 6; International OCSCO World Press: Gliwice, Poland, 2011; pp. 1–594. [Google Scholar]
- Dobrzańska-Danikiewicz, A.D.; Dobrzański, L.A.; Sękala, A. Results of Technology Foresight in the Surface Engineering Area. Appl. Mech. Mater. 2014, 657, 916–920. [Google Scholar] [CrossRef]
- Dobrzańska-Danikiewicz, A.D.; Dobrzański, L.A.; Mazurkiewicz, J.; Tomiczek, B.; Reimann, Ł. E-transfer of materials surface engineering e-foresight results. Arch. Mater. Sci. Eng. 2011, 52, 87–100. [Google Scholar]
- Dobrzańska-Danikiewicz, A.D.; Tański, T.; Malara, S.; Domagała-Dubiel, J. Technology Foresight Results Concerning Laser Surface Treatment of Casting Magnesium Alloys. In New Features on Magnesium Alloys; Monteiro, W.A., Ed.; IntechOpen: Rijeka, Croatia, 2012; pp. 1–30. [Google Scholar] [CrossRef] [Green Version]
- Dobrzańska-Danikiewicz, A.D. Foresight of Material Surface Engineering as a Tool Building a Knowledge-Based Economy. Mater. Sci. Forum 2012, 706–709, 2511–2516. [Google Scholar] [CrossRef]
- Dobrzański, L.A.; Achtelik-Franczak, A. Struktura i własności tytanowych szkieletowych materiałów mikroporowatych wytworzonych metodą selektywnego spiekania laserowego do zastosowań w implantologii oraz medycynie regeneracyjnej. In Metalowe Materiały Mikroporowate i Lite do Zastosowań Medycznych i Stomatologicznych; Open Access Library VII(1); Dobrzański, L.A., Dobrzańska-Danikiewicz, A.D., Eds.; International OCSCO World Press: Gliwice, Poland, 2017; pp. 186–244. [Google Scholar]
- Dobrzański, L.A. Effect of heat and surface treatment on the structure and properties of the Mg-Al-Zn-Mn casting alloys. In Magnesium and Its Alloys; Dobrzański, L.A., Totten, G.E., Bamberger, M., Eds.; CRC Press: Boca Raton, FL, USA, 2019; pp. 91–202. [Google Scholar]
- Dobrzański, L.A.; Dobrzańska-Danikiewicz, A.D. Perspektywy i trendy rozwojowe inżynierii powierzchni materiałów. In Inżynieria Powierzchni Materiałów: Kompendium Wiedzy i Podręcznik Akademicki; Open Access Library VIII(1); Dobrzański, L.A., Ed.; International OCSCO World Press: Gliwice, Poland, 2018; pp. 89–157. [Google Scholar]
- Salehrabi, R.; Rotstein, I. Endodontic treatment outcomes in a large patient population in the USA: An epidemiological study. J. Endod. 2004, 30, 846–850. [Google Scholar] [CrossRef] [Green Version]
- Lazarski, M.P.; Walker, W.A.; Flores, C.M.; Schindler, W.G.; Hargreaves, K.M. Epidemiological evaluation of the outcomes of nonsurgical root canal treatment in a large cohort of insured dental patients. J. Endod. 2001, 27, 791–796. [Google Scholar] [CrossRef] [Green Version]
- Chen, S.C.; Chueh, L.H.; Hsiao, C.K.; Tsai, M.Y.; Ho, S.C.; Chiang, C.P. An epidemiologic study of tooth retention after nonsurgical endodontic treatment in a large population in Taiwan. J. Endod. 2007, 33, 226–229. [Google Scholar] [CrossRef]
- Meuwissen, R.; Eschen, S. Twenty years of endodontic treatment. J. Endod. 1983, 9, 390–393. [Google Scholar] [CrossRef]
- Sunay, H.; Tanalp, J.; Dikbas, I.; Bayirli, G. Cross-sectional evaluation of the periapical status and quality of root canal treatment in a selected population of urban Turkish adults. Int. Endod. J. 2007, 40, 139–145. [Google Scholar] [CrossRef]
- Jiménez-Pinzón, A.; Seguro-Egea, J.J.; Poyato-Ferrera, H.; Velasco-Ortega, E.; Rios-Santos, J.V. Prevalence of apical periodontitis and frequency of root fillednteeth in an adult Spanish population. Int. Endod. J. 2004, 37, 167–173. [Google Scholar] [CrossRef]
- Loftus, J.J.; Keating, A.P.; McCartan, B.E. Periapical status and quality of endodontic treatment in an adult Irish population. Int. Endod. J. 2005, 38, 81–86. [Google Scholar] [CrossRef]
- Peciuliene, V.; Rimkuviene, J.; Maneliene, R.; Iranauskaite, D. Apical periodontitis in root filled teeth associated with the quality of root fillings. Stomatologija 2006, 8, 122–126. [Google Scholar] [PubMed]
- De Moor, R.J.G.; Hommez, G.M.G.; de Boever, J.G.; Delmé, K.I.M.; Martens, G.E.I. Periapical health related to the quality of root canal treatment in a Belgian population. Int. Endod. J. 2000, 33, 113–120. [Google Scholar] [CrossRef] [PubMed]
- Da Silva, K.; Lam, J.M.Y.; Wu, N.; Duckmanton, P. Cross-sectional study of endodontic treatment in an Australian population. Aust. Endod. J. 2009, 35, 140–146. [Google Scholar] [CrossRef] [PubMed]
- Terças, A.G.; de Oliveira, A.E.F.; Lopes, F.F.; Filho, E.M.M. Radiographic study of the prevalence of apical periodontitis and endodontic treatment in the adult population of São Luís, MA, Brazil. J. Appl. Oral. Sci. 2006, 14, 183–187. [Google Scholar] [CrossRef] [Green Version]
- Georgopoulou, M.K.; Spanaki-Voreadi, A.P.; Pantazis, N.; Kontakiotis, E.G. Frequency and distribution of root filled teeth and apical periodontitis in a Greek population. Int. Endod. J. 2005, 38, 105–111. [Google Scholar] [CrossRef] [PubMed]
- Kirkevang, L.L.; Hörsted-Bindslev, P.; Ostravik, D.; Wenzel, A. Frequency and distribution of endodontically treated teeth and apical periodontitis in an urban Danish population. Int. Endod. J. 2001, 34, 198–205. [Google Scholar] [CrossRef]
- Tsuneishi, M.; Yamamoto, T.; Yamanaka, R.; Tamaki, N.; Sakamoto, T.; Tsuji, K.; Watanabe, T. Radiographic evaluation of periapical status and prevalence of endodontic treatment in an adult Japanese population. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2005, 100, 631–635. [Google Scholar] [CrossRef] [PubMed]
- Gharib, S.R.; Tordik, P.A.; Imamura, G.M.; Bagiński, T.A.; Goodell, G.G. A confocal laser scanning microscope investigation of the Epiphany obturation system. J. Endod. 2007, 33, 957–961. [Google Scholar] [CrossRef] [PubMed]
- Kontakiotis, E.; Chaniotis, A.; Georgopoulou, M. Fluid filtration evaluation of 3 obturation techniques. Quint. Int. 2007, 38, 410–416. [Google Scholar]
- Dziedzic, A.; Turski, R.; Werszner, R.; Wojdyło, M. Ocena in vitro szczelności wypełnień kanałów korzeniowych systemem EndoREZ z wykorzystaniem ćwieków gutaperkowych o zwiększonym stopniu zbieżności. Mag. Stomatol. 2005, 15, 38–41. [Google Scholar]
- Vogt, B.F.; Xavier, C.B.; Demarco, F.F.; Padilha, M.S. Dentin penetrability evaluation of three different dyes in root-end cavities filled with mineral trioxide aggregate (MTA). Braz. Oral Res. 2006, 20, 132–136. [Google Scholar] [CrossRef]
- Gencoglu, N.; Garip, Y.; Bas, M.; Samani, S. Comparison of different gutta-percha Root filling techniques: Thermafil, Quick-fill, System B and Lateran condensation. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2002, 93, 333–336. [Google Scholar] [CrossRef]
- Sliva, G.; da Silva, E.J.N.; da Silva, J.M.; Andrande-Junior, C.V.; Ferraz, C.C.R. Sealing ability promoted by three different endodontic sealers. Iran. Endod. J. 2011, 6, 86–89. [Google Scholar] [CrossRef]
- Mannocci, F.; Innocenti, M.; Ferrari, M. Stereomicroscopic and scanning electron microscopic study of roots obturated with vertically condensed gutta-percha, epoxy resin cement and dentin bonding agent. J. Endod. 1998, 24, 397–400. [Google Scholar] [CrossRef]
- Mannocci, F.; Innocenti, M.; Bertelli, E.; Ferrari, M. Dye leakage and SEM study of roots obturated with Thermafill and dentin bonding agent. Endod. Dent. Traumatol. 1999, 15, 60–64. [Google Scholar] [CrossRef]
- Serafino, C.; Gallina, G.; Cumbo, E.; Ferrari, M. Surface debris of canal walls after post space preparation in endodontically treated teeth: A scanning electron microscopic study. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2004, 97, 381–387. [Google Scholar] [CrossRef] [PubMed]
- Bołtacz-Rzepkowska, E.; Pawlicka, H.; Klimek, L. Przyleganie wypełnień do ścian kanału korzeniowego wykonanych różnymi technikami-badania w mikroskopie skaningowym. Czas. Stomatol. 2003, 56, 163–168. [Google Scholar]
- Szkodny, K.; Postek-Stefańska, L.; Michalewicz, M.; Mangold, D.; Koziarz, A. Porównanie szczelności brzeżnej wypełnień kanałowych wykonanych metodą kondensacji bocznej i z użyciem Soft-Core. Badanie w SEM. Mag. Stomatol. 2002, 12, 68–72. [Google Scholar]
- Dobrzański, L.A. Podstawy Nauki o Materiałach i Metaloznawstwo; WNT: Warszawa, Poland, 2002; pp. 1–1500. [Google Scholar]
- Dobrzańska, J.; Dobrzański, L.B.; Dobrzański, L.A.; Gołombek, K.; Dobrzańska-Danikiewicz, A.D. Strengths, weaknesses, opportunities, and threats analysis of the resilon as filling material in endodontics. Appl. Sci. 2021, 11, 1–58. [Google Scholar]






















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
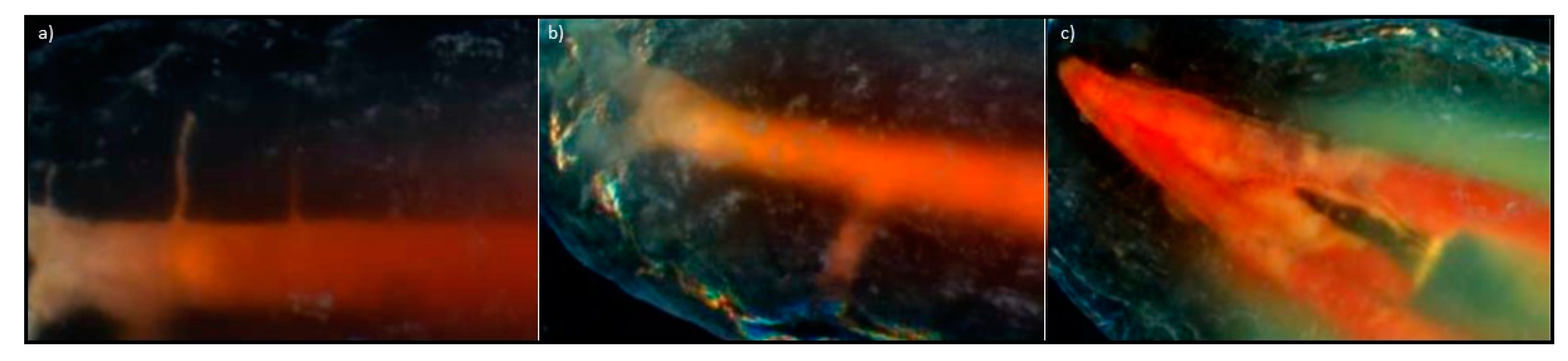{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| No. | Type of Context Matrix | Generalized Index on the x Axis | Generalized Index on the y Axis |
|---|---|---|---|
| A1 | Materials selection | generalized index of material quality for root canal filling | generalized index of material strength in the root canal |
| A2 | Root canal development technique selection | generalized organizational index of techniques for the development of root canals | generalized index of the quality of filling with selected techniques |
| A3 | Techniques of obturation selection | generalized index of material strength applied in root canal obturation techniques | generalized index of the effectiveness of root canal obturation techniques |
| A4 | Assessing the tightness of root canal filling selection | generalized index of organizational conditions | generalized index of investigations effectiveness |
| No. | Type of Action | Description of the Action | |
|---|---|---|---|
| B1 | Preparation of teeth for examination | Before processing, each tooth was cleaned and rinsed in 0.9% NaCl solution, and then the tooth crowns were cut off at the height of the tooth neck with a diamond separator placed on the prosthetic handpiece. During the mechanical preparation of the root canals, a lubricant containing glycerin, sodium edetate, and urea peroxide RC-Prep (Premier) was used. The task of the lubricant during the preparation of the canal was to remove the smear layer covering the canal dentin and to facilitate the mechanical preparation of the canal with the tools used. Between each instrument subsequently introduced into the root canal, irrigation with 2.25% sodium hypochlorite solution and 0.9% saline solution was performed alternately. | |
| B2 | Preparation of root canals of selected teeth | Hand tools | Each canal in a given group was prepared with hand tools (ProTaper—Dentsply/Maillefer) in two stages; in the first stage, the near-crown part was widened with the S1 tool; successively, the SX tool with the highest 19% taper was introduced into the same part of the canal, after which the length of the canal was measured with a Kerr file with the number 10 ISO, from which 1 mm has been subtracted. The working length was determined based on the length of the tooth canal minus 1 mm (as the average distance between the anatomical apex and the physiological narrowing of the root canal). The channel was subsequently developed to the full working length with the S1 and S2 tools. The next four tools, numbered F1, F2, F3, and F4, were introduced to the full working length, widening, and smoothing the root canal walls. Each tool introduced was followed by a canal recapitulation with the Kerr tool. |
| B3 | Rotary tools | Each canal in a given group was prepared with rotary tools up to the size of ISO 40 using the X-Smart endodontic micromotor (DentSply/Maillefer with K3 tools (Sybron Endo)). Each canal was prepared in two stages, 10/25 and 08/25, with a taper of the tool of 10 and 8%, respectively. Then, the root canal length was measured by inserting a 10 ISO Kerr file and subtracting from the full length of 1 mm, determining the working length as the average distance between the anatomical apex and the constriction. Then, the canal was prepared to its full working length with tools in sizes of 0.4/20, 0.4/25, 0.4/30, 0.4/35, and 0.4/40. | |
| No. | Method | Description of the Method of Filling the Root Canals |
|---|---|---|
| C1 | Lateral condensation | Each channel in a given group was filled with studs and pellets. After drying the root canal, an F4 size pin (DentSply/Maillefer) was fitted, corresponding to the last tool used to prepare the canal to the full working length. Before obturation, each canal was thoroughly dried with paper points. A thin layer of sealant (AH Plus type—DentSply/Maillefer) was applied to the walls with a paper filter in each canal. Each stud was disinfected in 2.25% sodium hypochlorite solution, and then placed in the root canal on the full, previously determined working length. Due to the large convergence of the main cone, which corresponded to the variable convergence of the ProTaper type tool, an expander with the size of 20 ISO, and with a convergence of 2%, was selected. Using a silicone stopper, a length 1 mm shorter than the length on which the main stud was inserted was determined on the plunger. After the placement was prepared by the manual pusher, the canal was supplemented with studs with a taper of 2% in the size corresponding to the pusher used. The filling of the channel was completed when it was not possible to introduce the plunger into the channel. |
| C2 | Thermoplastic with the Thermafil type system | Each channel in a given group was filled with studs and pellets. The use of the system began with the inspection of the canal with a 40 ISO verifier, the size of the last instrument introduced during root canal preparation. After selecting the appropriate obturator, the working length was marked with a stopper, then it was disinfected in a 2.25% sodium hypochlorite solution, dried, and placed in a ThermaPrep Plus oven to plasticize it. In each channel, a thin layer of AH Plus sealant (DentSply/Maillefer) was applied to the walls with a paper filter. After the gutta-percha was plasticized in the oven, the obturator was slowly withdrawn from the lift of the oven and placed in the channel for the working length previously indicated, maintaining a constant pressure on the polymer support for a few seconds. When placing the obturator, care was taken that it was precisely centered into the canal to prevent distortion of the gutta-percha matrix at the top of the obturator. The polymeric material carrier on the gutta-percha matrix was then cut off with a Therma-Cut drill without water cooling at 300,000 rpm, and the gutta-percha matrix material was condensed around the carrier with a plunger. |
| C3 | Thermoplastic with the use of System B and Obtura III devices (SybronEndo) | Each channel in a given group was filled with studs and pellets. The root canals were thoroughly dried with paper points, then the main pin with a convergence of 4% was selected; the selection criterion was the wedging of the pin in the periapical area after it was introduced to its full working length. A Buchanan plugger (SybronEndo), size 1, was subsequently fitted to the canal’s diameter, and its length was marked with a stopper, equal to the working length shortened by 4 mm. The root canal walls were covered with a thin layer of AH Plus sealant (DentSply/Maillefer) with a paper filter. During the introduction of the heated System B plugger through the stud placed in the root canal up to the length marked with a stopper, the temperature was set at 200 °C. After 3 s, the heating was turned off while maintaining the pressure of the tool towards the root apex for 10 s. The plugger was then reheated to 300 °C and immediately removed along with any excess uncondensed material. The apical portion of the material was condensed with pulsating movements for the next 10 s using a cold, previously selected Buchanan-type plugger (SybronEndo). The canal, filled in this way, at the apex, was filled with gutta-percha matrix material and fed into the canal with the use of an Obtura III type system (SybronEndo) with a temperature set at 160 °C. The canal was restored in stages, introducing small portions of liquid material, condensing each time with a Buchanan-type plugger (SybronEndo). |
| No. | Type of Activity | Methods of Specimen Preparation or Materialographic Test Methods | |
|---|---|---|---|
| D1 | Initial preparation of specimens for research | To prepare the specimens for materialographic tests, after tight-filling the canals with each technique, the root canal orifices of the selected teeth were secured with Ketac Molar glass ionomer cement (3M ESPE). For the next 7 days, the teeth were stored in a humid environment and room temperature to bind the sealant. Each tooth was wrapped in gauze soaked in physiological saline and tightly closed in plastic containers. | |
| D2 | Preparing breaktroughts | The prepared specimens were incised longitudinally along the root to a depth of 1 mm using a diamond disc placed on a prosthetic handpiece. The research material was placed in liquid nitrogen and then a breakthrough was made. Each sample, after making longitudinal cuts by breakthroughs in liquid nitrogen, was then sputtered with a thin layer of gold as a conductive material in a BAL—TEC SCD050 sputtering machine by Oerlikon Balzers (Balzers, Liechtenstein), to remove the electric charge from the surface of the specimen during the examination in the scanning electron microscope, as well as to improve the secondary electron emission factor. | |
| D3 | Tooth decalcification | Teeth filled with material based on gutta-percha were decalcified by immersion for 14 days in an aqueous solution consisting of 7% formic acid, 3% hydrochloric acid, and 8% sodium citrate. The specimens were then rinsed thoroughly under running water to eliminate the acid, and then immersed in 99% acetic acid for 12 h, and then the specimens were rinsed thoroughly with distilled water. Then, the specimens were dehydrated in ethanol solution of successively increasing concentrations of 25, 50, 70, 90, 95, and 100%, each for 30 min. Then the specimens were stored in methyl salicylate and observed in a Stereo Discovery V12 stereoscopic light microscope with the AxioCam HRC digital camera by Zeiss at 8–50× magnification, to the three-dimensional observation of the root canal lumen filled with a substitute material, with careful consideration of the root delta and its complicated internal system and side branches of the main canal. | |
| D4 | Materialographic research | LM | Teeth filled with material based on gutta-percha were cut in the longitudinal and transverse directions using the GATAN ISOTOM device, and the materialographic specimens were made by mounting in a thermosetting resin and mechanical grinding successively on abrasive papers with smaller and smaller grain size in Struers devices, and then on diamond pastes of granularity to 3 μm for observation with a Leica 8i light microscope. |
| D5 | SLM | Initial tests were performed on the Stereo Discovery V12 stereo microscope with the AxioCam HRC digital camera by Zeiss; the test results were documented using the digital photography method at 50× magnification. | |
| D6 | SEM | Tests were carried out using a SUPRA 35 high-resolution scanning microscope by Zeiss with a WDS, EDS spectrometer, and an EBSD TRIDENT XM4 camera by EDAX in the range of magnifications of 2000 and 5000×, and the test results were digitally archived. | |
| D7 | AFM | Observations were made using an AFM XE-100 atomic force microscope (AFM) by Park Systems with a scanning probe, using the forces of interatomic interactions and allowing the researchers to obtain an image of the surface with a resolving power corresponding to the size of an atom. | |
| D8 | CL | Observations were made in an Exciter confocal laser scanning microscope based on the Axio Observer microscope by ZEISS, with electronic recording of the test results. | |
| No. | Structure Assessment Elements | Used Microscopes |
|---|---|---|
| 1. | Connection of the filling material with the dentin of the root canal | LSM—light stereoscopic; SEM—scanning electron |
| 2. | Connection of the main stud with complementary material | |
| 3. | Filling the side tubules | |
| 4. | Filling the root delta | |
| 5. | Connection of the material with the dentin tubules | |
| 6. | Volume fraction of sealant | |
| 7. | Leakage on the border of the root canal wall and the filling material |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dobrzańska, J.; Dobrzański, L.B.; Dobrzański, L.A.; Gołombek, K.; Dobrzańska-Danikiewicz, A.D. Is Gutta-Percha Still the “Gold Standard” among Filling Materials in Endodontic Treatment? Processes 2021, 9, 1467. https://0-doi-org.brum.beds.ac.uk/10.3390/pr9081467
Dobrzańska J, Dobrzański LB, Dobrzański LA, Gołombek K, Dobrzańska-Danikiewicz AD. Is Gutta-Percha Still the “Gold Standard” among Filling Materials in Endodontic Treatment? Processes. 2021; 9(8):1467. https://0-doi-org.brum.beds.ac.uk/10.3390/pr9081467
Chicago/Turabian StyleDobrzańska, Joanna, Lech B. Dobrzański, Leszek A. Dobrzański, Klaudiusz Gołombek, and Anna D. Dobrzańska-Danikiewicz. 2021. "Is Gutta-Percha Still the “Gold Standard” among Filling Materials in Endodontic Treatment?" Processes 9, no. 8: 1467. https://0-doi-org.brum.beds.ac.uk/10.3390/pr9081467