
Influence of Electronic Cigarettes on Antioxidant Capacity and Nucleotide Metabolites in Saliva

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients’ Population
2.2. Saliva Collection
2.3. Analysis of Saliva
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Pink, R.; Simek, J.; Vondrakova, J. Saliva as a diagnostic medium. Biomed. Pap. Med. Fac. Univ. Palacky Olomouc Czech Republ. 2009, 153, 103–110. [Google Scholar] [CrossRef] [Green Version]
- Lynge Pedersen, A.M.; Belstrøm, D. The role of natural salivary defences in maintaining a healthy oral microbiota. J. Dent. 2019, 80, 3–12. [Google Scholar] [CrossRef] [PubMed]
- Dyba, J.; Lenkowski, M.; Surdacka, A. Evaluating the diagnostic potential of saliva in respect of periodontal disease as well as changes occurring within the endothelium. Dent. Forum 2017, 1, 21–25. [Google Scholar]
- Zappacosta, B.; Persichilli, S.; De Sole, P.; Mordente, A.; Giardia, B. Effect of smoking one cigarette on antioxidant metabolites in the saliva of healthy smoker. Arch. Oral Biol. 1999, 44, 485–488. [Google Scholar] [CrossRef]
- Battino, M.; Ferreiro, M.S.; Gallardo, I.; Newman, H.N.; Bullon, P. The antioxidant capacity of saliva. J. Clin. Periodontal. 2002, 29, 189–194. [Google Scholar] [CrossRef] [Green Version]
- Nagler, R.M.; Klein, I.; Zarzhersky, N.; Drigues, N.; Reznick, A.Z. Characterization of the differentiated antioxidant profile of human saliva. Free Radic. Biol. Med. 2002, 32, 268–277. [Google Scholar] [CrossRef]
- Mandel, I.D. The role of saliva in maintaining oral homeostasis. J. Am. Dent. Assoc. 1989, 119, 298–304. [Google Scholar] [CrossRef] [PubMed]
- Roblegg, E.; Coughran, A.; Sirjani, D. Saliva: An all-rounder of our body. Eur. J. Pharm. Biopharm. 2019, 142, 133–141. [Google Scholar] [CrossRef]
- Konopka, T.; Gmyrek-Marciniak, A.; Kozłowski, Z.; Kaczmarek, U.; Wnukiewicz, J. Potencjał antyoksydacyjny śliny u pacjentów z zapaleniem przyzębia i rakiem płaskonabłonkowym dna jamy ustnej. Dent. Med. Probl. 2006, 43, 354–362. [Google Scholar]
- Venditti, P.; Di Stefano, L.; Di Meo, S. Mitochondrial metabolism of reactive oxygen species. Mitochondrion 2013, 13, 71–82. [Google Scholar] [CrossRef] [PubMed]
- Betteridge, D.J. What is oxidative stress? Metabolism 2000, 49, 3–8. [Google Scholar] [CrossRef]
- Valko, M.; Leibfritz, D.; Moncol, J.; Cronin, M.T.D.; Mazur, M.; Teser, J. Free radicals and antioxidants in normal physiological functions and human disease. Int. J. Biochem. Cell Biol. 2006, 39, 44–84. [Google Scholar] [CrossRef]
- Becker, L.B. New concepts in reactive oxygen species and cardiovascular reperfusion physiology. Cardiovasc. Res. 2004, 61, 461–470. [Google Scholar] [CrossRef] [PubMed]
- Valko, M.; Leibfritz, D.; Moncol, J.; Cronin, M.T.D.; Mazur, M. Free radicals, metals and antioxidants in oxidative-stress included cancer. Chem. Biol. Interact. 2006, 160, 1–40. [Google Scholar] [CrossRef] [PubMed]
- Dąbrowska, Z.N.; Bijowska, K.; Dąbrowska, E.; Pietuska, M. Effect of oxidants and antioxidants on oral health. Med. Ogólna Nauki Zdrowiu 2020, 26, 87–93. [Google Scholar] [CrossRef]
- Kimura, S.; Yonemura, T.; Kaya, H. Increased oxidative product formation by peripheral blood polymofronuclear leukocytes in human periodontal disease. J. Periodontal. Res. 1993, 28, 197–203. [Google Scholar] [CrossRef]
- Knaś, M.; Maciejczyk, M.; Waszkiel, D.; Zalewska, A. Oxidative stress and salivary antioxidants. Dent. Med. Probl. 2013, 50, 461–466. [Google Scholar]
- Wang, Y.; Andrukhov, O.; Rausch-Fan, X. Oxidative stress and antioxidant system in periodontotitis. Front. Physiol. 2017, 8, 910. [Google Scholar] [CrossRef] [Green Version]
- Kusiak, A.; Kochańska, B.; Limon, J.; Ochocińska, J. The physico-chemical properties of saliva in Turner’s syndrome. Dent. Forum 2011, 39, 19–23. [Google Scholar]
- Weiner, D.; Levy, Y.; Khankin, E.V.; Reznick, A.Z. Inhibition of salivary amylase activity by cigarette smoke aldehydes. J. Physiol. Pharmacol. 2008, 59, 727–737. [Google Scholar]
- Cichońska, D.; Kusiak, A.; Kochańska, B.; Ochocińska, J.; Świetlik, D. Influence of electronic cigarettes on selected antibacterial properties of saliva. Int. J. Environ. Res. Public Health 2019, 16, 4433. [Google Scholar] [CrossRef] [Green Version]
- Chen, C.; Zhuang, Y.L.; Zhu, S.H. E-Cigarette design preference and smoking cessation: A U.S. population study. Am. J. Prev. Med. 2016, 51, 356–363. [Google Scholar] [CrossRef] [Green Version]
- Bertholon, J.F.; Becquemin, M.H.; Annesi-Maesano, I.; Dautzenberg, B. Electronic cigarettes: A short review. Respiration 2013, 86, 433–438. [Google Scholar] [CrossRef] [PubMed]
- McNeill, A.; Brose, L.S.; Calde, R.R.; Hitchman, S.C.; Hajek, P.; McRobbie, H. E-cigarettes: An evidence update. A report commissioned by Public Health England. Public Health Engl. 2015, 11, 14–15. [Google Scholar]
- Brown, C.J.; Cheng, J.M. Electronic cigarettes: Product characterization and design considerations. Tob. Control 2014, 23, 4–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, M.S.; Hall, M.G.; Parada, H.; Peebles, K.; Brodar, K.E.; Brewer, N.T. Symptoms during adolescents’ first use of cigarettes and e-cigarettes: A pilot study. Int. J. Environ. Res. Public Health 2017, 14, 1260. [Google Scholar] [CrossRef] [Green Version]
- Pisinger, C.; Dossing, M. A systematic review of health effects of electronic cigarettes. Prev. Med. 2014, 69, 248–260. [Google Scholar] [CrossRef] [Green Version]
- Yu, V.; Rahimy, M.; Korrapati, A. Electronic cigarettes induce DNA stand breaks and cell death independently of nicotine in cell lines. Oral Oncol. 2016, 52, 58–65. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Semlali, A.; Chakir, J.; Goulet, J.P.; Chmielewski, W.; Rouabhia, M. Whole cigarette smoke promotes human gingival epithelial cell apoptosis and inhibits cell repair processes. J. Periodontal Res. 2011, 46, 533–541. [Google Scholar] [CrossRef]
- Sundar, I.K.; Javed, F.; Romanos, G.E.; Rahman, I. E-cigarettes and flavorings induce inflammatory and pro-senescence responses in oral epithelial cells and periodontal fibroblasts. Oncotarget 2016, 7, 77196–77204. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Holliday, R.; Kist, R.; Bauld, L. E-cigarette vapour is not inert and exposure can lead to cell damage. Evid. Based Dent. 2016, 17, 2–3. [Google Scholar] [CrossRef] [PubMed]
- Salaspuro, V.; Salaspuro, M. Synergistic effect of alkohol drinking and smoking on in vitro acetaldehyde concentration in saliva. Int. J. Cancer 2004, 111, 480–483. [Google Scholar] [CrossRef] [PubMed]
- Alqahtani, S.; Cooper, B.; Spears, C.A.; Wright, C.; Shannahan, J. Electronic nicotine delivery system-induced alterations in oral health via saliva assessment. Exp. Biol. Med. 2020, 245, 1319–1325. [Google Scholar] [CrossRef] [PubMed]
- Smolenski, R.T.; Lachno, D.R.; Ledingham, S.J.; Yacoub, M.H. Determination of sixteen nucleotides, nucleosides and bases using high-performance liquid chromatography and its application to the study of purine metabolism in hearts for transplantation. J. Chromatogr. 1990, 18, 414–420. [Google Scholar] [CrossRef]
- Smolenski, R.T.; Yacoub, M.H. Liquid chromatographic evaluation of purine production in the donor human heart during transplantation. Biomed. Chromatogr. 1993, 7, 189–195. [Google Scholar] [CrossRef] [PubMed]
- Miller, N.J.; Rice-Evans, C.; Davies, M.J.; Gopinathan, V.; Milner, A. A novel method for measuring antioxidant capacity and its application to monitoring the antioxidant status in premature neonates. Clin. Sci. 1993, 84, 407–412. [Google Scholar] [CrossRef] [Green Version]
- Nagler, R.M.; Reznick, A.Z. Cigarette smoke effects on salivary antioxidants and oral cancer-novel concepts. IMAJ 2004, 6, 691–694. [Google Scholar]
- Nagler, R.; Lischinsky, S.; Diamond, E.; Drigues, N.; Klein, I.; Reznick, A.Z. Effect of cigarette smoke on salivary proteins and enzyme activities. Arch. Biochem. Biophys. 2000, 15, 229–236. [Google Scholar] [CrossRef]
- Kondakova, I.; Lissi, E.A.; Pizarro, M. Total reactive antioxidant potential in human saliva of smokers and non-smokers. Biochem. Mol. Biol. Int. 1999, 47, 911–920. [Google Scholar] [CrossRef]
- Kosmider, L.; Sobczak, A.; Fik, M.; Knysak, J.; Zaciera, M.; Kurek, J.; Goniewicz, M.L. Carbonyl compounds in electronic cigarette vapors: Effects of nicotine solvent and battery output voltage. Nicotine Tob. Res. 2014, 16, 1319–1326. [Google Scholar] [CrossRef]
- Goniewicz, M.L.; Knysak, J.; Gawron, M.; Kosmider, L.; Sobczak, A.; Kurek, J.; Prokopowicz, A.; Jablonska-Czapla, M.; Rosik-Dulewska, C.; Havel, C.; et al. Levels of selected carcinogens and toxicants in vapour from electronic cigarettes. Tob. Control 2014, 23, 133–139. [Google Scholar] [CrossRef] [Green Version]
- Derruau, S.; Robinet, J.; Untereiner, V.; Piot, O.; Sockalingum, G.D.; Lorimier, S. Vibrational spectroscopy saliva profiling as biometric tool for disease diagnostics: A systematic literature. Molecules 2020, 25, 4142. [Google Scholar] [CrossRef]
- Lerner, C.A.; Sundar, I.K.; Yao, H.; Gerloff, J.; Ossip, D.J.; McIntosh, S.; Robinson, R.; Rahman, I. Vapors produced by electronic cigarettes and e-juices with flavorings induce toxicity, oxidative stress, and inflammatory response in lung epithelial cells and in mouse lung. PLoS ONE 2015, 6, e0116732. [Google Scholar] [CrossRef]
- Gawron-Skarbek, A.; Prymont-Przymińska, A.; Sobczak, A.; Guligowska, A.; Kostka, T.; Nowak, D.; Szatko, F. A comparison of native and non-urate total antioxidant capacity of fasting plasma and saliva among middle-aged and older subjects. Redox Rep. 2018, 23, 7–62. [Google Scholar] [CrossRef] [Green Version]
- Almadori, G.; Bussu, F.; Galli, J.; Limongelli, A.; Persichilli, S.; Zappacosta, B.; Minucci, A.; Paludetti, G.; Giardina, B. Salivary glutathione and uric acid levels in patients with head and neck squamous cell carcinoma. Head Neck 2007, 29, 648–654. [Google Scholar] [CrossRef] [PubMed]
- Moore, S.; Calder, K.A.C.; Miller, N.J.; Rice-Evans, C.A. Antioxidant activity of saliva and periodontal disease. Free Radic. Res. 1994, 21, 417–425. [Google Scholar] [CrossRef] [PubMed]
- Greabu, M.; Battino, M.; Totan, A.; Mohora, M.; Mitrea, N.; Totan, C.; Spinu, T.; Didilescu, A. Effect of gas phase and particulate phase of cigarette smoke on salivary antioxidants. What can be the role of vitamin C and pyridoxine? Pharmacol. Rep. 2007, 59, 613–618. [Google Scholar] [PubMed]
- Ahmadi-Motamayel, F.; Falsafi, P.; Abolsamadi, H.; Goodarzi, M.T.; Poorolajal, J. Evaluation of salivary antioxidants and oxidative stress markers in male smokers. Comb. Chem. High Throughput Screen 2019, 22, 496–501. [Google Scholar] [CrossRef]
- Abdolsamadi, H.R.; Goodarzi, M.T.; Mortazavi, H.; Robati, M.; Ahmadi-Motemaye, F. Comparison of salivary antioxidants in healthy smoking and non-smoking men. Chang. Gung Med. J. 2011, 34, 607–611. [Google Scholar]
- Xiang, L.W.; Li, J.; Lin, J.M.; Li, H.F. Determination of gouty arthritis’ biomarkers in human urine using reversed-phase high-performance liquid chromatography. J. Pharm. Anal. 2014, 4, 153–158. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prior, R.L.; Cao, G. In vivo total antioxidant capacity: Comparison of different analytical methods. Free Radic. Biol. Med. 1999, 27, 1173–1181. [Google Scholar] [CrossRef]
- Hamo Mahmood, I.; Abdullah, K.S.; Othman, S.H. The total antioxidant status in cigarette smoking individuals. MJBU 2007, 25, 45–50. [Google Scholar] [CrossRef] [Green Version]
- Bakhtiari, S.; Azimi, S.; Mehdipour, M.; Amini, S.; Elmi, Z.; Namazi, Z. Effect of cigarette smoke on salivary total antioxidant capacity. J. Dent. Res. Dent. Clin. Dent. Prospects 2015, 9, 281–284. [Google Scholar] [CrossRef]
- Nagler, R.M. Altered salivary profile in heavy smokers and its possible connection to oral cancer. Int. J. Biol. Mark. 2007, 22, 274–280. [Google Scholar] [CrossRef]
- Van den Berg, R.; Haenen, G.R.M.M.; van den Berg, H.; Bast, A. Applicability of an improved TEAC assay for evaluation of antioxidant capacity measurements of mixtures. Food Chem. 1999, 66, 511–517. [Google Scholar] [CrossRef]
- Rao, R.K.; Thomas, D.W.; Pepperl, S.; Porreca, F. Salivary epidermal growth factor plays a role in protection of ileal mucosal integrity. Dig. Dis. Sci. 1997, 42, 2175–2181. [Google Scholar] [CrossRef]
- Valko, M.; Izakovic, M.; Mazur, M.; Rhodes, C.J.; Telser, J. Role of oxygen radicals in DNA damage and cancer incidence. Mol. Cell Biochem. 2004, 266, 37–56. [Google Scholar] [CrossRef] [PubMed]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
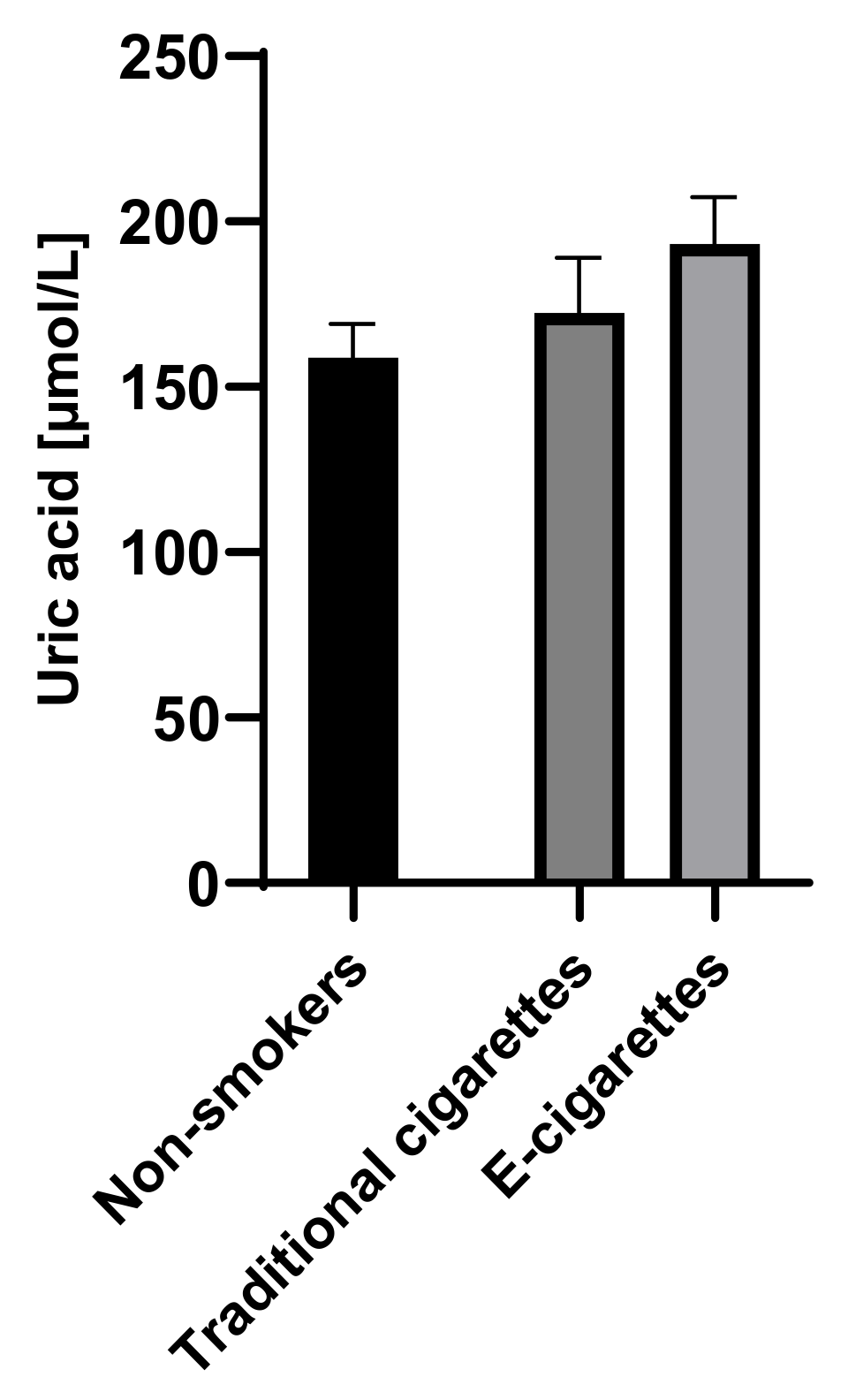
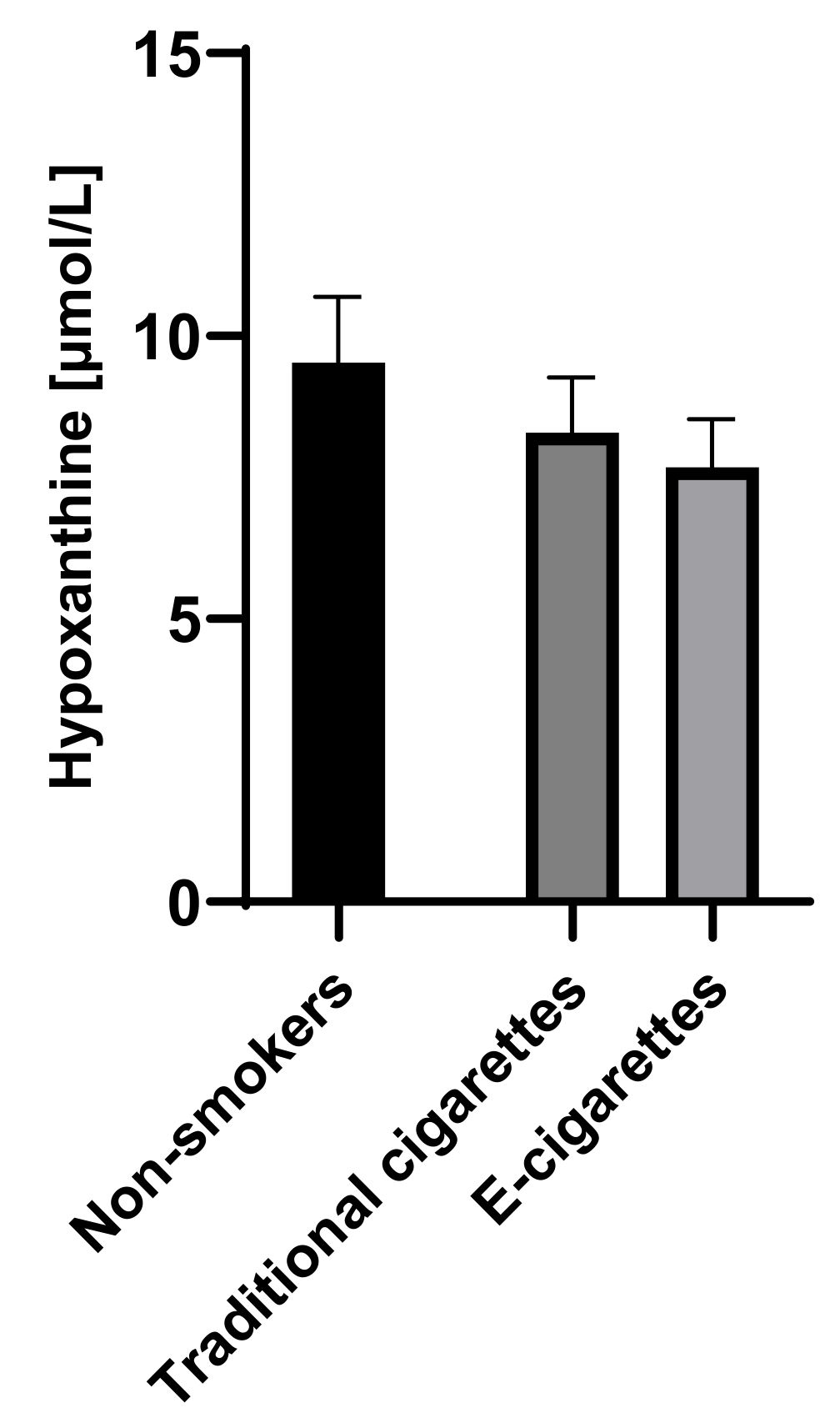
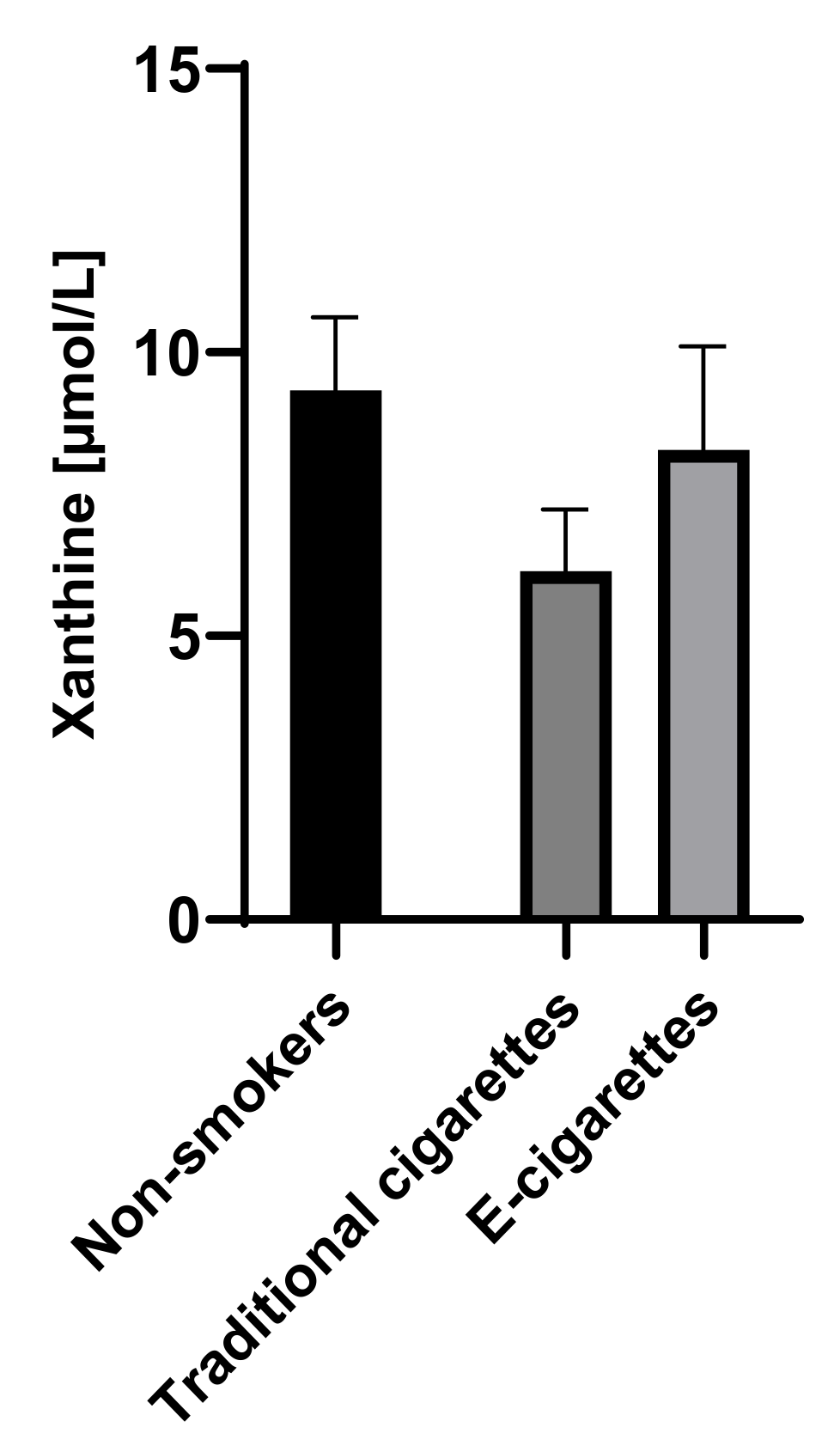
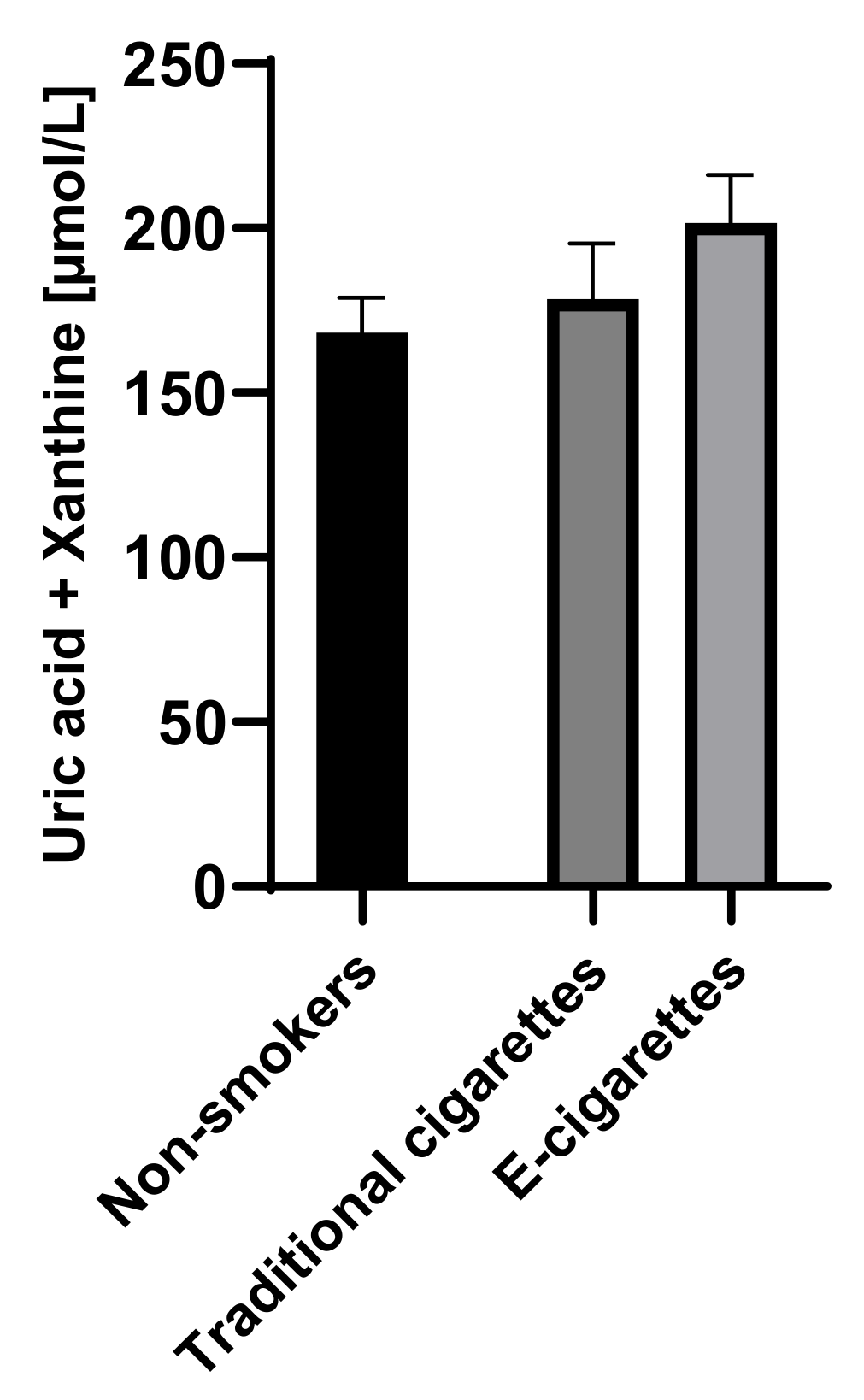
| Groups | UA [µmol/L] | Hx [µmol/L] | X [µmol/L] | UA + X [µmol/L] | TAOS [%] | TEAC [mM] |
|---|---|---|---|---|---|---|
| (SEM) | (SEM) | (SEM) | (SEM) | (SEM) | (SEM) | |
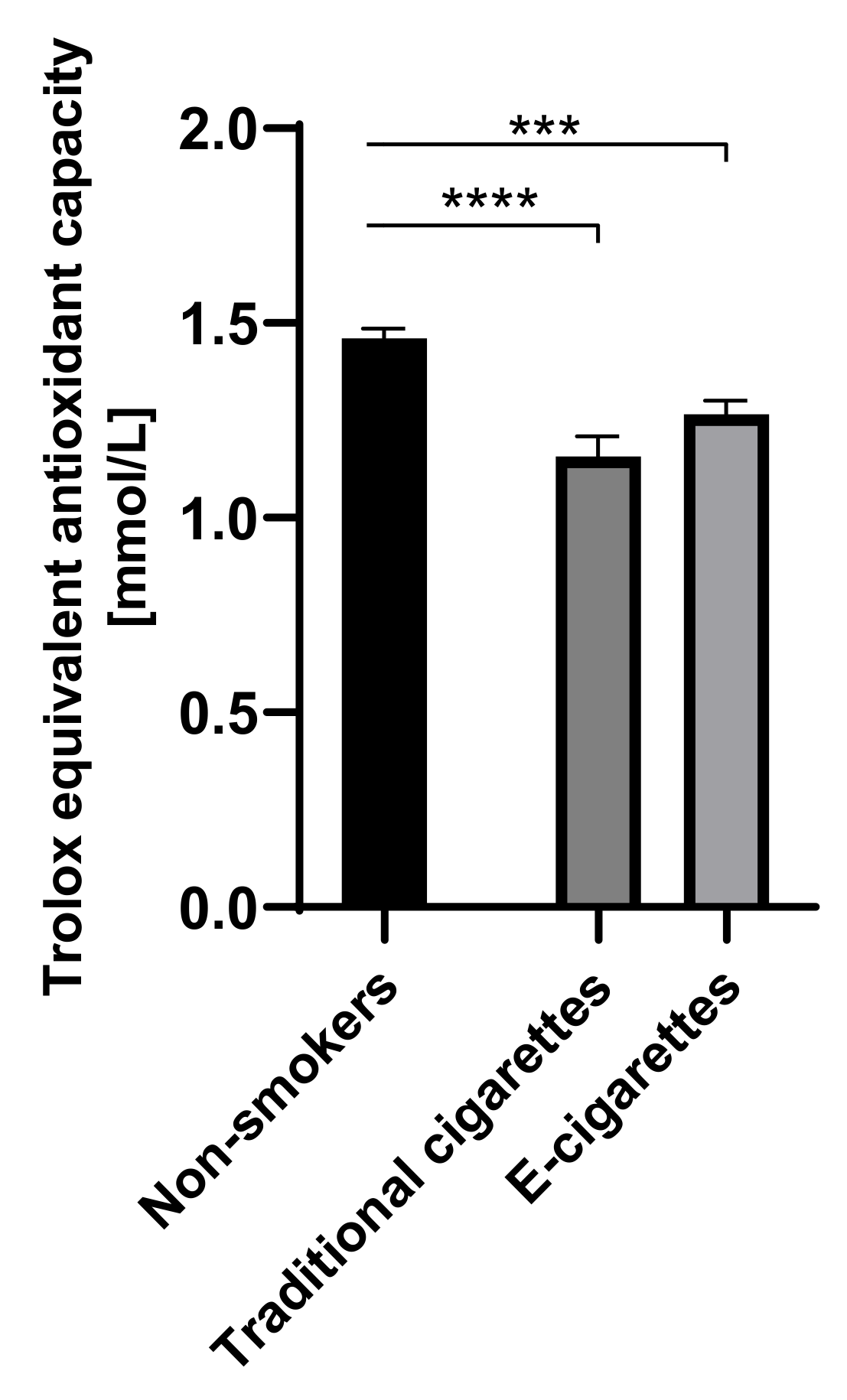
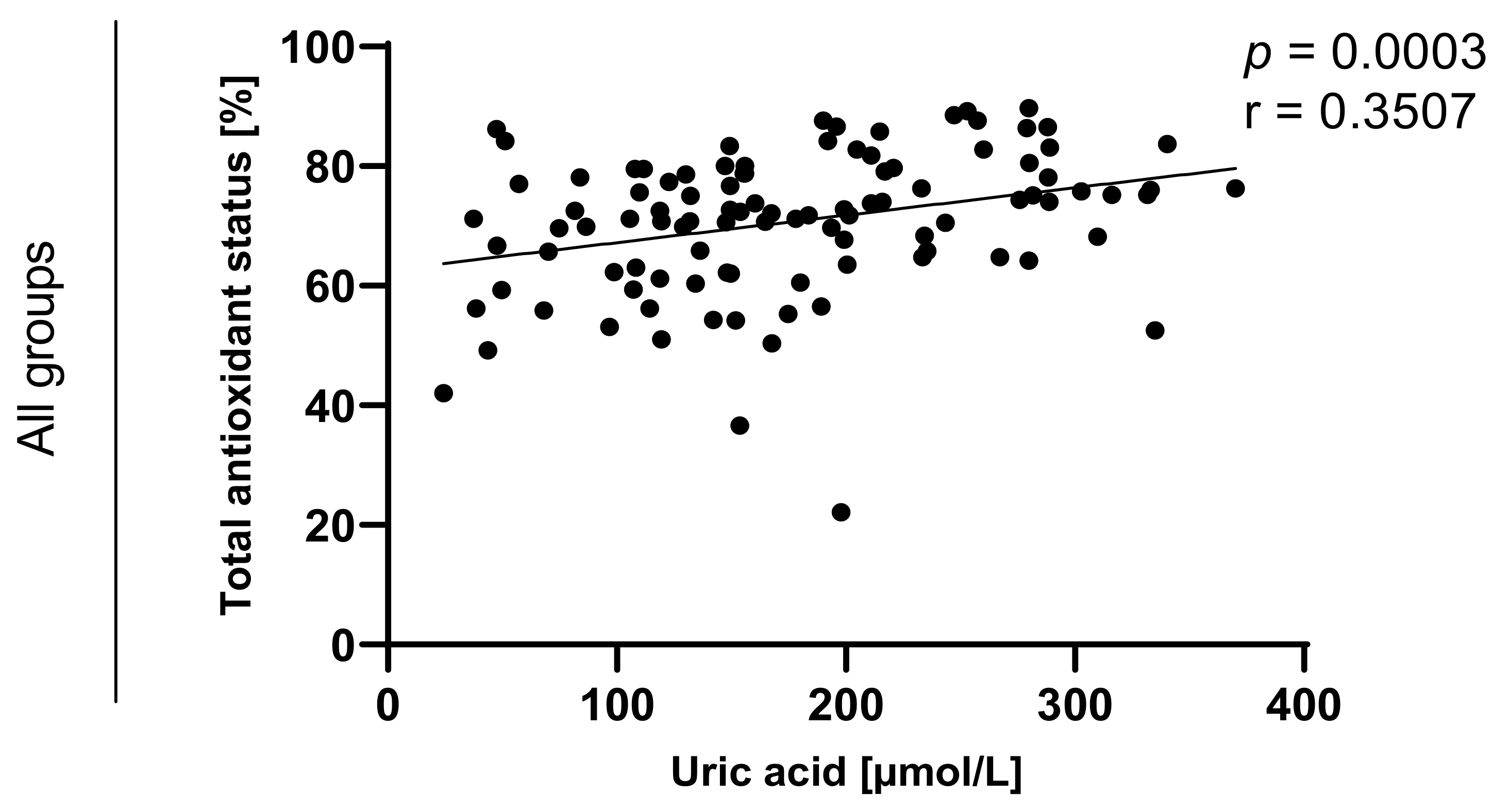
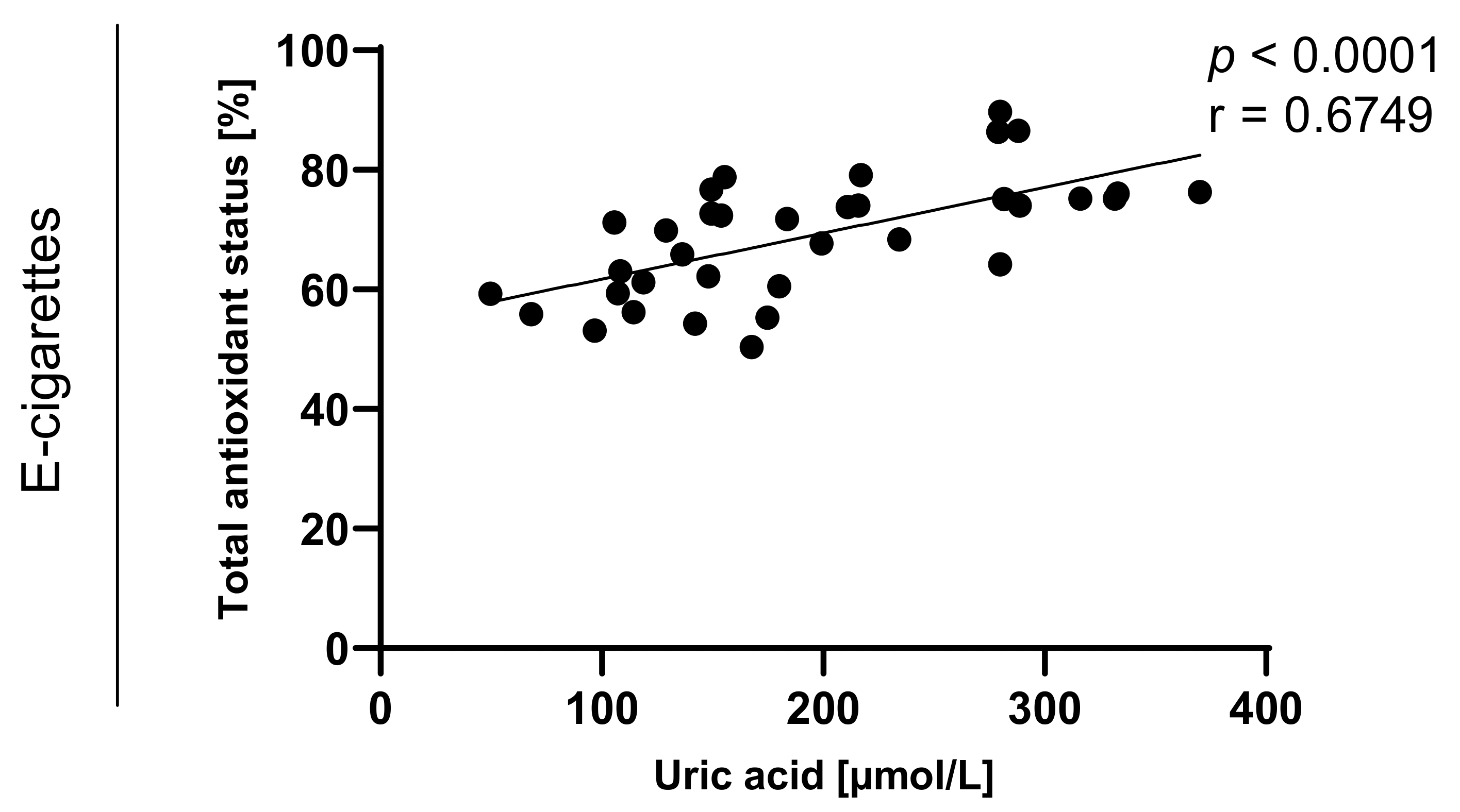
| E-cigarettes users | 193.3 (14.1) n = 35 | 7.7 (0.9) n = 35 | 8.3 (1.8) n = 35 | 201.6 (14.5) n = 35 | 68.9 (1.7) a n = 35 | 1.3 (0.04) c n = 35 |
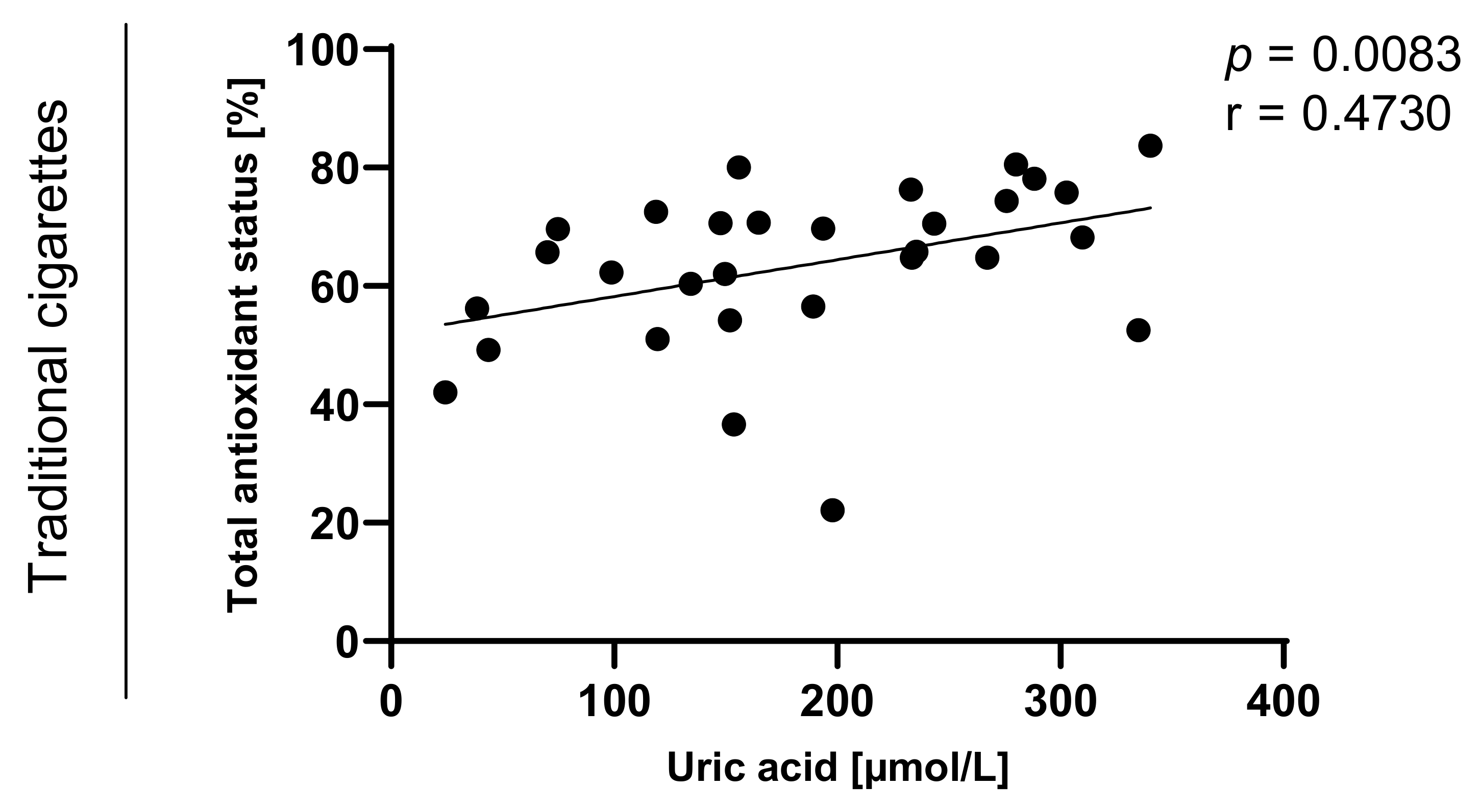
| Cigarettes smokers | 172.4 (16.8) n = 33 | 8.3 (1) n = 33 | 6.1 (1.1) n = 33 | 178.5 (16.8) n = 33 | 63.6 (2.4) b n = 31 | 1.2 (0.05) d n = 31 |
| Non-smokers | 158.9 (10.3) n = 42 | 9.5 (1.2) n = 42 | 9.3 (1.3) n = 42 | 168.2 (10.6) n = 42 | 78.1 (1.1) a,b n = 38 | 1.5 (0.03) c,d n = 38 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cichońska, D.; Król, O.; Słomińska, E.M.; Kochańska, B.; Świetlik, D.; Ochocińska, J.; Kusiak, A. Influence of Electronic Cigarettes on Antioxidant Capacity and Nucleotide Metabolites in Saliva. Toxics 2021, 9, 263. https://0-doi-org.brum.beds.ac.uk/10.3390/toxics9100263
Cichońska D, Król O, Słomińska EM, Kochańska B, Świetlik D, Ochocińska J, Kusiak A. Influence of Electronic Cigarettes on Antioxidant Capacity and Nucleotide Metabolites in Saliva. Toxics. 2021; 9(10):263. https://0-doi-org.brum.beds.ac.uk/10.3390/toxics9100263
Chicago/Turabian StyleCichońska, Dominika, Oliwia Król, Ewa M. Słomińska, Barbara Kochańska, Dariusz Świetlik, Jolanta Ochocińska, and Aida Kusiak. 2021. "Influence of Electronic Cigarettes on Antioxidant Capacity and Nucleotide Metabolites in Saliva" Toxics 9, no. 10: 263. https://0-doi-org.brum.beds.ac.uk/10.3390/toxics9100263