
Dentinogenic Specificity in the Preclinical Evaluation of Vital Pulp Treatment Strategies: A Critical Review

Abstract
:1. Introduction
1.1. Clinical Variables in Direct Pulp Capping and Pulpotomy
- i.
- Among various clinical variables that have been accounted as factors playing a role in the outcome of the vital pulp therapy, the most important are issues related to case selection, which remains the most important parameter for the clinical success of exposed pulp treatment [1]. It is generally accepted that prognosis of direct pulp capping or pulpotomy therapies in teeth with pulp exposures remains as one of the most problematic and unpredictable methods of dental treatment. Horsted et al. 1985 reported that pulp survival rates of carefully selected cases treated with calcium hydroxide as capping agent was initially high (more than 80% after 5 years), but they are declining over time [3]. Pulpal exposure due to caries shows very limited potential for pulp survival due to bacterial infection of the pulp for a substantial period of time, which compromises the defense reaction [4]. In the case selection parameter, the different treatment goals of vital pulp therapy in primary and developing permanent teeth might be critically reviewed. Dental treatment of primary teeth must satisfy different goals than treatment for mature permanent teeth, due to the limited life span of primary teeth and their possible relationship to the permanent tooth successor. Although recent advances in primary tooth biology clearly demonstrated that these teeth have also a potential for wound healing with tertiary dentin formation [5], the criteria used for evaluation of PCM have not been re-evaluated and in many cases PCM with different properties are used. Similarly, dental treatment of immature permanent teeth must satisfy different goals than treatment for mature permanent teeth, due to the central role of the pulp in the physiological continuation of root development and in further deposition of primary dentin which strengthens the root dentinal walls. Thus, preservation of pulp vitality is particularly important in the immature permanent teeth, even with very different treatment indications. The absence of toxicity in PCMs and their further ability to minimize pulp inflammation and enhance pulp healing has been recognized as an important factor in the outcome of VPT [6,7,8].
- ii.
- It has been recognized that dental pulp responds to external irritation with the set of stereotypic defensive mechanisms of the connective tissues. Whenever dentin and pulp is affected by caries, a network of inflammatory reactions of pulpal cells, micro-circulation and nerves, restorative procedures and trauma directly affects the outcome of the fundamental defensive mechanisms in the dental pulp. In patho-physiological terms the most significant difference between dental pulp and other connective tissues is the low compliance environment of the dentinal walls and the relatively constant pulp tissue volume [9]. Initial vascular reactions during pulp inflammation (vasodilatation and increased vessel permeability) taking place in the rigid enclosed pulp chamber create conditions of increased hydrostatic tissue pressure. Local reflex reactions due to activation of sensory nerve fibers and subsequent release of vasoactive peptides might be beneficial to the pulp organ under low-grade tissue irritations [10]. However, under prolonged irritation, and despite the oedema-preventing mechanisms [9], dental pulp pressure can quickly suffer irreversible damage. Thus dental pulp healing does not always follow the sequence of events taking place normally in other connective tissues. Since pulp repair is strongly dependent on a number of factors, exacerbation of an initial inflammatory reaction very often leads to general tissue necrosis.
- iii.
- It is well-known that pulpal wound healing depends largely on the extent to which infection can be avoided [2]. Control of pre-operative infection seems to be a prerequisite for the success of vital pulp therapy. Furthermore, the control of post-operative infection depends largely on the integrity of restoration and the ability of healed dentin-pulp complex to withstand the leaking oral bacteria. Thus, the nature of the healing mechanism determines the therapeutic validity of each vital pulp treatment modality and the PCM used. The role of physico-chemical and/or biological properties of PCM in the effective control of post-operative infection still remain an unknown clinical concern.
1.2. Dentinogenesis in Health and Disease
1.3. The Reparative and Regenerative Potential of Traumatized Dentin-Pulp Complex
- -
- Biocompatibility, defined as the absence of toxic effects which can interfere with the overall outcome of the inflammatory process in the pulp, and
- -
- Biological specificity, defined as the ability to signal odontoblast-like cell differentiation and reparative dentin formation instead the indirect stimulation of wound healing with hard tissue formation.
2. Data Sources and Resources Selection
- Unspecified matrix, where the type of newly formed mineralized matrix was characterized as hard tissue/matrix, mineralized tissue/matrix, calcified tissue/matrix or dentin bridge.
- Osteotypic matrix, where the type of newly formed mineralized matrix was characterized as osteodentin, fibrodentin, osteotypic hard tissue/matrix, atubular dentin or reparative dentin without any indication of tubular structure, and
- Dentin-like matrix, where the type of newly formed mineralized matrix was characterized by its tubular structure and was named as reparative dentin, tertiary dentin, new dentin, dentin-like or tubular mineralized tissue/matrix, with indication of presence of elongated formative cells, or odontoblast-like cells or new odontoblasts.
Review

{kind=link}
{kind=link}
{kind=link}
| References | Model | Capping Material(s) | Type of Matrix |
|---|---|---|---|
| Zhang et al. [22] | Rat | MTA, PC | DL |
| Cannon et al. [23] | Monkey | RS, PC | U |
| Swarup et al. [24] | Human | CP, MTA, CH | DL |
| Han et al. [25] | Rat | MTA | DL |
| Tziafa et al. [26] | Pig | MTA, BD | OSD + DL |
| Obeid et al. [27] | Dog | MTA, CP, Other | U |
| Nowicka et al. [28] | Human | BD, MTA | OSD + DL |
| Hutcheson et al. [29] | Human | MTA | U |
| Omar et al. [30] | Dog | FS, Other | U |
| Sushynski et al. [31] | Human | FS, MTA | DL |
| Nowicka et al. [32] | feline | RS, CH | DL |
| Cardoso-Silva et al. [33] | Human | MTA | U |
| Fransson et al. [34] | Human | BMA, CH | OSD + DL |
| Shahravan et al. [35] | Human | MTA | U |
| Zarrabi et al. [36] | Human | MTA, other | DL |
| Shayegan et al. [37] | Pig | HA, CH, FC | U |
| Zealand et al. [38] | Human | FC, MTA | U |
| Zarrabi et al. [39] | Human | MTA, other | DL |
| Parolia et al. [40] | Human | Other, MTA, CH | DL |
| Sakai et al. [41] | Human | MTA, PTC | U |
| Shayegan et al. [42] | Pig | CP, CH, MTA, PTC | U |
| Accorinte et al. [43] | Human | MTA | U |
| Kiatwateeratana et al. [44] | Human | EMP, CH | DL |
| Accorinte et al. [45] | Human | MTA, CH | U |
| Accorinte et al. [46] | Human | MTA, CH | U |
| Moretti et al. [47] | Human | MTA, CH, FC | U |
| Sawicki et al. [48] | Human | MTA, CH | U |
| Nair et al. [49] | Human | MTA or CH | U |
| Lu et al. [50] | Human | RS, CH | DL |
| Min et al. [51] | Human | MTA, CH | DL |
| Fernandes et al. [52] | Human | CH, RS | DL |
| Qudeimat et al. [53] | Human | MTA, CH | U |
| Tziafas et al. [54] | Dog | RS, CH, Other | U |
| Elias et al. [55] | Human | CH, RS | DL |
| Iwamoto et al. [56] | Human | MTA, CH | U |
| Caicedo et al. [57] | Human | MTA | U |
| Silva et al. [58] | Human | RS, CH | DL |
| Piva et al. [59] | Human | CH | OSD + DL |
| Olsson et al. [60] | Human | EMP, CH | U |
| Markovic et al. [61] | Human | FC, CH | U |
| Koliniotou & Tziafas. [62] | Dog | RS, CH | U |
| Maroto et al. [63] | Human | MTA | U |
| Suzuki et al. [64] | Rat | RS, Other | DL |
| Accorinte et al. [65] | Human | CH, RS | DL |
| Menezes et al. [66] | Dog | MTA, PTC | U |
| Agamy et al. [67] | Human | MTA, FC | DL |
| Iohara et al. [68] | Pig | BMA | DL |
| Nakashima et al. [69] | Dog | BMA | DL |
| Salako et al. [70] | Human | BG, MTA, FS, FC | DL |
| Hörsted-Bindslev et al. [71] | Human | RS, CH | DL |
| Scarano et al. [72] | Human | RS, CH, other | DL |
| Tziafas et al. [73] | Dog | MTA | OSD + DL |
| Tziafas et al. [74] | Dog | BMA, Other | OSD + DL |
| Kitasako et al. [75] | Monkey | RS, CH | DL |
| Murray et al. [76] | Monkey | CH, RS | DL |
| Hafez et al. [77] | Monkey | RS, CH | DL |
| Six et al. [78] | Rat | BMA, CH | OSD + DL |
| Nakamura et al. [79] | Pig | CH, EMP | OSD + DL |
| Tziafas et al. [80] | Dog | BMA, HA, CH, Other | OSD + DL |
| Goldberg et al. [81] | Rat | BMA, CH | OSD + DL |
| Lovschall et al. [82] | Rat | BMA, CH | DL |
| Rutherford. [83] | Rat | BMA | DL |
| Blanko et al. [84] | Human | CH | U |
| Pereira et al. [85] | Human | CH, RS | DL |
| Decup et al. [86] | Rat | BMA, CH | DL |
| Waterhouse et al. [87] | Human | FC, CH | DL |
| Hayashi et al. [88] | Rat | CP | OSD + DL |
| Kitasako et al. [89] | Monkey | RS | U |
| Hebling et al. [90] | Human | RS, CH | U |
| Tarim et al. [91] | Monkey | RS, ZOE, CH | U |
| Tziafas et al. [92] | Dog | BMA | OSD + DL |
| Tziafas & Papadimitriou. [93] | Dog | BMA | OSD + DL |
| Jepsen et al. [94] | Pig | BMA, CH | OSD + DL |
| Ford et al. [95] | Monkey | MTA, CH | U |
| Tziafas et al. [96] | Dog | CH | OSD + DL |
| Yoshiba et al. [97] | Human | CH | OSD + DL |
| Tziafas et al. [98] | Dog | BMA | OSD + DL |
| Sasaki & Kawamata-Kido. [99] | Rat | HA, CH | OSD + DL |
| Oguntebi et al. [100] | Pig | BG, CH, BMA, Other | U |
| Yoshimine et al. [101] | Rat | CP, CH | U |
| Yoshiba et al. [102] | Monkey | CP, CH, Other | U |
| Tziafas et al. [103] | Dog | BMA, CH | OSD + DL |
| Nakashima. [104] | Dog | BMA | OSD + DL |
| Tziafas et al. [105] | Dog | BMA | OSD + DL |
| Oguntebi et al. [106] | Pig | BG, BMA, CH | DL |
| Imai et al. [107] | Rat | CP, CH | OSD + DL |
| Lianjia et al. [108] | Bovine | BMA | OSD + DL |
| Rutherford et al. [109] | Monkey | BMA, CH | OSD + DL |
| Robson & Katz. [110] | Rat | BMA | OSD + DL |
| Inoue & Shimono. [111] | Rat | RS | U |
| Tziafas et al. [112] | Dog | BMA | OSD + DL |
| Tziafas et al. [113] | Dog | BMA | OSD + DL |
| Jaber et al. [114] | Rat | HA, CH | DL |
| Furusawa et al. [115] | Human | CP | U |
| Mjor et al. [116] | Monkey | CH | DL |
| Fitzgerald & Heys. [117] | Human | CH | U |
| van Mullem. [118] | Pig | Untreated | OSD + DL |
| Nakashima. [119] | Dog | BMA | OSD + DL |
| Smith et al. [120] | Ferret | BMA | OSD + DL |
| Fitzgerald et al. [121] | Monkey | CH | U |
| Ikami et al. [122] | Monkey | CP | U |
| Tziafas & Kolokuris. [123] | Dog | BMA | OSD + DL |
| Heys et al. [124] | Monkey | CH, Other | U |
| Nakashima. [125] | Dog | BMA | OSD + DL |
| Tziafas. [126] | Dog | CH, other | U |
| Oguntebi et al. [127] | Monkey | BMA, ZOE | U |
| Tziafas & Molyvdas. [128] | Dog | CH | OSD + DL |
| Jean et al. [129] | Pig | CP, HA, CH | OSD + DL |
| Cvek et al. [130] | Monkey | CH, other | OSD + DL |
| Cox et al. [131] | Monkey | RS, others | DL |
| Heide & Kerekes. [132] | Monkey | CH | U |
| Heide & Kerekes. [133] | Monkey | CH | U |
| Cox & Bergenholtz. [134] | Monkey | CH | OSD + DL |
| Schroder U. [20] | Human | CH | OSD + DL |
| Cox et al. [135] | Monkey | CH | U |
| Fuks et al. [136] | Monkey | BMA | OSD + DL |
| Goldberg et al. [137] | Human | CH, CP | U |
| Heide & Mjor. [138] | Human | Others | U |
| Garcia-Godoy et al. [139] | Dog | FC | U |
| Cox et al. [140] | Monkey | CH | U |
| Heys et al. [141] | Monkey | CH, ZOE, CP, Others | DL |
| Inoue et al. [142] | Rat | BMA | U |
| Horsted et al. [143] | Monkey | CH, Other | U |
| Dick & Carmichael. [144] | Dog | BMA | U |
| Fitzgerald. [145] | Monkey | CH | OSD + DL |
| McWalter et al. [146] | Monkey | CH, Others | U |
| Heller et al. [147] | Monkey | CP, CH | U |
| Cotton. [148] | Rat | CH, ZnOE | U |
| Cotton. [149] | Rat | CH | U |
| Tronstad. [150] | Monkey | CH | U |
| Schroder & Sundstrom. [151] | Human | CH | OSD + DL |
| Schroder. [152] | Human | CH | OSD + DL |
| Sella et al. [153] | Rat | CH | U |
| Mc Walter et al. [154] | Monkey | CH, Other | U |
| Stanley & Lundy. [155] | Human | CH | U |
| Anneroth & Bang. [156] | Monkey | BMA | U |
| Tronstad & Mjor. [157] | Monkey | CH, ZOE | U |
| Ulmansky et al. [158] | Human | CH | U |
| Schroder & Granath. [159] | Human | CH | OSD + DL |
| Berkman et al. [160] | Human | Others | U |
| Schroder & Granath. [161] | Human | CH | OSD + DL |
| Ulmansky et al. [162] | Human | CH, other | DL |
| Langer et al. [163] | Human | CH, ZOE | U |
| Bhaskar et al. [164] | Rat | CH, other | U |
| Kakehashi et al. [165] | Rat | Other | DL |
| Kakehashi et al. [18] | Rats | Untreated | U |
| Pisanti & Sciaky. [166] | Dog | CH | U |
| Sciaky & Pisanti. [167] | Dog | CH | U |
| Kalnins & Frisbie. [168] | Human | Untreated | U |
| Berman & Massler. [169] | Rat | CH, ZOE | U |
| Nyborg. [170] | Human, Dog | CH | U |
| Glass & Zander. [18] | Human | CH, ZOE, other | U |
3. Data Analysis
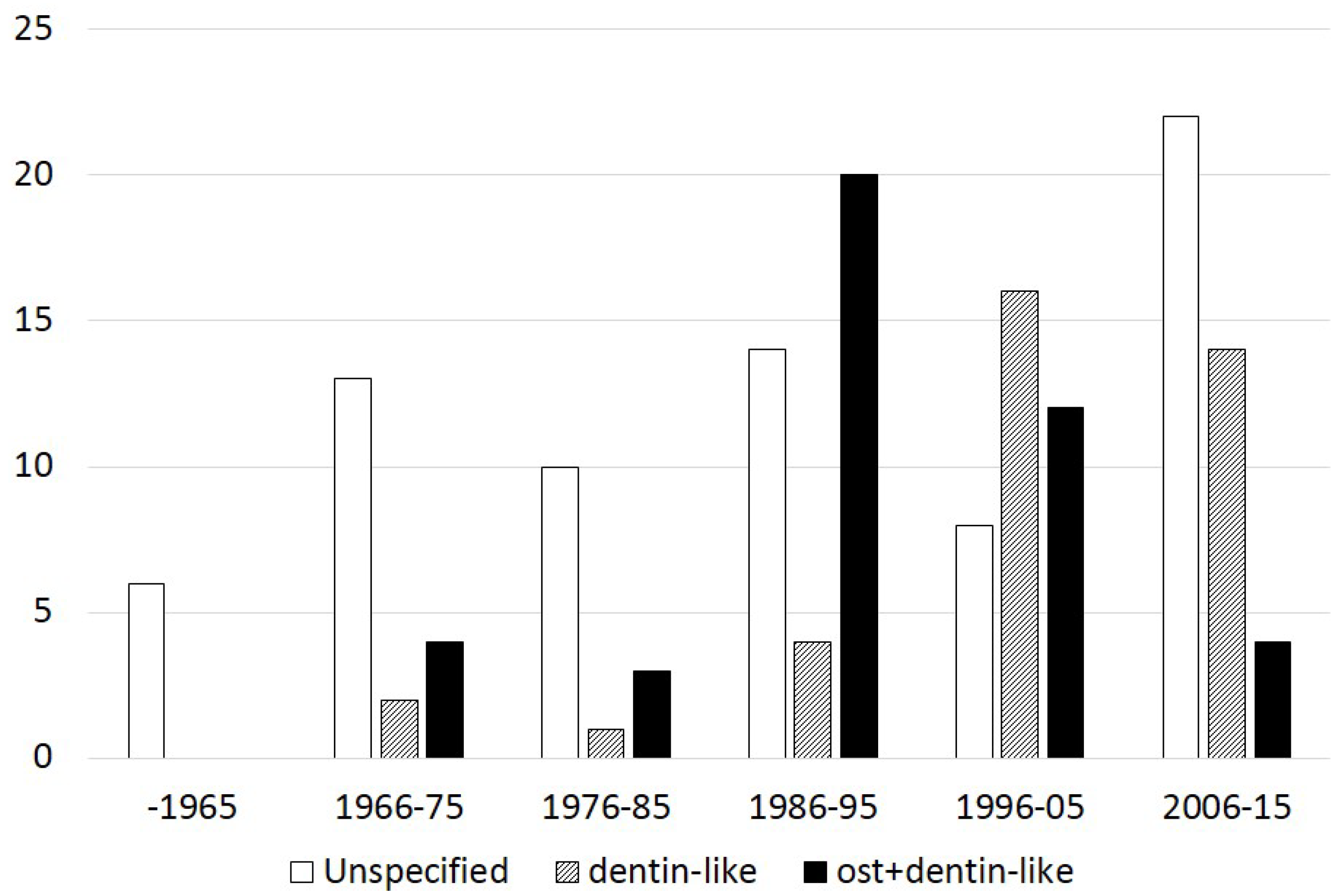
- In 74 (48.3%) studies, only the presence of a mineralized bridge was reported. The type of mineralized matrix was not adequately described and characterized as hard, mineralized or calcified tissue or dentin bridge.
- In 33 (21.6%) studies, the form of the mineralized bridge was evaluated according to morphological or molecular characterization of the newly formed matrix. The type of mineralized matrix was categorized as a dentin-like matrix, but without any information on whether this type of mineralized matrix characterized the whole structure of the mineralized bridge.
- In 46 (30.1%) studies, the form of the mineralized bridge was evaluated according to morphological or molecular characterization of the newly formed matrix, and two types of mineralized matrix have been reported. A firm zone of a mineralized matrix, which was categorized as an osteotypic mineralized matrix, was always followed by the mineralized matrix categorized as dentin-like matrix.



4. Conclusions
Acknowledgments
Conflicts of Interest
References
- Stanley, H.R. Pulp capping: Conserving the dental pulp—Can it be done? Is it worth it? Oral Surg. Oral Med. Oral Pathol. 1989, 68, 628–639. [Google Scholar] [CrossRef]
- Bergenholtz, G. Advances since the paper by Zander and Glass (1949) on the pursuit of healing methods for pulpal exposures: Historical perspectives. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2005, 100, S102–S108. [Google Scholar] [CrossRef] [PubMed]
- Horsted, P.; Sandergaard, B.; Thylstrup, A.; el Attar, K.; Fejerskov, O. A retrospective study of direct pulp capping with calcium hydroxide compounds. Endod. Dent. Traumatol. 1985, 1, 29–34. [Google Scholar] [CrossRef] [PubMed]
- Bergenholtz, G. Factors in pulpal repair after oral exposure. Adv. Dent. Res. 2001, 15, 84. [Google Scholar] [CrossRef] Waterhouse, P.J. “New age” pulp therapy: Personal thoughts on a hot debate. Pediatr. Dent. 2008, 30, 247–252. [Google Scholar] [CrossRef]
- Rutherford, B.R. Regeneration of the Pulp-Dentin complex. In Tissue Engineering. Applications in Maxillofacial Surgery and Periodontics; Lynch, S.E., Genco, R.J., Marx, R.E., Eds.; Quintessence Publishing Co, Inc.: Chicago, IL, USA, 1999; pp. 185–199. [Google Scholar]
- Tziafas, D.; Smith, A.J.; Lesot, H. Designing new treatment strategies in vital pulp therapy. J. Dent. 2000, 28, 77–92. [Google Scholar] [CrossRef]
- Smith, A.J. Vitality of the dentin-pulp complex in health and disease: Growth factors as key mediators. J. Dent. Educ. 2003, 67, 678–689. [Google Scholar] [PubMed]
- Heyeraas, K.J.; Sveen, O.B.; Mjor, I.A. Pulp-dentin biology in restorative dentistry. Part 3: Pulpal inflammation and its sequelae. Quintessence Int. 2001, 32, 611–625. [Google Scholar] [PubMed]
- Olgart, L.M. Functions of peptidergic nerves. In Dynamic Aspects of Dental Pulp; Inoki, R., Kudo, T., Olgart, L.M., Eds.; Chapman and Hall: London, UK, 1990; p. 349. [Google Scholar]
- Ruch, J.V.; Lesot, H.; Begue-Kirn, C. Odontoblast differentiation. Int. J. Dev. Biol. 1995, 39, 51–68. [Google Scholar] [PubMed]
- Thesleff, I.; Vaahtokari, A. The role of growth factors in determination and differentiation of the odontoblastic cell lineage. Proc. Finn. Dent. Soc. 1992, 88 (Suppl. S1), 357–368. [Google Scholar] [PubMed]
- Tziafas, D.; Kodonas, K. Differentiation potential of dental papilla, dental pulp, and apical papilla progenitor cells. J. Endod. 2010, 36, 781–789. [Google Scholar] [CrossRef] [PubMed]
- Goldberg, M.; Smith, A.J. Cells and extracellular matrices of dentin and pulp: A biological basis for repair and tissue engineering. Crit. Rev. Oral Biol. Med. 2004, 15, 13–27. [Google Scholar] [CrossRef] [PubMed]
- Simon, S.; Smith, A.J.; Berdal, A.; Lumley, P.J.; Cooper, P.R. The MAP kinase pathway is involved in odontoblast stimulation via p38 phosphorylation. J. Endod. 2010, 36, 256–259. [Google Scholar] [CrossRef] [PubMed]
- Baume, L.J. The biology of pulp and dentine. In Monographs in Oral Science; Myers, H.M., Ed.; Karger: Basel, Switzerland, 1980; Volume 8, pp. 67–182. [Google Scholar]
- Murray, P.E.; Smith, A.J.; Garcia-Godoy, F.; Lumley, P.J. Comparison of operative procedure variables on pulpal viability in an ex vivo model. Int. Endod. J. 2008, 41, 389–400. [Google Scholar] [CrossRef] [PubMed]
- Kakehashi, S.; Stanley, H.R.; Fitzgerald, R.J. The effects of surgical exposures of dental pulps in germ-free and conventional laboratory rats. Oral Surg. Oral Med. Oral Pathol. 1965, 20, 340–349. [Google Scholar] [CrossRef]
- Smith, A.J.; Scheven, B.A.; Takahashi, Y.; Ferracane, J.L.; Shelton, R.M.; Cooper, P.R. Dentine as a bioactive extracellular matrix. Arch. Oral Biol. 2012, 57, 109–121. [Google Scholar] [CrossRef] [PubMed]
- Schroder, U. Effects of calcium hydroxide-containing pulp-capping agents on pulp cell migration, proliferation, and differentiation. J. Dent. Res. 1985, 64, 541–548. [Google Scholar] [PubMed]
- Lesot, H.; Smith, A.J.; Tziafas, D.; Begue-Kirn, C.; Cassidy, N.; Ruch, J.V. Biologically active molecules and dental tissue repair: A comparative review of reactionary and reparative dentinogenesis with the induction of odontoblast differentiation in vitro. Cells Mater. 1994, 4, 199–218. [Google Scholar]
- Zhang, J.; Zhu, L.X.; Cheng, X.; Lin, Y.; Yan, P.; Peng, B. Promotion of Dental Pulp Cell Migration and Pulp Repair by a Bioceramic Putty Involving FGFR-mediated Signaling Pathways. J. Dent. Res. 2015, 94, 853–862. [Google Scholar] [CrossRef] [PubMed]
- Cannon, M.; Gerodias, N.; Viera, A.; Percinoto, C.; Jurado, R. Primate pulpal healing after exposure and TheraCal application. J. Clin. Pediatr. Dent. 2014, 38, 333–337. [Google Scholar] [CrossRef] [PubMed]
- Swarup, S.J.; Rao, A.; Boaz, K.; Srikant, N.; Shenoy, R. Pulpal response to nano hydroxyapatite, mineral trioxide aggregate and calcium hydroxide when used as a direct pulp capping agent: An in vivo study. J. Clin. Pediatr. Dent. 2014, 38, 201–206. [Google Scholar] [CrossRef] [PubMed]
- Han, N.; Zheng, Y.; Li, R.; Li, X.; Zhou, M.; Niu, Y.; Zhang, Q. Beta-catenin enhances odontoblastic differentiation of dental pulp cells through activation of Runx2. PLoS ONE 2014, 9, e88890. [Google Scholar] [CrossRef] [PubMed]
- Tziafa, C.; Koliniotou-Koumpia, E.; Papadimitriou, S.; Tziafas, D. Dentinogenic responses after direct pulp capping of miniature swine teeth with Biodentine. J. Endod. 2014, 40, 1967–1971. [Google Scholar] [CrossRef] [PubMed]
- Obeid, M.; Saber Sel, D.; Ismael Ael, D.; Hassanien, E. Mesenchymal stem cells promote hard-tissue repair after direct pulp capping. J. Endod. 2013, 39, 626–631. [Google Scholar] [CrossRef] [PubMed]
- Nowicka, A.; Lipski, M.; Parafiniuk, M.; Sporniak-Tutak, K.; Lichota, D.; Kosierkiewicz, A.; Kaczmarek, W.; Buczkowska-Radlinska, J. Response of human dental pulp capped with biodentine and mineral trioxide aggregate. J. Endod. 2013, 39, 743–747. [Google Scholar] [CrossRef] [PubMed]
- Hutcheson, C.; Seale, N.S.; McWhorter, A.; Kerins, C.; Wright, J. Multi-surface composite vs. stainless steel crown restorations after mineral trioxide aggregate pulpotomy: A randomized controlled trial. Pediatr. Dent. 2012, 34, 460–467. [Google Scholar] [PubMed]
- Omar, O.M.; Khattab, N.M.; Khater, D.S. Nigella sativa oil as a pulp medicament for pulpotomized teeth: A histopathological evaluation. J. Clin. Pediatr. Dent. 2012, 36, 335–341. [Google Scholar] [CrossRef] [PubMed]
- Sushynski, J.M.; Zealand, C.M.; Botero, T.M.; Boynton, J.R.; Majewski, R.F.; Shelburne, C.E.; Hu, J.C. Comparison of gray mineral trioxide aggregate and diluted formocresol in pulpotomized primary molars: A 6- to 24-month observation. Pediatr. Dent. 2012, 34, 120–128. [Google Scholar] [PubMed]
- Nowicka, A.; Parafiniuk, M.; Lipski, M.; Lichota, D.; Buczkowska-Radlinska, J. Pulpo-dentin complex response after direct capping with self-etch adhesive systems. Folia Histochem. Cytobiol. Pol. Acad. Sci. Pol. Histochem. Cytochem. Soc. 2012, 50, 565–573. [Google Scholar] [CrossRef]
- Cardoso-Silva, C.; Barberia, E.; Maroto, M.; Garcia-Godoy, F. Clinical study of Mineral Trioxide Aggregate in primary molars. Comparison between Grey and White MTA—A long term follow-up (84 months). J. Dent. 2011, 39, 187–193. [Google Scholar] [CrossRef] [PubMed]
- Fransson, H.; Petersson, K.; Davies, J.R. Dentine sialoprotein and collagen I expression after experimental pulp capping in humans using emdogain gel. Int. Endod. J. 2011, 44, 259–267. [Google Scholar] [CrossRef] [PubMed]
- Shahravan, A.; Jalali, S.P.; Torabi, M.; Haghdoost, A.A.; Gorjestani, H. A histological study of pulp reaction to various water/powder ratios of white mineral trioxide aggregate as pulp-capping material in human teeth: A double-blinded, randomized controlled trial. Int. Endod. J. 2011, 44, 1029–1033. [Google Scholar] [CrossRef] [PubMed]
- Zarrabi, M.H.; Javidi, M.; Jafarian, A.H.; Joushan, B. Immunohistochemical expression of fibronectin and tenascin in human tooth pulp capped with mineral trioxide aggregate and a novel endodontic cement. J. Endod. 2011, 37, 1613–1618. [Google Scholar] [CrossRef] [PubMed]
- Shayegan, A.; Atash, R.; Petein, M.; Abbeele, A.V. Nanohydroxyapatite used as a pulpotomy and direct pulp capping agent in primary pig teeth. J. Dent. Child. 2010, 77, 77–83. [Google Scholar]
- Zealand, C.M.; Briskie, D.M.; Botero, T.M.; Boynton, J.R.; Hu, J.C. Comparing gray mineral trioxide aggregate and diluted formocresol in pulpotomized human primary molars. Pediatr. Dent. 2010, 32, 393–399. [Google Scholar] [PubMed]
- Zarrabi, M.H.; Javidi, M.; Jafarian, A.H.; Joushan, B. Histologic assessment of human pulp response to capping with mineral trioxide aggregate and a novel endodontic cement. J. Endod. 2010, 36, 1778–1781. [Google Scholar] [CrossRef] [PubMed]
- Parolia, A.; Kundabala, M.; Rao, N.N.; Acharya, S.R.; Agrawal, P.; Mohan, M.; Thomas, M. A comparative histological analysis of human pulp following direct pulp capping with Propolis, mineral trioxide aggregate and Dycal. Aust. Dent. J. 2010, 55, 59–64. [Google Scholar] [CrossRef] [PubMed]
- Sakai, V.T.; Moretti, A.B.; Oliveira, T.M.; Fornetti, A.P.; Santos, C.F.; Machado, M.A.; Abdo, R.C. Pulpotomy of human primary molars with MTA and Portland cement: A randomised controlled trial. Br. Dent. J. 2009, 207, 128–129. [Google Scholar] [CrossRef] [PubMed]
- Shayegan, A.; Petein, M.; Vanden Abbeele, A. The use of beta-tricalcium phosphate, white MTA, white Portland cement and calcium hydroxide for direct pulp capping of primary pig teeth. Dent. Traumatol. 2009, 25, 413–419. [Google Scholar] [CrossRef] [PubMed]
- Accorinte, M.L.; Loguercio, A.D.; Reis, A.; Bauer, J.R.; Grande, R.H.; Murata, S.S.; Souza, V.; Holland, R. Evaluation of two mineral trioxide aggregate compounds as pulp-capping agents in human teeth. Int. Endod. J. 2009, 42, 122–128. [Google Scholar] [CrossRef] [PubMed]
- Kiatwateeratana, T.; Kintarak, S.; Piwat, S.; Chankanka, O.; Kamaolmatyakul, S.; Thearmontree, A. Partial pulpotomy on caries-free teeth using enamel matrix derivative or calcium hydroxide: A randomized controlled trial. Int. Endod. J. 2009, 42, 584–592. [Google Scholar] [CrossRef] [PubMed]
- Accorinte Mde, L.; Holland, R.; Reis, A.; Bortoluzzi, M.C.; Murata, S.S.; Dezan, E., Jr.; Souza, V.; Alessandro, L.D. Evaluation of mineral trioxide aggregate and calcium hydroxide cement as pulp-capping agents in human teeth. J. Endod. 2008, 34, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Accorinte, M.L.; Loguercio, A.D.; Reis, A.; Carneiro, E.; Grande, R.H.; Murata, S.S.; Holland, R. Response of human dental pulp capped with MTA and calcium hydroxide powder. Oper. Dent. 2008, 33, 488–495. [Google Scholar] [CrossRef] [PubMed]
- Moretti, A.B.; Sakai, V.T.; Oliveira, T.M.; Fornetti, A.P.; Santos, C.F.; Machado, M.A.; Abdo, R.C. The effectiveness of mineral trioxide aggregate, calcium hydroxide and formocresol for pulpotomies in primary teeth. Int. Endod. J. 2008, 41, 547–555. [Google Scholar] [CrossRef] [PubMed]
- Sawicki, L.; Pameijer, C.H.; Emerich, K.; Adamowicz-Klepalska, B. Histological evaluation of mineral trioxide aggregate and calcium hydroxide in direct pulp capping of human immature permanent teeth. Am. J. Dent. 2008, 21, 262–266. [Google Scholar] [PubMed]
- Nair, P.N.; Duncan, H.F.; Pitt Ford, T.R.; Luder, H.U. Histological, ultrastructural and quantitative investigations on the response of healthy human pulps to experimental capping with mineral trioxide aggregate: A randomized controlled trial. Int. Endod. J. 2008, 41, 128–150. [Google Scholar] [PubMed]
- Lu, Y.; Liu, T.; Li, H.; Pi, G. Histological evaluation of direct pulp capping with a self-etching adhesive and calcium hydroxide on human pulp tissue. Int. Endod. J. 2008, 41, 643–650. [Google Scholar] [CrossRef] [PubMed]
- Min, K.S.; Park, H.J.; Lee, S.K.; Park, S.H.; Hong, C.U.; Kim, H.W.; Lee, H.H.; Kim, E.C. Effect of mineral trioxide aggregate on dentin bridge formation and expression of dentin sialoprotein and heme oxygenase-1 in human dental pulp. J. Endod. 2008, 34, 666–670. [Google Scholar] [CrossRef] [PubMed]
- Fernandes, A.M.; Silva, G.A.; Lopes, N., Jr.; Napimoga, M.H.; Benatti, B.B.; Alves, J.B. Direct capping of human pulps with a dentin bonding system and calcium hydroxide: An immunohistochemical analysis. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2008, 105, 385–390. [Google Scholar] [CrossRef] [PubMed]
- Qudeimat, M.A.; Barrieshi-Nusair, K.M.; Owais, A.I. Calcium hydroxide vs. mineral trioxide aggregates for partial pulpotomy of permanent molars with deep caries. Eur. Arch. Paediatr. Dent. 2007, 8, 99–104. [Google Scholar] [CrossRef] [PubMed]
- Tziafas, D.; Koliniotou-Koumpia, E.; Tziafa, C.; Papadimitriou, S. Effects of a new antibacterial adhesive on the repair capacity of the pulp-dentine complex in infected teeth. Int. Endod. J. 2007, 40, 58–66. [Google Scholar] [CrossRef] [PubMed]
- Elias, R.V.; Demarco, F.F.; Tarquinio, S.B.; Piva, E. Pulp responses to the application of a self-etching adhesive in human pulps after controlling bleeding with sodium hypochlorite. Quintessence Int. 2007, 38, e67–e77. [Google Scholar] [PubMed]
- Iwamoto, C.E.; Adachi, E.; Pameijer, C.H.; Barnes, D.; Romberg, E.E.; Jefferies, S. Clinical and histological evaluation of white ProRoot MTA in direct pulp capping. Am. J. Dent. 2006, 19, 85–90. [Google Scholar] [PubMed]
- Caicedo, R.; Abbott, P.V.; Alongi, D.J.; Alarcon, M.Y. Clinical, radiographic and histological analysis of the effects of mineral trioxide aggregate used in direct pulp capping and pulpotomies of primary teeth. Aust. Dent. J. 2006, 51, 297–305. [Google Scholar] [CrossRef] [PubMed]
- Silva, G.A.; Lanza, L.D.; Lopes-Junior, N.; Moreira, A.; Alves, J.B. Direct pulp capping with a dentin bonding system in human teeth: A clinical and histological evaluation. Oper. Dent. 2006, 31, 297–307. [Google Scholar] [CrossRef] [PubMed]
- Piva, E.; Tarquinio, S.B.; Demarco, F.F.; Silva, A.F.; de Araujo, V.C. Immunohistochemical expression of fibronectin and tenascin after direct pulp capping with calcium hydroxide. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2006, 102, e66–e71. [Google Scholar] [CrossRef] [PubMed]
- Olsson, H.; Davies, J.R.; Holst, K.E.; Schroder, U.; Petersson, K. Dental pulp capping: Effect of Emdogain Gel on experimentally exposed human pulps. Int. Endod. J. 2005, 38, 186–194. [Google Scholar] [CrossRef] [PubMed]
- Markovic, D.; Zivojinovic, V.; Vucetic, M. Evaluation of three pulpotomy medicaments in primary teeth. Eur. J. Paediatr. Dent. 2005, 6, 133–138. [Google Scholar] [PubMed]
- Koliniotou-Koumpia, E.; Tziafas, D. Pulpal responses following direct pulp capping of healthy dog teeth with dentine adhesive systems. J. Dent. 2005, 33, 639–647. [Google Scholar] [CrossRef] [PubMed]
- Maroto, M.; Barberia, E.; Planells, P.; Garcia Godoy, F. Dentin bridge formation after mineral trioxide aggregate (MTA) pulpotomies in primary teeth. Am. J. Dent. 2005, 18, 151–154. [Google Scholar] [PubMed]
- Suzuki, M.; Katsumi, A.; Watanabe, R.; Shirono, M.; Katoh, Y. Effects of an experimentally developed adhesive resin system and CO2 laser irradiation on direct pulp capping. Oper. Dent. 2005, 30, 702–718. [Google Scholar] [PubMed]
- Accorinte Mde, L.; Loguercio, A.D.; Reis, A.; Muench, A.; de Araujo, V.C. Response of human pulp capped with a bonding agent after bleeding control with hemostatic agents. Oper. Dent. 2005, 30, 147–155. [Google Scholar] [PubMed]
- Menezes, R.; Bramante, C.M.; Letra, A.; Carvalho, V.G.; Garcia, R.B. Histologic evaluation of pulpotomies in dog using two types of mineral trioxide aggregate and regular and white Portland cements as wound dressings. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2004, 98, 376–379. [Google Scholar] [CrossRef]
- Agamy, H.A.; Bakry, N.S.; Mounir, M.M.; Avery, D.R. Comparison of mineral trioxide aggregate and formocresol as pulp-capping agents in pulpotomized primary teeth. Pediatr. Dent. 2004, 26, 302–309. [Google Scholar] [PubMed]
- Iohara, K.; Nakashima, M.; Ito, M.; Ishikawa, M.; Nakasima, A.; Akamine, A. Dentin regeneration by dental pulp stem cell therapy with recombinant human bone morphogenetic protein 2. J. Dent. Res. 2004, 83, 590–595. [Google Scholar] [CrossRef] [PubMed]
- Nakashima, M.; Tachibana, K.; Iohara, K.; Ito, M.; Ishikawa, M.; Akamine, A. Induction of reparative dentin formation by ultrasound-mediated gene delivery of growth/differentiation factor 11. Hum. Gene Ther. 2003, 14, 591–597. [Google Scholar] [CrossRef] [PubMed]
- Salako, N.; Joseph, B.; Ritwik, P.; Salonen, J.; John, P.; Junaid, T.A. Comparison of bioactive glass, mineral trioxide aggregate, ferric sulfate, and formocresol as pulpotomy agents in rat molar. Dent. Traumatol. 2003, 19, 314–320. [Google Scholar] [CrossRef] [PubMed]
- Horsted-Bindslev, P.; Vilkinis, V.; Sidlauskas, A. Direct capping of human pulps with a dentin bonding system or with calcium hydroxide cement. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2003, 96, 591–600. [Google Scholar] [CrossRef]
- Scarano, A.; Manzon, L.; Di Giorgio, R.; Orsini, G.; Tripodi, D.; Piattelli, A. Direct capping with four different materials in humans: Histological analysis of odontoblast activity. J. Endod. 2003, 29, 729–734. [Google Scholar] [CrossRef] [PubMed]
- Tziafas, D.; Pantelidou, O.; Alvanou, A.; Belibasakis, G.; Papadimitriou, S. The dentinogenic effect of mineral trioxide aggregate (MTA) in short-term capping experiments. Int. Endod. J. 2002, 35, 245–254. [Google Scholar] [CrossRef] [PubMed]
- Tziafas, D.; Kalyva, M.; Papadimitriou, S. Experimental dentin-based approaches to tissue regeneration in vital pulp therapy. Connect. Tissue Res. 2002, 43, 391–395. [Google Scholar] [CrossRef] [PubMed]
- Kitasako, Y.; Murray, P.E.; Tagami, J.; Smith, A.J. Histomorphometric analysis of dentinal bridge formation and pulpal inflammation. Quintessence Int. 2002, 33, 600–608. [Google Scholar] [PubMed]
- Murray, P.E.; Hafez, A.A.; Windsor, L.J.; Smith, A.J.; Cox, C.F. Comparison of pulp responses following restoration of exposed and non-exposed cavities. J. Dent. 2002, 30, 213–222. [Google Scholar] [CrossRef]
- Hafez, A.A.; Cox, C.F.; Tarim, B.; Otsuki, M.; Akimoto, N. An in vivo evaluation of hemorrhage control using sodium hypochlorite and direct capping with a one- or two-component adhesive system in exposed nonhuman primate pulps. Quintessence Int. 2002, 33, 261–272. [Google Scholar] [PubMed]
- Six, N.; Lasfargues, J.J.; Goldberg, M. Differential repair responses in the coronal and radicular areas of the exposed rat molar pulp induced by recombinant human bone morphogenetic protein 7 (osteogenic protein 1). Arch. Oral Biol. 2002, 47, 177–187. [Google Scholar] [CrossRef]
- Nakamura, Y.; Hammarstrom, L.; Matsumoto, K.; Lyngstadaas, S.P. The induction of reparative dentine by enamel proteins. Int. Endod. J. 2002, 35, 407–417. [Google Scholar] [CrossRef] [PubMed]
- Tziafas, D.; Belibasakis, G.; Veis, A.; Papadimitriou, S. Dentin regeneration in vital pulp therapy: Design principles. Adv. Dent. Res. 2001, 15, 96–100. [Google Scholar] [CrossRef] [PubMed]
- Goldberg, M.; Six, N.; Decup, F.; Buch, D.; Soheili Majd, E.; Lasfargues, J.J.; Salih, E.; Stanislawski, L. Application of bioactive molecules in pulp-capping situations. Adv. Dent. Res. 2001, 15, 91–95. [Google Scholar] [CrossRef] [PubMed]
- Lovschall, H.; Fejerskov, O.; Flyvbjerg, A. Pulp-capping with recombinant human insulin-like growth factor I (rhIGF-I) in rat molars. Adv. Dent. Res. 2001, 15, 108–112. [Google Scholar] [CrossRef] [PubMed]
- Rutherford, R.B. BMP-7 gene transfer to inflamed ferret dental pulps. Eur. J. Oral Sci. 2001, 109, 422–424. [Google Scholar] [CrossRef] [PubMed]
- Blanco, L.; Cohen, S. Treatment of crown fractures with exposed pulps. J. Calif. Dent. Assoc. 2002, 30, 419–425. [Google Scholar] [PubMed]
- Pereira, J.C.; Segala, A.D.; Costa, C.A. Human pulpal response to direct pulp capping with an adhesive system. Am. J. Dent. 2000, 13, 139–147. [Google Scholar] [PubMed]
- Decup, F.; Six, N.; Palmier, B.; Buch, D.; Lasfargues, J.J.; Salih, E.; Goldberg, M. Bone sialoprotein-induced reparative dentinogenesis in the pulp of rat’s molar. Clin. Oral Investig. 2000, 4, 110–119. [Google Scholar] [CrossRef] [PubMed]
- Waterhouse, P.J.; Nunn, J.H.; Whitworth, J.M.; Soames, J.V. Primary molar pulp therapy—Histological evaluation of failure. Int. J. Paediatr. Dent./Br. Paedodontic Soc. Int. Assoc. Dent. Child. 2000, 10, 313–321. [Google Scholar] [CrossRef]
- Hayashi, Y.; Imai, M.; Yanagiguchi, K.; Viloria, I.L.; Ikeda, T. Hydroxyapatite applied as direct pulp capping medicine substitutes for osteodentin. J. Endod. 1999, 25, 225–229. [Google Scholar] [CrossRef]
- Kitasako, Y.; Inokoshi, S.; Tagami, J. Effects of direct resin pulp capping techniques on short-term response of mechanically exposed pulps. J. Dent. 1999, 27, 257–263. [Google Scholar] [CrossRef]
- Hebling, J.; Giro, E.M.; Costa, C.A. Biocompatibility of an adhesive system applied to exposed human dental pulp. J. Endod. 1999, 25, 676–682. [Google Scholar] [CrossRef]
- Tarim, B.; Hafez, A.A.; Cox, C.F. Pulpal response to a resin-modified glass-ionomer material on nonexposed and exposed monkey pulps. Quintessence Int. 1998, 29, 535–542. [Google Scholar] [PubMed]
- Tziafas, D.; Alvanou, A.; Papadimitriou, S.; Gasic, J.; Komnenou, A. Effects of recombinant basic fibroblast growth factor, insulin-like growth factor-II and transforming growth factor-beta 1 on dog dental pulp cells in vivo. Arch. Oral Biol. 1998, 43, 431–444. [Google Scholar] [CrossRef]
- Tziafas, D.; Papadimitriou, S. Role of exogenous TGF-beta in induction of reparative dentinogenesis in vivo. Eur. J. Oral Sci. 1998, 106 (Suppl. S1), 192–196. [Google Scholar] [CrossRef] [PubMed]
- Jepsen, S.; Albers, H.K.; Fleiner, B.; Tucker, M.; Rueger, D. Recombinant human osteogenic protein-1 induces dentin formation: An experimental study in miniature swine. J. Endod. 1997, 23, 378–382. [Google Scholar] [CrossRef]
- Ford, T.R.; Torabinejad, M.; Abedi, H.R.; Bakland, L.K.; Kariyawasam, S.P. Using mineral trioxide aggregate as a pulp-capping material. J. Am. Dent. Assoc. 1996, 127, 1491–1494. [Google Scholar] [CrossRef] [PubMed]
- Tziafas, D.; Veis, A.; Alvanou, A. Inability of calcium hydroxide to induce reparative dentinogenesis at non-peripheral sites of dog dental pulp. Eur. J. Oral Sci. 1996, 104, 623–626. [Google Scholar] [CrossRef] [PubMed]
- Yoshiba, K.; Yoshiba, N.; Nakamura, H.; Iwaku, M.; Ozawa, H. Immunolocalization of fibronectin during reparative dentinogenesis in human teeth after pulp capping with calcium hydroxide. J. Dent. Res. 1996, 75, 1590–1597. [Google Scholar] [CrossRef] [PubMed]
- Tziafas, D.; Alvanou, A.; Panagiotakopoulos, N.; Smith, A.J.; Lesot, H.; Komnenou, A.; Ruch, J.V. Induction of odontoblast-like cell differentiation in dog dental pulps after in vivo implantation of dentine matrix components. Arch. Oral Biol. 1995, 40, 883–893. [Google Scholar] [CrossRef]
- Sasaki, T.; Kawamata-Kido, H. Providing an environment for reparative dentine induction in amputated rat molar pulp by high molecular-weight hyaluronic acid. Arch. Oral Biol. 1995, 40, 209–219. [Google Scholar] [CrossRef]
- Oguntebi, B.R.; Heaven, T.; Clark, A.E.; Pink, F.E. Quantitative assessment of dentin bridge formation following pulp-capping in miniature swine. J. Endod. 1995, 21, 79–82. [Google Scholar] [CrossRef]
- Yoshimine, Y.; Maeda, K. Histologic evaluation of tetracalcium phosphate-based cement as a direct pulp-capping agent. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 1995, 79, 351–358. [Google Scholar] [CrossRef]
- Yoshiba, K.; Yoshiba, N.; Iwaku, M. Effects of antibacterial capping agents on dental pulps of monkeys mechanically exposed to oral microflora. J. Endod. 1995, 21, 16–20. [Google Scholar] [CrossRef]
- Tziafas, D.; Panagiotakopoulos, N.; Komnenou, A. Immunolocalization of fibronectin during the early response of dog dental pulp to demineralized dentine or calcium hydroxide-containing cement. Arch. Oral Biol. 1995, 40, 23–31. [Google Scholar] [CrossRef]
- Nakashima, M. Induction of dentin formation on canine amputated pulp by recombinant human bone morphogenetic proteins (BMP)-2 and -4. J. Dent. Res. 1994, 73, 1515–1522. [Google Scholar] [PubMed]
- Tziafas, D.; Lambrianidis, T.; Beltes, P. Inductive effect of native dentin on the dentinogenic potential of adult dog teeth. J. Endod. 1993, 19, 116–122. [Google Scholar] [CrossRef]
- Oguntebi, B.; Clark, A.; Wilson, J. Pulp capping with Bioglass and autologous demineralized dentin in miniature swine. J. Dent. Res. 1993, 72, 484–489. [Google Scholar] [CrossRef] [PubMed]
- Imai, M.; Hayashi, Y. Ultrastructure of wound healing following direct pulp capping with calcium-beta-glycerophosphate (Ca-BGP). J. Oral Pathol. Med. 1993, 22, 411–417. [Google Scholar] [CrossRef] [PubMed]
- Lianjia, Y.; Yuhao, G.; White, F.H. Bovine bone morphogenetic protein-induced dentinogenesis. Clin. Orthop. Relat. Res. 1993, 295, 305–312. [Google Scholar] [CrossRef] [PubMed]
- Rutherford, R.B.; Wahle, J.; Tucker, M.; Rueger, D.; Charette, M. Induction of reparative dentine formation in monkeys by recombinant human osteogenic protein-1. Arch. Oral Biol. 1993, 38, 571–576. [Google Scholar] [CrossRef]
- Robson, W.C.; Katz, R.W. Preliminary studies on pulp capping with demineralized dentin. Proc. Finn. Dent. Soc. 1992, 88 (Suppl. S1), 279–283. [Google Scholar] [PubMed]
- Inoue, T.; Shimono, M. Repair dentinogenesis following transplantation into normal and germ-free animals. Proc. Finn. Dent. Soc. 1992, 88 (Suppl. S1), 183–194. [Google Scholar] [PubMed]
- Tziafas, D.; Kolokuris, I.; Alvanou, A.; Kaidoglou, K. Short-term dentinogenic response of dog dental pulp tissue after its induction by demineralized or native dentine, or predentine. Arch. Oral Biol. 1992, 37, 119–128. [Google Scholar] [CrossRef]
- Tziafas, D.; Alvanou, A.; Kaidoglou, K. Dentinogenic activity of allogenic plasma fibronectin on dog dental pulp. J. Dent. Res. 1992, 71, 1189–1195. [Google Scholar] [CrossRef] [PubMed]
- Jaber, L.; Mascres, C.; Donohue, W.B. Reaction of the dental pulp to hydroxyapatite. Oral Surg. Oral Med. Oral Pathol. 1992, 73, 92–98. [Google Scholar] [CrossRef]
- Furusawa, M.; Nakagawa, K.; Asai, Y. Clinico-pathological studies on the tissue reactions of human pulp treated with various kinds of calcium phosphate ceramics. Bull. Tokyo Dent. Coll. 1991, 32, 111–120. [Google Scholar] [PubMed]
- Mjor, I.A.; Dahl, E.; Cox, C.F. Healing of pulp exposures: An ultrastructural study. J. Oral Pathol. Med. 1991, 20, 496–501. [Google Scholar] [CrossRef] [PubMed]
- Fitzgerald, M.; Heys, R.J. A clinical and histological evaluation of conservative pulpal therapy in human teeth. Oper. Dent. 1991, 16, 101–112. [Google Scholar] [PubMed]
- Van Mullem, P.J. Healing of the guinea pig incisor after partial pulp removal. Endod. Dent. Traumatol. 1991, 7, 164–176. [Google Scholar] [CrossRef] [PubMed]
- Nakashima, M. The induction of reparative dentine in the amputated dental pulp of the dog by bone morphogenetic protein. Arch. Oral Biol. 1990, 35, 493–497. [Google Scholar] [CrossRef]
- Smith, A.J.; Tobias, R.S.; Plant, C.G.; Browne, R.M.; Lesot, H.; Ruch, J.V. In vivo morphogenetic activity of dentine matrix proteins. J. Biol. Buccale 1990, 18, 123–129. [Google Scholar] [PubMed]
- Fitzgerald, M.; Chiego, D.J., Jr.; Heys, D.R. Autoradiographic analysis of odontoblast replacement following pulp exposure in primate teeth. Arch. Oral Biol. 1990, 35, 707–715. [Google Scholar] [CrossRef]
- Ikami, K.; Iwaku, M.; Ozawa, H. An ultrastructural study of the process of hard tissue formation in amputated dental pulp dressed with alpha-tricalcium phosphate. Arch. Histol. Cytol. 1990, 53, 227–243. [Google Scholar] [CrossRef] [PubMed]
- Tziafas, D.; Kolokuris, I. Inductive influences of demineralized dentin and bone matrix on pulp cells: An approach of secondary dentinogenesis. J. Dent. Res. 1990, 69, 75–81. [Google Scholar] [CrossRef] [PubMed]
- Heys, D.R.; Fitzgerald, M.; Heys, R.J.; Chiego, D.J., Jr. Healing of primate dental pulps capped with Teflon. Oral Surg. Oral Med. Oral Pathol. 1990, 69, 227–237. [Google Scholar] [CrossRef]
- Nakashima, M. Dentin induction by implants of autolyzed antigen-extracted allogeneic dentin on amputated pulps of dogs. Endod. Dent. Traumatol. 1989, 5, 279–286. [Google Scholar] [CrossRef] [PubMed]
- Tziafas, D. Experimental bacterial anachoresis in dog dental pulps capped with calcium hydroxide. J. Endod. 1989, 15, 591–595. [Google Scholar] [CrossRef]
- Oguntebi, B.R.; Dover, M.S.; Franklin, C.J.; Tuwaijri, A.S. The effect of collagen and indomethacin on inflamed dental pulp wounds of baboon teeth. Oral Surg. Oral Med. Oral Pathol. 1988, 65, 233–239. [Google Scholar] [CrossRef]
- Tziafas, D.; Molyvdas, I. The tissue reactions after capping of dog teeth with calcium hydroxide experimentally crammed into the pulp space. Oral Surg. Oral Med. Oral Pathol. 1988, 65, 604–608. [Google Scholar] [CrossRef]
- Jean, A.; Kerebel, B.; Kerebel, L.M.; Legeros, R.Z.; Hamel, H. Effects of various calcium phosphate biomaterials on reparative dentin bridge formation. J. Endod. 1988, 14, 83–87. [Google Scholar] [CrossRef]
- Cvek, M.; Granath, L.; Cleaton-Jones, P.; Austin, J. Hard tissue barrier formation in pulpotomized monkey teeth capped with cyanoacrylate or calcium hydroxide for 10 and 60 minutes. J. Dent. Res. 1987, 66, 1166–1174. [Google Scholar] [CrossRef] [PubMed]
- Cox, C.F.; Keall, C.L.; Keall, H.J.; Ostro, E.; Bergenholtz, G. Biocompatibility of surface-sealed dental materials against exposed pulps. J. Prosthet. Dent. 1987, 57, 1–8. [Google Scholar] [CrossRef]
- Heide, S.; Kerekes, K. Delayed direct pulp capping in permanent incisors of monkeys. Int. Endod. J. 1987, 20, 65–74. [Google Scholar] [CrossRef] [PubMed]
- Heide, S.; Kerekes, K. Delayed partial pulpotomy in permanent incisors of monkeys. Int. Endod. J. 1986, 19, 78–89. [Google Scholar] [CrossRef]
- Cox, C.F.; Bergenholtz, G. Healing sequence in capped inflamed dental pulps of Rhesus monkeys (Macaca mulatta). Int. Endod. J. 1986, 19, 113–120. [Google Scholar] [CrossRef] [PubMed]
- Cox, C.F.; Bergenholtz, G.; Heys, D.R.; Syed, S.A.; Fitzgerald, M.; Heys, R.J. Pulp capping of dental pulp mechanically exposed to oral microflora: A 1–2 year observation of wound healing in the monkey. J. Oral Pathol. 1985, 14, 156–168. [Google Scholar] [CrossRef] [PubMed]
- Fuks, A.B.; Michaeli, Y.; Sofer-Saks, B.; Shoshan, S. Enriched collagen solution as a pulp dressing in pulpotomized teeth in monkeys. Pediatr. Dent. 1984, 6, 243–247. [Google Scholar] [PubMed]
- Goldberg, F.; Massone, E.J.; Spielberg, C. Evaluation of the dentinal bridge after pulpotomy and calcium hydroxide dressing. J. Endod. 1984, 10, 318–320. [Google Scholar] [CrossRef]
- Heide, S.; Mjor, I.A. Pulp reactions to experimental exposures in young permanent monkey teeth. Int. Endod. J. 1983, 16, 11–19. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Godoy, F.; Novakovic, D.P.; Carvajal, I.N. Pulpal response to different application times of formocresol. J. Pedodontics 1982, 6, 176–193. [Google Scholar]
- Cox, C.F.; Bergenholtz, G.; Fitzgerald, M.; Heys, D.R.; Heys, R.J.; Avery, J.K.; Baker, J.A. Capping of the dental pulp mechanically exposed to the oral microflora—A 5 week observation of wound healing in the monkey. J. Oral Pathol. 1982, 11, 327–339. [Google Scholar] [CrossRef] [PubMed]
- Heys, D.R.; Cox, C.F.; Heys, R.J.; Avery, J.K. Histological considerations of direct pulp capping agents. J. Dent. Res. 1981, 60, 1371–1379. [Google Scholar] [CrossRef] [PubMed]
- Inoue, T.; Sasaki, A.; Shimono, M.; Yamamura, T. Bone morphogenesis induced by implantation of dentin and cortical bone matrices. Bull. Tokyo Dent. Coll. 1981, 22, 213–221. [Google Scholar] [PubMed]
- Horsted, P.; el Attar, K.; Langeland, K. Capping of monkey pulps with Dycal and a Ca-eugenol cement. Oral Surg. Oral Med. Oral Pathol. 1981, 52, 531–553. [Google Scholar] [CrossRef]
- Dick, H.M.; Carmichael, D.J. Reconstituted antigen-poor collagen preparations as potential pulp-capping agents. J. Endod. 1980, 6, 641–644. [Google Scholar] [CrossRef]
- Fitzgerald, M. Cellular mechanics of dentinal bridge repair using 3H-thymidine. J. Dent. Res. 1979, 58, 2198–2206. [Google Scholar] [CrossRef] [PubMed]
- McWalter, G.M.; el-Kafrawy, A.H.; Mitchell, D.F. Long-term study of pulp capping in monkeys with three agents. J. Am. Dental Assoc. 1976, 93, 105–110. [Google Scholar] [CrossRef]
- Heller, A.L.; Koenigs, J.F.; Brilliant, J.D.; Melfi, R.C.; Driskell, T.D. Direct pulp capping of permanent teeth in primates using a resorbable form of tricalcium phosphate ceramic. J. Endod. 1975, 1, 95–101. [Google Scholar] [CrossRef]
- Cotton, W.R. Bacterial contamination as a factor in healing of pulp exposures. Oral Surg. Oral Med. Oral Pathol. 1974, 38, 441–450. [Google Scholar] [CrossRef]
- Cotton, W.R.; Kueter, K.E. Penicillin prophylaxis as an adjunct to the capping of pulps infected with Streptococcus mutans. Oral Surg. Oral Med. Oral Pathol. 1974, 38, 618–622. [Google Scholar] [CrossRef]
- Tronstad, L. Reaction of the exposed pulp to Dycal treatment. Oral Surg. Oral Med. Oral Pathol. 1974, 38, 945–953. [Google Scholar] [CrossRef]
- Schroder, U.; Sundstrom, B. Transmission electron microscopy of tissue changes following experimental pulpotomy of intact human teeth and capping with calcium hydroxide. Odontol. Rev. 1974, 25, 57–68. [Google Scholar]
- Schröder, U. Reaction of human dental pulp to experimental pulpotomy and capping with calcium hydroxide. Odontol. Rev. 1973, 24, 5–22. [Google Scholar]
- Sela, J.; Hirschfeld, Z.; Ulmansky, M. Reaction of the rat molar pulp to direct capping with the separate components of Hydrex. Oral Surg. Oral Med. Oral Pathol. 1973, 35, 118–122. [Google Scholar] [CrossRef]
- McWalter, G.M.; el-Kafrawy, A.H.; Mitchell, D.F. Pulp capping in monkeys with a calcium-hydroxide compound, an antibiotic, and a polycarboxylate cement. Oral Surg. Oral Med. Oral Pathol. 1973, 36, 90–100. [Google Scholar] [CrossRef]
- Stanley, H.R.; Lundy, T. Dycal therapy for pulp exposures. Oral Surg. Oral Med. Oral Pathol. 1972, 34, 818–827. [Google Scholar] [CrossRef]
- Anneroth, G.; Bang, G. The effect of allogeneic demineralized dentin as a pulp capping agent in Java monkeys. Odontol. Rev. 1972, 23, 315–328. [Google Scholar]
- Tronstad, L.; Mjor, I.A. Capping of the inflamed pulp. Oral Surg. Oral Med. Oral Pathol. 1972, 34, 477–485. [Google Scholar] [CrossRef]
- Ulmansky, M.; Sela, J.; Sela, M. Scanning electron microscopy of calcium hydroxide induced bridges. J. Oral Pathol. 1972, 1, 244–248. [Google Scholar] [CrossRef] [PubMed]
- Schroder, U.; Granath, L.E. Scanning electron microscopy of hard tissue barrier following experimental pulpotomy of intact human teeth and capping with calcium hydroxide. Odontol. Rev. 1972, 23, 211–220. [Google Scholar]
- Berkman, M.D.; Cucolo, F.A.; Levin, M.P.; Brunelle, L.J. Pulpal response to isobutyl cyanoacrylate in human teeth. J. Am. Dent. Assoc. 1971, 83, 140–145. [Google Scholar] [CrossRef] [PubMed]
- Schroder, U.; Granath, L.E. Early reaction of intact human teeth to calcium hydroxide following experimental pulpotomy and its significance to the development of hard tissue barrier. Odontol. Rev. 1971, 22, 379–395. [Google Scholar]
- Ulmansky, M.; Sela, J.; Langer, M.; Yaari, A. Response of pulpotomy wounds in normal human teeth to successively applied Ledermix and Calxyl. Arch. Oral Biol. 1971, 16, 1393–1398. [Google Scholar] [CrossRef]
- Langer, M.; Ulmansky, M.; Sela, J. Behaviour of human dental pulp to Calxyl with or without zinc oxide eugenol. Arch. Oral Biol. 1970, 15, 189–194. [Google Scholar] [CrossRef]
- Bhaskar, S.N.; Cutright, D.E.; van Osdel, V. Tissue response to cortisone containing and cortisone free calcium hydroxide. ASDC J. Dent. Child. 1969, 36, 193–198. [Google Scholar] [PubMed]
- Kakehashi, S.; Stanley, H.R.; Fitzgerald, R. The exposed germ-free pulp: Effects of topical corticosteroid medication and restoration. Oral Surg. Oral Med. Oral Pathol. 1969, 27, 60–67. [Google Scholar] [CrossRef]
- Pisanti, S.; Sciaky, I. Origin of Calcium in the Repair Wall after Pulp Exposure in the Dog. J. Dent. Res. 1964, 43, 641–644. [Google Scholar] [CrossRef] [PubMed]
- Sciaky, I.; Pisanti, S. Localization of calcium placed over amputated pulps in dogs’ teeth. J. Dent. Res. 1960, 39, 1128–1132. [Google Scholar] [CrossRef] [PubMed]
- Kalnins, V.; Frisbie, H.E. The effect of dentine fragments on the healing of the exposed pulp. Arch. Oral Biol. 1960, 2, 96–103. [Google Scholar] [CrossRef]
- Berman, D.S.; Massler, M. Experimental pulpotomies in rat molars. J. Dent. Res. 1958, 37, 229–242. [Google Scholar] [CrossRef] [PubMed]
- Nyborg, H. Healing processes in the pulp on capping; a morphologic study; experiments on surgical lesions of the pulp in dog and man. Acta Odontol. Scand. 1955, 13, 1–130. [Google Scholar] [PubMed]
- Glass, R.L.; Zander, H.A. Pulp healing. J. Dent. Res. 1949, 28, 97–107. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tziafas, D.; Kodonas, K. Dentinogenic Specificity in the Preclinical Evaluation of Vital Pulp Treatment Strategies: A Critical Review. Dent. J. 2015, 3, 133-156. https://0-doi-org.brum.beds.ac.uk/10.3390/dj3040133
Tziafas D, Kodonas K. Dentinogenic Specificity in the Preclinical Evaluation of Vital Pulp Treatment Strategies: A Critical Review. Dentistry Journal. 2015; 3(4):133-156. https://0-doi-org.brum.beds.ac.uk/10.3390/dj3040133
Chicago/Turabian StyleTziafas, Dimitrios, and Konstantinos Kodonas. 2015. "Dentinogenic Specificity in the Preclinical Evaluation of Vital Pulp Treatment Strategies: A Critical Review" Dentistry Journal 3, no. 4: 133-156. https://0-doi-org.brum.beds.ac.uk/10.3390/dj3040133