Oral Hygiene in a Sample of Children/Adolescents Living in Family-Homes from the Province of Milan (Italy): A Pilot Study

 ,
, 
Abstract
:1. Introduction
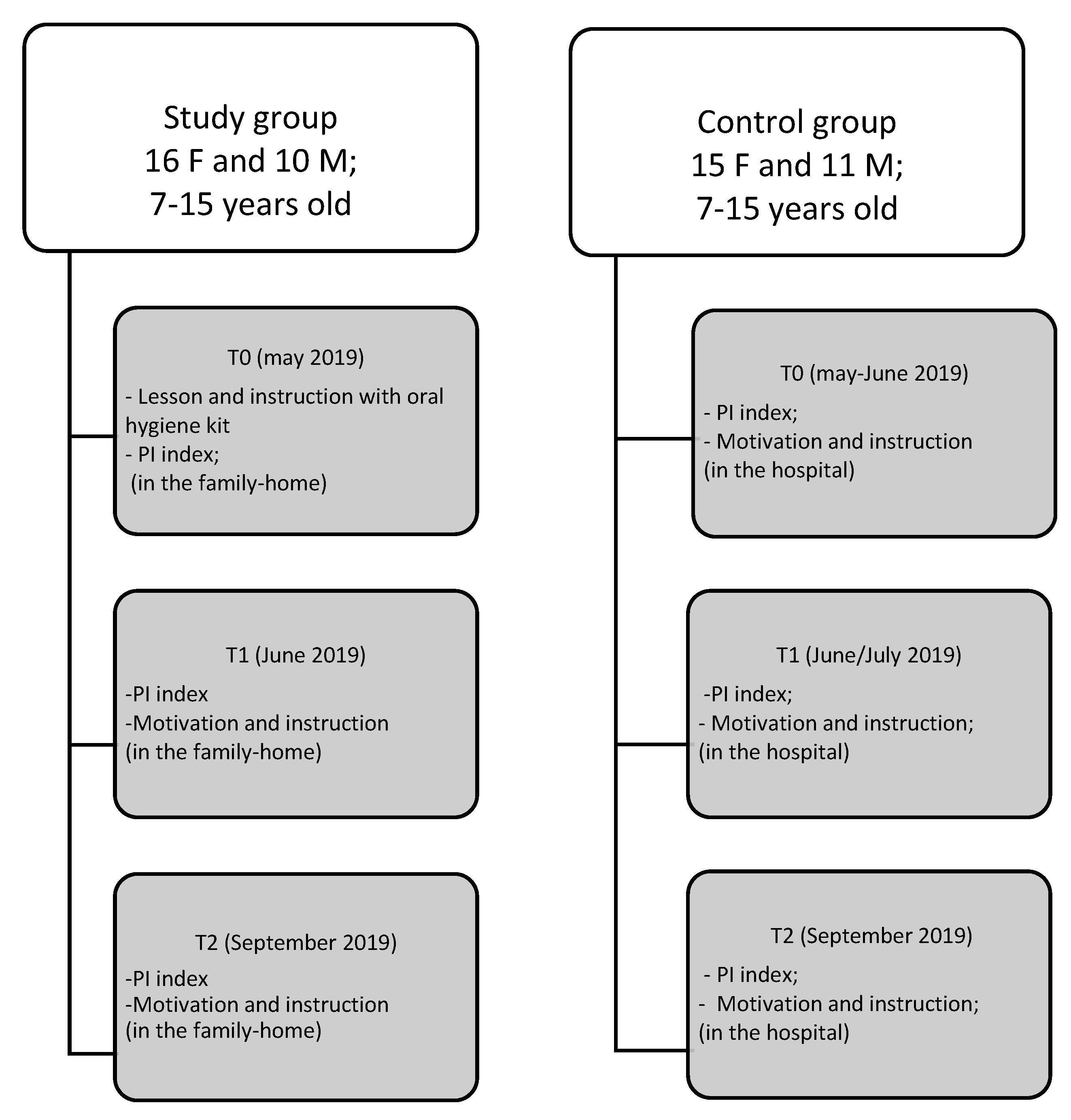
2. Subjects and Methods
Analysis of Data
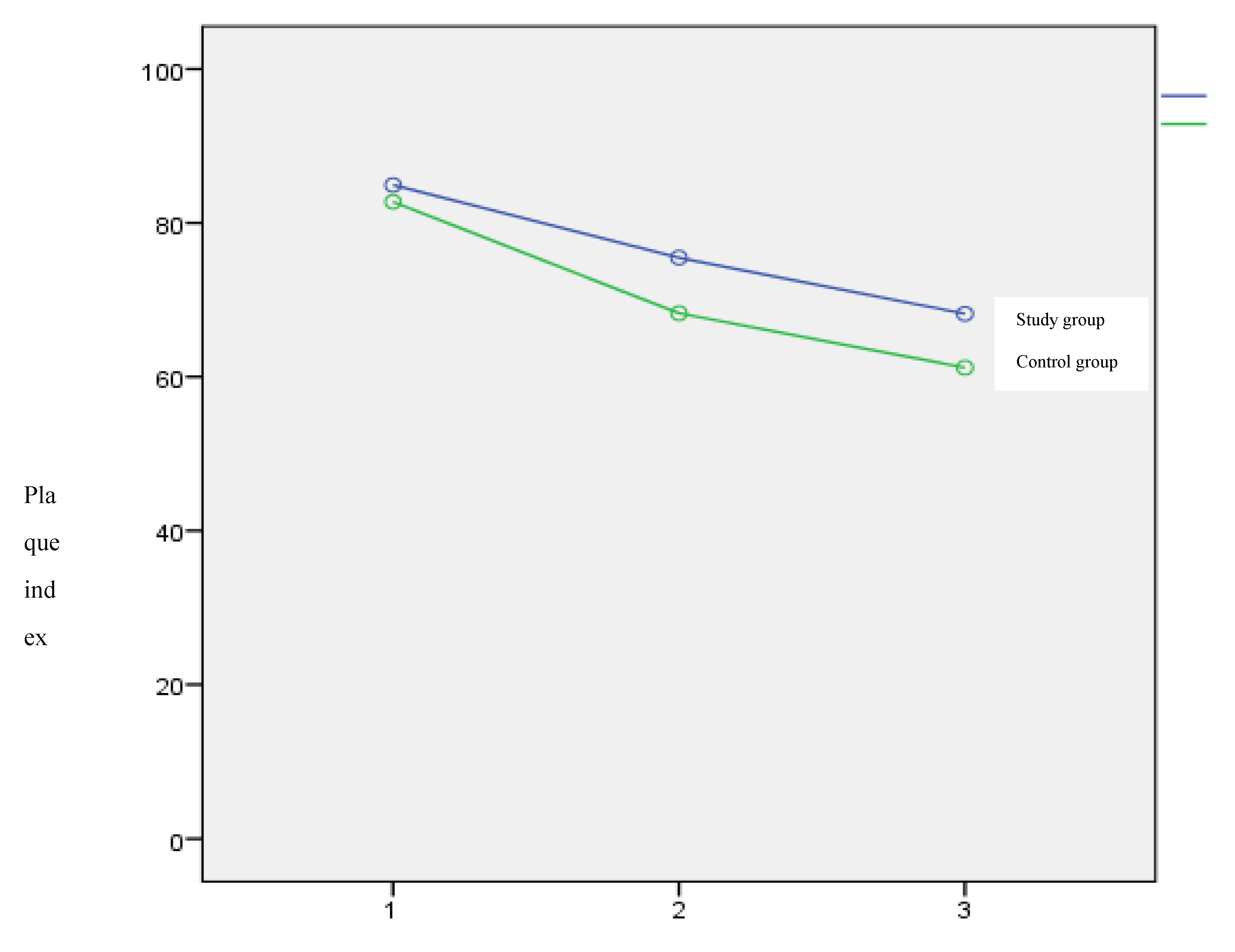
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Constitution of the World Health Organization. Am. J. Public Health Nations Health 1946, 36, 1315–1323. [CrossRef] [Green Version]
- Vik, M.H.; Carlquist, E. Measuring subjective well-being for policy purposes: The example of well-being indicators in the WHO “Health 2020” framework. Scand. J. Public Health 2018, 46, 279–286. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Turney, K.; Wildeman, C. Mental and Physical Health of Children in Foster Care. Pediatrics 2016, 138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Silvestrini-Biavati, A.; Migliorati, M.; Demarziani, E.; Tecco, S.; Silvestrini-Biavati, P.; Polimeni, A.; Saccucci, M. Clinical association between teeth malocclusions, wrong posture and ocular convergence disorders: An epidemiological investigation on primary school children. BMC Pediatr. 2013, 13, 12. [Google Scholar] [CrossRef] [PubMed]
- Tecco, S.; Nota, A.; Caruso, S.; Primozic, J.; Marzo, G.; Baldini, A.; Gherlone, E.F. Temporomandibular clinical exploration in Italian adolescents. Cranio J. Craniomandib. Pract. 2017, 37, 77–84. [Google Scholar] [CrossRef] [PubMed]
- Okolo, S.N.; Chukwu, G.A.; Egbuonu, I.; Ezeogu, F.A.; Onwuanaku, C.; Adeleke, O.A.; Hassan, A.; Ngoe-Nesoah, A. Oral hygiene and nutritional status of children aged 1–7 years in a rural community. Ghana Med. J. 2006, 40, 22–25. [Google Scholar] [PubMed]
- Darout, I. Knowledge and behavior related to oral health among Jimma University Health Sciences students, Jimma, Ethiopia. Eur. J. Gen. Dent. 2014, 3, 185. [Google Scholar] [CrossRef]
- Doğru, A.G.; Kaya, F.A.; Doğru, M.; Sarıbaş, E.; Uysal, E.Y.T. Association Between Level Of Education And Oral Health Status in 12–79 Year Olds. IAMR 2012, 3, 1–6. [Google Scholar]
- Kahabuka, F.; Mbawalla, H. Oral health knowledge and practices among Dar es Salaam institutionalized former street children aged 7–16 years. Int. J. Dent. Hyg. 2006, 4, 174–178. [Google Scholar] [CrossRef]
- Nota, A.; Caruso, S.; Cantile, T.; Gatto, R.; Ingenito, A.; Tecco, S.; Ferrazzano, G.F. Socioeconomic Factors and Oral Health-Related Behaviours Associated with Dental Caries in Preschool Children from Central Italy (Province of Ascoli Piceno). BioMed Res. Int. 2019, 2019, 7981687. [Google Scholar] [CrossRef] [Green Version]
- Tecco, S.; Sciara, S.; Pantaleo, G.; Nota, A.; Visone, A.; Germani, S.; Polizzi, E.; Gherlone, E.F. The association between minor recurrent aphthous stomatitis (RAS), children’s poor oral condition, and underlying negative psychosocial habits and attitudes towards oral hygiene. BMC Pediatr. 2018, 18, 136. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ojahanon, P.; Akionbare, O.; Umoh, A. The oral hygiene status of institution dwelling orphans in Benin City, Nigeria. Niger. J. Clin. Pract. 2013, 16, 41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al-Maweri, S.; Al-Soneidar, W.; Halboub, E. Oral lesions and dental status among institutionalized orphans in Yemen: A matched case-control study. Contemp. Clin. Dent. 2014, 5, 81. [Google Scholar] [CrossRef] [PubMed]
- Watson, M.R.; Manski, R.J.; Macek, M.D. The impact of income on children’s and adolescents’ preventive dental visits. J. Am. Dent. Assoc. 2001, 132, 1580–1587. [Google Scholar] [CrossRef]
- O’Leary, T.J.; Drake, R.B.; Naylor, J.E. The plaque control record. J. Periodontol. 1972, 43, 38. [Google Scholar] [CrossRef]
- Wainwright, J.; Sheiham, A. An analysis of methods of toothbrushing recommended by dental associations, toothpaste and toothbrush companies and in dental texts. Br. Dent. J. 2014, 217, E5. [Google Scholar] [CrossRef]
- Pattussi, M.P.; Olinto, M.T.A.; Hardy, R.; Sheiham, A. Clinical, social and psychosocial factors associated with self-rated oral health in Brazilian adolescents. Community Dent. Oral Epidemiol. 2007, 35, 377–386. [Google Scholar] [CrossRef]
- Fiorillo, L. Oral Health: The First Step to Well-Being. Medicina 2019, 55, 676. [Google Scholar] [CrossRef] [Green Version]
- Bourgeois, D.; Inquimbert, C.; Ottolenghi, L.; Carrouel, F. Periodontal Pathogens as Risk Factors of Cardiovascular Diseases, Diabetes, Rheumatoid Arthritis, Cancer, and Chronic Obstructive Pulmonary Disease-Is There Cause for Consideration? Microorganisms 2019, 7, 424. [Google Scholar] [CrossRef] [Green Version]
- Fiorillo, L.; Cervino, G.; Laino, L.; D’Amico, C.; Mauceri, R.; Tozum, T.F.; Gaeta, M.; Cicciù, M. Porphyromonas gingivalis, Periodontal and Systemic Implications: A Systematic Review. Dent. J. 2019, 7. [Google Scholar] [CrossRef] [Green Version]
- Marino, A.; Nota, A.; Caruso, S.; Gatto, R.; Malagola, C.; Tecco, S. Obstructive sleep apnea severity and dental arches dimensions in children with late primary dentition: An observational study. Cranio 2019, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Inquimbert, C.; Bourgeois, D.; Bravo, M.; Viennot, S.; Tramini, P.; Llodra, J.C.; Molinari, N.; Dussart, C.; Giraudeau, N.; Carrouel, F. The Oral Bacterial Microbiome of Interdental Surfaces in Adolescents According to Carious Risk. Microorganisms 2019, 7, 319. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schwendicke, F.; Paris, S.; Stolpe, M. Detection and treatment of proximal caries lesions: Milieu-specific cost-effectiveness analysis. J. Dent. 2015, 43, 647–655. [Google Scholar] [CrossRef] [PubMed]
- Mummolo, S.; Tieri, M.; Tecco, S.; Mattei, A.; Albani, F.; Giuca, M.R.; Marzo, G. Clinical evaluation of salivary indices and levels of Streptococcus mutans and Lactobacillus in patients treated with Occlus-o-Guide. Eur. J. Paediatr. Dent. 2014, 15, 367–370. [Google Scholar]
- Mummolo, S.; Nota, A.; Caruso, S.; Quinzi, V.; Marchetti, E.; Marzo, G. Salivary Markers and Microbial Flora in Mouth Breathing Late Adolescents. BioMed Res. Int. 2018, 2018, 8687608. [Google Scholar] [CrossRef]
- Nihtila, A.; West, N.; Lussi, A.; Bouchard, P.; Ottolenghi, L.; Senekola, E.; Llodra, J.C.; Viennot, S.; Bourgeois, D. Oral Health Behavior and Lifestyle Factors among Overweight and Non-Overweight Young Adults in Europe: A Cross-Sectional Questionnaire Study. Healthcare 2016, 4, 21. [Google Scholar] [CrossRef] [Green Version]
- Giuca, M.R.; Pasini, M.; Tecco, S.; Marchetti, E.; Giannotti, L.; Marzo, G. Skeletal maturation in obese patients. Am. J. Orthod. Dentofac. Orthop. 2012, 142, 774–779. [Google Scholar] [CrossRef]
- Fiorillo, L. Chlorhexidine Gel Use in the Oral District: A Systematic Review. Gels 2019, 5, 31. [Google Scholar] [CrossRef] [Green Version]
- Khedekar, M.; Suresh, K.V.; Parkar, M.I.; Malik, N.; Patil, S.; Taur, S.; Pradhan, D. Implementation of Oral Health Education to Orphan Children. J. Coll. Phys. Surg. Pak. 2015, 25, 856–859. [Google Scholar]
- Koyuncuoglu, C.Z.; Kazak, M.; Pamuk, F.; Cifcibasi, E. Oral hygiene habits and oral health status of female adolescents under state protection: A pilot study. J. Istanbul Univ. Fac. Dent. 2017, 51, 1–7. [Google Scholar] [CrossRef]
- Hans, R.; Thomas, S.; Dagli, R.; Bhateja, G.A.; Sharma, A.; Singh, A. Oral health knowledge, attitude and practices of children and adolescents of orphanages in jodhpur city rajasthan, India. J. Clin. Diagn. Res. 2014, 8, ZC22. [Google Scholar] [CrossRef] [PubMed]
- Libonati, A.; Nardi, R.; Gallusi, G.; Angotti, V.; Caruso, S.; Coniglione, F.; Marzo, G.; Mattei, A.; Tecco, S.; Paglia, L. Pain and anxiety associated with Computer-Controlled Local Anaesthesia: systematic review and meta-analysis of cross-over studies. Eur J Paediatr Dent. 2018, 19, 324–332. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Group | Study Group | Control Group |
|---|---|---|
| Total sample | 26 | 26 |
| Female | 16 | 15 |
| Males | 10 | 11 |
| Mean age (+/- SD) | 11.71 ± 2.08 | 10.63 ± 1.86 |
| Time | Study Group | Control Group | p |
|---|---|---|---|
| Mean ± SD | Mean ± SD | ||
| T0 | 85 ± 19 | 83 ± 17 | 0.660 (ns) |
| T1 | 75 ± 20 | 68 ± 22 | 0.213 (ns) |
| T2 | 68 ± 18 | 61 ± 20 | 0.192 (ns) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nota, A.; Bosco, F.; Ehsani, S.; Giugliano, F.; Moreo, G.; Tecco, S. Oral Hygiene in a Sample of Children/Adolescents Living in Family-Homes from the Province of Milan (Italy): A Pilot Study. Dent. J. 2020, 8, 33. https://0-doi-org.brum.beds.ac.uk/10.3390/dj8020033
Nota A, Bosco F, Ehsani S, Giugliano F, Moreo G, Tecco S. Oral Hygiene in a Sample of Children/Adolescents Living in Family-Homes from the Province of Milan (Italy): A Pilot Study. Dentistry Journal. 2020; 8(2):33. https://0-doi-org.brum.beds.ac.uk/10.3390/dj8020033
Chicago/Turabian StyleNota, Alessandro, Floriana Bosco, Shideh Ehsani, Francesca Giugliano, Giulia Moreo, and Simona Tecco. 2020. "Oral Hygiene in a Sample of Children/Adolescents Living in Family-Homes from the Province of Milan (Italy): A Pilot Study" Dentistry Journal 8, no. 2: 33. https://0-doi-org.brum.beds.ac.uk/10.3390/dj8020033