
The Critical Role of Consumers in the Prevention of Foodborne Diseases: An Ethnographic Study of Italian Families

 ,
,  , , , and
, , , and
Abstract
:1. Introduction
1.1. Subject and Aims of the Study
1.2. State of the Art
2. Methods
2.1. Sampling
2.2. Method and Data Collection
2.3. Data Analysis
3. Results and Discussion
3.1. Overview of Practices and Factors That Facilitate Food-Related Risks
3.2. Factors That Facilitate Microbiological Risks
3.2.1. Inappropriate Hand Washing and Improper Handling of Food
After taking the chicken slices with her hands and putting them in a dish with breadcrumbs, the mother throws away the polystyrene package and rinses her hands. After that, she uses a tea towel to dry her hands, and the same tea towel is used several times to clean surfaces. […] During the preparation / breading of the chicken, the children help their mother by touching the ingredients with their hands without washing them. […] The child licks his hands after handling the raw chicken and offers his dad to lick him, too. The dad says, ‘It is not okay!’ The child stands up on the kitchen counter. The father then cleans, with his own hands, the breadcrumbs that came from breading the chicken.(Family 1)
The fish is taken from the fish market packaging by hand. Before starting this operation, I [the observer] did not notice if the mother washed her hands. After adding the breadcrumbs, she quickly rinses her hands without detergent. The fish was rinsed underwater in the sink before being placed in the pan. After this operation, the sink was not disinfected.(Family 2)
‘It’s almost ready. Have you washed your hands?’ ‘Yes, yes’ replies the child. ‘No, you didn’t wash them’ says the dad. ‘But I washed them first!’ says the little girl. ‘Yes, but now you’ve touched things.’ She replies, ‘No, no, [points to the games] I didn’t touch!’ Dad argues with the daughter, tells her that she has to wash her hands. The little girl sitting at the table does not want to wash her hands. ‘Come on, then help me clear the table’, says the mother. […] ‘Did you wash your hands in the end?’ asks mom. But the little girl sits there, and in the end, she doesn’t wash her hands.(Family 12)
3.2.2. Inappropriate Washing of Utensils, Work Surfaces and Food
She takes the eggs, puts them near the sink, rinses them, and puts them in a pot. She touches the faucet and then two drawers to take the saucepan’s lid with her hands. She opens the garbage and throws away the potato skins. She rinses her hands only with water and dries herself.(Family 12)
He takes three courgettes from the fridge (he does not wash them) and starts cutting them with the same knife as the onion and on the same cutting board; both tools have not been rinsed […] Then, he cleans the knife used for cutting the vegetables using the cloth hanging above the sink. Then, he takes a large piece of Parmesan cheese and cuts it into cubes with the same knife.(Family 8)
3.2.3. Improper Use of Tea Towels, Dishcloths, and Sponges
There were three sponges: a steel scouring pad; a thin, soft pink sponge; and a two-layer, yellow-green, abrasive sponge. They say that ‘there is no real reason’ why they have two sponges and that apart from the straw, others are used in an undifferentiated way; ‘it is more because they accumulate there than for a real reason’.(Family 8)
The mother gets up and rinses her fingertips, dries them on the cloth hung on the door under the sink that contains the garbage, looks at her cell phone then sits down […]. Opening the door, the tea towel falls to the ground; she picks it up and puts it back on the door. The child takes the pear; ‘at least I’ll wash it’ she says, then rinses it and dries it in the towel stuck on the door under the sink. She hands it over to the son, who throws it on the floor, making vocalisations. […] He [the father] takes the leftovers in the sink with his hands, puts them in the trash, rinses his fingers, and dries them with a towel.(Family 2)
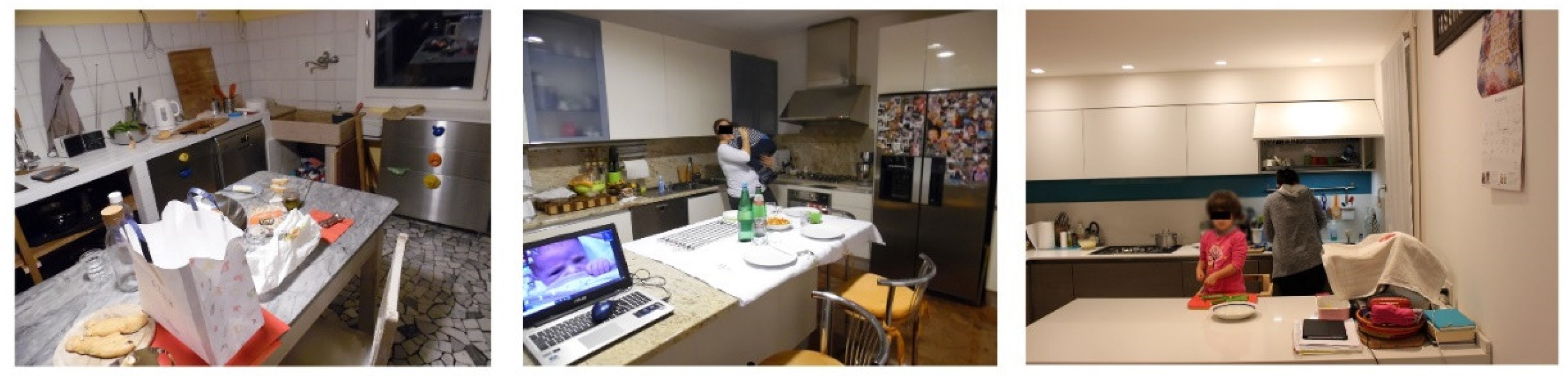
3.2.4. Presence of Objects Unrelated to the Preparation of Food
During preparation, the kitchen shelves are crowded with objects (bottles, dishes used for cooking, utensils), and a plate containing parsley remains outside the fridge […] The father prepares the table, which appears clean with three placemats; on the table, there are a cellphone, a used glass, a battery charger hanging from the wall, and a basket with taralli.(Family 2)
At a certain point, the child arrives with papers and colours to finish her drawing. Mom tells her not to get on the table but to ‘get on the kitchen counter’, where, shortly before, there had been raw chicken. The little girl, standing, draws on the kitchen counter.(Family 1)
3.2.5. Problematic Conservation Practices
She always keeps the eggs out. ‘I consume them within nine days; my mom goes to the chicken coop every day to get the eggs and writes the date on the shell. If I have to do raw stuff, I use them super fresh’.(Family 12)
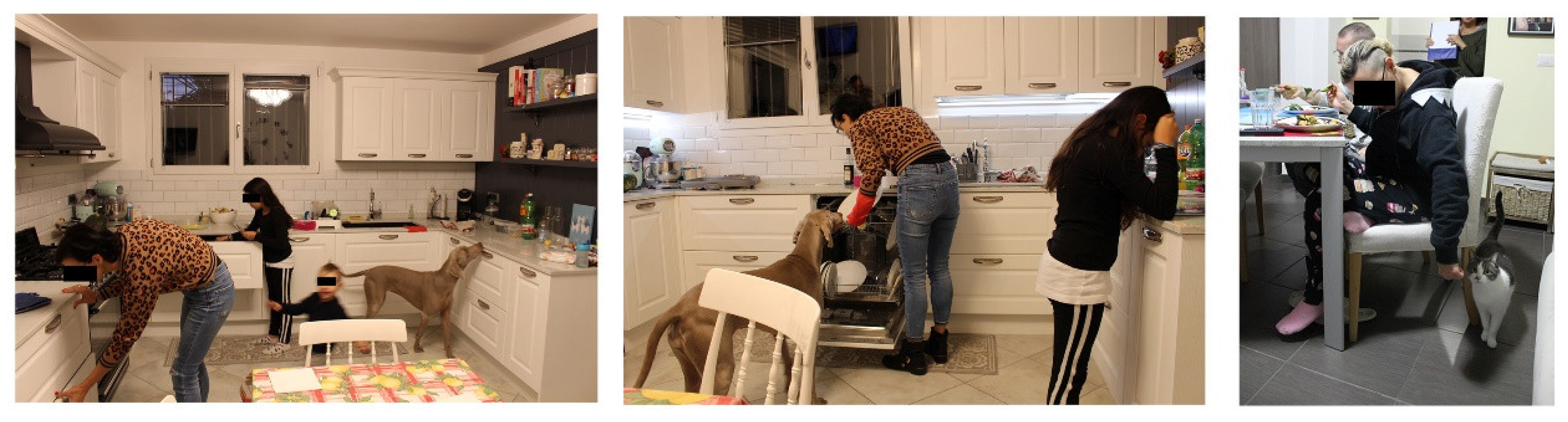
3.2.6. Problematic Management of Pets and Children
Before sitting down at the table, no one washed their hands. All the members are at the table; the baby is in his high-chair, where his mother helps him eat. The dog is free to move around them and is stroked/touched several times by the child and her father. The dog moves around the table, putting its muzzle on the table near the various diners, searching for food. […] At a certain point, the dog has its muzzle on the little girl’s plate. She asks if she can give chicken to the dog. The dog eats the chicken directly from the child’s plate, then she puts it back in the sink.(Family 1)
‘Cats are free to move anywhere but not on the table during meals.’ She, who is pregnant, strokes the cat as she passes by her chair during dinner.(Family 8)
I ask her if the children are always in the room or come to play in the living room. She says that ‘they tend to expand, but then they also stay in place’ […] actually, during the evening, the children seem very calm, polite, and disciplined, and even if they stay for periods of time in the kitchen, they do not create confusion but occupy a specific space at the back of the room on an armchair.(Family 7)
The mother turns to the little girl, who, in the meantime, has arrived in the kitchen. ‘Look at the little fish in the oven; this is a dangerous place’, she says. The grandmother comes to get the children and takes them back to the living room. […] The little girl arrives in the kitchen again and is sent away ‘You have to be with her grandmother; it’s dangerous here’.(Family 11)
[The mother] offers the little girl to help her prepare dinner, asks her if she wants to wash the cabbage; ‘You have to involve them [children]’, she says. ‘Let us get down, so you help me. Are the hands clean?’ ‘Yes!’ replies the little girl. ‘Let me hear it […] No, they are not clean’ mom says, sniffing her little hands […]. They wash their hands with soap […]. The girl is cutting courgettes on a cutting board. The mother rinses the courgettes, cuts them lengthwise, and the little girl slices them.(Family 12)
3.3. Factors That Facilitate Chemical Risks
3.3.1. Food Storage in Unsuitable Containers/Materials
She takes the cheese and three saucepans out of the fridge. We ask what is inside: one contains chicken slices, bought the day before, raw or only seared; in another one is pumpkin, pre-cooked; and the last contains courgettes, picked from a small back garden with her husband and pre-cooked.(Family 9)
3.3.2. Overcooking of Food
I noticed that the cooking is speedy, over high heat, with consequent burning of the pans’ surfaces and the food, such as when sautéing, which I noticed from the fact that the onions used became black, and she put them aside as she ate. The pots seem heavily used, not well preserved, and usually washed in the dishwasher. Above the sink, there is an abrasive sponge used to scrape the bottom of the pots; they tell us that they use it precisely to clean food residues, which happens when food burns.(Family 8)
Then he turns on the pan for sautéing, adds some olive oil, takes some garlic, pops it out, and adds it to the oil. With the addition of garlic, the oil begins to gush and seems to be burning; he realises it and lowers the temperature.(Family 4)
They tell us about their reuse of the oil used to fry the chicken; they usually use it twice […] For frying, bottled (still sealed) olive oil is used; it is poured into a non-stick pan over high heat before dipping the meat … after dinner, the used oil is recovered and placed in a glass jar (without filtering it) to be reused once more.(Family 1)
3.3.3. Contamination by Detergents
She goes back to the kitchen, takes a clean fork, tastes the pasta, says it lacks salt, and adds salt. […] She takes the colander, places it on the sink, takes the pasta pot, and drains the pasta. The sink fills with water. She says the sink gets clogged right away. She brings the drainer over the pot of turnip greens and tosses the pasta into the pan.(Family 4)
3.4. Practices Adopted by Families to Limit Food Risks
The mum goes back to the fish bag, opens it, lifts the trout fillets with her hands, looks at them, and puts them back down.(Family 2)
She goes to open the chicken, which is wrapped in paper towels. She lifts the slices with her hands, looks at them, and then puts them back down.(Family 3)
The little girl sitting at the table cuts the chicken breast and says, ‘It is raw!’ ‘It cannot be’ her mother replies; ‘But inside, it is red’ the little girl says. ‘Because it is a tendon’ the mother answers. She eats the chicken.(Family 1)
But I prefer oat milk, rice milk, even almond milk, which is sweet; not soy milk because they say it is full of pesticides.(Family 13)
He says that he does not like the vegetables of the supermarket because they are processed […] They tell us that the courgettes are from the garden that the husband takes care of, and the vegetables from the garden are eaten willingly. At the same time, they prefer not to buy vegetables from the supermarket because they are ‘processed’ but do not specify with what.(Family 9)
I get fruit and vegetables at the market near my house on Wednesdays and Saturdays. Virtually zero kilometres, and all grown in the countryside nearby! It is beautiful, also beautiful to look at! It is nice to go there early because they bring what they have, and the vegetables have a taste that you do not always find.(Family 3)
My mom always ate homemade tomato puree. Since I got married, it has been hard to get used to different tastes, and I did not know which packaged ones to buy … I tried to make tomato puree at home because it is tastier and healthier, and the tomatoes are from my mother’s garden, without preservatives or other substances … it is a matter of taste but also of the food’s healthy quality.(Family 7)
4. Conclusions
5. Limitations
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Byrd-Bredbenner, C.; Berning, J.; Martin-Biggers, J.; Quick, V. Food safety in home kitchens: A synthesis of the literature. Int. J. Environ. Res. Public Health 2013, 10, 4060–4085. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- European Food Safety Authority; European Centre for Disease Prevention and Control. The European Union One Health 2019 Zoonoses Report. EFSA J. 2021, 19. [Google Scholar] [CrossRef]
- McLinden, T.; Sargeant, J.M.; Thomas, M.K.; Papadopoulos, A.; Fazil, A. Component costs of foodborne illness: A scoping review. BMC Public Health 2014, 14, 509. [Google Scholar] [CrossRef] [Green Version]
- WHO Regional Office for Europe. The Burden of Foodborne Diseases in the WHO European Region; WHO: Copenhagen, Denmark, 2017; Available online: http://www.euro.who.int/en/health-topics/disease-prevention/food-safety/publications/2017/the-burden-of-foodborne-diseases-in-the-who-european-region-2017 (accessed on 2 February 2022).
- World Health Organization. WHO Estimates of the Global Burden of Foodborne Diseases: Foodborne Disease Burden Epidemiology Reference GROUP 2007–2015; WHO: Geneva, Switzerland, 2015; Available online: https://www.who.int/publications/i/item/9789241565165 (accessed on 2 February 2022).
- Mihalache, A.O.; Møretrø, T.; Borda, D.; Dumitraşcu, L.; Neagu, C.; Nguyen-The, C.; Maître, I.; Didier, P.; Teixeira, P.; Junqueira, L.O.L.; et al. Kitchen layouts and consumers’ food hygiene practices: Ergonomics versus safety. Food Control 2022, 131, 108433. [Google Scholar] [CrossRef]
- Borrusso, P.A.; Quinlan, J.J. Prevalence of pathogens and indicator organisms in home kitchens and correlation with unsafe food handling practices and conditions. J. Food Prot. 2017, 80, 590–597. [Google Scholar] [CrossRef]
- Langiano, E.; Ferrara, M.; Lanni, L.; Viscardi, V.; Abbatecola, A.M.; De Vito, E. Food safety at home: Knowledge and practices of consumers. Z. Gesundh. Wiss. 2012, 20, 47–57. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roccato, A.; Uyttendaele, M.; Membré, J.M. Analysis of domestic refrigerator temperatures and home storage time distributions for shelf-life studies and food safety risk assessment. Food Res. Int. 2017, 96, 171–181. [Google Scholar] [CrossRef] [PubMed]
- Cavazza, N.; Guidetti, M. Scelte Alimentari: Foodies, Vegani, Neofobici e Altre Storie; Il Mulino: Bologna, Italy, 2020. [Google Scholar]
- Pellegrini, G.; Farinello, F. Organic consumers and new lifestyles: An Italian country survey on consumption patterns. Br. Food J. 2009, 111, 948–974. [Google Scholar] [CrossRef]
- Taché, J.; Carpentier, B. Hygiene in the home kitchen: Changes in behaviour and impact of key microbiological hazard control measures. Food Control 2014, 35, 392–400. [Google Scholar] [CrossRef]
- Mascarello, G.; Pinto, A.; Marcolin, S.; Crovato, S.; Ravarotto, L. Ethnic food consumption: Habits and risk perception in Italy. J. Food Saf. 2017, 37, 1–9. [Google Scholar] [CrossRef]
- Cenci-Goga, B.; Amicabile, A.; Karama, M.; El-Ashram, S.; Saraiva, C.; García-Díez, J.; Finotti, S.; Genna, V.; Moretti, G.; Murari, R.; et al. Effect of delayed refrigeration on the microbial carcass contamination of wild boars (Sus scrofa). Animals 2021, 11, 1434. [Google Scholar] [CrossRef] [PubMed]
- Bloomfield, S.F.; Exner, M.; Fara, M.G.; Nath, K.J.; Scott, E.A.; Van der Voorden, C. The Global Burden of Hygiene-Related Diseases in Relation to the Home and Community; International Scientific Forum on Home Hygiene: London, UK, 2009; Available online: https://www.ifh-homehygiene.org/review/global-burden-hygiene-related-diseases-relation-home-and-community?OpenDocument (accessed on 1 February 2022).
- Simmons, D.; Chapman, G.E. The significance of home cooking within families. Br. Food J. 2012, 114, 1184–1195. [Google Scholar] [CrossRef]
- Fonte, M. Food systems, consumption models and risk perception in late modernity. Int. J. Sociol. Agric. Food 2002, 10, 13–21. [Google Scholar] [CrossRef]
- Møretrø, T.; Martens, L.; Teixeira, P.; Ferreira, V.B.; Maia, R.; Maugesten, T.; Langsrud, S. Is visual motivation for cleaning surfaces in the kitchen consistent with a hygienically clean environment? Food Control 2020, 111, 107077. [Google Scholar] [CrossRef]
- Tirado, C.; Schmidt, K. WHO surveillance programme for control of foodborne infections and intoxications: Preliminary results and trends across greater Europe. J. Infect. 2001, 43, 80–84. [Google Scholar] [CrossRef]
- Griffith, C.; Worsfold, D.; Mitchell, R. Food preparation, risk communication and the consumer. Food Control 1998, 9, 225–232. [Google Scholar] [CrossRef]
- Wills, W.J.; Meah, A.; Dickinson, A.M.; Short, F. “I don’t think I ever had food poisoning”. A practice-based approach to understanding foodborne disease that originates in the home. Appetite 2015, 85, 118–125. [Google Scholar] [CrossRef] [Green Version]
- Fischer, A.R.H.; Frewer, L.J. Food-safety practices in the domestic kitchen: Demographic, personality, and experiential determinants. J. Appl. Soc. Psychol. 2008, 38, 2859–2884. [Google Scholar] [CrossRef]
- Røssvoll, E.H.; Ueland, Ø.; Hagtvedt, T.; Jacobsen, E.; Lavik, R.; Langsrud, S. Application of hazard analysis and critical control point methodology and risk-based grading to consumer food safety surveys. J. Food Prot. 2012, 75, 1673–1690. [Google Scholar] [CrossRef]
- Veflen, N.; Røssvoll, E.; Langsrud, S.; Scholderer, J. Situated food safety behavior. Appetite 2020, 153, 104751. [Google Scholar] [CrossRef]
- Fischer, A.R.H.; De Jong, A.E.I.; De Jonge, R.; Frewer, L.J.; Nauta, M.J. Perspective: Improving food safety in the domestic environment: The need for a transdisciplinary approach. Risk Anal. 2005, 25, 503–517. [Google Scholar] [CrossRef] [PubMed]
- Humphrey, T.J.; Martin, K.W.; Slader, J.; Durham, K. Campylobacter spp. in the kitchen: Spread and persistence. J. Appl. Microbiol. 2001, 90, 115S–120S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mattick, K.L.; Bailey, R.A.; Jørgensen, F.; Humphrey, T.J. The prevalence and number of Salmonella in sausages and their destruction by frying, grilling or barbecuing. J. Appl. Microbiol. 2002, 93, 541–547. [Google Scholar] [CrossRef] [PubMed]
- Beck, U. Risk Society: Towards a New Modernity; Sage: London, UK, 1992. [Google Scholar]
- Tonkin, E.; Coveney, J.; Meyer, S.B.; Wilson, A.M.; Webb, T. Managing uncertainty about food risks—Consumer use of food labelling. Appetite 2016, 107, 242–252. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rather, I.A.; Koh, W.Y.; Paek, W.K.; Lim, J. The sources of chemical contaminants in food and their health implications. Front. Pharmacol. 2017, 8, 830. [Google Scholar] [CrossRef] [Green Version]
- Prati, G.; Cicognani, E. Percezione e comunicazione del rischio: Uno sguardo alla letteratura. In Uranio Impoverito. Percezione e Comunicazione Del Rischio; Cicognani, E., Prati, G., Zani, B., Eds.; Heuresis: Bologna, Italy, 2011; pp. 26–66. [Google Scholar]
- Tonkin, E.; Webb, T.; Henderson, J.; Ward, P.R.; Coveney, J.; Meyer, S.B.; McCullum, D.; Wilson, A.M. The health implications of distrust in the food system: Findings from the dimensions of trust in food systems scale (DOTIFS scale). BMC Public Health 2021, 21, 21. [Google Scholar] [CrossRef]
- Hawkes, G.; Rowe, G. A characterisation of the methodology of qualitative research on the nature of perceived risk: Trends and omissions. J. Risk Res. 2008, 11, 617–643. [Google Scholar] [CrossRef]
- Ojima, M.; Toshima, Y.; Koya, E.; Ara, K.; Tokuda, H.; Kawai, S.; Kasuga, F.; Ueda, N. Hygiene measures considering actual distributions of microorganisms in Japanese households. J. Appl. Microbiol. 2002, 93, 800–809. [Google Scholar] [CrossRef]
- Redmond, E.C.; Griffith, C.J. Consumer food handling in the home: A review of food safety studies. J. Food Prot. 2003, 66, 130–161. [Google Scholar] [CrossRef]
- Rusin, P.; Orosz-Coughlin, P.; Gerba, C. Reduction of faecal coliform, coliform and heterotrophic plate count bacteria in the household kitchen and bathroom by disinfection with hypochlorite cleaners. J. Appl. Microbiol. 1998, 85, 819–828. [Google Scholar] [CrossRef] [Green Version]
- Kendall, H.; Brennan, M.; Seal, C.; Ladha, C.; Kuznesof, S. Behind the kitchen door: A novel mixed method approach for exploring the food provisioning practices of the older consumer. Food Qual. Prefer. 2016, 53, 105–116. [Google Scholar] [CrossRef] [Green Version]
- Martens, L. The Politics and Practices of Looking: CCTV Video and Domestic Kitchen Practices. In Advances in Visual Methodology; Pink, S., Ed.; SAGE: New York, NY, USA, 2012; pp. 39–56. [Google Scholar] [CrossRef]
- Meah, A. Still blaming the consumer? Geographies of responsibility in domestic food safety practices. Crit. Public Health 2014, 24, 88–103. [Google Scholar] [CrossRef]
- Meah, A.; Watson, M. Saints and slackers: Challenging discourses about the decline of domestic cooking. Sociol. Res. Online 2011, 16, 527–540. [Google Scholar] [CrossRef]
- Mihalache, O.A.; Dumitraşcu, L.; Nicolau, A.I.; Borda, D. Food safety knowledge, food shopping attitude and safety kitchen practices among Romanian consumers: A structural modelling approach. Food Control 2021, 120, 107545. [Google Scholar] [CrossRef]
- Møretrø, T.; Nguyen-The, C.; Didier, P.; Maître, I.; Izsó, T.; Kasza, G.; Skuland, S.E.; Cardoso, M.J.; Ferreira, V.B.; Teixeira, P.; et al. Consumer practices and prevalence of Campylobacter, Salmonella and norovirus in kitchens from six European countries. Int. J. Food Microbiol. 2021, 347, 109172. [Google Scholar] [CrossRef]
- Rotheram, S.; Cooper, J.; Barr, B.; Whitehead, M. How are inequalities generated in the management and consequences of gastrointestinal infections in the UK? An ethnographic study. Soc. Sci. Med. 2021, 282, 114131. [Google Scholar] [CrossRef]
- Sutton, D. The Mindful Kitchen, The Embodied Cook: Tools, Technology and Knowledge Transmission on a Greek Island; Material Culture Review: Sackville, NB, Canada, 2009; Available online: https://journals.lib.unb.ca/index.php/MCR/article/view/18165 (accessed on 1 February 2022).
- Brennan, M.; McCarthy, M. Food Handling in the Home; Elsevier: Amsterdam, The Netherlands, 2016. [Google Scholar] [CrossRef]
- Halkier, B.; Jensen, I. Methodological challenges in using practice theory in consumption research. Examples from a study on handling nutritional contestations of food consumption. J. Consum. Cult. 2011, 11, 101–123. [Google Scholar] [CrossRef]
- Trappmann, M.; Krumpal, I.; Kirchner, A.; Jann, B. Item sum: A new technique for asking quantitative sensitive questions. J. Surv. Stat. Methodol. 2014, 2, 58–77. [Google Scholar] [CrossRef] [Green Version]
- Simon, H.A. A Behavioral Model of Rational Choice. Q. J. Econ. 1955, 69, 99–118. [Google Scholar] [CrossRef]
- Corbetta, P. Social Research: Theory, Methods and Techniques; SAGE: London, UK, 2003. [Google Scholar]
- Glaser, B.G.; Strauss, A.L. The Discovery of Grounded Theory: Strategies for Qualitative Research; Aldine De Gruyter: New York, NY, USA, 1967. [Google Scholar]
- Hammersley, M.; Atkinson, P. Ethnography: Principles in Practice; Routledge: New York, NY, USA, 1995. [Google Scholar]
- Bateson, G. Verso Un’ecologia Della Mente, 12th ed.; Adelphi: Milano, Italy, 1993. [Google Scholar]
- Geertz, C. The Interpretation of Cultures: Selected Essays; Fontana: London, UK, 1973. [Google Scholar]
- Sclavi, M. Arte Di Ascoltare e Mondi Possibili: Come Si Esce Dalle Cornici Di Cui Siamo Parte; Bruno Mondadori: Milano, Italy, 2003. [Google Scholar]
- Evans, E.W.; Redmond, E.C. Domestic kitchen microbiological contamination and self-reported food hygiene practices of older adult consumers. J. Food Prot. 2019, 82, 1326–1335. [Google Scholar] [CrossRef]
- Cogan, T.A.; Bloomfield, S.F.; Humphrey, T.J. The effectiveness of hygiene procedures for prevention of cross-contamination from chicken carcases in the domestic kitchen. Lett. Appl. Microbiol. 1999, 29, 354–358. [Google Scholar] [CrossRef] [PubMed]
- Clayton, D.A.; Griffith, C.J.; Price, P.; Peters, A.C. Food handlers’ beliefs and self-reported practices. Int. J. Environ. Health Res. 2002, 12, 25–39. [Google Scholar] [CrossRef] [PubMed]
- Mandal, R.; Shi, Y.; Singh, A.; Yada, R.Y.; Pratap Singh, A. Food Safety and Preservation. Biomed Sci. 2020, 467–479. [Google Scholar] [CrossRef]
- Gibson, L.L.; Rose, J.B.; Haas, C.N.; Gerba, C.P.; Rusin, P.A. Quantitative assessment of risk reduction from hand washing with antibacterial soaps. J. Appl. Microbiol. Symp. Suppl. 2002, 92, 136–143. [Google Scholar] [CrossRef]
- World Health Organization; WHO Patient Safety. WHO Guidelines on Hand Hygiene in Health Care; WHO: Geneva, Switzerland, 2009; Available online: https://www.who.int/publications/i/item/9789241597906 (accessed on 2 February 2022).
- Luber, P. Cross-contamination versus undercooking of poultry meat or eggs—Which risks need to be managed first? Int. J. Food Microbiol. 2009, 134, 21–28. [Google Scholar] [CrossRef]
- Kusumaningrum, H.D.; Riboldi, G.; Hazeleger, W.C.; Beumer, R.R. Survival of foodborne pathogens on stainless steel surfaces and cross-contamination to foods. Int. J. Food Microbiol. 2003, 85, 227–236. [Google Scholar] [CrossRef]
- Redmond, E.C.; Griffith, C.J. The importance of hygiene in the domestic kitchen: Implications for preparation and storage of food and infant formula. Perspect. Public Health 2009, 129, 69–76. [Google Scholar] [CrossRef]
- Whiley, H.; Clarke, B.; Ross, K. Knowledge and attitudes towards handling eggs in the home: An unexplored food safety issue. Int. J. Environ. Res. Public Health 2017, 14, 48. [Google Scholar] [CrossRef] [Green Version]
- Lange, M.; Göranzon, H.; Marklinder, I. Self-reported food safety knowledge and behaviour among Home and Consumer Studies students. Food Control 2016, 67, 265–272. [Google Scholar] [CrossRef]
- Cloutier, A.; Peetz, J. Relationships’ best friend links between pet ownership, empathy, and romantic relationship outcomes. Anthrozoos 2016, 29, 395–408. [Google Scholar] [CrossRef]
- Krueger, W.S.; Hilborn, E.D.; Dufour, A.P.; Sams, E.A.; Wade, T.J. Self-Reported Acute Health Effects and Exposure to Companion Animals. Zoonoses Public Health 2016, 63, 311–319. [Google Scholar] [CrossRef] [PubMed]
- Byrd-Bredbenner, C.; Maurer, J.; Wheatley, V.; Cottone, E.; Clancy, M. Food safety hazards lurk in the kitchens of young adults. J. Food Prot. 2007, 70, 991–996. [Google Scholar] [CrossRef] [PubMed]
- Ehlert, K.; Beumer, C. Migration study of bisphenol A into water from polycarbonate baby bottles during microwave heating. Food Addit. Contam. 2008, 25, 904–910. [Google Scholar] [CrossRef] [PubMed]
- Nerín, C.; Aznar, M.; Carrizo, D. Food contamination during food process. Trends Food Sci. Technol. 2016, 48, 63–68. [Google Scholar] [CrossRef]
- Roccato, A.; Uyttendaele, M.; Cibin, V.; Barrucci, F.; Cappa, V.; Zavagnin, P.; Longo, A.; Ricci, A. Survival of Salmonella Typhimurium in poultry-based meat preparations during grilling, frying and baking. Int. J. Food Microbiol. 2015, 197, 1–8. [Google Scholar] [CrossRef]
- Kusumaningrum, H.D.; Paltinaite, R.; Koomen, A.J.; Hazeleger, W.C.; Rombouts, F.M.; Beumer, R.R. Tolerance of Salmonella Enteritidis and Staphylococcus aureus to Surface Cleaning and Household Bleach. J. Food Prot. 2003, 66, 2289–2295. [Google Scholar] [CrossRef]
- Young, I.; Waddell, L. Barriers and facilitators to safe food handling among consumers: A systematic review and thematic synthesis of qualitative research studies. PLoS ONE 2016, 11, e0167695. [Google Scholar] [CrossRef]
- Curtis, V.; Aunger, R.; Rabie, T. Evidence that disgust evolved to protect from risk of disease. Proc. R. Soc. B Biol. Sci. 2004, 271, S131–S133. [Google Scholar] [CrossRef] [Green Version]
- Fernandes, N.L.; Pandeirada, J.N.S.; Soares, S.C.; Nairne, J.S. Adaptive memory: The mnemonic value of contamination. Evol. Hum. Behav. 2017, 38, 451–460. [Google Scholar] [CrossRef]
- Nemeroff, C.; Rozin, P. The Contagion Concept in Adult Thinking in the United States: Transmission of Germs and of Interpersonal Influence. Ethos 1994, 22, 158–186. [Google Scholar] [CrossRef]
- Buchler, S.; Smith, K.; Lawrence, G. Food risks, old and new: Demographic characteristics and perceptions of food additives, regulation and contamination in Australia. J. Sociol. 2010, 46, 353–374. [Google Scholar] [CrossRef]
- Saleh, R.; Bearth, A.; Siegrist, M. “Chemophobia” Today: Consumers’ Knowledge and Perceptions of Chemicals. Risk Anal. 2019, 39, 2668–2682. [Google Scholar] [CrossRef] [PubMed]
- Kher, S.V.; De Jonge, J.; Wentholt, M.T.A.; Deliza, R.; de Andrade, J.C.; Cnossen, H.J.; Luijckx, N.B.L.; Frewer, L.J. Consumer perceptions of risks of chemical and microbiological contaminants associated with food chains: A cross-national study. Int. J. Consum. Stud. 2013, 37, 73–83. [Google Scholar] [CrossRef]
- Beck, U. World at Risk; Polity Press: Malden, MA, USA, 2009. [Google Scholar]
- Bruhn, C.M.; Schutz, H.G. Consumer Food Safety Knowledge and Practices. J. Food Saf. 1999, 19, 73–87. [Google Scholar] [CrossRef]
- Mascarello, G.; Pinto, A.; Parise, N.; Crovato, S.; Ravarotto, L. The perception of food quality. Profiling Italian consumers. Appetite 2015, 89, 175–182. [Google Scholar] [CrossRef]
- Ekici, A. Consumer Trust and Distrust in the Food System: Some Implications for the Debates on Food Biotechnologies. In Advances in Consumer Research; Kahn, B.E., Luce, M.F., Eds.; Association for Consumer Research: Valdosta, GA, 2004; Volume 31, pp. 555–564. Available online: http://hdl.handle.net/11693/48631 (accessed on 2 February 2022).
- Isaacs, E. The value of rapid ethnography. In Advancing Ethnography in Corporate Environments: Challenges and Emerging Opportunities; Jordan, B., Ed.; Routledge: Oxfordshire, UK, 2013; pp. 92–107. [Google Scholar] [CrossRef]
- Moses, N.D.; Pakravan, M.H.; MacCarty, N.A. Development of a practical evaluation for cookstove usability. Energy Sustain. Dev. 2019, 48, 154–163. [Google Scholar] [CrossRef]
- Goffman, E.; Best, J. Interaction Ritual: Essays in Face-to-Face Behavior; Routledge: New York, NY, USA, 1967. [Google Scholar]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Id | Family Components Present on Observation | Presence of Pets |
|---|---|---|
| Family unit: parents and children | ||
| 1 | Mother (32 years), Father (35 years), 2 Children (9 e 2 years) | 1 dog |
| 2 | Mother (44 years), Father (45 years), 2 Children (2 e 2 years) | |
| 3 | Mother (51 years), Father (52 years), 1 Child (14 years) | |
| 4 | Mother (50 years), Father (14 years), Grandpa (80 years) | 1 cat |
| 7 | Mother (43 years), Father (40 anni), 2 Children (7 e 4 years) | |
| 11 | Mother (35 years), 2 Children (3 e 1 anno), Grandma | |
| 12 | Mother (31 years), Father (35 years), 1 Child (3 years) | |
| 13 | Mother (50 years), Father (54 years), 1 Child (13 years) | 1 dog |
| 14 | Mother (40 years), Father (40 years), 2 Children (5 e 3 years) | |
| Family unit: presence of a pregnant woman | ||
| 6 | Mother (41 years), Father (42 years), 1 Child (1 year) | |
| 8 | Mother (32 anni), Father (32 years) | 2 cats, 1 snake |
| Family unit: couple over 60 | ||
| 5 | Wife (59 years), Husband (74 years) | |
| 9 | Wife (71 years), Husband (74 years) | |
| 10 | Wife (76 years), Husband (81 years) | 1 cat |
| Risks and Factors | Number of Families |
|---|---|
| Microbiological risk | |
| Inappropriate hand washing and improper handling of food | 13 |
| Inappropriate washing of utensils, work surfaces, and food | 11 |
| Improper use of tea towels and sponges | 11 |
| Presence of objects unrelated to the preparation of food | 11 |
| Problematic conservation practices | 5 |
| Problematic management of pets and children | 3 |
| Chemical risk | |
| Food storage in unsuitable containers/materials | 7 |
| Overcooking of food | 5 |
| Contamination by detergents | 1 |
| Factors Explored | Families ID |
|---|---|
| Inappropriate hand washing and improper handling of food | 1, 2, 3, 4, 5, 6, 7, 8, 10, 11, 12, 13, 14 |
| Inappropriate washing of utensils, work surfaces, and food | 1, 2, 3, 5, 6, 8, 10, 11, 12, 13, 14 |
| Improper use of tea towels and sponges | 1, 2, 3, 6, 8, 9, 10, 11, 12, 13, 14 |
| Presence of objects unrelated to the preparation of food | 1, 2, 4, 5, 7, 8, 9, 11, 12, 13, 14 |
| Problematic conservation practices | 2, 4, 5, 9, 12 |
| Problematic management of pets and children | 1, 8, 13 |
| Factors Explored | Families ID |
|---|---|
| Food storage in unsuitable containers/materials | 2, 3, 4, 8, 9, 12, 13 |
| Overcooking of food | 1, 4, 8, 10, 13 |
| Contamination by detergents | 4 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Menini, A.; Mascarello, G.; Giaretta, M.; Brombin, A.; Marcolin, S.; Personeni, F.; Pinto, A.; Crovato, S. The Critical Role of Consumers in the Prevention of Foodborne Diseases: An Ethnographic Study of Italian Families. Foods 2022, 11, 1006. https://0-doi-org.brum.beds.ac.uk/10.3390/foods11071006
Menini A, Mascarello G, Giaretta M, Brombin A, Marcolin S, Personeni F, Pinto A, Crovato S. The Critical Role of Consumers in the Prevention of Foodborne Diseases: An Ethnographic Study of Italian Families. Foods. 2022; 11(7):1006. https://0-doi-org.brum.beds.ac.uk/10.3390/foods11071006
Chicago/Turabian StyleMenini, Alessio, Giulia Mascarello, Mosè Giaretta, Alice Brombin, Silvia Marcolin, Fabrizio Personeni, Anna Pinto, and Stefania Crovato. 2022. "The Critical Role of Consumers in the Prevention of Foodborne Diseases: An Ethnographic Study of Italian Families" Foods 11, no. 7: 1006. https://0-doi-org.brum.beds.ac.uk/10.3390/foods11071006