
Neuron-Specific Enolase (NSE) Predicts Long-Term Mortality in Adult Patients after Cardiac Arrest: Results from a Prospective Trial

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Material and Methods
2.1. Study Setting
2.2. Study Population and Treatment of Patients during the Trial
2.3. Data Collection
2.4. Outcomes
2.5. Statistical Analyses
3. Results
3.1. Baseline Characteristics
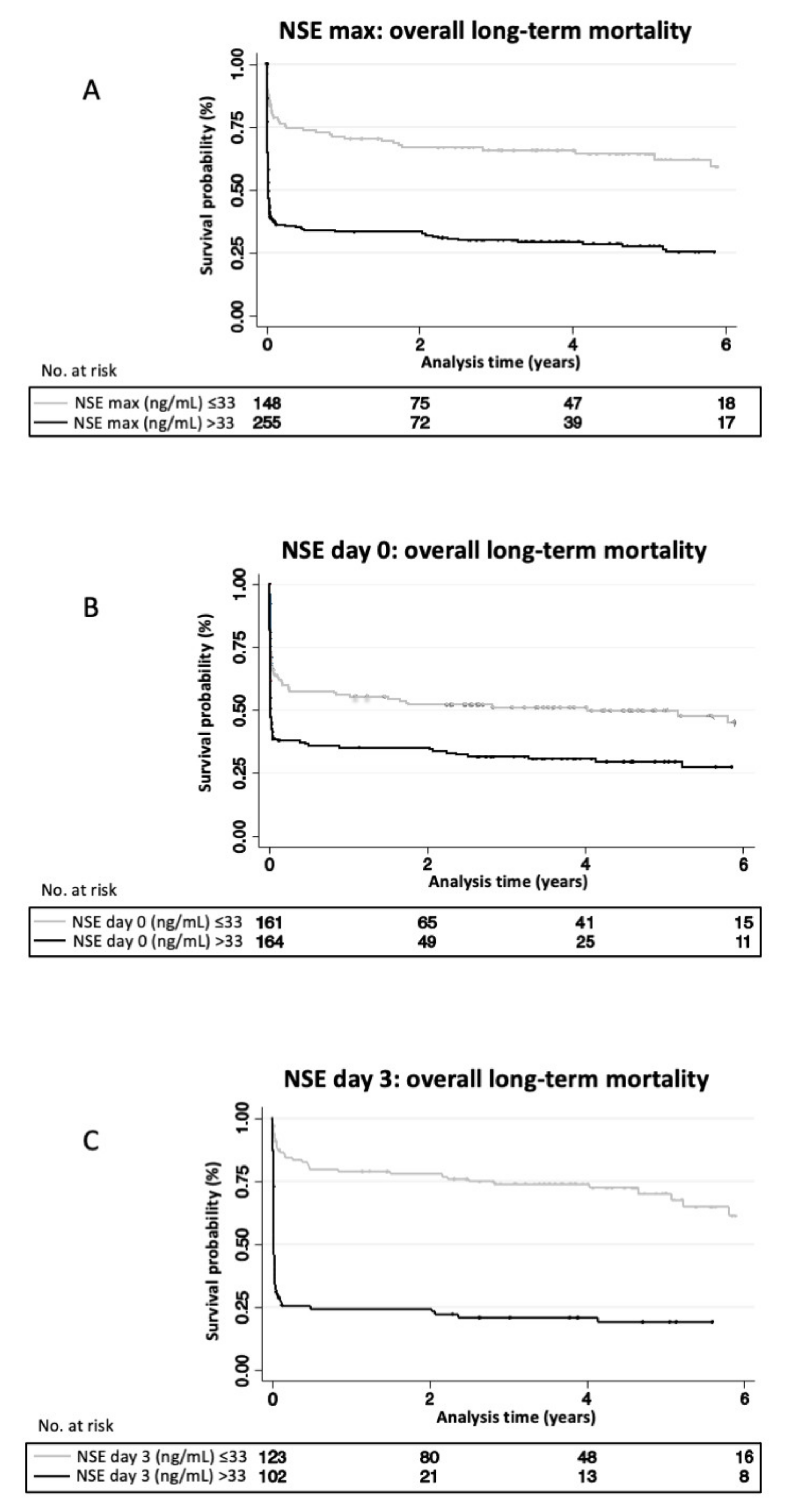
3.2. Association between NSE Blood Levels and Overall Long-Term Mortality
3.3. Association between NSE Blood Levels and Neurological Outcome at 2 Years
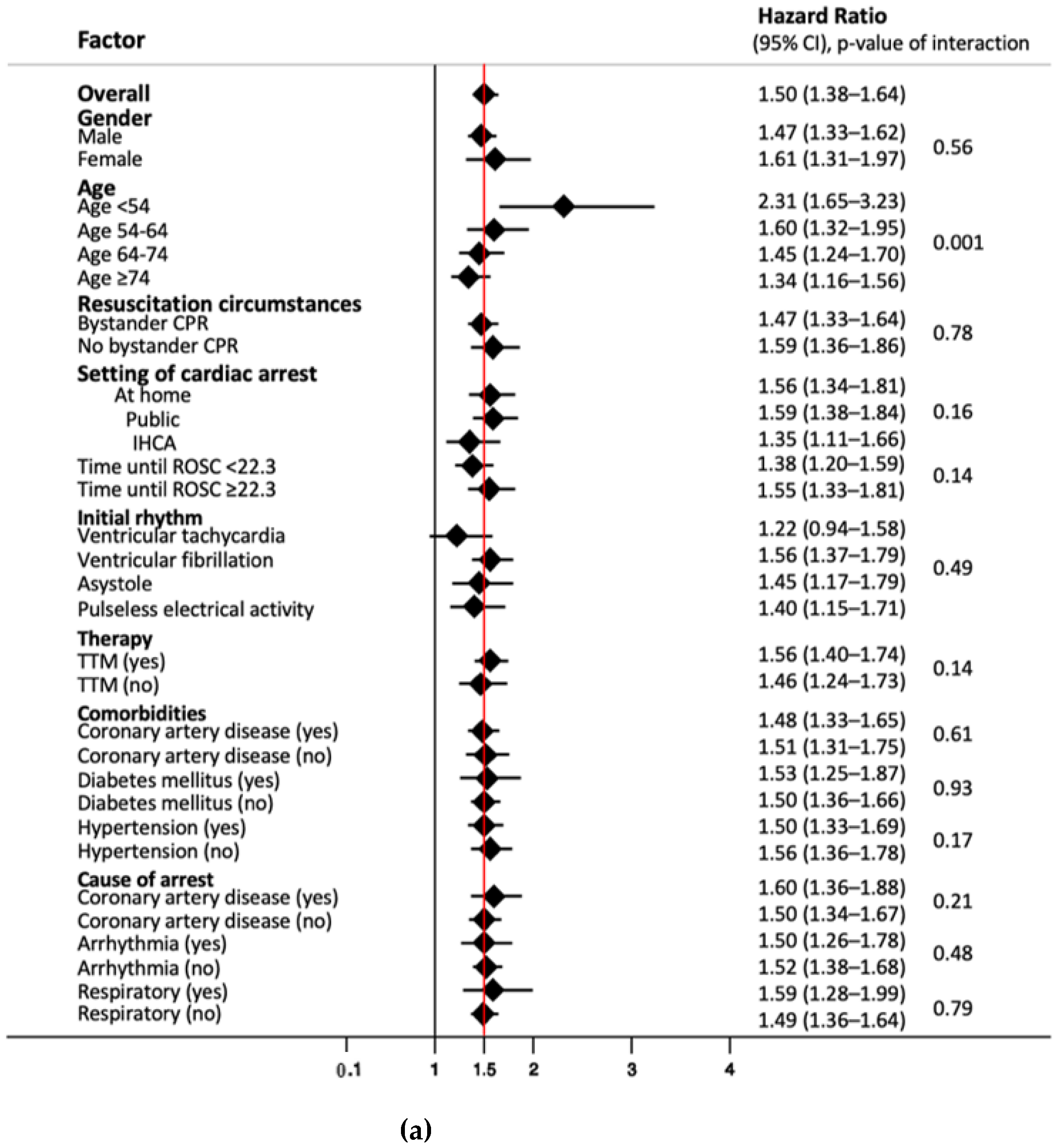
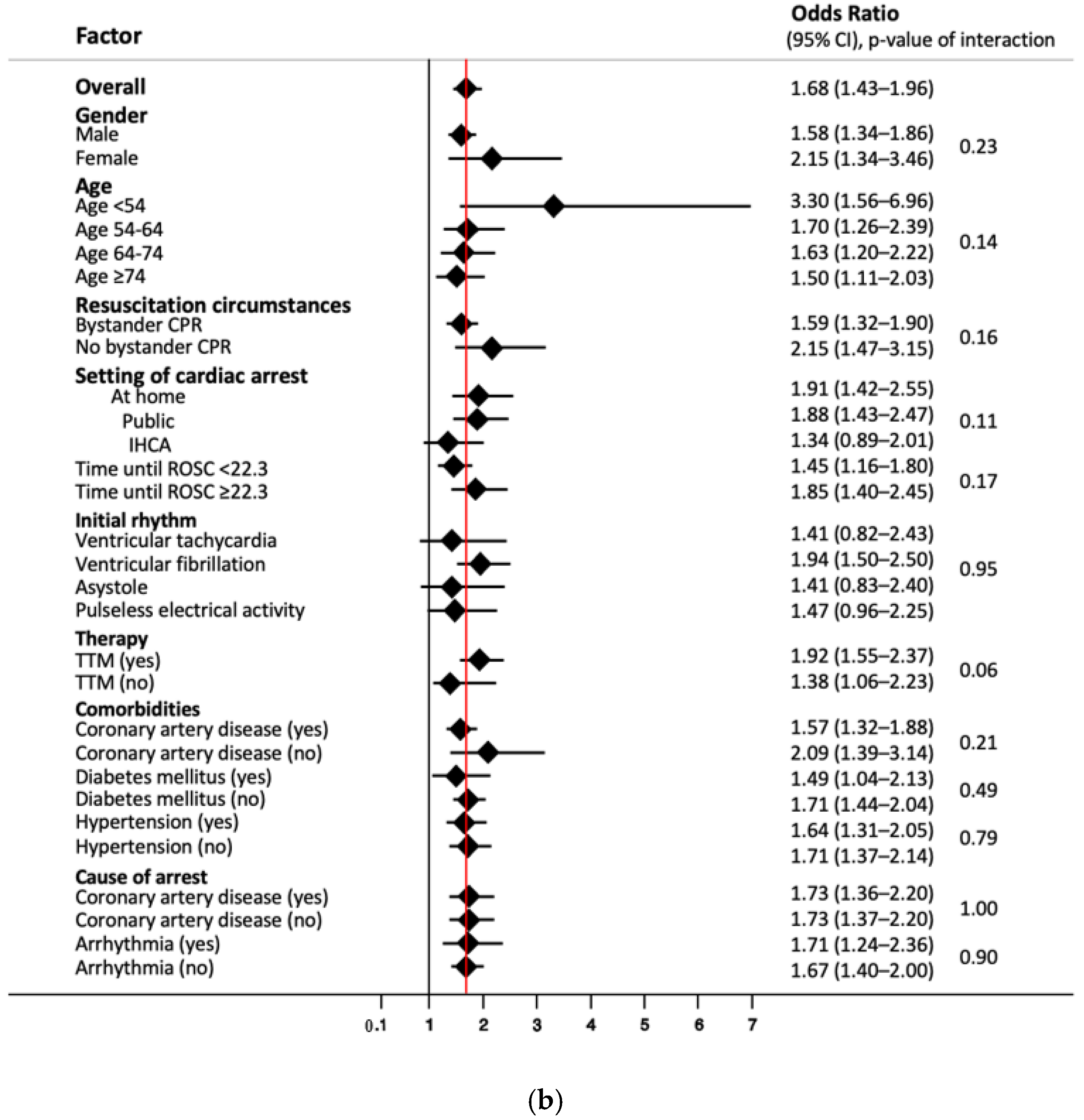
3.4. Subgroup Analyses
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Yan, S.; Gan, Y.; Jiang, N.; Wang, R.; Chen, Y.; Luo, Z.; Zong, Q.; Chen, S.; Lv, C. The global survival rate among adult out-of-hospital cardiac arrest patients who received cardiopulmonary resuscitation: A systematic review and meta-analysis. Crit. Care 2020, 24, 61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rey, J.R.; Caro-Codon, J.; Rodriguez Sotelo, L.; Lopez-de-Sa, E.; Rosillo, S.O.; Gonzalez Fernandez, O.; Fernandez de Bobadilla, J.; Iniesta, A.M.; Pena Conde, L.; Antorrena Miranda, I.; et al. Long term clinical outcomes in survivors after out-of-hospital cardiac arrest. Eur. J. Intern. Med. 2020, 74, 49–54. [Google Scholar] [CrossRef]
- Bernard, S.A.; Gray, T.W.; Buist, M.D.; Jones, B.M.; Silvester, W.; Gutteridge, G.; Smith, K. Treatment of comatose survivors of out-of-hospital cardiac arrest with induced hypothermia. N. Engl. J. Med. 2002, 346, 557–563. [Google Scholar] [CrossRef] [PubMed]
- Sandroni, C.; D’Arrigo, S.; Cacciola, S.; Hoedemaekers, C.W.E.; Kamps, M.J.A.; Oddo, M.; Taccone, F.S.; Di Rocco, A.; Meijer, F.J.A.; Westhall, E.; et al. Prediction of poor neurological outcome in comatose survivors of cardiac arrest: A systematic review. Intensive Care Med. 2020, 46, 1803–1851. [Google Scholar] [CrossRef] [PubMed]
- Isenschmid, C.; Luescher, T.; Rasiah, R.; Kalt, J.; Tondorf, T.; Gamp, M.; Becker, C.; Tisljar, K.; Sutter, R.; Schuetz, P.; et al. Performance of clinical risk scores to predict mortality and neurological outcome in cardiac arrest patients. Resuscitation 2019, 136, 21–29. [Google Scholar] [CrossRef]
- Andrew, E.; Nehme, Z.; Wolfe, R.; Bernard, S.; Smith, K. Long-term survival following out-of-hospital cardiac arrest. Heart 2017, 103, 1104–1110. [Google Scholar] [CrossRef]
- Andrew, E.; Nehme, Z.; Bernard, S.; Smith, K. The influence of comorbidity on survival and long-term outcomes after out-of-hospital cardiac arrest. Resuscitation 2017, 110, 42–47. [Google Scholar] [CrossRef]
- Gräsner, J.T.; Herlitz, J.; Tjelmeland, I.B.M.; Wnent, J.; Masterson, S.; Lilja, G.; Bein, B.; Böttiger, B.W.; Rosell-Ortiz, F.; Nolan, J.P.; et al. European Resuscitation Council Guidelines 2021: Epidemiology of cardiac arrest in Europe. Resuscitation 2021, 161, 61–79. [Google Scholar] [CrossRef]
- Brønnick, K.; Evald, L.; Duez, C.H.V.; Grejs, A.M.; Jeppesen, A.N.; Kirkegaard, H.; Nielsen, J.F.; Søreide, E. Biomarker prognostication of cognitive impairment may be feasible even in out-of hospital cardical arrest survivors with good neurological outcome. Resuscitation 2021, 162, 396–402. [Google Scholar] [CrossRef]
- Nolan, J.P.; Sandroni, C.; Bottiger, B.W.; Cariou, A.; Cronberg, T.; Friberg, H.; Genbrugge, C.; Haywood, K.; Lilja, G.; Moulaert, V.R.M.; et al. European Resuscitation Council and European Society of Intensive Care Medicine guidelines 2021: Post-resuscitation care. Intensive Care Med. 2021, 47, 369–421. [Google Scholar] [CrossRef]
- Callaway, C.W.; Donnino, M.W.; Fink, E.L.; Geocadin, R.G.; Golan, E.; Kern, K.B.; Leary, M.; Meurer, W.J.; Peberdy, M.A.; Thompson, T.M.; et al. Part 8: Post-Cardiac Arrest Care: 2015 American Heart Association Guidelines Update for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation 2015, 132, S465–S482. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schmechel, D.; Marangos, P.J.; Brightman, M. Neurone-specific enolase is a molecular marker for peripheral and central neuroendocrine cells. Nature 1978, 276, 834–836. [Google Scholar] [CrossRef] [PubMed]
- Gul, S.S.; Huesgen, K.W.; Wang, K.K.; Mark, K.; Tyndall, J.A. Prognostic utility of neuroinjury biomarkers in post out-of-hospital cardiac arrest (OHCA) patient management. Med. Hypotheses 2017, 105, 34–47. [Google Scholar] [CrossRef] [PubMed]
- Johnsson, P.; Blomquist, S.; Lührs, C.; Malmkvist, G.; Alling, C.; Solem, J.O.; Ståhl, E. Neuron-specific enolase increases in plasma during and immediately after extracorporeal circulation. Ann. Thorac. Surg. 2000, 69, 750–754. [Google Scholar] [CrossRef]
- Wang, C.H.; Chang, W.T.; Su, K.I.; Huang, C.H.; Tsai, M.S.; Chou, E.; Lu, T.C.; Chen, W.J.; Lee, C.C.; Chen, S.C. Neuroprognostic accuracy of blood biomarkers for post-cardiac arrest patients: A systematic review and meta-analysis. Resuscitation 2020, 148, 108–117. [Google Scholar] [CrossRef]
- Stevens, R.D.; Sutter, R. Prognosis in severe brain injury. Crit. Care Med. 2013, 41, 1104–1123. [Google Scholar] [CrossRef]
- Stammet, P.; Collignon, O.; Hassager, C.; Wise, M.P.; Hovdenes, J.; Aneman, A.; Horn, J.; Devaux, Y.; Erlinge, D.; Kjaergaard, J.; et al. Neuron-Specific Enolase as a Predictor of Death or Poor Neurological Outcome After Out-of-Hospital Cardiac Arrest and Targeted Temperature Management at 33 degrees C and 36 degrees C. J. Am. Coll. Cardiol. 2015, 65, 2104–2114. [Google Scholar] [CrossRef]
- Vondrakova, D.; Kruger, A.; Janotka, M.; Malek, F.; Dudkova, V.; Neuzil, P.; Ostadal, P. Association of neuron-specific enolase values with outcomes in cardiac arrest survivors is dependent on the time of sample collection. Crit. Care 2017, 21, 172. [Google Scholar] [CrossRef] [Green Version]
- Storm, C.; Krannich, A.; Schachtner, T.; Engels, M.; Schindler, R.; Kahl, A.; Otto, N.M. Impact of acute kidney injury on neurological outcome and long-term survival after cardiac arrest—A10 year observational follow up. J. Crit. Care 2018, 47, 254–259. [Google Scholar] [CrossRef]
- Wihersaari, L.; Tiainen, M.; Skrifvars, M.B.; Bendel, S.; Kaukonen, K.M.; Vaahersalo, J.; Romppanen, J.; Pettilä, V.; Reinikainen, M. Usefulness of neuron specific enolase in prognostication after cardiac arrest: Impact of age and time to ROSC. Resuscitation 2019, 139, 214–221. [Google Scholar] [CrossRef]
- Floerchinger, B.; Philipp, A.; Camboni, D.; Foltan, M.; Lunz, D.; Lubnow, M.; Zausig, Y.; Schmid, C. NSE serum levels in extracorporeal life support patients-Relevance for neurological outcome? Resuscitation 2017, 121, 166–171. [Google Scholar] [CrossRef] [PubMed]
- Petzinka, V.N.; Endisch, C.; Streitberger, K.J.; Salih, F.; Ploner, C.J.; Storm, C.; Nee, J.; Leithner, C. Unresponsive wakefulness or coma after cardiac arrest-A long-term follow-up study. Resuscitation 2018, 131, 121–127. [Google Scholar] [CrossRef] [PubMed]
- Luescher, T.; Mueller, J.; Isenschmid, C.; Kalt, J.; Rasiah, R.; Tondorf, T.; Gamp, M.; Becker, C.; Sutter, R.; Tisljar, K.; et al. Neuron-specific enolase (NSE) improves clinical risk scores for prediction of neurological outcome and death in cardiac arrest patients: Results from a prospective trial. Resuscitation 2019, 142, 50–60. [Google Scholar] [CrossRef]
- Metzger, K.; Gamp, M.; Tondorf, T.; Hochstrasser, S.; Becker, C.; Luescher, T.; Rasiah, R.; Boerlin, A.; Tisljar, K.; Emsden, C.; et al. Depression and anxiety in relatives of out-of-hospital cardiac arrest patients: Results of a prospective observational study. J. Crit. Care 2019, 51, 57–63. [Google Scholar] [CrossRef] [PubMed]
- Hypothermia after Cardiac Arrest Study Group. Mild therapeutic hypothermia to improve the neurologic outcome after cardiac arrest. N. Engl. J. Med. 2002, 346, 549–556. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, N.; Wetterslev, J.; Cronberg, T.; Erlinge, D.; Gasche, Y.; Hassager, C.; Horn, J.; Hovdenes, J.; Kjaergaard, J.; Kuiper, M.; et al. Targeted temperature management at 33 degrees C versus 36 degrees C after cardiac arrest. N. Engl. J. Med. 2013, 369, 2197–2206. [Google Scholar] [CrossRef] [Green Version]
- Sterner, R. 2008 American Society of Naturalists Awards: E. O. Wilson Award—Ulrich G. Mueller. Am. Nat. 2009, 173, iv. [Google Scholar] [CrossRef]
- Jennett, B.; Bond, M. Assessment of outcome after severe brain damage. Lancet 1975, 1, 480–484. [Google Scholar] [CrossRef]
- Mak, M.; Moulaert, V.R.; Pijls, R.W.; Verbunt, J.A. Measuring outcome after cardiac arrest: Construct validity of Cerebral Performance Category. Resuscitation 2016, 100, 6–10. [Google Scholar] [CrossRef]
- Wijdicks, E.F.; Hijdra, A.; Young, G.B.; Bassetti, C.L.; Wiebe, S.; Quality Standards Subcommittee of the American Academy of Neurology. Practice parameter: Prediction of outcome in comatose survivors after cardiopulmonary resuscitation (an evidence-based review): Report of the Quality Standards Subcommittee of the American Academy of Neurology. Neurology 2006, 67, 203–210. [Google Scholar] [CrossRef]
- Streitberger, K.J.; Leithner, C.; Wattenberg, M.; Tonner, P.H.; Hasslacher, J.; Joannidis, M.; Pellis, T.; Di Luca, E.; Fodisch, M.; Krannich, A.; et al. Neuron-Specific Enolase Predicts Poor Outcome After Cardiac Arrest and Targeted Temperature Management: A Multicenter Study on 1,053 Patients. Crit. Care Med. 2017, 45, 1145–1151. [Google Scholar] [CrossRef] [PubMed]
- Rey, A.; Rossetti, A.O.; Miroz, J.P.; Eckert, P.; Oddo, M. Late Awakening in Survivors of Postanoxic Coma: Early Neurophysiologic Predictors and Association With ICU and Long-Term Neurologic Recovery. Crit. Care Med. 2019, 47, 85–92. [Google Scholar] [CrossRef]
- Sandroni, C.; Cariou, A.; Cavallaro, F.; Cronberg, T.; Friberg, H.; Hoedemaekers, C.; Horn, J.; Nolan, J.P.; Rossetti, A.O.; Soar, J. Prognostication in comatose survivors of cardiac arrest: An advisory statement from the European Resuscitation Council and the European Society of Intensive Care Medicine. Resuscitation 2014, 85, 1779–1789. [Google Scholar] [CrossRef]
- Zandbergen, E.G.; Hijdra, A.; Koelman, J.H.; Hart, A.A.; Vos, P.E.; Verbeek, M.M.; de Haan, R.J. Prediction of poor outcome within the first 3 days of postanoxic coma. Neurology 2006, 66, 62–68. [Google Scholar] [CrossRef] [PubMed]
- Roedl, K.; Jarczak, D.; Becker, S.; Fuhrmann, V.; Kluge, S.; Muller, J. Long-term neurological outcomes in patients aged over 90 years who are admitted to the intensive care unit following cardiac arrest. Resuscitation 2018, 132, 6–12. [Google Scholar] [CrossRef] [PubMed]
- Cour, M.; Turc, J.; Madelaine, T.; Argaud, L. Risk factors for progression toward brain death after out-of-hospital cardiac arrest. Ann. Intensive Care 2019, 9, 45. [Google Scholar] [CrossRef]
- Witten, L.; Gardner, R.; Holmberg, M.J.; Wiberg, S.; Moskowitz, A.; Mehta, S.; Grossestreuer, A.V.; Yankama, T.; Donnino, M.W.; Berg, K.M. Reasons for death in patients successfully resuscitated from out-of-hospital and in-hospital cardiac arrest. Resuscitation 2019, 136, 93–99. [Google Scholar] [CrossRef]
- Hsu, J.W.; Madsen, C.D.; Callaham, M.L. Quality-of-life and formal functional testing of survivors of out-of-hospital cardiac arrest correlates poorly with traditional neurologic outcome scales. Ann. Emerg. Med. 1996, 28, 597–605. [Google Scholar] [CrossRef]
- Rittenberger, J.C.; Raina, K.; Holm, M.B.; Kim, Y.J.; Callaway, C.W. Association between Cerebral Performance Category, Modified Rankin Scale, and discharge disposition after cardiac arrest. Resuscitation 2011, 82, 1036–1040. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Factor | All Patients | Survivor | Non-Survivor | p-Value |
|---|---|---|---|---|
| Number (% of total) | 403 (100) | 176 (43.7) | 227 (56.3) | |
| Sociodemographics | ||||
| Age, years, mean (SD) | 64.1 (14.6) | 59.7 (14.4) | 67.6 (13.8) | <0.001 |
| Male gender, n (%) | 284 (70.5) | 138 (78.4) | 146 (64.3) | 0.002 |
| Comorbidities (n, %) | ||||
| Coronary artery disease | 260 (64.8) | 129 (73.7) | 131 (58.0) | 0.001 |
| Congestive heart failure | 56 (14.0) | 16 (9.1) | 40 (17.7) | 0.014 |
| COPD | 34 (8.5) | 4 (2.3) | 30 (13.3) | <0.001 |
| Hypertension | 203 (50.6) | 85 (48.6) | 118 (52.2) | 0.47 |
| Diabetes mellitus | 86 (21.4) | 28 (16.0) | 58 (25.7) | 0.019 |
| Chronic kidney disease | 54 (13.5) | 13 (7.4) | 41 (18.1) | 0.002 |
| Malignant disease | 44 (11.0) | 9 (5.1) | 35 (15.5) | 0.001 |
| Neurological disease | 47 (11.7) | 14 (8.0) | 33 (14.6) | 0.042 |
| Resuscitation measures | ||||
| Time until ROSC, mean (SD) | 22.3 (16.7) | 17.3 (15.3) | 26.4 (16.7) | <0.001 |
| Observed cardiac arrest, n (%) | 330 (82.3) | 162 (92.0) | 168 (74.7) | <0.001 |
| Bystander CPR, n (%) | 264 (65.7) | 140 (79.5) | 124 (54.9) | <0.001 |
| Setting of cardiac arrest (n, %) | ||||
| At home | 151 (38.7) | 44 (26.2) | 107 (48.2) | <0.001 |
| Public | 177 (45.4) | 97 (57.7) | 80 (36.0) | |
| IHCA | 62 (15.9) | 27 (16.1) | 35 (15.8) | |
| Initial rhythm (n, %) | ||||
| Ventricular tachycardia | 19 (4.7) | 9 (5.1) | 10 (4.4) | <0.001 |
| Ventricular fibrillation | 206 (51.2) | 123 (69.9) | 83 (36.7) | |
| Asystole | 62 (15.4) | 8 (4.5) | 54 (23.9) | |
| Pulseless electrical activity | 84 (20.9) | 16 (9.1) | 68 (30.1) | |
| Unknown | 31 (7.7) | 20 (11.4) | 11 (4.9) | |
| Diagnostic measures (mean, SD) | ||||
| Initial lactate (mmol/L) | 6.6 (4.3) | 5.1 (3.3) | 7.7 (4.6) | <0.001 |
| Initial pH | 7.2 (0.2) | 7.3 (0.1) | 7.2 (0.2) | 0.003 |
| Cause of cardiac arrest (n, %) | ||||
| Coronary artery disease | 199 (49.4) | 117 (66.5) | 82 (36.1) | <0.001 |
| Arrhythmia | 70 (17.4) | 26 (14.8) | 44 (19.4) | 0.23 |
| Respiratory | 67 (16.6) | 13 (7.4) | 54 (23.8) | <0.001 |
| Other/unknown | 67 (16.6) | 20 (11.4) | 47 (20.7) | 0.012 |
| (a) Primary Endpoint: Long-Term Mortality | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| N | All | Survivors | Non-Survivors | p-Value | Univariable HR (95%CI), p-Value | Multivariable * Adjusted HR (95%CI), p-Value | Multivariable ** Adjusted HR (95%CI), p-Value | ROC AUC (95% CI) | |
| n = 176 | n = 227 | ||||||||
| NSE max, median (IQR) | 403 | 43.8 (27.6, 108.6) | 29.7 (22.9, 45.7) | 75.7 (35.2, 197.7) | <0.001 | 1.29 (1.23, 1.36), p < 0.001 | 1.32 (1.25, 1.39), p < 0.001 | 1.24 (1.17, 1.31), p < 0.001 | 0.77 (0.73, 0.82) |
| NSE day 0, median (IQR) | 325 | 33.8 (24.3, 49.4) | 28.6 (21.5, 41.8) | 36.8 (27.6, 59.9) | <0.001 | 1.14 (1.08, 1.2), p < 0.001 | 1.16 (1.1, 1.23), p < 0.001 | 1.07 (1, 1.13), p = 0.038 | 0.64 (0.58, 0.70) |
| NSE day 1, median (IQR) | 346 | 33.4 (23.4, 63.9) | 26.9 (19.3, 37.3) | 50.1 (29.8, 105) | <0.001 | 1.27 (1.2, 1.34), p < 0.001 | 1.3 (1.22, 1.38), p < 0.001 | 1.24 (1.15, 1.32), p < 0.001 | 0.74 (0.69, 0.80) |
| NSE day 2, median (IQR) | 294 | 29.9 (19.5, 94.1) | 22.3 (17.4, 30.6) | 76.5 (29.8, 192) | <0.001 | 1.43 (1.33, 1.54), p < 0.001 | 1.47 (1.36, 1.6), p < 0.001 | 1.42 (1.31, 1.55), p < 0.001 | 0.8 (0.74, 0.85) |
| NSE day 3, median (IQR) | 225 | 27.8 (17.4, 95.6) | 19.8 (15.7, 27.8) | 72.6 (26, 194) | <0.001 | 1.5 (1.38, 1.64), p < 0.001 | 1.55 (1.41, 1.71), p < 0.001 | 1.51 (1.37, 1.66), p < 0.001 | 0.81 (0.75, 0.87) |
| (b) Secondary Endpoint: Neurological Outcome (CPC) after 2 Years | |||||||||
| N | All | Good Neurological Outcome (CPC 1–2) | Poor Neurological Outcome (CPC 3–5) | p-Value | Univariable OR (95%CI), p-Value | Multivariable * Adjusted OR (95%CI), p-Value | Multivariable ** Adjusted OR (95%CI), p-Value | ROC AUC (95%CI) | |
| n = 88 | n = 215 | ||||||||
| NSE max, median (IQR) | 303 | 55.9 (29.8, 148.9) | 29.8 (21.35, 46.5) | 80.1 (36.3, 204.8) | <0.001 | 1.45 (1.31, 1.61), p < 0.001 | 1.68 (1.45, 1.94), p < 0.001 | 1.41 (1.22, 1.62), p < 0.001 | 0.78 (0.73, 0.84) |
| NSE day 0, median (IQR) | 247 | 35.4 (24.6, 54.7) | 30.1 (21.1, 41.6) | 37.7 (28, 65.1) | <0.001 | 1.19 (1.08, 1.32), p = 0.001 | 1.33 (1.16, 1.51), p < 0.001 | 1.09 (0.95, 1.24), p = 0.223 | 0.65 (0.57, 0.73) |
| NSE day 1, median (IQR) | 256 | 38.4 (25.8, 76.1) | 26.9 (16.7, 36.7) | 53.9 (29.9, 109) | <0.001 | 1.41 (1.27, 1.57), p < 0.001 | 1.58 (1.37, 1.82), p < 0.001 | 1.35 (1.17, 1.55), p < 0.001 | 0.76 (0.70, 0.82) |
| NSE day 2, median (IQR) | 208 | 35.5 (22.1, 137) | 22.7 (17.3, 30.5) | 87.8 (30.4, 212) | <0.001 | 1.52 (1.34, 1.73), p < 0.001 | 1.69 (1.42, 2.01), p < 0.001 | 1.53 (1.29, 1.81), p < 0.001 | 0.81 (0.75, 0.87) |
| NSE day 3, median (IQR) | 167 | 38.5 (19.7, 134) | 19.5 (14.5, 26.2) | 87.1 (33.2, 200) | <0.001 | 1.68 (1.43, 1.96), p < 0.001 | 1.81 (1.49, 2.2), p < 0.001 | 1.67 (1.37, 2.03), p < 0.001 | 0.85 (0.79, 0.91) |
| Max. NSE | Survivors below Cut-off (n) | Survivors above Cut-off (n) | Non-Survivors below Cut-off (n) | Non-Survivors above Cut-off (n) | Sensitivity Pr(+A), % (95%CI) | Specificity Pr(-N), % (95%CI) | ROC Area, (95%CI) | Likelihood Ratio (+), (95%CI) | Likelihood Ratio (−), (95%CI) | Hazard Ratio (95%CI) | PPV, % (95%CI) | NPV, % (95%CI) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 33 ng/mL | 100 | 76 | 48 | 179 | 78.9 (51.3–61.2) | 56.8 (73.0–84.0) | 0.68 (0.63–0.72) | 1.83 (1.52–2.19) | 0.37 (0.28–0.49) | 4.91 (3.17–7.58) | 70.2 (64.2–75.7) | 67.6 (59.4–75.0) |
| 45.9 ng/mL | 133 | 43 | 77 | 150 | 66.1 (59.5–72.2) | 75.6 (68.5–81.7) | 0.71 (0.66–0.75) | 2.70 (2.05–3.56) | 0.45 (0.37–0.55) | 6.03 (3.88–9.35) | 77.7 (71.2–83.4) | 63.3 (56.4–69.9) |
| Day 0 NSE | ||||||||||||
| 33 ng/mL | 85 | 51 | 76 | 113 | 59.8 (52.4–66.8) | 62.5 (53.8–70.6) | 0.61 (0.56–0.67) | 1.59 (1.25–2.04) | 0.64 (0.52–0.80) | 2.48 (1.58–3.89) | 68.9 (61.2–75.9) | 52.8 (44.8–60.7) |
| 32.9 ng/mL | 85 | 51 | 74 | 115 | 60.8 (53.5–67.8) | 62.5 (53.8–70.6) | 0.62 (0.56–0.67) | 1.62 (1.27–2.07) | 0.63 (0.50–0.67) | 2.59 (1.65–4.07) | 69.3 (61.7–76.2) | 53.5 (45.4–61.4) |
| Day 1 NSE | ||||||||||||
| 33 ng/mL | 110 | 49 | 62 | 125 | 66.8 (59.6–73.5) | 69.2 (61.4–76.3) | 0.68 (0.63–0.73) | 2.17 (1.68–2.80) | 0.48 (0.38–0.60) | 4.53 (2.88–7.12) | 71.8 (64.5–78.4) | 64.0 (56.3–71.1) |
| 31.1 ng/mL | 105 | 54 | 53 | 134 | 71.7 (64.6–78.0) | 66.0 (58.1–73.4) | 0.69 (0.64–0.74) | 2.11 (1.67–2.67) | 0.43 (0.33–0.55) | 4.92 (3.12–7.76) | 71.3 (64.2–77.6) | 66.5 (58.5–73.8) |
| Day 2 NSE | ||||||||||||
| 33 ng/mL | 121 | 28 | 46 | 99 | 68.3 (60.0–75.7) | 81.2 (74.0–87.1) | 0.75 (0.70–0.80) | 3.63 (2.56–5.16) | 0.39 (0.30–0.50) | 9.30 (5.43–15.92) | 78.0 (69.7–84.8) | 72.5 (65.0–79.1) |
| 29.5 ng/mL | 110 | 39 | 36 | 109 | 75.2 (67.3–82.0) | 73.8 (66.0–80.7) | 0.74 (0.70–0.79) | 2.87 (2.16–3.82) | 0.34 (0.25–0.45) | 8.54 (5.06–14.41) | 73.6 (65.8–80.5) | 75.3 (67.5–82.1) |
| Day 3 NSE | ||||||||||||
| 33 ng/mL | 89 | 22 | 34 | 80 | 70.2 (60.9–78.4) | 80.2 (71.5–87.1) | 0.75 (0.70–0.81) | 3.54 (2.39–5.24) | 0.37 (0.28–0.50) | 9.52 (5.16–17.56) | 78.4 (69.2–86.0) | 72.4 (63.6–80.0) |
| 35.9 ng/mL | 94 | 17 | 36 | 78 | 68.4 (59.1–76.8) | 84.7 (76.6–90.8) | 0.77 (0.71–0.82) | 4.47 (2.83–7.04) | 0.37 (0.28–0.49) | 11.98 (6.28–22.85) | 82.1 (72.9–89.2) | 72.3 (63.8–79.8) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Müller, J.; Bissmann, B.; Becker, C.; Beck, K.; Loretz, N.; Gross, S.; Amacher, S.A.; Bohren, C.; Pargger, H.; Tisljar, K.; et al. Neuron-Specific Enolase (NSE) Predicts Long-Term Mortality in Adult Patients after Cardiac Arrest: Results from a Prospective Trial. Medicines 2021, 8, 72. https://0-doi-org.brum.beds.ac.uk/10.3390/medicines8110072
Müller J, Bissmann B, Becker C, Beck K, Loretz N, Gross S, Amacher SA, Bohren C, Pargger H, Tisljar K, et al. Neuron-Specific Enolase (NSE) Predicts Long-Term Mortality in Adult Patients after Cardiac Arrest: Results from a Prospective Trial. Medicines. 2021; 8(11):72. https://0-doi-org.brum.beds.ac.uk/10.3390/medicines8110072
Chicago/Turabian StyleMüller, Jonas, Benjamin Bissmann, Christoph Becker, Katharina Beck, Nina Loretz, Sebastian Gross, Simon A. Amacher, Chantal Bohren, Hans Pargger, Kai Tisljar, and et al. 2021. "Neuron-Specific Enolase (NSE) Predicts Long-Term Mortality in Adult Patients after Cardiac Arrest: Results from a Prospective Trial" Medicines 8, no. 11: 72. https://0-doi-org.brum.beds.ac.uk/10.3390/medicines8110072