
Urban Neighbourhood Environments, Cardiometabolic Health and Cognitive Function: A National Cross-Sectional Study of Middle-Aged and Older Adults in Australia

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Measures
2.1.1. Environmental Measures (Exposures)
2.1.2. Cognitive Function Measures (Outcomes)
2.1.3. Cardiometabolic Risk Factors (Potential Mediators)
2.1.4. Confounders and Covariates
2.2. Statistical Analyses
3. Results
4. Discussion
4.1. Air Pollution
4.2. Natural Environment
4.3. Built Environment
4.4. Strength and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- United Nations. Global Issues: Ageing. Available online: https://www.un.org/en/global-issues/ageing (accessed on 30 June 2021).
- United Nations, Department of Economic and Social Affairs, Population Division. World Urbanization Prospects: The 2018 Revision, online ed.; United Nations: New York, NY, USA, 2018. [Google Scholar]
- United Nations, Department of Economic and Social Affairs, Population Division. Urban and Rural Population by Age and Sex, 1980–2015; United Nations: New York, NY, USA, 2014; Available online: https://esa.un.org/unpd/popdev/urpas/urpas2014.aspx (accessed on 30 June 2021).
- Prince, M.J.; Wu, F.; Guo, Y.; Gutierrez Robledo, L.M.; O’Donnell, M.; Sullivan, R.; Yusuf, S. The burden of disease in older people and implications for health policy and practice. Lancet 2015, 385, 549–562. [Google Scholar] [CrossRef]
- Alzheimer’s Disease International. Policy Brief for G8 Heads of Government—The Global Impact of Dementia 2013–2050; Alzheimer’s Disease International: London, UK, 2013; Available online: http://www.alz.co.uk/research/G8-policy-brief (accessed on 25 August 2014).
- Livingston, G.; Huntley, J.; Sommerlad, A.; Ames, D.; Ballard, C.; Banerjee, S.; Brayne, C.; Burns, A.; Cohen-Mansfield, J.; Cooper, C.; et al. Dementia prevention, intervention, and care: 2020 report of the Lancet Commission. Lancet 2020, 396, 413–446. [Google Scholar] [CrossRef]
- Li, X.Y.; Zhang, M.; Xu, W.; Li, J.Q.; Cao, X.P.; Yu, J.T.; Tan, L. Midlife modifiable risk factors for dementia: A systematic review and meta-analysis of 34 prospective cohort studies. Curr. Alzheimer Res. 2019, 16, 1254–1268. [Google Scholar] [CrossRef] [PubMed]
- Chandrabose, M.; Rachele, J.N.; Gunn, L.; Kavanagh, A.; Owen, N.; Turrell, G.; Giles-Corti, B.; Sugiyama, T. Built environment and cardio-metabolic health: Systematic review and meta-analysis of longitudinal studies. Obes. Rev. 2019, 20, 41–54. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cerin, E.; Nathan, A.; van Cauwenberg, J.; Barnett, D.W.; Barnett, A.; Council on Environment and Physical Activity (CEPA)—Older Adults working group. The neighbourhood physical environment and active travel in older adults: A systematic review and meta-analysis. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barnett, A.; Cerin, E.; Ching, C.S.; Johnston, J.M.; Lee, R.S. Neighbourhood environment, sitting time and motorised transport in older adults: A cross-sectional study in Hong Kong. BMJ Open 2015, 5, e007557. [Google Scholar] [CrossRef] [Green Version]
- Gaio, V.; Roquette, R.; Dias, C.M.; Nunes, B. Ambient air pollution and lipid profile: Systematic review and meta-analysis. Environ. Pollut. 2019, 254 Pt B, 113036. [Google Scholar] [CrossRef]
- Voss, S.; Schneider, A.; Huth, C.; Wolf, K.; Markevych, I.; Schwettmann, L.; Rathmann, W.; Peters, A.; Breitner, S. Long-term exposure to air pollution, road traffic noise, residential greenness, and prevalent and incident metabolic syndrome: Results from the population-based KORA F4/FF4 cohort in Augsburg, Germany. Environ. Int. 2021, 147, 106364. [Google Scholar] [CrossRef] [PubMed]
- Dzhambov, A.M.; Dimitrova, D.D. Residential road traffic noise as a risk factor for hypertension in adults: Systematic review and meta-analysis of analytic studies published in the period 2011–2017. Environ. Pollut. 2018, 240, 306–318. [Google Scholar] [CrossRef]
- Van Cauwenberg, J.; Nathan, A.; Barnett, A.; Barnett, D.W.; Cerin, E.; Council on Environment and Physical Activity (CEPA)-Older Adults Working Group. Relationships between neighbourhood physical environmental attributes and older adults’ leisure-time physical activity: A systematic review and meta-analysis. Sports Med. 2018, 48, 1635–1660. [Google Scholar] [CrossRef] [PubMed]
- Cerin, E.; Van Dyck, D.; Zhang, C.J.P.; Van Cauwenberg, J.; Lai, P.C.; Barnett, A. Urban environments and objectively-assessed physical activity and sedentary time in older Belgian and Chinese community dwellers: Potential pathways of influence and the moderating role of physical function. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 73. [Google Scholar] [CrossRef]
- Besser, L.M.; McDonald, N.C.; Song, Y.; Kukull, W.A.; Rodriguez, D.A. Neighborhood environment and cognition in older adults: A systematic review. Am. J. Prev. Med. 2017, 53, 241–251. [Google Scholar] [CrossRef] [Green Version]
- Cerin, E. Building the evidence for an ecological model of cognitive health. Health Place 2019, 60, 102206. [Google Scholar] [CrossRef]
- Power, M.C.; Adar, S.D.; Yanosky, J.D.; Weuve, J. Exposure to air pollution as a potential contributor to cognitive function, cognitive decline, brain imaging, and dementia: A systematic review of epidemiologic research. Neurotoxicology. 2016, 56, 235–253. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cerin, E.; Barnett, A.; Chaix, B.; Nieuwenhuijsen, M.J.; Caeyenberghs, K.; Jalaludin, B.; Sugiyama, T.; Sallis, J.F.; Lautenschlager, N.T.; Ni, M.Y.; et al. International Mind, Activities and Urban Places (iMAP) study: Methods of a cohort study on environmental and lifestyle influences on brain and cognitive health. BMJ Open 2020, 10, e036607. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dunstan, D.W.; Zimmet, P.Z.; Welborn, T.A.; Cameron, A.J.; Shaw, J.; de Courten, M.; Jolley, D.; McCarty, D.J.; Australian Diabetes, Obesity and Lifestyle Study (AusDiab). The Australian Diabetes, Obesity and Lifestyle Study (AusDiab)—Methods and response rates. Diabetes Res. Clin. Pract. 2002, 57, 119–129. [Google Scholar] [CrossRef] [Green Version]
- Tanamas, S.K.; Magliano, D.J.; Lynch, B.M.; Sethi, P.; Willenberg, L.; Polkinghorne, K.R.; Chadban, S.; Dunstan, D.; Shaw, J.E. AusDiab 2012: The Australian Diabetes, Obesity and Lifestyle Study; Baker Heart and Diabetes Institute: Melbourne, Australia, 2013. [Google Scholar]
- Anstey, K.J.; Sargent-Cox, K.; Eramudugolla, R.; Magliano, D.J.; Shaw, J.E. Association of cognitive function with glucose tolerance and trajectories of glucose tolerance over 12 years in the AusDiab study. Alzheimer’s Res. Ther. 2015, 7, 48. [Google Scholar] [CrossRef] [Green Version]
- Cerin, E.; Barnett, A.; Shaw, J.E.; Martino, E.; Knibbs, L.D.; Tham, R.; Wheeler, A.J.; Anstey, K.J. From Urban Neighbourhood Environments to Cognitive Health: The Role of Physical Activity and Sedentary Behaviours. BMC Public Health 2021, 21, 2320. [Google Scholar] [CrossRef] [PubMed]
- Knibbs, L.D.; Coorey, C.P.; Bechle, M.J.; Cowie, C.T.; Dirgawati, M.; Heyworth, J.S.; Marks, G.B.; Marshall, J.D.; Morawska, L.; Pereira, G.; et al. Independent validation of national satellite-based land-use regression models for nitrogen dioxide using passive samplers. Environ. Sci. Technol. 2016, 50, 12331–12338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Knibbs, L.D.; van Donkelaar, A.; Martin, R.V.; Bechle, M.J.; Brauer, M.; Cohen, D.D.; Cowie, C.T.; Dirgawati, M.; Guo, Y.; Hanigan, I.C.; et al. Satellite-based land-use regression for continental-scale long-term ambient PM2.5 exposure assessment in Australia. Environ. Sci. Technol. 2018, 52, 12445–12455. [Google Scholar] [CrossRef] [Green Version]
- Institute of Medicine. Cognitive Aging: Progress in Understanding and Opportunities for Action; The National Academies Press: Washington, DC, USA, 2015. [Google Scholar] [CrossRef]
- Delis, D.C.; Kramer, J.H.; Kaplan, E.; Ober, B.A. California Verbal Learning Test; Psychological Corporation Harcourt Brace Jovanovich: San Antonio, TX, USA, 1987. [Google Scholar]
- Smith, A. Symbol Digit Modalities Test (SDMT) Manual; Western Psychological Services: Los Angeles, CA, USA, 1982. [Google Scholar]
- Van Buuren, S.; Groothuis-Oudshoorn, K. mice: Multivariate Imputation by Chained Equations in R. J. Stat. Softw. 2011, 45, 1–67. [Google Scholar] [CrossRef] [Green Version]
- Wood, S.N. Generalised Additive Models: An Introduction with R, 2nd ed.; Chapman & Hall/CRC: Boca Raton, FL, USA, 2017. [Google Scholar]
- Klein, S.; Allison, D.B.; Heymsfield, S.B.; Kelley, D.E.; Leibel, R.L.; Nonas, C.; Kahn, R. Waist circumference and cardiometabolic risk: A consensus statement from Shaping America’s Health: Association for Weight Management and Obesity Prevention; NAASO, the Obesity Society; the American Society for Nutrition; and the American Diabetes Association. Obesity 2007, 15, 1061–1067. [Google Scholar] [CrossRef] [PubMed]
- Bays, H.E.; Toth, P.P.; Kris-Etherton, P.M.; Abate, N.; Aronne, L.J.; Brown, W.V.; Gonzalez-Campoy, J.M.; Jones, S.R.; Kumar, R.; La Forge, R.; et al. Obesity, adiposity, and dyslipidemia: A consensus statement from the National Lipid Association. J. Clin. Lipidol. 2013, 7, 304–383. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kilian, J.; Kitazawa, M. The emerging risk of exposure to air pollution on cognitive decline and Alzheimer’s disease—Evidence from epidemiological and animal studies. Biomed. J. 2018, 41, 141–162. [Google Scholar] [CrossRef]
- An, R.; Ji, M.; Yan, H.; Guan, C. Impact of ambient air pollution on obesity: A systematic review. Int. J. Obes. 2018, 42, 1112–1126. [Google Scholar] [CrossRef] [PubMed]
- Zhang, N.; Wang, L.; Zhang, M.; Nazroo, J. Air quality and obesity at older ages in China: The role of duration, severity and pollutants. PLoS ONE 2019, 14, e0226279. [Google Scholar] [CrossRef] [Green Version]
- Fall, T.; Hägg, S.; Ploner, A.; Mägi, R.; Fischer, K.; Draisma, H.H.; Sarin, A.P.; Benyamin, B.; Ladenvall, C.; Åkerlund, M.; et al. Age- and sex-specific causal effects of adiposity on cardiovascular risk factors. Diabetes 2015, 64, 1841–1852. [Google Scholar] [CrossRef] [Green Version]
- Kivipelto, M.; Ngandu, T.; Laatikainen, T.; Winblad, B.; Soininen, H.; Tuomilehto, J. Risk score for the prediction of dementia risk in 20 years among middle aged people: A longitudinal, population-based study. Lancet Neurol. 2006, 5, 735–741. [Google Scholar] [CrossRef]
- Luchsinger, J.A.; Palmas, W.; Teresi, J.A.; Silver, S.; Kong, J.; Eimicke, J.P.; Weinstock, R.S.; Shea, S. Improved diabetes control in the elderly delays global cognitive decline. J. Nutr. Health Aging 2011, 15, 445–449. [Google Scholar] [CrossRef] [Green Version]
- Zhang, X.; Jiang, X.; Han, S.; Liu, Q.; Zhou, J. Type 2 diabetes mellitus is associated with the risk of cognitive impairment: A meta-analysis. J. Mol. Neurosci. 2019, 68, 251–260. [Google Scholar] [CrossRef]
- Honda, T.; Pun, V.C.; Manjourides, J.; Suh, H. Associations between long-term exposure to air pollution, glycosylated hemoglobin and diabetes. Int. J. Hyg. Environ. Health 2017, 220, 1124–1132. [Google Scholar] [CrossRef]
- Coogan, P.F.; White, L.F.; Jerrett, M.; Brook, R.D.; Su, J.G.; Seto, E.; Burnett, R.; Palmer, J.R.; Rosenberg, L. Air pollution and incidence of hypertension and diabetes mellitus in black women living in Los Angeles. Circulation 2012, 125, 767–772. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kramer, U.; Herder, C.; Sugiri, D.; Strassburger, K.; Schikowski, T.; Ranft, U.; Rathmann, W. Traffic-related air pollution and incident type 2 diabetes: Results from the SALIA cohort study. Environ. Health Perspect. 2010, 118, 1273–1279. [Google Scholar] [CrossRef] [Green Version]
- Knibbs, L.D.; Hewson, M.G.; Bechle, M.J.; Marshall, J.D.; Barnett, A.G. A national satellite-based land-use regression model for air pollution exposure assessment in Australia. Environ. Res. 2014, 135, 204–211. [Google Scholar] [CrossRef] [Green Version]
- de Keijzer, C.; Gascon, M.; Nieuwenhuijsen, M.J.; Dadvand, P. Long-term green space exposure and cognition across the life course: A systematic review. Curr. Environ. Health Rep. 2016, 3, 468–477. [Google Scholar] [CrossRef] [PubMed]
- de Keijzer, C.; Bauwelinck, M.; Dadvand, P. Long-term exposure to residential greenspace and healthy ageing: A systematic review. Curr. Environ. Health Rep. 2020, 7, 65–88. [Google Scholar] [CrossRef] [PubMed]
- Maas, J.; van Dillen, S.M.E.; Verheij, R.A.; Groenwegen, P.P. Social contacts as a possible mechanism behind the relation between green space and health. Health Place 2009, 15, 586–595. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berman, M.G.; Jonides, J.; Kaplan, S. The cognitive benefits of interacting with nature. Psychol. Sci. 2008, 19, 1207–1212. [Google Scholar] [CrossRef] [PubMed]
- Dadvand, P.; Rivas, I.; Basagaña, X.; Alvarez-Pedrerol, M.; Su, J.; De Castro Pascual, M.; Amato, F.; Jerret, M.; Querol, X.; Sunyer, J.; et al. The association between greenness and traffic-related air pollution at schools. Sci. Total Environ. 2015, 523, 59–63. [Google Scholar] [CrossRef] [PubMed]
- Chang, L.T.C.; Scorgie, Y.; Duc, H.N.; Monk, K.; Fuchs, D.; Trieu, T. Major source contributions to ambient PM2.5 and exposures within the New South Wales greater metropolitan region. Atmosphere 2019, 10, 138. [Google Scholar] [CrossRef] [Green Version]
- Hyde, J.C.; Yedinak, K.M.; Talhelm, A.F.; Smith, A.M.S.; Bowman, D.M.J.S.; Johnston, F.H.; Lahm, P.; Fitch, M.; Tinkham, W.T. Air quality policy and fire management response addressing smoke from wildland fires in the United States and Australia. Int. J. Wildland Fire 2017, 26, 347–363. [Google Scholar] [CrossRef] [Green Version]
- Banks, J.L.; McConnell, R. National Emissions from Lawn and Garden Equipment. Available online: https://www.epa.gov/sites/production/files/2015-09/documents/banks.pdf (accessed on 10 June 2021).
- Gascon, M.; Zijlema, W.; Vert, C.; White, M.P.; Nieuwenhuijsen, M.J. Outdoor blue spaces, human health and well-being: A systematic review of quantitative studies. Int. J. Hyg. Environ. Health 2017, 220, 1207–1221. [Google Scholar] [CrossRef] [PubMed]
- Warburton, D.E.R.; Bredin, S.S.D. Health benefits of physical activity: A systematic review of current systematic reviews. Curr. Opin. Cardiol. 2017, 32, 541–556. [Google Scholar] [CrossRef] [PubMed]
- Pasanen, T.P.; White, M.P.; Wheeler, B.W.; Garrett, J.K.; Elliott, L.R. Neighbourhood blue space, health and wellbeing: The mediating role of different types of physical activity. Environ. Int. 2019, 131, 105016. [Google Scholar] [CrossRef] [PubMed]
- Snyder, A.; Valdebran, M.; Terrero, D.; Amber, K.T.; Kelly, K.M. Solar ultraviolet exposure in individuals who perform outdoor sport activities. Sports Med.-Open 2020, 6, 42. [Google Scholar] [CrossRef]
- Hajhashemy, Z.; Shahdadian, F.; Ziaei, R.; Saneei, P. Serum vitamin D levels in relation to abdominal obesity: A systematic review and dose-response meta-analysis of epidemiologic studies. Obes. Rev. 2021, 22, e12124. [Google Scholar] [CrossRef]
- Mirhosseini, N.; Vatanparast, H.; Mazidi, M.; Kimball, S.M. The effect of improved serum 25-hydroxyvitamin D status on glycemic control in diabetic patients: A meta-analysis. J. Clin. Endocrinol. Metab. 2017, 102, 3097–3110. [Google Scholar] [CrossRef] [Green Version]
- Cerin, E.; Barnett, A.; Zhang, C.J.P.; Lai, P.C.; Sit, C.H.P.; Lee, R.S.Y. How urban densification shapes walking behaviours in older community dwellers: A cross-sectional analysis of potential pathways of influence. Int. J. Health Geogr. 2020, 19, 14. [Google Scholar] [CrossRef]
- Cerin, E.; Rainey-Smith, S.R.; Ames, D.; Lautenschlager, N.T.; Macaulay, S.L.; Fowler, C.; Robertson, J.S.; Rowe, C.C.; Maruff, P.; Martins, R.N.; et al. Associations of neighborhood environment with brain imaging outcomes in the Australian Imaging, Biomarkers and Lifestyle cohort. Alzheimer’s Dement. 2017, 13, 388–398. [Google Scholar] [CrossRef]
- Riiser, A.; Solbraa, A.; Jenum, A.K.; Birkeland, K.I.; Andersen, L.B. Cycling and walking for transport and their associations with diabetes and risk factors for cardiovascular disease. J. Trans. Health 2018, 11, 193–201. [Google Scholar] [CrossRef]
- Zhang, C.J.P.; Barnett, A.; Sit, C.H.P.; Lai, P.C.; Johnston, J.M.; Lee, R.S.Y.; Cerin, E. To what extent does physical activity explain the associations between neighborhood environment and depressive symptoms in older adults living in an Asian metropolis? Ment. Health Phys. Act. 2019, 16, 96–104. [Google Scholar] [CrossRef]
- Malambo, P.; Kengne, A.P.; De Villiers, A.; Lambert, E.V.; Puoane, T. Built environment, selected risk factors and major cardiovascular disease outcomes: A systematic review. PLoS ONE 2016, 11, e0166846. [Google Scholar] [CrossRef] [PubMed]
- Zhang, K.; Jiang, F.; Luo, H.; Liu, F. Occupational noise exposure and the prevalence of dyslipidemia in a cross-sectional study. BMC Public Health 2021, 21, 1258. [Google Scholar] [CrossRef] [PubMed]
- King, G.; Roland-Mieszkowski, M.; Jason, T.; Rainham, D.G. Noise levels associated with urban land use. J. Urban Health 2012, 89, 1017–1030. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ellis, K.A.; Szoeke, C.; Bush, A.I.; Darby, D.; Graham, P.L.; Lautenschlager, N.T.; Macaulay, S.L.; Martins, R.N.; Maruff, P.; Masters, C.L.; et al. Rates of diagnostic transition and cognitive change at 18-month follow-up among 1112 participants in the Australian Imaging, Biomarkers and Lifestyle Flagship Study of Ageing (AIBL). Int. Psychogeriatr. 2014, 26, 543–554. [Google Scholar] [CrossRef] [PubMed] [Green Version]
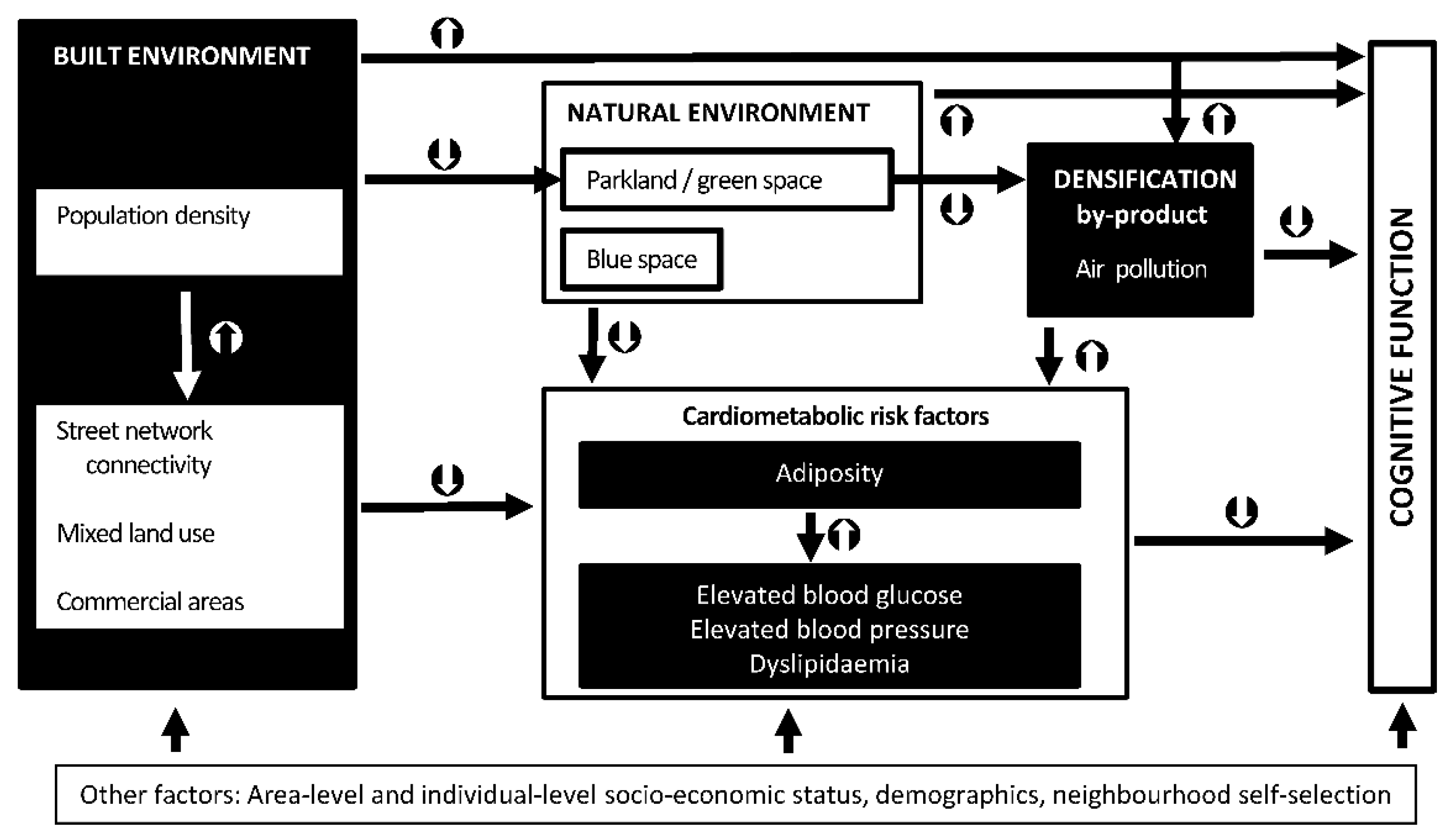
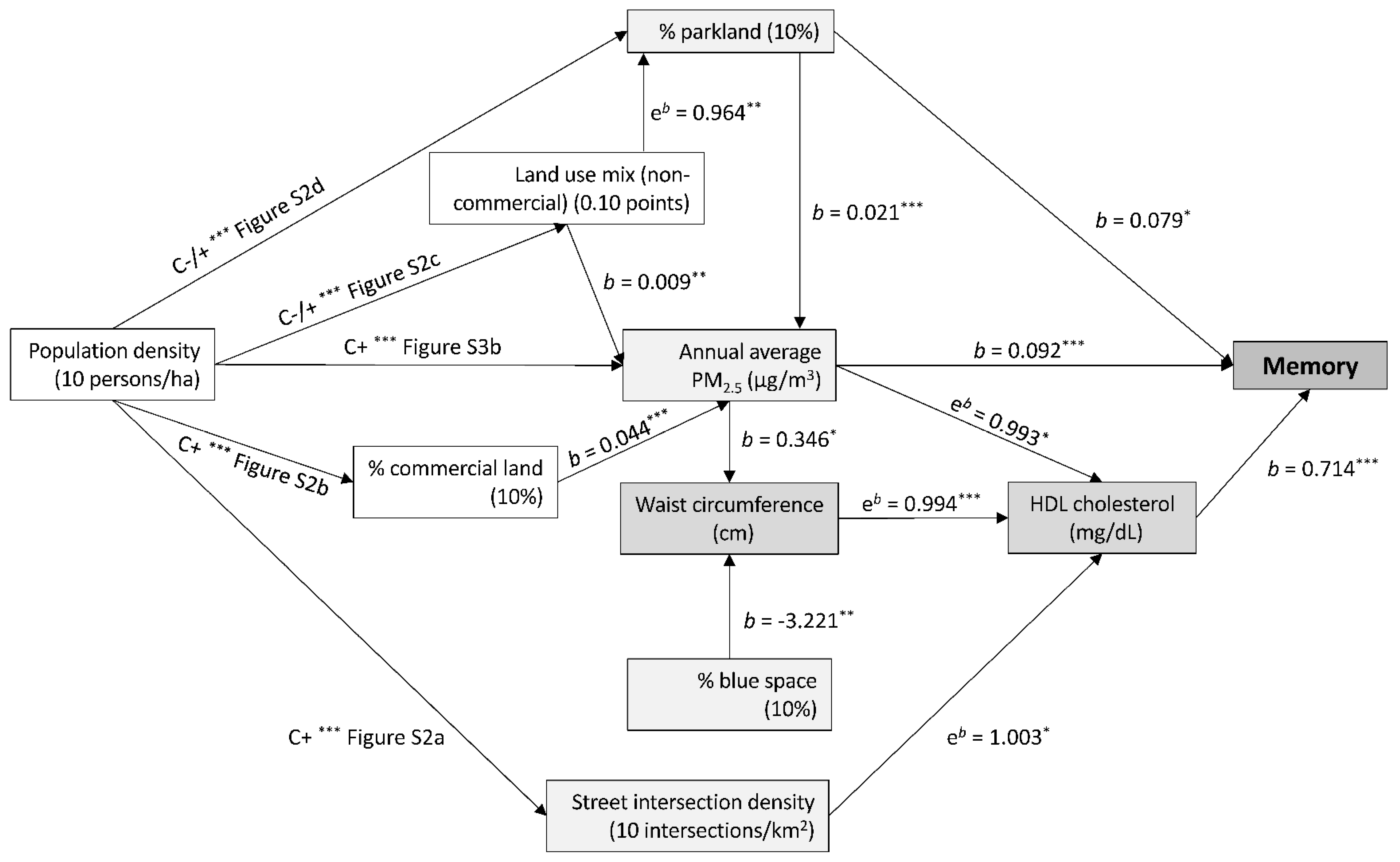
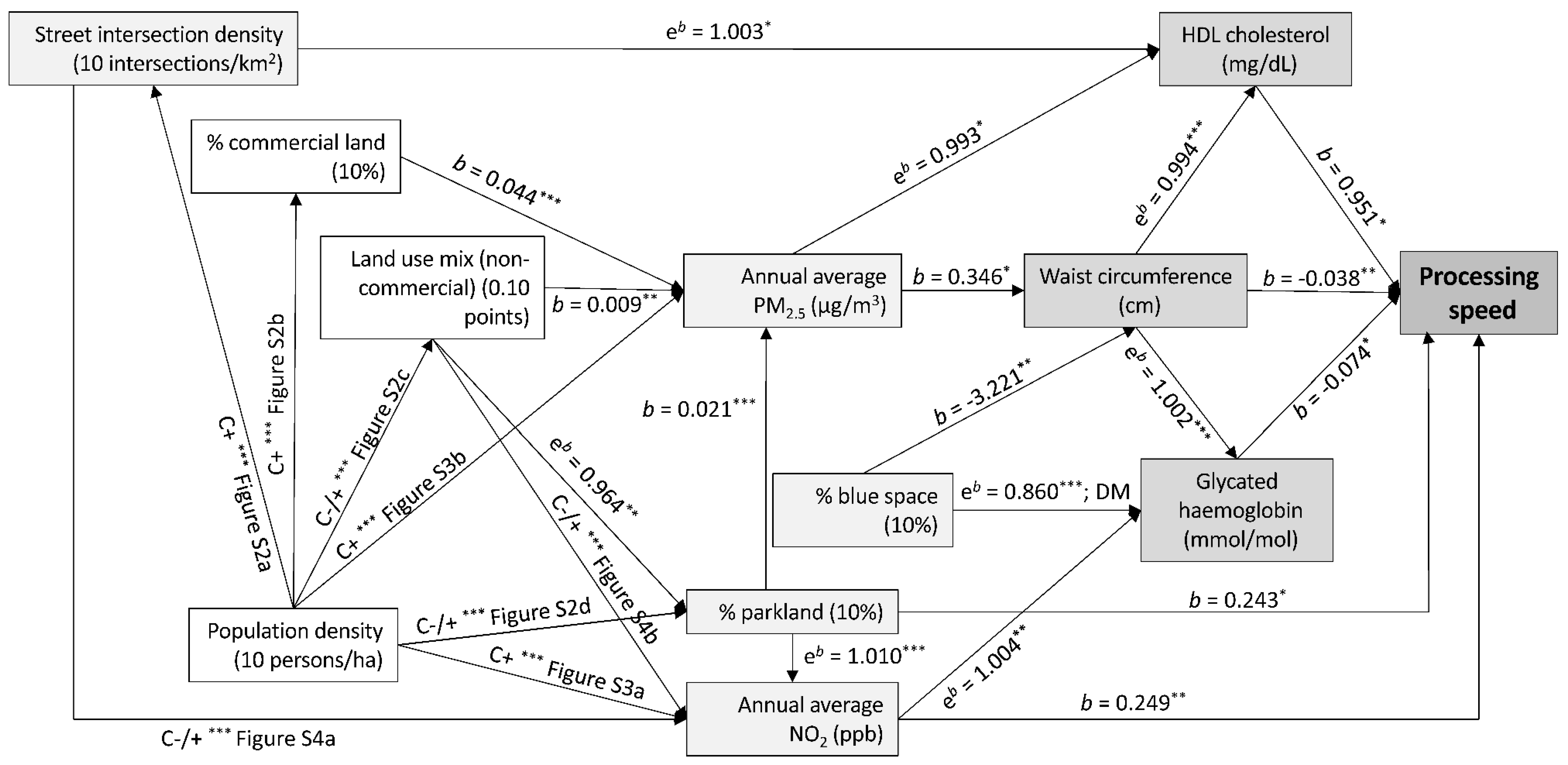
 indicate positive associations;
indicate positive associations;  indicate negative associations.
indicate positive associations; indicate negative associations.
indicate negative associations.
indicate positive associations; indicate negative associations.



{kind=link}
{kind=link}
{kind=link}
| Characteristics | Statistics | Characteristics | Statistics |
|---|---|---|---|
| Socio-demographic characteristics | |||
| Age (years), M ± SD | 61.1 ± 11.4 | Sex, female, % | 55.2 |
| Educational attainment, % | Employment status, % | ||
| Up to secondary | 32.7 | Not employed | 30.4 |
| Trade, associate diploma | 43.6 | Paid employment | 52.2 |
| Bachelor degree, postgraduate | 23.1 | Volunteering | 15.1 |
| Missing data | 0.6 | Missing data | 2.3 |
| Living arrangements, % | Household income (annual), % | ||
| Couple without children | 48.2 | Up to $49,999 | 32.9 |
| Couple with children | 26.8 | $50,000–$99,999 | 26.8 |
| Other | 22.4 | $100,000 and over | 28.9 |
| Missing data | 2.4 | Missing data | 11.5 |
| Area-level IRSAD, M ± SD | 6.4 ± 2.7 | English-speaking background, % | 89.9 |
| Residential self-selection—access to destinations, M ± SD | 3.0 ± 1.4 | Residential self-selection—recreational facilities, M ± SD | 3.1 ± 1.5 |
| Missing data, % | 7.8 | Missing data, % | 7.8 |
| Cardiometabolic risk factors and other health-related variables | |||
| Heart problems/stroke history, % | 8.7 | Tobacco-smoking status, % | |
| Missing data, % | 1.0 | Current smoker | 7.0 |
| LDL cholesterol, mg/dL, M ± SD | 3.0 ± 0.9 | Previous smoker | 35.9 |
| Missing data, % | 1.4 | Non-smoker | 54.5 |
| HDL cholesterol, mg/dL, M ± SD | 1.5 ± 0.4 | Missing data | 2.6 |
| Missing data, % | 0.3 | Waist circumference (cm), M ± SD | 94.6 ± 14.2 |
| Triglycerides, mg/dL, M ± SD | 1.3 ± 0.9 | Missing data, % | 0.2 |
| Missing data, % | 0.3 | ||
| Glycated haemoglobin (HbA1C), mmol/mol, M ± SD | 39.9 ± 6.3 | Mean arterial pressure, mmHg, M ± SD | 92.0 ± 12.3 |
| Missing data, % | 0.5 | Missing data, % | 0.2 |
| Diabetes medication, % | 6.3 | Anti-hypertensive medication, % | 32.0 |
| Missing data, % | 1.8 | Missing data, % | 1.8 |
| Lipid-lowering medication, % | 24.5 | ||
| Missing data, % | 1.8 | ||
| Cognitive function, M ± SD | |||
| Memory, CVLT score | 6.5 ± 2.4 | Processing speed, SDMT score | 49.7 ± 11.6 |
| Missing data, % | 2.3 | Missing data, % | 2.0 |
| Neighbourhood environmental characteristics (1 km-radius street-network buffers), M ± SD | |||
| Population density, persons/ha | 17.4 ± 10.0 | Street intersection density, intersections/km2 | 62.2 ± 32.2 |
| Percentage of commercial land use in residential buffer | 2.5 ± 6.1 | Non-commercial land use mix, entropy score (0 to 1) | 0.14 ± 0.13 |
| Percentage of parkland in residential buffer | 11.6 ± 12.5 | Percentage of blue space (waterbody) in residential buffer | 0.24 ± 1.98 |
| NO2, ppb | 5.5 ± 2.1 | PM2.5, μg/m3 | 6.3 ± 1.7 |
| Environmental Characteristic (Units) | Waist Circumference (cm) | HDL Cholesterol (mg/dL) | LDL Cholesterol (mg/dL) | Triglycerides (mg/dL) | Glycated Haemoglobin (mmol/mol) | Mean Arterial Pressure (mmHg) |
|---|---|---|---|---|---|---|
| b (95% CI) | eb (95% CI) | b (95% CI) | eb (95% CI) | eb (95% CI) | b (95% CI) | |
| Population density | −0.163 | 0.998 | −0.011 | 0.992 | 1.006 | −0.659 |
| (10 persons/ha) | (−0.646, 0.320) | (0.989, 1.008) | (−0.037, 0.014) | (0.972, 1.012) | (1.002, 1.010) | (−1.083, −0.234) |
| Street intersection density | 0.145 | 1.001 | 0.010 | 1.012 | 1.000 | 0.706 |
| (10 intersections/km2) | (−0.035, 0.326) | (0.998, 1.005) | (0.001, 0.019) | (1.004, 1.019) | (0.999, 1.002) | (0.553, 0.859) |
| Percentage of commercial land | 0.270 | 0.986 | −0.010 | 1.026 | 0.998 | 0.761 |
| (10%) | (−0.504, 1.044) | (0.972, 1.001) | (−0.051, 0.031) | (0.993, 1.060) | (0.991, 1.004) | (0.086, 1.435) |
| Non-commercial land use mix | 0.377 | 0.990 | 0.014 | 1.015 | 1.002 | 0.761 |
| (0.10 score) | (−0.004, 0.770) | (0.983, 0.997) | (−0.006, 0.034) | (1.000, 1.031) | (0.999, 1.006) | (0.424, 1.098) |
| Percentage of parkland | −0.314 | 0.996 | −0.021 | 1.003 | 1.001 | −0.303 |
| (10%) | (−0.714, 0.087) | (0.989, 1.004) | (−0.041, −0.001) | (0.987, 1.019) | (0.997, 1.004) | (−0.660, 0.053) |
| Percentage of blue space | −3.237 | 1.041 | −0.076 | 0.972 | 0.989 * | −1.566 |
| (10%) | (−5.461, −1.013) | (1.003, 1.088) | (−0.197, 0.045) | (0.882, 1.070) | (0.971, 1.006) | (−3.477, 0.346) |
| NO2 | 0.066 | 0.999 | −0.002 | 1.000 | 1.003 | −0.381 |
| (ppb) | (−0.242, 0.373) | (0.993, 1.006) | (−0.018, 0.015) | (0.988, 1.013) | (1.000, 1.006) | (−0.647, −0.115) |
| PM2.5 | 0.372 | 0.994 | 0.026 | 1.008 | 1.001 | Curvilinear (see Figure S5) |
| (μg/m3) | (0.064, 0.681) | (0.990, 0.999) | (0.006, 0.047) | (0.996, 1.021) | (0.998, 1.006) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cerin, E.; Barnett, A.; Shaw, J.E.; Martino, E.; Knibbs, L.D.; Tham, R.; Wheeler, A.J.; Anstey, K.J. Urban Neighbourhood Environments, Cardiometabolic Health and Cognitive Function: A National Cross-Sectional Study of Middle-Aged and Older Adults in Australia. Toxics 2022, 10, 23. https://0-doi-org.brum.beds.ac.uk/10.3390/toxics10010023
Cerin E, Barnett A, Shaw JE, Martino E, Knibbs LD, Tham R, Wheeler AJ, Anstey KJ. Urban Neighbourhood Environments, Cardiometabolic Health and Cognitive Function: A National Cross-Sectional Study of Middle-Aged and Older Adults in Australia. Toxics. 2022; 10(1):23. https://0-doi-org.brum.beds.ac.uk/10.3390/toxics10010023
Chicago/Turabian StyleCerin, Ester, Anthony Barnett, Jonathan E. Shaw, Erika Martino, Luke D. Knibbs, Rachel Tham, Amanda J. Wheeler, and Kaarin J. Anstey. 2022. "Urban Neighbourhood Environments, Cardiometabolic Health and Cognitive Function: A National Cross-Sectional Study of Middle-Aged and Older Adults in Australia" Toxics 10, no. 1: 23. https://0-doi-org.brum.beds.ac.uk/10.3390/toxics10010023