
Placental Transfer and Composition of Perfluoroalkyl Substances (PFASs): A Korean Birth Panel of Parent-Infant Triads

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population and Sample Collection
2.2. Analysis of PFASs in Serum and Quality Assurance
2.3. Statistical Analysis
3. Results
3.1. Demographic Characteristics of the Study Population
3.2. Detection of PFASs in Maternal, Paternal, and Cord Serum
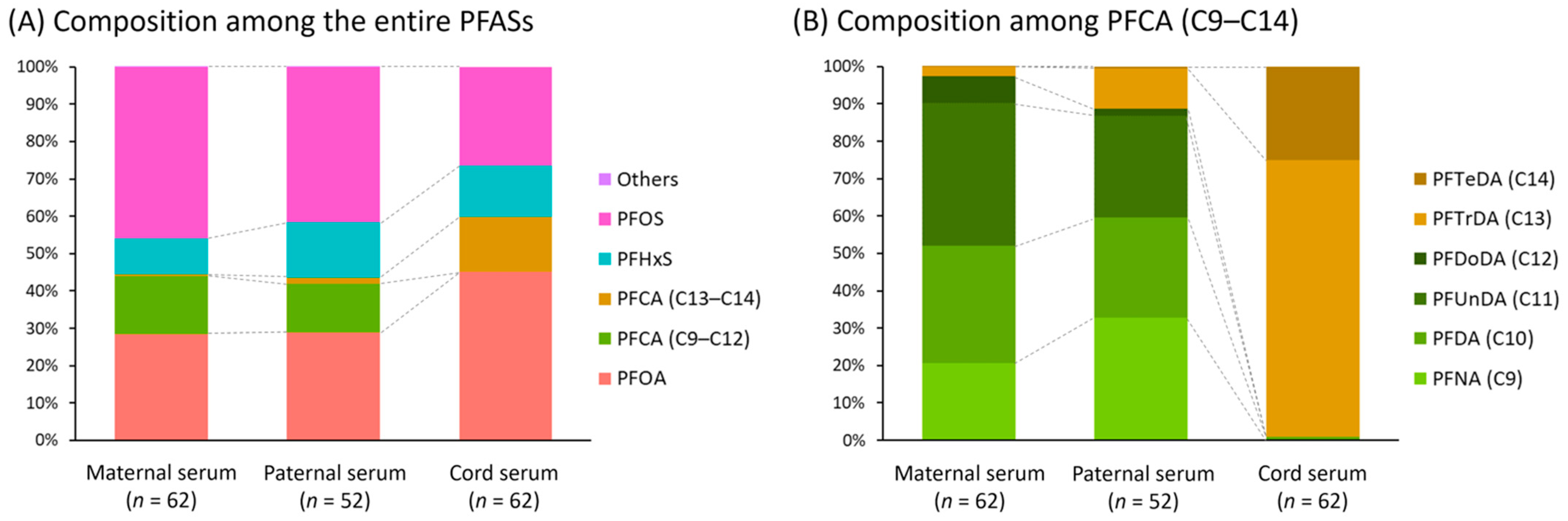
3.3. Composition Profiles of PFASs in Maternal, Paternal, and Cord Serum
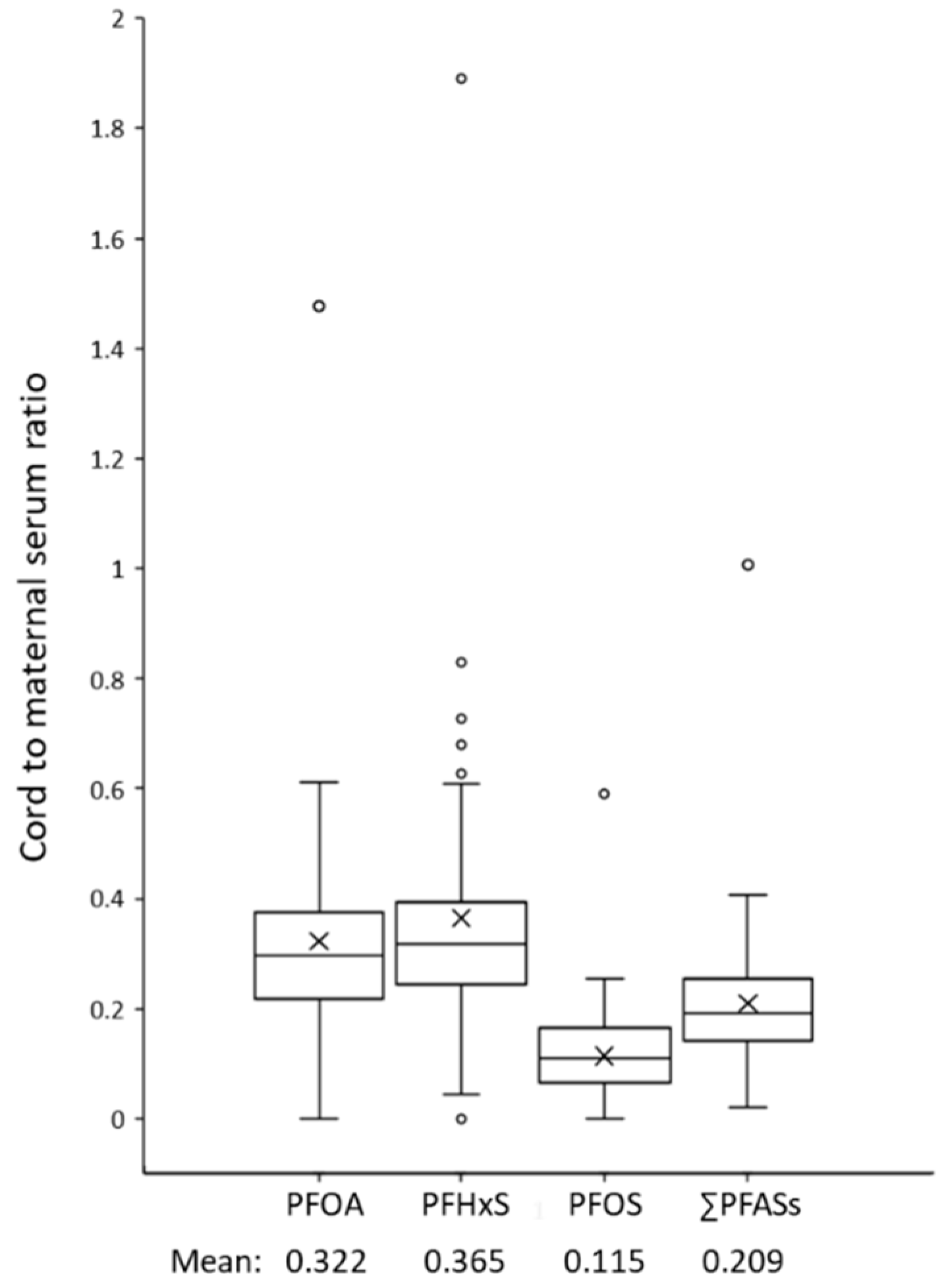
3.4. Placental Transfer Rates and Their Determinants
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Renner, R. Growing concern over perfluorinated chemicals. Environ. Sci. Technol. 2001, 35, 154A–160A. [Google Scholar] [CrossRef] [Green Version]
- Seacat, A.M.; Thomford, P.J.; Hansen, K.J.; Olsen, G.W.; Case, M.T.; Butenhoff, J.L. Subchronic toxicity studies on perfluorooctanesulfonate potassium salt in cynomolgus monkeys. Toxicol. Sci. 2002, 68, 249–264. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shoeib, M.; Harner, T.; Wilford, B.H.; Jones, K.C.; Zhu, J. Polyfluorinated compounds in the home: Levels in air and dust and human exposure. In Proceedings of the Fluoros International Symposium on Fluorinated Alkyl Organics in the Environment, Toronto, ON, Canada, 18–20 August 2005. [Google Scholar]
- Kang, H.; Lee, H.-K.; Moon, H.-B.; Kim, S.; Lee, J.; Ha, M.; Hong, S.; Kim, S.; Choi, K. Perfluoroalkyl acids in serum of Korean children: Occurrences, related sources, and associated health outcomes. Sci. Total Environ. 2018, 645, 958–965. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y.; Ro, A.; Bartell, S.M. Household low pile carpet usage was associated with increased serum PFAS concentrations in 2005–2006. Environ. Res. 2021, 195, 110758. [Google Scholar] [CrossRef] [PubMed]
- Domingo, J.L.; Nadal, M. Human exposure to per-and polyfluoroalkyl substances (PFAS) through drinking water: A review of the recent scientific literature. Environ. Res. 2019, 177, 108648. [Google Scholar] [CrossRef]
- Tittlemier, S.A.; Pepper, K.; Seymour, C.; Moisey, J.; Bronson, R.; Cao, X.-L.; Dabeka, R.W. Dietary exposure of Canadians to perfluorinated carboxylates and perfluorooctane sulfonate via consumption of meat, fish, fast foods, and food items prepared in their packaging. J. Agric. Food Chem. 2007, 55, 3203–3210. [Google Scholar] [CrossRef]
- Fenton, S.E.; Ducatman, A.; Boobis, A.; DeWitt, J.C.; Lau, C.; Ng, C.; Smith, J.S.; Roberts, S.M. Per- and polyfluoroalkyl substance toxicity and human health review: Current state of knowledge and strategies for informing future research. Environ. Toxicol. Chem. 2021, 40, 606–630. [Google Scholar] [CrossRef]
- Sweeney, J.B. The 3M company: Applying the theory and changing the world. J. Corp. Citizsh. 2016, 64, 37–46. [Google Scholar] [CrossRef]
- CEC. Regulation (EC) No. 1907/2006 of the European Parliament and of the Council of 18 December 2006 Concerning the Registration, Evaluation, Authorisation and Restriction of Chemicals (REACH). 2006. Available online: https://www.legislation.gov.uk/eur/2006/1907/contents (accessed on 9 April 2021).
- Wang, T.; Wang, Y.; Liao, C.; Cai, Y.; Jiang, G. Perspectives on the inclusion of perfluorooctane sulfonate into the Stockholm Convention on persistent organic pollutants. Environ. Sci Technol. 2009, 43, 5171–5175. [Google Scholar] [CrossRef] [Green Version]
- EPA—United States Environmental Protection Agency. PFOA Stewardship Program Homepage. 2010. Available online: http://www.epa.gov/oppt/pfoa/pubs/stewardship (accessed on 9 April 2021).
- EPA—United States Environmental Protection Agency. 2010/2015 PFOA Stewardship Program. 2006. Available online: https://www.epa.gov/assessing-and-managing-chemicals-under-tsca/fact-sheet-20102015-pfoa-stewardship-program (accessed on 9 April 2021).
- Ding, N.; Harlow, S.D.; Batterman, S.; Mukherjee, B.; Park, S.K. Longitudinal trends in perfluoroalkyl and polyfluoroalkyl substances among multiethnic midlife women from 1999 to 2011: The study of women’s health across the nation. Environ. Int. 2020, 135, 105381. [Google Scholar] [CrossRef]
- Toms, L.-M.; Thompson, J.; Rotander, A.; Hobson, P.; Calafat, A.; Kato, K.; Ye, X.; Broomhall, S.; Harden, F.; Mueller, J. Decline in perfluorooctane sulfonate and perfluorooctanoate serum concentrations in an Australian population from 2002 to 2011. Environ. Int. 2014, 71, 74–80. [Google Scholar] [CrossRef] [Green Version]
- Tsai, M.-S.; Miyashita, C.; Araki, A.; Itoh, S.; Bamai, Y.A.; Goudarzi, H.; Okada, E.; Kashino, I.; Matsuura, H.; Kishi, R. Determinants and temporal trends of perfluoroalkyl substances in pregnant women: The Hokkaido study on environment and children’s health. Int. J. Environ. Res. Public Health 2018, 15, 989. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Centers for Disease Control and Prevention. National Health and Nutrition Examination Survey 2017–2018: Data Documentation, Codebook, and Frequencies. Available online: https://www.cdc.gov/nchs/nhanes/index.htm (accessed on 9 April 2021).
- Vabre, P.; Gatimel, N.; Moreau, J.; Gayrard, V.; Picard-Hagen, N.; Parinaud, J.; Leandri, R.D. Environmental pollutants, a possible etiology for premature ovarian insufficiency: A narrative review of animal and human data. Environ. Health 2017, 16, 1–18. [Google Scholar] [CrossRef] [Green Version]
- Rashtian, J.; Chavkin, D.E.; Merhi, Z. Water and soil pollution as determinant of water and food quality/contamination and its impact on female fertility. Reprod. Biol. Endocrinol. 2019, 17, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, S.; Tan, R.; Pan, R.; Xiong, J.; Tian, Y.; Wu, J.; Chen, L. Association of perfluoroalkyl and polyfluoroalkyl substances with premature ovarian insufficiency in Chinese women. J. Clin. Endocrinol. Metab. 2018, 103, 2543–2551. [Google Scholar] [CrossRef] [Green Version]
- Wang, W.; Zhou, W.; Wu, S.; Liang, F.; Li, Y.; Zhang, J.; Cui, L.; Feng, Y.; Wang, Y. Perfluoroalkyl substances exposure and risk of polycystic ovarian syndrome related infertility in Chinese women. Environ. Pollut. 2019, 247, 824–831. [Google Scholar] [CrossRef] [PubMed]
- Ding, N.; Harlow, S.D.; Randolph, J.F., Jr.; Loch-Caruso, R.; Park, S.K. Perfluoroalkyl and polyfluoroalkyl substances (PFAS) and their effects on the ovary. Hum. Reprod. Update 2020, 26, 724–752. [Google Scholar] [CrossRef]
- Blake, B.E.; Fenton, S.E. Early life exposure to per- and polyfluoroalkyl substances (PFAS) and latent health outcomes: A review including the placenta as a target tissue and possible driver of peri- and postnatal effects. Toxicology 2020, 443, 152565. [Google Scholar] [CrossRef]
- Loccisano, A.E.; Longnecker, M.P.; Campbell, J.L., Jr.; Andersen, M.E.; Clewell, H.J. Development of PBPK models for PFOA and PFOS for human pregnancy and lactation life stages. J. Toxicol. Environ. Health Part A 2013, 76, 25–57. [Google Scholar] [CrossRef]
- Liu, Y.; Li, A.; An, Q.; Liu, K.; Zheng, P.; Yin, S.; Liu, W. Prenatal and postnatal transfer of perfluoroalkyl substances from mothers to their offspring. Crit. Rev. Environ. Sci. Technol. 2021, 1–28. [Google Scholar] [CrossRef]
- Cai, D.; Li, Q.-Q.; Chu, C.; Wang, S.-Z.; Tang, Y.-T.; Appleton, A.A.; Qiu, R.-L.; Yang, B.-Y.; Hu, L.-W.; Dong, G.-H. High trans-placental transfer of perfluoroalkyl substances alternatives in the matched maternal-cord blood serum: Evidence from a birth cohort study. Sci. Total Environ. 2020, 705, 135885. [Google Scholar] [CrossRef] [PubMed]
- Robledo, C.A.; Yeung, E.; Mendola, P.; Sundaram, R.; Maisog, J.; Sweeney, A.M.; Barr, D.B.; Louis, G.M.B. Preconception maternal and paternal exposure to persistent organic pollutants and birth size: The LIFE study. Environ. Health Perspect. 2015, 123, 88–94. [Google Scholar] [CrossRef] [PubMed]
- Tarapore, P.; Ouyang, B. Perfluoroalkyl chemicals and male reproductive health: Do PFOA and PFOS increase risk for male infertility? Int. J. Environ. Res. Public Health 2021, 18, 3794. [Google Scholar] [CrossRef]
- Steves, A.N.; Turry, A.; Gill, B.; Clarkson-Townsend, D.; Bradner, J.M.; Bachli, I.; Caudle, W.M.; Miller, G.W.; Chan, A.W.S.; Easley, C.A.T. Per- and polyfluoroalkyl substances impact human spermatogenesis in a stem-cell-derived model. Syst. Biol. Reprod. Med. 2018, 64, 225–239. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bae, J.; Kim, S.; Schisterman, E.F.; Boyd Barr, D.; Buck Louis, G.M. Maternal and paternal serum concentrations of perfluoroalkyl and polyfluoroalkyl substances and the secondary sex ratio. Chemosphere 2015, 133, 31–40. [Google Scholar] [CrossRef]
- Harada, K.H.; Hitomi, T.; Niisoe, T.; Takanaka, K.; Kamiyama, S.; Watanabe, T.; Moon, C.S.; Yang, H.R.; Hung, N.N.; Koizumi, A. Odd-numbered perfluorocarboxylates predominate over perfluorooctanoic acid in serum samples from Japan, Korea and Vietnam. Environ. Int. 2011, 37, 1183–1189. [Google Scholar] [CrossRef] [Green Version]
- Mamsen, L.S.; Jönsson, B.A.G.; Lindh, C.H.; Olesen, R.H.; Larsen, A.; Ernst, E.; Kelsey, T.W.; Andersen, C.Y. Concentration of perfluorinated compounds and cotinine in human foetal organs, placenta, and maternal plasma. Sci. Total Environ. 2017, 596, 97–105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bjerregaard-Olesen, C.; Bach, C.C.; Long, M.; Ghisari, M.; Bossi, R.; Bech, B.H.; Nohr, E.A.; Henriksen, T.B.; Olsen, J.; Bonefeld-Jørgensen, E.C. Time trends of perfluorinated alkyl acids in serum from Danish pregnant women 2008–2013. Environ. Int. 2016, 91, 14–21. [Google Scholar] [CrossRef]
- Lee, S.; Kim, S.; Park, J.; Kim, H.J.; Choi, G.; Choi, S.; Kim, S.; Kim, S.Y.; Kim, S.; Choi, K.; et al. Perfluoroalkyl substances (PFASs) in breast milk from Korea: Time-course trends, influencing factors, and infant exposure. Sci. Total Environ. 2018, 612, 286–292. [Google Scholar] [CrossRef]
- Lee, Y.A.; Kim, J.H.; Jung, H.W.; Lim, Y.-H.; Bae, S.; Kho, Y.; Hong, Y.-C.; Shin, C.H.; Yang, S.W. The serum concentrations of perfluoroalkyl compounds were inversely associated with growth parameters in 2-year old children. Sci. Total Environ. 2018, 628, 226–232. [Google Scholar] [CrossRef]
- Lee, Y.-M.; Lee, J.-Y.; Kim, M.-K.; Yang, H.; Lee, J.-E.; Son, Y.; Kho, Y.; Choi, K.; Zoh, K.-D. Concentration and distribution of per-and polyfluoroalkyl substances (PFAS) in the Asan Lake area of South Korea. J. Hazard. Mater. 2020, 381, 120909. [Google Scholar] [CrossRef]
- Barr, D.B.; Landsittel, D.; Nishioka, M.; Thomas, K.; Curwin, B.; Raymer, J.; Donnelly, K.C.; McCauley, L.; Ryan, P.B. A survey of laboratory and statistical issues related to farmworker exposure studies. Environ. Health Perspect. 2006, 114, 961–968. [Google Scholar] [CrossRef]
- Barrera-Gómez, J.; Basagaña, X. Models with transformed variables: Interpretation and software. Epidemiology 2015, 26, e16–e17. [Google Scholar] [CrossRef] [PubMed]
- Manzano-Salgado, C.B.; Casas, M.; Lopez-Espinosa, M.J.; Ballester, F.; Basterrechea, M.; Grimalt, J.O.; Jiménez, A.M.; Kraus, T.; Schettgen, T.; Sunyer, J.; et al. Transfer of perfluoroalkyl substances from mother to fetus in a Spanish birth cohort. Environ. Res. 2015, 142, 471–478. [Google Scholar] [CrossRef] [PubMed]
- Pan, Y.; Zhu, Y.; Zheng, T.; Cui, Q.; Buka, S.L.; Zhang, B.; Guo, Y.; Xia, W.; Yeung, L.W.; Li, Y.; et al. Novel chlorinated polyfluorinated ether sulfonates and legacy per-/polyfluoroalkyl substances: Placental transfer and relationship with serum albumin and glomerular filtration rate. Environ. Sci. Technol. 2017, 51, 634–644. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.; Choi, K.; Ji, K.; Seo, J.; Kho, Y.; Park, J.; Kim, S.; Park, S.; Hwang, I.; Jeon, J. Trans-placental transfer of thirteen perfluorinated compounds and relations with fetal thyroid hormones. Environ. Sci. Technol. 2011, 45, 7465–7472. [Google Scholar] [CrossRef]
- Eryasa, B.; Grandjean, P.; Nielsen, F.; Valvi, D.; Zmirou-Navier, D.; Sunderland, E.; Weihe, P.; Oulhote, Y. Physico-chemical properties and gestational diabetes predict transplacental transfer and partitioning of perfluoroalyl substances. Environ. Int. 2019, 130, 104874. [Google Scholar] [CrossRef]
- Zhao, L.; Zhang, Y.; Zhu, L.; Ma, X.; Wang, Y.; Sun, H.; Luo, Y. Isomer-specific transplacental efficiencies of perfluoroalkyl substances in human whole blood. Environ. Sci. Technol. Lett. 2017, 4, 391–398. [Google Scholar] [CrossRef]
- Li, J.; Cai, D.; Chu, C.; Li, Q.; Zhou, Y.; Hu, L.; Yang, B.; Dong, G.; Zeng, X.; Chen, D. Transplacental transfer of per- and polyfluoroalkyl substances (PFASs): Differences between preterm and full-term deliveries and associations with placental transporter mRNA expression. Environ. Sci. Technol. 2020, 54, 5062–5070. [Google Scholar] [CrossRef]
- Chen, F.; Yin, S.; Kelly, B.C.; Liu, W. Isomer-specific transplacental transfer of perfluoroalkyl acids: Results from a survey of paired maternal, cord sera, and placentas. Environ. Sci. Technol. 2017, 51, 5756–5763. [Google Scholar] [CrossRef]
- Li, Y.; Yu, N.; Du, L.; Shi, W.; Yu, H.; Song, M.; Wei, S. Transplacental transfer of per- and polyfluoroalkyl substances identified in paired maternal and cord sera using suspect and nontarget screening. Environ. Sci. Technol. 2020, 54, 3407–3416. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.J.; Kim, M.-K.; Bae, J.; Yang, J.-H. Concentrations of perfluoroalkyl compounds in maternal and umbilical cord sera and birth outcomes in Korea. Chemosphere 2013, 90, 1603–1609. [Google Scholar] [CrossRef] [PubMed]
- Zhang, T.; Sun, H.; Lin, Y.; Qin, X.; Zhang, Y.; Geng, X.; Kannan, K. Distribution of poly- and perfluoroalkyl substances in matched samples from pregnant women and carbon chain length related maternal transfer. Environ. Sci. Technol. 2013, 47, 7974–7981. [Google Scholar] [CrossRef]
- Liu, J.; Li, J.; Liu, Y.; Chan, H.M.; Zhao, Y.; Cai, Z.; Wu, Y. Comparison on gestation and lactation exposure of perfluorinated compounds for newborns. Environ. Int. 2011, 37, 1206–1212. [Google Scholar] [CrossRef]
- Seo, S.-H.; Son, M.-H.; Choi, S.-D.; Lee, D.-H.; Chang, Y.-S. Influence of exposure to perfluoroalkyl substances (PFASs) on the Korean general population: 10-year trend and health effects. Environ. Int. 2018, 113, 149–161. [Google Scholar] [CrossRef] [PubMed]
- Gao, K.; Zhuang, T.; Liu, X.; Fu, J.; Zhang, J.; Fu, J.; Wang, L.; Zhang, A.; Liang, Y.; Song, M. Prenatal exposure to per- and polyfluoroalkyl substances (PFASs) and association between the placental transfer efficiencies and dissociation constant of serum proteins–PFAS complexes. Environ. Sci. Technol. 2019, 53, 6529–6538. [Google Scholar] [CrossRef]
- Gützkow, K.B.; Haug, L.S.; Thomsen, C.; Sabaredzovic, A.; Becher, G.; Brunborg, G. Placental transfer of perfluorinated compounds is selective—A Norwegian mother and child sub-cohort study. Int. J. Hyg. Environ. Health 2012, 215, 216–219. [Google Scholar] [CrossRef]
- Han, W.; Gao, Y.; Yao, Q.; Yuan, T.; Wang, Y.; Zhao, S.; Shi, R.; Bonefeld-Jorgensen, E.C.; Shen, X.; Tian, Y. Perfluoroalkyl and polyfluoroalkyl substances in matched parental and cord serum in Shandong, China. Environ. Int. 2018, 116, 206–213. [Google Scholar] [CrossRef]
- Ma, X.; Cui, L.; Chen, L.; Zhang, J.; Zhang, X.; Kang, Q.; Jin, F.; Ye, Y. Parental plasma concentrations of perfluoroalkyl substances and in vitro fertilization outcomes. Environ. Pollut. 2021, 269, 116159. [Google Scholar] [CrossRef]
- Wu, X.M.; Bennett, D.H.; Calafat, A.M.; Kato, K.; Strynar, M.; Andersen, E.; Moran, R.E.; Tancredi, D.J.; Tulve, N.S.; Hertz-Picciotto, I. Serum concentrations of perfluorinated compounds (PFC) among selected populations of children and adults in California. Environ. Res. 2015, 136, 264–273. [Google Scholar] [CrossRef] [Green Version]
- Forsthuber, M.; Kaiser, A.M.; Granitzer, S.; Hassl, I.; Hengstschläger, M.; Stangl, H.; Gundacker, C. Albumin is the major carrier protein for PFOS, PFOA, PFHxS, PFNA and PFDA in human plasma. Environ. Int. 2020, 137, 105324. [Google Scholar] [CrossRef]
- Mamsen, L.S.; Björvang, R.D.; Mucs, D.; Vinnars, M.T.; Papadogiannakis, N.; Lindh, C.H.; Andersen, C.Y.; Damdimopoulou, P. Concentrations of perfluoroalkyl substances (PFASs) in human embryonic and fetal organs from first, second, and third trimester pregnancies. Environ. Int. 2019, 124, 482–492. [Google Scholar] [CrossRef] [PubMed]
- Wikström, S.; Lin, P.I.; Lindh, C.H.; Shu, H.; Bornehag, C.G. Maternal serum levels of perfluoroalkyl substances in early pregnancy and offspring birth weight. Pediatric Res. 2020, 87, 1093–1099. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Manea, S.; Salmaso, L.; Lorenzoni, G.; Mazzucato, M.; Russo, F.; Mantoan, D.; Martuzzi, M.; Fletcher, T.; Facchin, P. Exposure to PFAS and small for gestational age new-borns: A birth records study in Veneto region (Italy). Environ. Res. 2020, 184, 109282. [Google Scholar] [CrossRef] [PubMed]
- Conley, J.M.; Lambright, C.S.; Evans, N.; McCord, J.; Strynar, M.J.; Hill, D.; Medlock-Kakaley, E.; Wilson, V.S.; Gray, L.E., Jr. Hexafluoropropylene oxide-dimer acid (HFPO-DA or GenX) alters maternal and fetal glucose and lipid metabolism and produces neonatal mortality, low birthweight, and hepatomegaly in the Sprague-Dawley rat. Environ. Int. 2021, 146, 106204. [Google Scholar] [CrossRef]
- Kafle, R.; Nibedita, K.; Gupta, B.K. Mean birth weight and mean placental weight among deliveries in a tertiary care hospital. J. Nepal Med. Assoc. 2019, 57, 364–366. [Google Scholar] [CrossRef] [Green Version]
- Torous, V.F.; Roberts, D.J. Placentas from women of advanced maternal age. Arch. Pathol. Lab. Med. 2020, 144, 1254–1261. [Google Scholar] [CrossRef] [Green Version]
- Miremerg, H.; Frig, O.; Rona, S.; Ganer Herman, H.; Mizrachi, Y.; Schreiber, L.; Bar, J.; Kovo, M.; Weiner, E. Is advanced maternal age associated with placental vascular malperfusion? A prospective study from a single tertiary center. Arch. Gynecol. Obstet. 2020, 301, 1441–1447. [Google Scholar] [CrossRef] [PubMed]
- Woods, L.; Perez-Garcia, V.; Kieckbusch, J.; Wang, X.; DeMayo, F.; Colucci, F.; Hemberger, M. Decidualisation and placentation defects are a major cause of age-related reproductive decline. Nat. Commun. 2017, 8, 352. [Google Scholar] [CrossRef] [Green Version]
- Cunningham, F.G.; Leveno, K.J.; Bloom, S.L.; Hauth, J.C.; Gilstrap, L.C., III; Wenstrom, K.D. Williams Obstetrics, 22nd ed.; McGraw-Hill: New York, NY, USA, 2005. [Google Scholar]



{kind=link}
{kind=link}
| n (%) | Arithmetic Mean ± SD (Range) a | |
|---|---|---|
| Maternal Variables | ||
| Maternal age (year) | 62 (100) | 32 ± 3 (26–41) |
| Maternal education | ||
| ≤12 year | 11 (18) | |
| >12 year | 51 (82) | |
| Family income | ||
| <3000 USD/month | 30 (48) | |
| ≥3000 USD/month | 32 (52) | |
| Smoking history | ||
| Never smoker | 58 (94) | |
| Former smoker | 4 (6) | |
| Current smoker | 0 (0) | |
| Pre-pregnant BMI (kg/m2) b | 62 (100) | 22.0 ± 3.9 (16.6–32.2) |
| Pre-pregnant weight (kg) | 62 (100) | 57.4 ± 11.0 (43.0–95.0) |
| Parity | ||
| 0 | 34 (55) | |
| 1 | 21 (34) | |
| ≥2 | 7 (11) | |
| Paternal Variable c | ||
| Paternal age (year) | 52 (100) | 34 ± 4 (27–41) |
| Paternal education | ||
| ≤12 year | 11 (21) | |
| >12 year | 41 (79) | |
| Smoking history | ||
| Never smoker | 14 (27) | |
| Former smoker | 21 (40) | |
| Current smoker | 17 (33) | |
| Birth Outcome | ||
| Birth weight (kg) | 62 (100) | 2.94 ± 0.56 (1.71–3.94) |
| Placental weight (g) | 58 (94) d | 567 ± 127 (335–800) |
| Gestational age (week) | 62 (100) | 37.5 ± 2.5 (30.6–41.0) |
| Infant sex | ||
| Male | 35 (56) | |
| Female | 27 (44) |
| Compound | Serum Type | n | Detection Frequency (%) | GM ± SD a | Percentiles | ||
|---|---|---|---|---|---|---|---|
| 25th | 50th | 75th | |||||
| PFOA | Maternal serum | 62 | 100 | 1.41 ± 1.63 | 1.08 | 1.32 | 1.96 |
| Paternal serum | 52 | 100 | 1.44 ± 1.92 | 0.98 | 1.29 | 1.79 | |
| Cord serum | 62 | 98 | 0.40 ± 2.03 | 0.30 | 0.41 | 0.61 | |
| PFNA | Maternal serum | 62 | 85 | 0.15 ± 2.67 | 0.04 | 0.14 | 0.25 |
| Paternal serum | 52 | 56 | - | <0.03 | 0.13 | 0.37 | |
| Cord serum | 62 | 0 | - | <0.03 | <0.03 | <0.03 | |
| PFDA | Maternal serum | 62 | 100 | 0.26 ± 1.58 | 0.19 | 0.26 | 0.33 |
| Paternal serum | 52 | 90 | 0.21 ± 2.00 | 0.11 | 0.18 | 0.28 | |
| Cord serum | 62 | 3 | - | <0.06 | <0.06 | <0.06 | |
| PFUnDA | Maternal serum | 62 | 92 | 0.32 ± 1.85 | 0.17 | 0.29 | 0.52 |
| Paternal serum | 52 | 69 | - | <0.05 | 0.16 | 0.28 | |
| Cord serum | 62 | 0 | - | <0.05 | <0.05 | <0.05 | |
| PFDoDA | Maternal serum | 62 | 60 | - | <0.07 | 0.08 | 0.10 |
| Paternal serum | 52 | 10 | - | <0.07 | <0.07 | <0.07 | |
| Cord serum | 62 | 0 | - | <0.07 | <0.07 | <0.07 | |
| PFTrDA | Maternal serum | 62 | 8 | - | <0.05 | <0.05 | <0.05 |
| Paternal serum | 52 | 65 | - | <0.05 | 0.06 | 0.15 | |
| Cord serum | 62 | 55 | - | <0.05 | 0.14 | 0.22 | |
| PFTeDA | Maternal serum | 62 | 2 | - | <0.03 | <0.03 | <0.03 |
| Paternal serum | 52 | 10 | - | <0.03 | <0.03 | <0.03 | |
| Cord serum | 62 | 52 | - | <0.03 | 0.03 | 0.06 | |
| PFHxS | Maternal serum | 62 | 100 | - | 0.32 | 0.44 | 0.60 |
| Paternal serum | 52 | 100 | - | 0.61 | 0.72 | 0.87 | |
| Cord serum | 62 | 97 | - | 0.10 | 0.15 | 0.20 | |
| PFOS | Maternal serum | 62 | 100 | 2.31 ± 1.58 | 1.75 | 2.35 | 3.18 |
| Paternal serum | 52 | 100 | 2.21 ± 1.84 | 1.48 | 2.04 | 3.05 | |
| Cord serum | 62 | 90 | 0.25 ± 2.03 | 0.13 | 0.26 | 0.39 | |
| ∑PFCAs b | Maternal serum | 62 | - | 2.17 ± 1.72 | 1.62 | 2.07 | 2.95 |
| Paternal serum | 52 | - | 2.01 ± 2.12 | 1.27 | 1.75 | 2.92 | |
| Cord serum | 62 | - | 0.51 ± 2.24 | 0.37 | 0.62 | 0.89 | |
| ∑PFSAs c | Maternal serum | 62 | - | 2.79 ± 1.57 | 2.01 | 2.87 | 3.63 |
| Paternal serum | 52 | - | 3.05 ± 1.78 | 2.12 | 2.78 | 3.82 | |
| Cord serum | 62 | - | 0.36 ± 2.07 | 0.25 | 0.42 | 0.61 | |
| ∑PFASs d | Maternal serum | 62 | - | 5.02 ± 1.61 | 3.76 | 5.19 | 6.30 |
| Paternal serum | 52 | - | 5.11 ± 1.90 | 3.51 | 4.59 | 6.47 | |
| Cord serum | 62 | - | 0.87 ± 2.15 | 0.65 | 1.02 | 1.55 | |
| Reference | Country | Sample Size | Blood Type | Sampling of Maternal Blood | Placental Transfer Rate b | ||
|---|---|---|---|---|---|---|---|
| PFOA | PFHxS | PFOS | |||||
| Wang et al., 2019 [21] | China | 369 | Serum | Not specified | 0.83 | 0.95 | 0.30 |
| Manzano-Salgado et al., 2015 [39] | Spain | 53–66 | Serum | 12nd week | 1.90 | 0.40 | 1.86 |
| Pan et al., 2017 [40] | China | ≤100 | Serum | 1st, 2nd, or 3rd trimester | 0.66 | 0.49 | 0.35 |
| Kim et al., 2011 [41] a | Korea | ≤44 | Serum | Mostly during the third trimester of pregnancy, but several subjects were sampled earlier | 1.02 | 0.72 | 0.48 |
| Eryasa et al., 2019 [42] | FaroeIslands | 151 | Serum | 32nd week | 0.80 | 0.62 | 0.38 |
| Zhao et al., 2017 [43] | China | ≤63 | Blood | 3rd trimester or within the 1st week after delivery | 0.57 | 0.35 | 0.20 |
| Cai et al., 2020 [26] | China | ≤423 | Serum | Within 1 week before delivery | 0.73 | 0.46 | 0.42 |
| Li, Cai et al., 2020 [44] | China | ≤187 | Serum | Within 1 week before delivery | 0.85 | 0.72 | 0.58 |
| Chen et al., 2017 [45] | China | ≤32 | Serum | Within 3 days before delivery | 0.77 | 0.55 | 0.40 |
| Li, Yu, et al., 2020 [46] | China | 117 | Serum | Within 3 days before delivery | 1.03 | 0.83 | 0.46 |
| Lee et al., 2013 [47] | Korea | 59 | Serum | At delivery | 0.80 | 0.50 | 0.32 |
| Zhang et al., 2013 [48] | China | 30 | Blood | Within 1 hour of delivery | 0.57 | 0.32 | 0.18 |
| Liu et al., 2011 [49] | China | ≤50 | Serum | Within the first week after delivery | 0.89 | 0.73 | 0.54 |
| This study | Korea | 62 | Serum | At delivery | 0.32 | 0.36 | 0.12 |
| Potential Determinant | PFOA | PFHxS | PFOS | ∑PFCAs | ∑PFSAs | ∑PFASs |
|---|---|---|---|---|---|---|
| Maternal age (IQR: 30–34 y) b | −0.05 (−0.11, 0.01) | −0.04 (−0.11, 0.04) | −0.03 (−0.05, 0.00) | −0.06 (−0.11, −0.01) * | −0.03 (−0.06, 0.00) | −0.04 (−0.08, 0.00) * |
| Pre-pregnant BMI (IQR: 19.7–23.9 kg/m2) b | −0.05 (−0.10, 0.01) | −0.05 (−0.12, 0.02) | −0.03 (−0.05, 0.00) * | −0.05 (−0.09, 0.00) * | −0.03 (−0.05, 0.00) | −0.04 (−0.07, 0.00) |
| Pre-pregnant weight (IQR: 50–62 kg) b | −0.05 (−0.11, 0.00) | −0.06 (−0.13, 0.01) | −0.03 (−0.05, 0.00) * | −0.06 (−0.10, 0.00) * | −0.03 (−0.06, 0.00) * | −0.04 (−0.08, 0.00) * |
| Weight gain (IQR: 8–17 kg) b | 0.05 (−0.03, 0.14) | −0.02 (−0.08, 0.13) | 0.02 (−0.02, 0.06) | 0.05 (−0.02, 0.12) | 0.02 (−0.02, 0.06) | 0.03 (−0.02, 0.09) |
| Birth weight (IQR: 2.56–3.38 kg) b | 0.10 (0.04, 0.18) ** | 0.09 (−0.01, 0.18) | 0.04 (0.01, 0.08) ** | 0.07 (0.01, 0.13) * | 0.05 (0.01, 0.08) * | 0.06 (0.01, 0.11) * |
| Placental weight (IQR: 478–650 g) b | 0.04 (−0.03, 0.12) | 0.07 (−0.03, 0.16) | 0.02 (−0.01, 0.06) | 0.03 (−0.03, 0.10) | 0.03 (−0.01, 0.06) | 0.03 (−0.02, 0.08) |
| Gestational age (IQR: 35.4–39.6 wk) b | 0.12 (0.03, 0.20) ** | 0.10 (−0.01, 0.20) | 0.04 (0.01, 0.08) * | 0.07 (0.00, 0.14) | 0.05 (0.00, 0.09) * | 0.06 (0.00, 0.12) * |
| Infant sex (female vs. male) c | 0.01 (−0.10, 0.11) | −0.03 (−0.16, 0.10) | 0.00 (−0.05, 0.04) | 0.02 (−0.07, 0.11) | 0.00 (−0.06, 0.05) | 0.01 (−0.06, 0.08) |
| Parity (≥ 1 vs. 0) c | −0.07 (−0.18, 0.03) | −0.01 (−0.14, 0.12) | −0.02 (−0.07, 0.02) | −0.05 (−0.14, 0.04) | −0.03 (−0.08, 0.03) | −0.04 (−0.11, 0.02) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kang, H.; Kim, H.-S.; Yoon, Y.S.; Lee, J.; Kho, Y.; Lee, J.; Chang, H.J.; Cho, Y.H.; Kim, Y.A. Placental Transfer and Composition of Perfluoroalkyl Substances (PFASs): A Korean Birth Panel of Parent-Infant Triads. Toxics 2021, 9, 168. https://0-doi-org.brum.beds.ac.uk/10.3390/toxics9070168
Kang H, Kim H-S, Yoon YS, Lee J, Kho Y, Lee J, Chang HJ, Cho YH, Kim YA. Placental Transfer and Composition of Perfluoroalkyl Substances (PFASs): A Korean Birth Panel of Parent-Infant Triads. Toxics. 2021; 9(7):168. https://0-doi-org.brum.beds.ac.uk/10.3390/toxics9070168
Chicago/Turabian StyleKang, Habyeong, Hee-Sun Kim, Yeong Sook Yoon, Jeongsun Lee, Younglim Kho, Jisun Lee, Hye Jin Chang, Yoon Hee Cho, and Young Ah Kim. 2021. "Placental Transfer and Composition of Perfluoroalkyl Substances (PFASs): A Korean Birth Panel of Parent-Infant Triads" Toxics 9, no. 7: 168. https://0-doi-org.brum.beds.ac.uk/10.3390/toxics9070168