
Alexithymia as a Risk Factor for an Internet Addiction in Adolescents and Young Adults with Autism Spectrum Disorder
 , , and
, , and
Abstract
:1. Introduction
- (1)
- Difficulties in differentiating emotions and insufficient understanding that selected somatic sensations can be a manifestation of emotional experiences;
- (2)
- Difficulty verbalising emotions;
- (3)
- Limited imagination and fantasy;
- (4)
- Thoughts focused primarily on reality combined with a very limited or complete lack of introspection.
2. Materials and Methods
2.1. Participants
2.2. Methods
- Toronto Alexithymia Scale (TAS-20) [25]—A tool for measuring the severity of alexithymia traits translated and validated for the Polish population by Ścigała D. et al. (2020), in accordance with international guidelines [26]. It is a scale consisting of twenty items, evaluated on a five-point Likert scale, in which 1 means “strongly disagree” and 5 means “strongly agree”. In total, you can get from 20 to 100 points. It is possible to get from 20 to 100 points. The TAS-20 scale measures 3 dimensions of alexithymia: difficulty in identifying emotions (DIF), difficulty in verbalizing emotions (DDF) and tendency to operational thinking style (EOT). The interpretation of individual results is as follows: a score equal to or less than 51 indicates the absence of alexithymia (130 people), 52–60 very likely alexithymia (45 people), while results equal to or greater than 61 indicate alexithymia (54 people).
- Young’s Internet Addiction Test (IAT)—A tool used to assess the degree of Internet addiction [27]. The study used the Polish version of the IAT, validated by Hawi N. et al. (2015) [28]. It is a self-report scale of twenty points, which were assessed on a five-point Likert scale from 1 (rarely) to 5 (always). By answering individual questions, it is possible to get a total of 20 to 100 points. Based on the above test, the following groups of Internet users can be distinguished: below 30 indicates the absence of Internet addiction (49 people), the total results in the range of 31–49 indicate mild addiction (125 people), 50–79 moderate addiction (54 people), while 80–100 indicates severe addiction (1 person).
- Autism spectrum quotient (AQ)—A tool used to measure the severity and profile of features of autism spectrum disorders. The Polish version of the AQ scale was translated by Pisula et al. (2013) [29]. The AQ test consists of 50 statements assessing five different areas: social skills, change of attention, attention to detail, communication, imagination. Participants marked their answers on a four-point Likert scale, with 1 meaning “strongly disagree” and 4 “strongly agree”. The respondent was awarded 1 point for each answer suggesting an autistic trait (poor social skills, poor communication skills, attentiveness, exceptional attention to detail, poor imagination) [30]. A score greater than or equal to 30 points meant an increased intensity of ASD features (26 people) [31].
- In addition, the respondents completed a short demographic questionnaire including questions about age, place of residence, major, field and year of study and type of activity on the Internet. In the question about online activity, the participants had a choice of social media, games, movies/series/livestreams, content creation, exploring interests, learning and other activities.
3. Statistical Analysis and Results
Results
- -
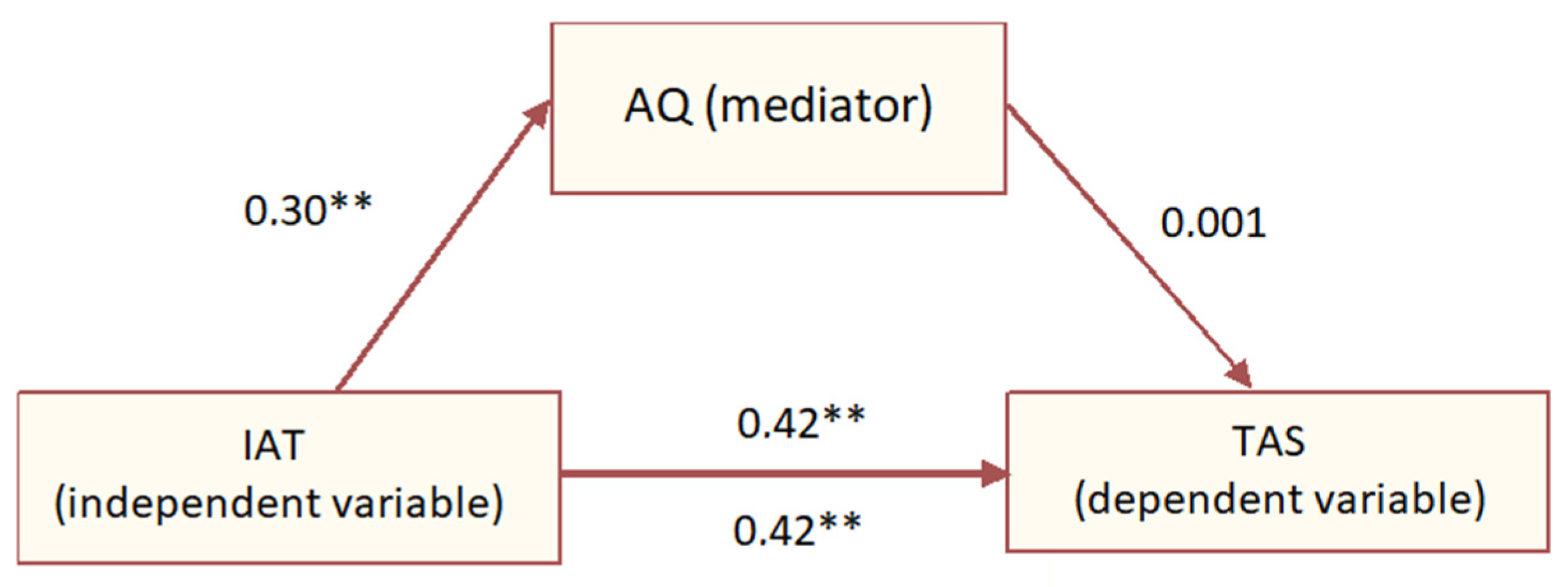
- The presence of ASD features increased the risk of Internet addiction (min. 31 points of the IAT questionnaire) 0.88 times (CI: 0.35–2.19; p > 0.05), this result was statistically insignificant;
- -
- The presence of ASD features increased the risk of alexithymia features (at least 52 points in the TAS-20 questionnaire) 4.36 times (CI: 1.85–10.28; p < 0.05), this result was statistically significant;
- -
- The presence of alexithymia features (min. 52 points in the TAS-20 questionnaire) increased the risk of Internet addiction (min. 31 points in the IAT questionnaire) 2.74 times (95%CI: 1.34–5.58); p < 0.05), this result was statistically significant.
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
References
- Maruszewski, T.; Ścigała, E. Emotions–Alexithymia–Cognition; Humaniora Foundation Publishing House: Poznań, Poland, 1998; pp. 134–238. [Google Scholar]
- Halicka, M.; Herzog-Krzywoszańska, R. Unfathomable emotions—Alexithymia from a neuropsychological perspective. Neuropsychiatr. Neuropsychol. 2016, 11, 72–79. [Google Scholar] [CrossRef]
- Kooiman, C.G.; Spinhoven, P.; Trijsburg, R.W. The assessment of alexithymia: A critical review of the literature and a psychometric study of the Toronto Alexithymia Scale-20. J. Psychosom. Res. 2002, 53, 1083–1090. [Google Scholar] [CrossRef] [PubMed]
- Larsen, J.K.; Brand, N.; Bermond, B.; Hijman, R. Cognitive and emotional characteristics of alexithymia: A review of neurobiological studies. J. Psychosom. Res. 2003, 54, 533–541. [Google Scholar] [CrossRef] [PubMed]
- Hemming, L.; Haddock, G.; Shaw, J.; Pratt, D. Alexithymia and its associations with depression, suicidality, and aggression: An overview of the literature. Front. Psychiatry 2019, 10, 203. [Google Scholar] [CrossRef] [PubMed]
- Berthoz, S.; Hill, E.L. The validity of using self-reports to assess emotion regulation abilities in adults with autism spectrum disorder. Eur. Psychiatry 2005, 20, 291–298. [Google Scholar] [CrossRef] [PubMed]
- Poquérusse, J.; Pastore, L.; Dellantonio, S.; Esposito, G. Corrigendum: Alexithymia and Autism Spectrum Disorder:A Complex Relationship. Front. Psychol. 2018, 9, 1638. [Google Scholar] [CrossRef]
- Doernberg, E.; Hollander, E. Neurodevelopmental Disorders (ASD and ADHD): DSM-5, ICD-10, and ICD-11. CNS Spectrums 2016, 21, 295–299. [Google Scholar] [CrossRef]
- Trambacz-Oleszak, S.; Nosulia, T. Genetic factors in Autism Spectrum Disorders (ASD). Progress Biochem. 2021, 67, 28–33. (In Polish) [Google Scholar] [CrossRef]
- Siegal, M.; Varley, R. Neural systems involved in “theory of mind”. Nat. Rev. Neurosci. 2002, 3, 463–471. [Google Scholar] [CrossRef]
- Bird, G.; Cook, R. Mixed emotions: The contribution of alexithymia to the emotional symptoms of autism. Transl. Psychiatry 2013, 3, e285. [Google Scholar] [CrossRef]
- Brewer, R.; Happé, F.; Cook, R.; Bird, G. Commentary on “Autism, oxytocin and interoception”: Alexithymia, not Autism Spectrum disorders, is the consequence of interoceptive failure. Neurosci. Biobehav. Rev. 2015, 56, 348–353. [Google Scholar] [CrossRef]
- Wijngaarden-Cremers, P.; Gaag, R. Co-Occurring Addictive and Psychiatric Disorders: A Practice-Based Handbook from a European Perspective; Springer: Berlin/Heidelberg, Germany, 2015; pp. 193–204. [Google Scholar] [CrossRef]
- Kervin, R.; Berger, C.; Moon, S.J.; Hill, H.; Park, D.; Kim, J.W. Behavioral addiction and autism spectrum disorder: A systematic review. Res. Dev. Disabil. 2021, 117, 104033. [Google Scholar] [CrossRef] [PubMed]
- Bird, G.; Silani, G.; Brindley, R.; White, S.; Frith, U.; Singer, T. Empathic brain responses in insula are modulated by levels of alexithymia but not autism. Brain 2010, 133, 1515–1525. [Google Scholar] [CrossRef] [PubMed]
- Makaruk, K.; Włodarczyk, J.; Skoneczna, P. Problematic Internet Use by Youth—Research Report; Empowering Children Foundation: Warsaw, Poland, 2019. [Google Scholar]
- Augustynek, A. Computer Addictions. Diagnosis, Prevalence, Therapy; Difin: Warsaw, Poland, 2010. [Google Scholar]
- Woronowicz, B.T. Computer and Internet addictions. In Addiction. Genesis, Therapy, Recovery; Woronowicz, B.T., Ed.; Media Family: Warsaw, Poland, 2009; pp. 548–556. [Google Scholar]
- Young, K.S. Internet addiction: The emergence of a new clinical disorder. CyberPsychology Behav. 1998, 1, 237–244. [Google Scholar] [CrossRef]
- Restrepo, A.; Scheininger, T.; Clucas, J.; Alexander, L.; Salum, G.A.; Georgiades, K.; Paksarian, D.; Merikangas, K.R.; Milham, M.P. Problematic internet use in children and adolescents: Associations with psychiatric disorders and impairment. BMC Psychiatry 2020, 20, 252. [Google Scholar] [CrossRef] [PubMed]
- Coskun, M.; Hajdini, A.; Alnak, A.; Karayagmurlu, A. Internet Use Habits, Parental Control and Psychiatric Comorbidity in Young Subjects with Asperger Syndrome. J. Autism Dev. Disord. 2020, 50, 171–179. [Google Scholar] [CrossRef] [PubMed]
- Pluhar, E.; Kavanaugh, J.R.; A Levinson, J.; Rich, M. Problematic interactive media use in teens: Comorbidities, assessment, and treatment. Psychol. Res. Behav. Manag. 2019, 12, 447–455. [Google Scholar] [CrossRef] [PubMed]
- Hirota, T.; Takahashi, M.; Adachi, M.; Sakamoto, Y.; Nakamura, K. Neurodevelopmental Traits and Longitudinal Transition Patterns in Internet Addiction: A 2-year Prospective Study. J. Autism Dev. Disord. 2021, 51, 1365–1374. [Google Scholar] [CrossRef] [PubMed]
- Mahapatra, A.; Sharma, P. Association of Internet addiction and alexithymia—A scoping review. Addict. Behav. 2018, 81, 175–182. [Google Scholar] [CrossRef]
- Bagby, R.M.; Parker, J.D.A.; Taylor, G.J. The twenty-item Toronto Alexithymia scale—I. Item selection and cross-validation of the factor structure. J. Psychosom. Res. 1994, 38, 23–32. [Google Scholar] [CrossRef]
- Ścigała, D.K.; Zdankiewicz-Ścigała, E.; Bedyńska, S.; Kokoszka, A. Psychometric Properties and Configural Invariance of the Polish—Language Version of the 20-Item Toronto Alexithymia Scale in Non-clinical and Alcohol Addict Persons. Front. Psychol. 2020, 11, 1241. [Google Scholar] [CrossRef]
- Young, K.S. Internet addiction: Symptoms, evaluation and treatment. In Innovations in Clinical Practice: A Source Book; Van de Creek, L., Jackson, C., Eds.; Professional Resource Press: Sarasota, FL, USA, 1999; Volume 17, pp. 19–31. [Google Scholar]
- Hawi, N.S.; Blachnio, A.; Przepiorka, A. Polish validation of the internet addiction test. Comput. Hum. Behav. 2015, 48, 548–553. [Google Scholar] [CrossRef]
- Pisula, E.; Kawa, R.; Shostakevich, Ł.; Lutsk, I.; Kawa, M.; Rynkiewicz, A. Autistic traits in male and female students and individuals with high functioning autism spectrum disorders measured by the Polish version of the autism-spectrum quotient. PLoS ONE 2013, 8, e75236. [Google Scholar] [CrossRef] [PubMed]
- Baron-Cohen, S.; Wheelwright, S.; Skinner, R.; Martin, J.; Clubley, E. The Autism-Spectrum Quotient (AQ): Evidence from Asperger Syndrome/High-Functioning Autism, Males and Females, Scientists and Mathematicians. J. Autism Dev. Disord. 2001, 31, 5–17. [Google Scholar] [CrossRef] [PubMed]
- Baron-Cohen, S.; Hoekstra, R.A.; Knickmeyer, R.; Wheelwright, S. The Autism-Spectrum Quotient (AQ)—Adolescent version. J. Autism Dev. Disord. 2006, 36, 343–350. [Google Scholar] [CrossRef]
- Lotufo Denucci, B.; Silva de Lima, L.; Ferreira Lima Mota, I.; Rocha Madureira Azevedo, J.; Germino Veras, L.; Montenegro Luzardo Bicca, J.V.; de Miranda Santana, B.; Beserra Pinheiro, G.; Gonçalves Coelho, G.; Mortari, M.R. Current knowledge, challenges, new perspectives of the study, and treatments of Autism Spectrum Disorder. Reprod. Toxicol. 2021, 106, 82–93. [Google Scholar] [CrossRef]
- Williams, O.O.F.; Coppolino, M.; Perreault, M.L. Sex differences in neuronal systems function and behaviour: Beyond a single diagnosis in autism spectrum disorders. Transl. Psychiatry 2021, 11, 625. [Google Scholar] [CrossRef]
- Beggiato, A.; Peyre, H.; Maruani, A.; Scheid, I.; Rastam, M.; Amsellem, F.; Gillberg, C.I.; Leboyer, M.; Bourgeron, T.; Gillberg, C.; et al. Gender differences in autism spectrum disorders: Divergence among specific core symptoms. Autism Res. 2017, 10, 680–689. [Google Scholar] [CrossRef]
- Green, R.M.; Travers, A.M.; Howe, Y.; McDougle, C.J. Women and Autism Spectrum Disorder: Diagnosis and Implications for Treatment of Adolescents and Adults. Curr. Psychiatry Rep. 2019, 21, 22. [Google Scholar] [CrossRef]
- Długosz, P. Report from the Second Stage of Research of UP Students. Opinion on Remote Learning and Mental Well-Being; The Institute of Philosophy and Sociology of the Pedagogical University of Cracow: Cracow, Poland, 2020; Available online: https://ifis.up.krakow.pl/wp-content/uploads/sites/9/2020/06/Raport-Studenci-UP-II-etap.pdf (accessed on 27 February 2024).
- Cat, M. Conference Poll Polish. Method, Ethics, Media. Guarding the Polls. Available online: http://nastrazysondazy.uw.edu.pl/konferencja2/M_Kot.pdf?fbclid=IwAR2Y7fUAjIQHbmzkDW5N03-rj1sk3xU2BO1RjK3cJFURUlFPkjhmshceGS0 (accessed on 27 February 2024).
- Levant, R.F.; Hall, R.J.; Williams, C.M.; Hasan, N.T. Sex differences in alexithymia: A review. Psychol. Men Masculinities 2009, 10, 190–203. [Google Scholar] [CrossRef]
- Oakley, B.F.M.; Jones, E.J.H.; Crawley, D.; Charman, T.; Buitelaar, J.; Tillmann, J.; Murphy, D.G.; Loth, E.; EU-AIMS LEAP Group. Alexithymia in autism: Cross-sectional and longitudinal associations with social-communication difficulties, anxiety and depression symptoms. Psychol. Med. 2022, 52, 1458–1470. [Google Scholar] [CrossRef]
- Huang, Y.; Huang, X.; Ebstein, R.P.; Yu, R. Intranasal oxytocin in the treatment of autism spectrum disorders: A multilevel meta-analysis. Neurosci. Biobehav. Rev. 2021, 122, 18–27. [Google Scholar] [CrossRef]
- Luminet, O.; Grynberg, D.; Ruzette, N.; Mikolajczak, M. Personality-dependent effects of oxytocin: Greater social benefits for high alexithymia scorers. Biol. Psychol. 2011, 87, 401–406. [Google Scholar] [CrossRef] [PubMed]
- So, R.; Makino, K.; Fujiwara, M.; Hirota, T.; Ohcho, K.; Ikeda, S.; Tsubouchi, S.; Inagaki, M. The Prevalence of Internet Addiction Among a Japanese Adolescent Psychiatric Clinic Sample with Autism Spectrum Disorder and/or Attention-Deficit Hyperactivity Disorder: A Cross-Sectional Study. J. Autism Dev. Disord. 2017, 47, 2217–2224. [Google Scholar] [CrossRef] [PubMed]
- Scarpazza, C.; Sellitto, M.; di Pellegrino, G. Now or not-now? The influence of alexithymia on intertemporal decision-making. Brain Cogn. 2017, 114, 20–28. [Google Scholar] [CrossRef] [PubMed]
- Marin, M.G.; Nuñez, X.; de Almeida, R.M.M. Internet Addiction and Attention in Adolescents: A Systematic Review. Cyberpsychol. Behav. Soc. Netw. 2021, 24, 237–249. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| N = 229 | b * | Std. Error from b * | b | t (220) | t (220) | p |
|---|---|---|---|---|---|---|
| Absolute term | 39.562 | 6.785 | 5.831 | 0.000 | ||
| Gender | −0.060 | 0.065 | −1.442 | 1.570 | −0.918 | 0.359 |
| Age | −0.038 | 0.062 | −0.564 | 0.210 | −2.680 | 0.008 |
| Place of residence | −0.038 | 0.062 | −0.434 | 0.703 | −0.618 | 0.537 |
| Education | −0.100 | 0.061 | −0.014 | 0.009 | −1.629 | 0.105 |
| Field of study | 0.042 | 0.066 | 0.001 | 0.002 | 0.644 | 0.520 |
| Way of spending time on the internet | −0.115 | 0.062 | −0.782 | 0.421 | −1.860 | 0.064 |
| Level of alexithymia | 0.338 | 0.071 | 0.320 | 0.069 | 4.762 | 0.000 |
| Level of ASD | 0.090 | 0.069 | 0.147 | 0.112 | 1.310 | 0.191 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Skotalczyk, M.A.; Dąbrowska, K.A.; Smorońska-Rypel, J.; Wilczyński, K.M.; Janas-Kozik, M. Alexithymia as a Risk Factor for an Internet Addiction in Adolescents and Young Adults with Autism Spectrum Disorder. Eur. J. Investig. Health Psychol. Educ. 2024, 14, 669-684. https://0-doi-org.brum.beds.ac.uk/10.3390/ejihpe14030044
Skotalczyk MA, Dąbrowska KA, Smorońska-Rypel J, Wilczyński KM, Janas-Kozik M. Alexithymia as a Risk Factor for an Internet Addiction in Adolescents and Young Adults with Autism Spectrum Disorder. European Journal of Investigation in Health, Psychology and Education. 2024; 14(3):669-684. https://0-doi-org.brum.beds.ac.uk/10.3390/ejihpe14030044
Chicago/Turabian StyleSkotalczyk, Magdalena Anna, Karolina Anna Dąbrowska, Joanna Smorońska-Rypel, Krzysztof Maria Wilczyński, and Małgorzata Janas-Kozik. 2024. "Alexithymia as a Risk Factor for an Internet Addiction in Adolescents and Young Adults with Autism Spectrum Disorder" European Journal of Investigation in Health, Psychology and Education 14, no. 3: 669-684. https://0-doi-org.brum.beds.ac.uk/10.3390/ejihpe14030044