

Psychological Distress and Behavioral Vigilance in Response to Minority Stress and Threat among Members of the Asian American and Pacific Islander Community during the COVID-19 Pandemic


Abstract
:1. Introduction
1.1. COVID-19 Pandemic and Anti-AAPI Racism
1.2. Minority Stress
1.3. Moderating the Effects of Minority Stress
1.4. Integrated Threat and the COVID-19 Pandemic
1.5. The Present Study
1.5.1. Correlational Hypotheses
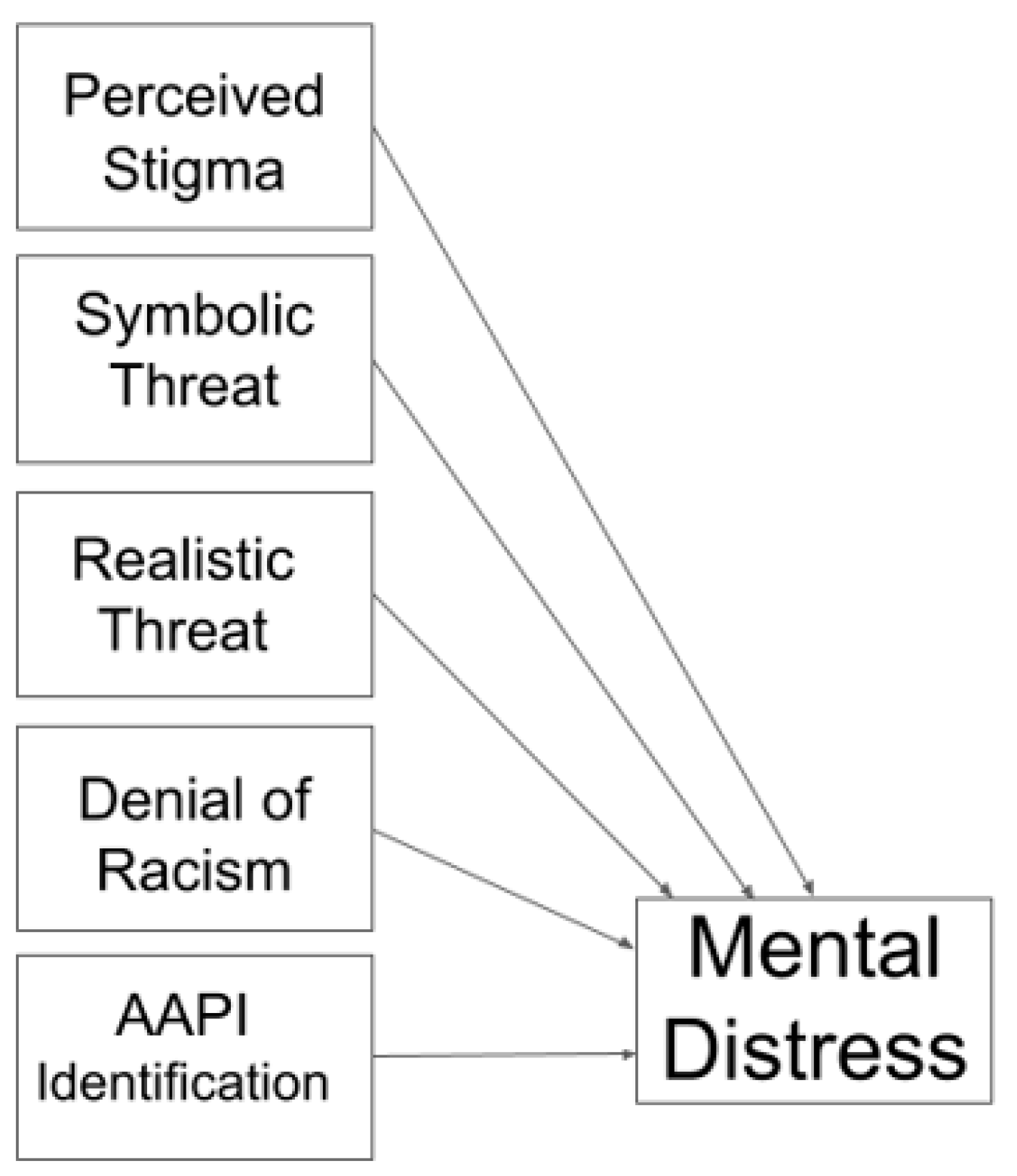
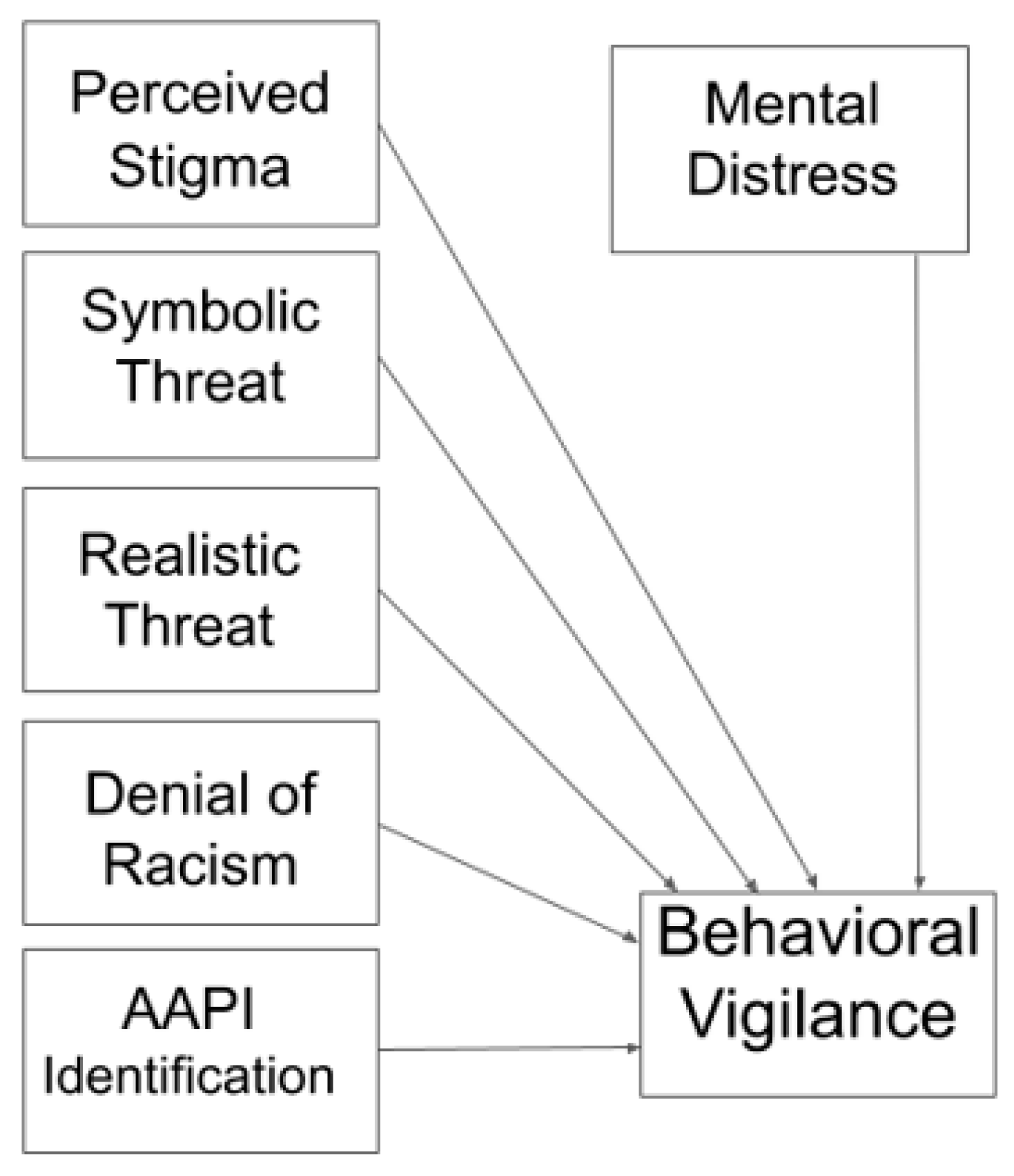
1.5.2. Regression Hypotheses
1.5.3. Moderation Hypothesis
2. Materials and Methods
2.1. Participants
2.2. Measures and Procedure
2.3. Data Analysis
3. Results
3.1. Correlation Analyses
3.2. Regression Analyses
3.2.1. Predicting Psychological Distress
3.2.2. Predicting Pandemic-Related Behavioral Vigilance
3.3. Moderation Analyses
3.3.1. Stigma (x), Denial of Racism (w), and Psychological Distress (y)
3.3.2. Stigma (x), Asian American Identification (w), and Psychological Distress (y)
3.3.3. Stigma (x), Denial of Racism (w), and Behavioral Vigilance (y)
3.3.4. Stigma (x), Asian American Identification (w), and Behavioral Vigilance (y)
3.4. A Footnote on Exploratory Analyses
4. Discussion
4.1. Integration with Previous Scholarship
4.2. Conclusions
4.3. Limitations and Future Directions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A. Recruitment Language
Appendix B. Perceived AAPI Stigmatization
- During the pandemic, I have noticed more negative depictions of Asian-Americans in the media.
- During the pandemic, I have noticed an increase in anti-Asian sentiment expressed by political leaders.
- During the pandemic, I have noticed an increase in anti-Asian hostility on social networking websites.
Appendix C. Pandemic-Related Behavioral Vigilance
- Since the start of the pandemic, I have been doing more to actively avoid anti-Asian harassment.
- Since the start of the pandemic, I have been leaving the house less often due to a fear of being harassed for being Asian-American
- Since the start of the pandemic, I have been more alert and vigilant for threats when I have to be out in public.
References
- Kurashige, L. Two Faces of Exclusion: The Untold History of Anti-Asian Racism in the United States; University of North Carolina Press Books: Chapel Hill, NC, USA, 2016. [Google Scholar]
- Petersen, W. Success Story, Japanese American Style. New York Times Magazine. 1966, p. 22ff. Available online: https://inside.sfuhs.org/dept/history/US_History_reader/Chapter14/modelminority.pdf (accessed on 21 November 2023).
- Yi, V.; Museus, S.D. Model minority myth. In The Wiley Blackwell Encyclopedia of Race, Ethnicity, and Nationalism; John Wiley & Sons: Hoboken, NJ, USA, 2015; pp. 1–2. [Google Scholar]
- Lee, E. America for Americans: A History of Xenophobia in the United States; Basic Books: New York, NY, USA, 2019. [Google Scholar]
- Li, Y.; Nicholson, H.L., Jr. When “model minorities” become “yellow peril”—Othering and the racialization of Asian Americans in the COVID-19 pandemic. Sociol. Compass 2021, 15, e12849. [Google Scholar] [CrossRef]
- Cheng, H.-L.; Kim, H.Y.; Reynolds, J.D.; Tson, Y.; Wong, Y.J. COVID-19 anti-Asian racism: A tripartite model of collective psychosocial resilience. Am. Psychol. 2021, 76, 627–642. [Google Scholar] [CrossRef]
- Meyer, I.H. Prejudice, social stress, and mental health in lesbian, gay, and bisexual populations: Conceptual issues and research evidence. Psychol. Bull. 2023, 129, 674–697. [Google Scholar] [CrossRef]
- Botha, M.; Frost, D.M. Extending the minority stress model to understand mental health problems experienced by the autistic population. Soc. Ment. Health 2018, 10, 20–34. [Google Scholar] [CrossRef]
- English, D.; Rendina, H.J.; Parsons, T. The effects of intersecting stigma: A longitudinal examination of minority stress, mental health, and substance use among Black, Latino, and multiracial gay and bisexual men. Psychol. Violence 2019, 8, 669–679. [Google Scholar] [CrossRef]
- Ehlke, S.J.; Braitman, A.L.; Dawson, C.A.; Heron, K.E.; Lewis, R.J. Sexual minority stress and social support explain the association between sexual identity with physical and mental health problems among young lesbian and bisexual women. Sex Roles 2020, 83, 370–381. [Google Scholar] [CrossRef] [PubMed]
- Flentje, A.; Heck, N.C.; Brennan, J.M.; Meyer, I.H. The relationship between minority stress and biological outcomes: A systematic review. J. Behav. Med. 2019, 43, 673–694. [Google Scholar] [CrossRef]
- Cheng, H.-L.; Wong, Y.J.; Li, P.F.J.; McDermott, R.C. COVID-19 racism, anxiety, and racial/ethnic attitudes among Asian American college students. Couns. Psychol. Q. 2021, 35, 897–920. [Google Scholar] [CrossRef]
- Zarate, M.A.; Garcia, B.; Garza, A.A.; Hitlan, R.T. Cultural threat and perceived realistic group conflict as dual predictors of prejudice. J. Exp. Soc. Psychol. 2004, 40, 99–105. [Google Scholar] [CrossRef]
- Kachanoff, F.J.; Bigman, Y.E.; Kapsaskis, K.; Gray, K. Measuring Realistic and Symbolic Threats of COVID-19 and Their Unique Impacts on Well-Being and Adherence to Public Health Behaviors. Soc. Psychol. Personal. Sci. 2021, 12, 603–616. [Google Scholar] [CrossRef]
- DC, T.V.; McGill Terrace, N.W. U.S. Department of Justice; Office of Justice Programs, Office of Juvenile Justice and Delinquency Prevention: Washington, DC, USA, 2022. [Google Scholar]
- Jeung, R.; Horse, A.Y.; Popovic, T.; Lim, R. Stop AAPI Hate National Report; Stop AAPI Hate: San Francisco, CA, USA, 2021; 3/19/20–12/31/21. [Google Scholar]
- Jeung, R. Incidents of Coronavirus Discirmination March 19–25, 2020. Available online: https://www.asianpacificpolicyandplanningcouncil.org/wp-content/uploads/A3PCON_Public_Weekly_Report_3.pdf (accessed on 21 November 2023).
- Stop AAPI Hate. Two Years and Thousands of Voices: What Community-Generated Data Tells Us About Anti-AAPI Hate; Stop AAPI Hate: San Francisco, CA, USA, 2022. [Google Scholar]
- Lantz, B.; Wenger, M.R. Are Asian victims less likely to report hate crime victimization to the police? Implications for research and policy in the wake of the COVID-19 pandemic. Crime Delinq. 2021, 68, 1292–1319. [Google Scholar] [CrossRef]
- Liu, J.L.; Cheong, Y.; Wang, C.; Cheah, C.S.L.; Ma, R.; Zhang, X. The voices of Chinese American parents during COVID-19: Recommendations for addressing anti-Asian racism and supporting adolescents in school. Asian Am. J. Psychol. 2023, 15, 1–11. [Google Scholar] [CrossRef]
- Wang, C.; SL Cheah, C.; Liu, J.L.; Zhu, Q.; Havewala, M.; Ma, R.; Cheong, Y.; Housden, M. Parents’ perspectives regarding anti-Asian racism during COVID-19: Supporting elementary students at school. Sch. Psychol. Rev. 2023, 52, 435–452. [Google Scholar] [CrossRef]
- Budhwani, H.; Sun, R. Creating COVID-19 stigma by referencing the novel coronavirus as the “Chinese virus” on Twitter: Quantitative analysis of social media data. J. Med. Internet Res. 2020, 22, e19301. [Google Scholar] [CrossRef]
- Croucher, S.M.; Nguyen, T.; Rahmani, D. Prejudice toward Asian Americans in the COVID-19 pandemic: The effects of social media use in the United States. Front. Commun. 2020, 5, 39. [Google Scholar] [CrossRef]
- Gardner, D.M.; Briggs, C.Q.; Ryan, A.M. It is your fault: Workplace consequences of anti-Asian stigma during COVID-19. Equal. Divers. Incl. Int. J. 2022, 41, 3–18. [Google Scholar] [CrossRef]
- Reny, T.T.; Barreto, M.A. Xenophobia in the time of pandemic: Othering, anti-Asian attitudes, and COVID-19. Politics Groups Identities 2022, 10, 209–232. [Google Scholar] [CrossRef]
- Rubin, D.I.; Agostinone Wilson, F. Blame China: Trump and anti-Asian sentiment during COVID-19. In A Time of Covidiocy: Media, Politics, and Social Pheaval; Brill: Leiden, The Netherlands, 2021. [Google Scholar]
- Aria Adibrata, J.; Fikhri Khairi, N. The impact of COVID-19 blame game towards anti-Asian discrimination phenomena. J. Soc. Media 2022, 6, 17–38. [Google Scholar] [CrossRef]
- Lantz, B.; Wenger, M.R.; Mills, J.M. Fear, political legitimization, and racism: Examining anti-Asian xenophobia during the COVID-19 pandemic. Race Justice 2023, 13, 80–104. [Google Scholar] [CrossRef]
- Fairlie, R. The impact of COVID-19 on small business owners: Evidence from the first three months after widespread social-distancing restrictions. J. Econ. Manag. Strategy 2020, 29, 727–740. [Google Scholar] [CrossRef] [PubMed]
- Kim, A.T.; Kim, C.; Tuttle, S.E.; Zhang, Y. COVID-19 and the decline in Asian American employment. Res. Soc. Stratif. Mobil. 2021, 71, 100563. [Google Scholar] [CrossRef]
- Lee, S.; Waters, S.F. Asians and Asian Americans’ experiences of racial discrimination during the COVID-19 pandemic: Impacts on health outcomes and the buffering role of social support. Stigma Health 2021, 6, 70–78. [Google Scholar] [CrossRef]
- Wu, C.; Qian, Y.; Wilkes, R. Anti-Asian discrimination and the Asian-white mental health gap during COVID-19. Ethn. Racial Stud. 2021, 44, 819–835. [Google Scholar] [CrossRef]
- Zhou, S.; Banawa, R.; Oh, H. The mental health impact of COVID-19 racial and ethnic discrimination against Asian American and Pacific Islanders. Front. Psychiatry 2021, 12, 708426. [Google Scholar] [CrossRef]
- Huang, J.T.; Krupenkin, M.; Rothschild, D.; Lee Cunningham, J. The cost of anti-Asian racism during the COVID-19 pandemic. Nat. Hum. Behav. 2023, 7, 682–695. [Google Scholar] [CrossRef] [PubMed]
- Lozano, P.; Rueger, S.Y.; Lam, H.; Louie, N.; Southworth, A.; Maene, C.; Mo, Y.; Randal, F.; Kim, K. Prevalence of depression symptoms before and during the COVID-19 pandemic among two Asian American ethnic groups. J. Immigr. Minor. Health 2021, 24, 909–917. [Google Scholar] [CrossRef]
- Hahm, H.C.; Ha, Y.; Scott, J.C.; Wongchai, V.; Chen, J.A.; Liu, C.H. Perceived COVID-19-related anti-Asian discrimination predicts post traumatic stress disorder symptoms among Asian and Asian American young adults. Psychiatry Res. 2021, 303, 114084. [Google Scholar] [CrossRef]
- Comas-Díaz, L.; Hall, G.N.; Neville, H.A. Racial trauma: Theory, research, and healing: Introduction to the special issue. Am. Psychol. 2019, 74, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Abbott, D.M.; Franks, A.S. Coping with COVID-19: An examination of the role of (non) religiousness/(non) spirituality. J. Relig. Health 2021, 60, 2395–2410. [Google Scholar] [CrossRef]
- Aneshensel, C.S. Social stress: Theory and research. Annu. Rev. Sociol. 1992, 18, 15–38. [Google Scholar] [CrossRef]
- Valentine, S.E.; Shipherd, J.C. A systematic review of social stress and mental health among transgender and gender non-conforming people in the United States. Clin. Psychol. Rev. 2018, 66, 24–38. [Google Scholar] [CrossRef] [PubMed]
- Brooks, V. Minority Stress and Lesbian Women; Lexington Press: Lexington, KY, USA, 1981. [Google Scholar]
- Cerezo, A. The impact of discrimination on mental health symptomatology in sexual minority immigrant Latinas. Psychol. Sex. Orientat. Gend. Divers. 2016, 3, 283–292. [Google Scholar] [CrossRef]
- Nie, F. Asian hate, minority stress, and religious coping: A study of Asian and Asian American adults in the USA during the COVID-19 pandemic. J. Relig. Health 2022, 62, 681–701. [Google Scholar] [CrossRef] [PubMed]
- Lei, N.; Velez, B.L.; Seoud, J.M.; Motulsky, W.N. A test of minority stress theory with Asian Americans. Couns. Psychol. 2022, 50, 1009–1038. [Google Scholar] [CrossRef]
- Szymanski, D.M.; Sung, M.R. Minority stress and psychological distress among Asian American sexual minority persons. Couns. Psychol. 2010, 38, 848–872. [Google Scholar] [CrossRef]
- Wei, M.; Ku, T.-Y.; Russell, D.W.; Mallinckrodt, B.; Liao, K.Y.-H. Moderating effects of three coping strategies and self-esteem on perceived discrimination and depressive symptoms: A minority stress model for Asian international students. J. Couns. Psychol. 2008, 55, 451–462. [Google Scholar] [CrossRef] [PubMed]
- Wei, M.; Liao, K.Y.-H.; Chao, R.C.-L.; Mallinckrodt, B.; Tsai, P.-C.; Botello-Zamarron, R. Minority stress, perceived bicultural competence, and depressive symptoms among ethnic minority college students. J. Couns. Psychol. 2010, 57, 411–422. [Google Scholar] [CrossRef]
- Chen, Y.-C.; Tryon, G.S. Dual minority stress and Asian American gay men’s psychological distress. J. Community Psychol. 2012, 40, 539–554. [Google Scholar]
- Hwang, W.C.; Goto, S. The impact of perceived racial discrimination on the mental health of Asian American and Latino college students. Cult. Divers. Ethn. Minor. Psychol. 2008, 14, 326–335. [Google Scholar] [CrossRef]
- Ong, A.D.; Burrow, A.L.; Fuller-Rowell, T.; Ja, N.M.; Sue, D.W. Racial microaggressions and daily well-being among Asian Americans. J. Couns. Psychol. 2013, 60, 188–199. [Google Scholar] [CrossRef]
- Park, M.; Choi, Y.; Yasui, M.; Hedeker, D. Specificity and Generalizability in Social-Emotional Development Special Section Editors, C. Racial discrimination and the moderating effects of racial and ethnic socialization on the mental health of Asian American youth. Child Dev. 2021, 92, 2284–2298. [Google Scholar] [CrossRef]
- Chia-Chen Chen, A.; Szalacha, L.A.; Menon, U. Perceived discrimination and its associations with mental health and substance use among Asian American and Pacific Islander undergraduate and graduate students. J. Am. Coll. Health 2014, 62, 390–398. [Google Scholar] [CrossRef] [PubMed]
- Nadimpalli, S.B.; Hutchinson, M.K. An integrative review of relationships between discrimination and Asian American health. J. Nurs. Scholarsh. 2021, 44, 127–135. [Google Scholar] [CrossRef] [PubMed]
- Yoo, H.C.; Gee, G.C.; Takeuchi, D. Discrimination and health among Asian American immigrants: Disentangling racial from language discrimination. Soc. Sci. Med. 2009, 68, 726–732. [Google Scholar] [CrossRef] [PubMed]
- Nadal, K.L.; Griffin, K.E.; Wong, Y.; Hamit, S.; Rasmus, M. The impact of racial microaggressions on mental health: Counseling implications for clients of color. J. Couns. Dev. 2014, 92, 57–66. [Google Scholar] [CrossRef]
- Nadal, K.L.; Wong, Y.; Sriken, J.; Griffin, K.; Fujii-Doe, W. Racial microaggressions and Asian Americans: An exploratory study on within-group differences and mental health. Asian Am. J. Psychol. 2015, 6, 136–144. [Google Scholar] [CrossRef]
- Ong, A.D.; Cerrada, C.; Lee, R.A.; Williams, D.R. Stigma consciousness, racial microaggressions, and sleep disturbance among Asian Americans. Asian Am. J. Psychol. 2017, 8, 72–81. [Google Scholar] [CrossRef]
- Kim, P.Y.; Kendall, D.L.; Cheon, H.S. Racial microaggressions, cultural mistrust, and mental health outcomes among Asian American college students. Am. J. Orthopsychiatry 2017, 87, 663–670. [Google Scholar] [CrossRef]
- Torres, L.; Ong, A.D. A daily diary investigation of Latino ethnic identity, discrimination, and depression. Cult. Divers. Ethn. Minor. Psychol. 2010, 16, 561. [Google Scholar] [CrossRef]
- Hwang, W.C. Demystifying and addressing internalized racism and oppression among Asian Americans. Am. Psychol. 2021, 76, 596–610. [Google Scholar] [CrossRef]
- Lee, D.L.; Ahn, S. Racial Discrimination and Asian mental health: A meta-analysis. Couns. Psychol. 2011, 39, 463–489. [Google Scholar] [CrossRef]
- Haft, S.L.; Mauss, I.B.; Zhou, Q. Perceived discrimination, model minority stereotyping, and anxiety symptoms in chinese-heritage college students. Cult. Divers. Ethn. Minor. Psychol. 2022, 30, 61–711. [Google Scholar] [CrossRef]
- Albuja, A.F.; Gaither, S.E.; Sanchez, D.T.; Straka, B.; Cipollina, R. Psychophysiological stress responses to bicultural and biracial identity denial. J. Soc. Issues 2019, 75, 1165–1191. [Google Scholar] [CrossRef]
- Museus, S.D.; Park, J.J. The continuing significance of racism in the lives of Asian American college students. J. Coll. Stud. Dev. 2015, 56, 551–569. [Google Scholar] [CrossRef]
- Lee, S.; Juon, H.-S.; Martinez, G.; Hsu, C.E.; Robinson, E.S.; Bawa, J.; Ma, G.X. Model minority at risk: Expressed needs of mental health by Asian American young adults. J. Community Health 2008, 34, 144. [Google Scholar] [CrossRef]
- Liao, L. Development of the Internalized Racism Scale for Asian Americans; Arizona State University: Tempe, AZ, USA, 2016. [Google Scholar]
- Hennekens, C.H.; George, S.; Adirim, T.A.; Johnson, H.; Maki, D.G. The emerging pandemic of coronavirus and the urgent need for public health leadership. Am. J. Med. 2020, 133, 648–650. [Google Scholar] [CrossRef]
- Stephan, W.G.; Renfro, C.L.; Esses, V.M.; Stephan, C.W.; Martin, T. The effects of feeling threatened on attitudes toward immigrants. Int. J. Intercult. Relat. 2005, 29, 1–19. [Google Scholar] [CrossRef]
- Stephan, W.G.; Ybarra, O.; Bachman, G. Prejudice toward immigrants. J. Appl. Soc. Psychol. 1999, 29, 2221–2237. [Google Scholar] [CrossRef]
- Major, B.; Mendes, W.B.; Dovidio, J.F. Intergroup relations and health disparities: A social psychological perspective. Health Psychol. 2013, 32, 514–524. [Google Scholar] [CrossRef] [PubMed]
- Franks, A.S.; Xiao, Y.J.; Hesami, F. Racial framing of pandemic outcomes has conditional indirect effects on support for COVID-19 mitigation policies: Examining moral and threat-based mediating mechanisms. Anal. Soc. Issues Public Policy 2022, 22, 130–149. [Google Scholar] [CrossRef]
- Leach, C.W.; van Zomeren, M.; Zebel, S.; Vliek, M.L.W.; Pennekamp, S.F.; Doosje, B.; Ouwerkerk, J.W.; Spears, R. Group-level self-definition and self-investment: A hierarchical (multicomponent) model of in-group identification. J. Personal. Soc. Psychol. 2008, 95, 144–165. [Google Scholar] [CrossRef] [PubMed]
- Lovibond, P.F.; Lovibond, S.H. The structure of negative emotional states: Comparison of the Depression Anxiety Stress Scales (DASS) with the Beck Depression and Anxiety Inventories. Behav. Res. Ther. 1995, 33, 335–343. [Google Scholar] [CrossRef]
- Hayes, A.F. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach; Guilford Press: New York, NY, USA, 2013. [Google Scholar]
- McClain, S.; Beasley, S.T.; Jones, B.; Awosogba, O.; Jackson, S.; Cokley, K. An examination of the impact of racial and ethnic identity, imposter feelings, and minority status stress on the mental health of Black college students. J. Multicult. Couns. Dev. 2016, 44, 101–117. [Google Scholar] [CrossRef]
- Blaya, C. Cyberhate: A review and content analysis of intervention strategies. Aggress. Violent Behav. 2019, 45, 163–172. [Google Scholar] [CrossRef]
- Schwartz, J.P.; Griffin, L.D.; Russell, M.M.; Frontaura-Duck, S. Prevention of dating violence on college campuses: An innovative program. J. Coll. Couns. 2006, 9, 90–96. [Google Scholar] [CrossRef]
- Museus, S.D.; Ravello, J.N. Characteristics of academic advising that contribute to racial and ethnic minority student success at predominantly White institutions. NACADA J. 2010, 30, 47–58. [Google Scholar] [CrossRef]
- Mossakowski, K.N. Coping with perceived discrimination: Does ethnic identity protect mental health? J. Health Soc. Behav. 2003, 44, 318–331. [Google Scholar] [CrossRef]
- Rivas-Drake, D.; Hughes, D.; Way, N. A closer look at peer discrimination, ethnic identity, and psychological well-being among urban Chinese American sixth graders. J. Youth Adolesc. 2008, 37, 12–21. [Google Scholar] [CrossRef]
- Yoo, H.C.; Lee, R.M. Ethnic identity and approach-type coping as moderators of the racial discrimination/well-being relation in Asian Americans. J. Couns. Psychol. 2005, 52, 497. [Google Scholar] [CrossRef]
- Cook, C.L.; Franks, A.S. Religious identity and intersectional privilege: (A) symmetric biases in Christians and atheists are unaffected by prompts to consider religious and racial privilege. Psychol. Relig. Spiritual. 2022. advanced online publication. [Google Scholar] [CrossRef]
- Franks, A.S.; Scherr, K.C.; Gibson, B. Godless by association: Deficits in trust mediate antiatheist stigma-by-association. J. Exp. Psychol. Appl. 2019, 25, 303. [Google Scholar] [CrossRef]
- Franks, A.S.; Otani, H.; Roupe, G.T. (A)symmetries in memory and directed forgetting of political stimuli. Exp. Psychol. 2023. advanced online publication. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variable | M | SD | 1 | 2 | 3 | 4 | 5 | 6 | 7 |
|---|---|---|---|---|---|---|---|---|---|
| 1. Perceived Stigma | 5.28 | 1.43 | - | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 |
| 2. Realistic Threat | 2.41 | 0.73 | 0.522 | - | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 |
| 3. Symbolic Threat | 2.68 | 0.84 | 0.576 | 0.614 | - | <0.001 | <0.001 | <0.001 | <0.001 |
| 4. Denial of Racism | 14.75 | 1.17 | −0.579 | −0.561 | −0.609 | - | <0.001 | <0.001 | <0.001 |
| 5. Asian American ID | 17.35 | 0.95 | 0.265 | 0.309 | 0.363 | −0.350 | - | 0.223 | <0.001 |
| 6. Psych Distress | 1.76 | 0.65 | 0.135 | 0.333 | 0.247 | −0.194 | −0.051 | - | <0.001 |
| 7. Behavioral Vigilance | 16.15 | 1.53 | 0.492 | 0.650 | 0.538 | −0.498 | 0.260 | 0.257 | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Franks, A.S.; Nguyen, R.; Xiao, Y.J.; Abbott, D.M. Psychological Distress and Behavioral Vigilance in Response to Minority Stress and Threat among Members of the Asian American and Pacific Islander Community during the COVID-19 Pandemic. Eur. J. Investig. Health Psychol. Educ. 2024, 14, 488-504. https://0-doi-org.brum.beds.ac.uk/10.3390/ejihpe14030033
Franks AS, Nguyen R, Xiao YJ, Abbott DM. Psychological Distress and Behavioral Vigilance in Response to Minority Stress and Threat among Members of the Asian American and Pacific Islander Community during the COVID-19 Pandemic. European Journal of Investigation in Health, Psychology and Education. 2024; 14(3):488-504. https://0-doi-org.brum.beds.ac.uk/10.3390/ejihpe14030033
Chicago/Turabian StyleFranks, Andrew S., Rin Nguyen, Y. Jenny Xiao, and Dena M. Abbott. 2024. "Psychological Distress and Behavioral Vigilance in Response to Minority Stress and Threat among Members of the Asian American and Pacific Islander Community during the COVID-19 Pandemic" European Journal of Investigation in Health, Psychology and Education 14, no. 3: 488-504. https://0-doi-org.brum.beds.ac.uk/10.3390/ejihpe14030033