Effects of Lasers and Their Delivery Characteristics on Machined and Micro-Roughened Titanium Dental Implant Surfaces



Abstract
:1. Introduction
2. Materials and Methods
2.1. Lasers and Optical Fibres
2.2. Titanium Discs
2.3. Experimental Setup
2.4. Experimental Groups
2.5. Emission Measurements
2.6. Surface Profilometry
2.7. Analysis of Results
3. Results
3.1. Surface Roughness
3.1.1. Control Group
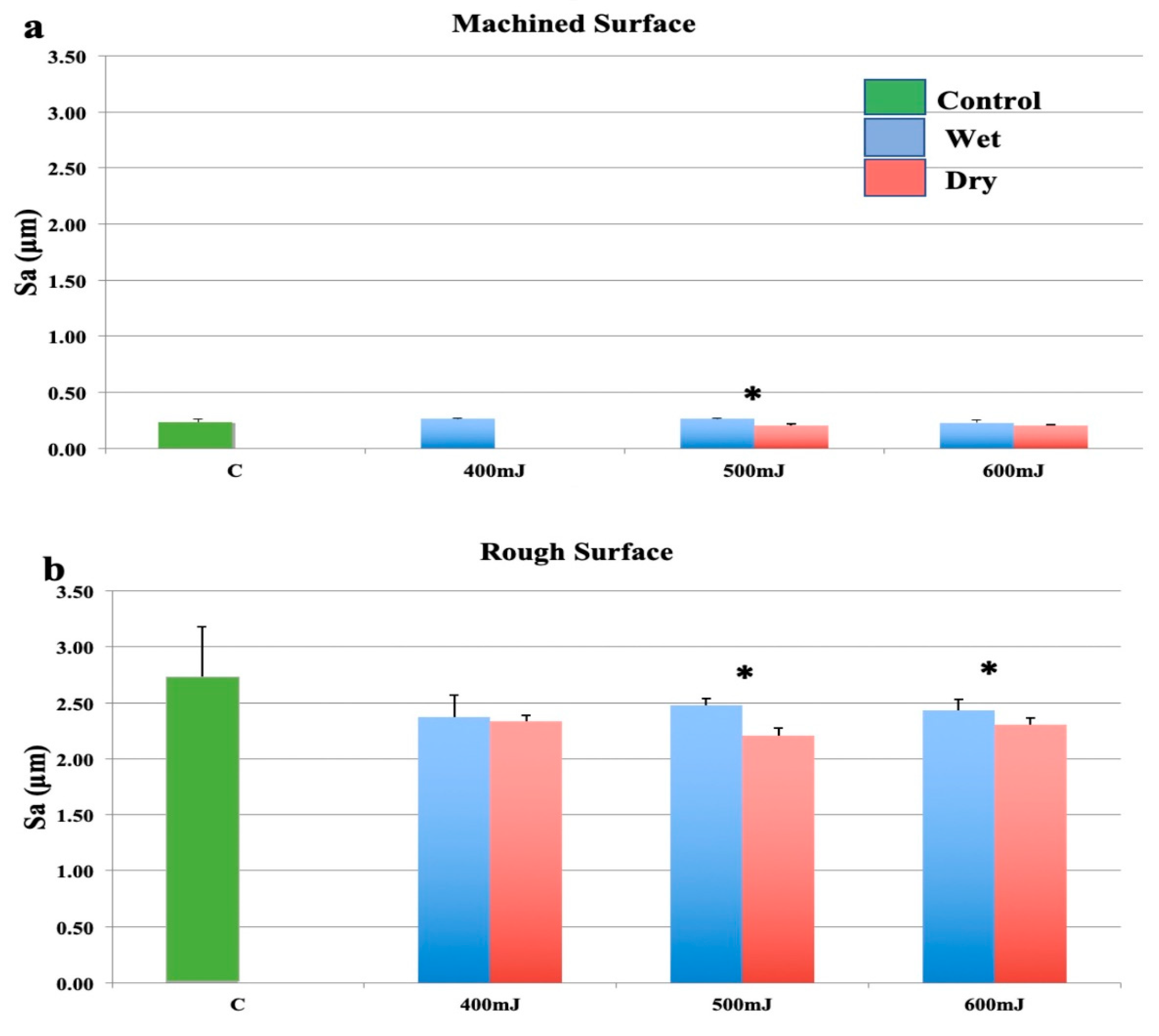
3.1.2. Group 1—Er:YAG Laser with Focusing Handpiece
3.1.3. Group 2—Er:YAG Laser with an Optical Fibre
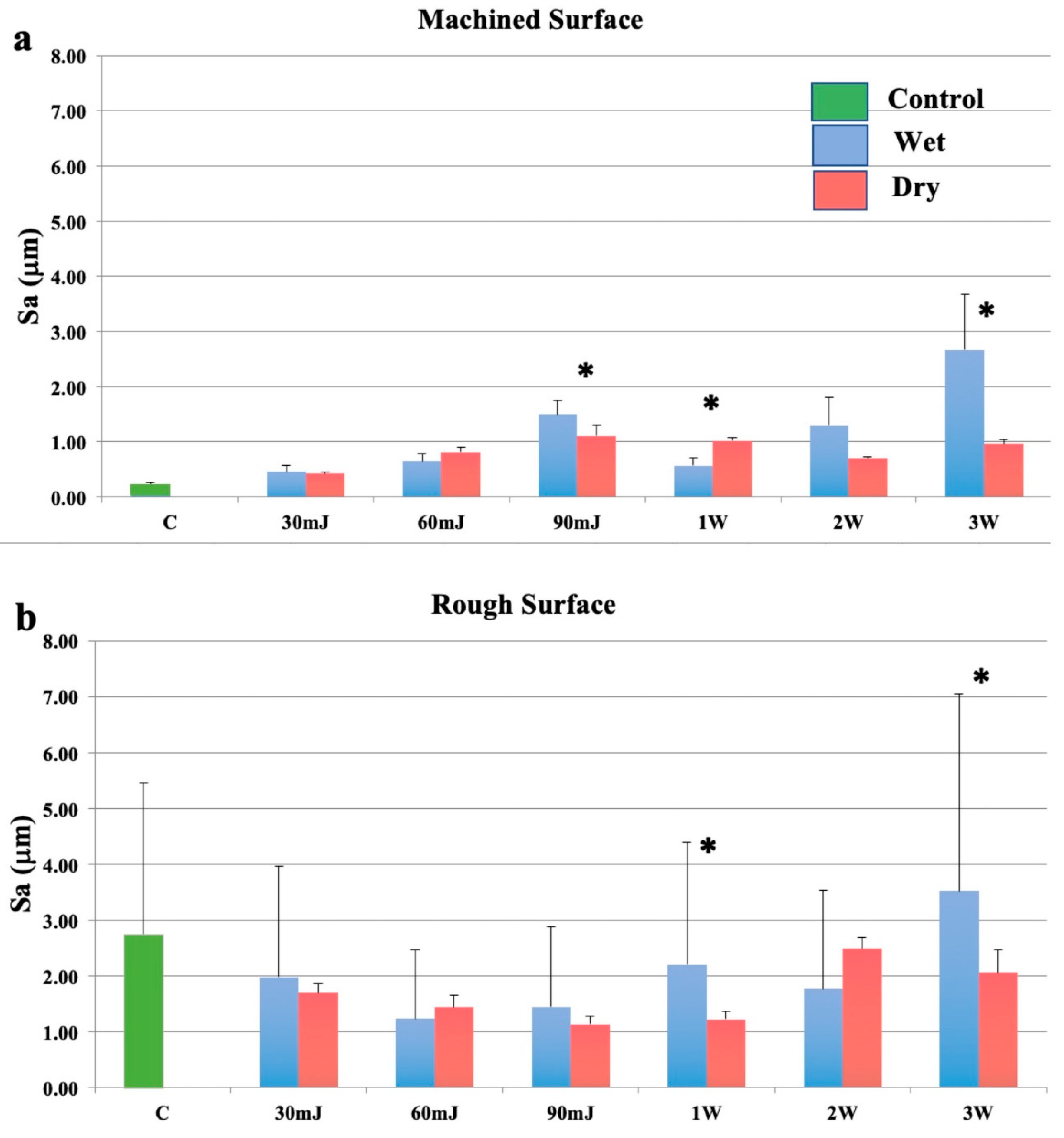
3.1.4. Group 3—Nd:YAG Laser with an Optical Fibre
3.2. Volume of Peaks in the Ablation Zone
3.2.1. Group 1—Er:YAG Laser with Focusing Handpiece
3.2.2. Group 2—Er:YAG Laser with Optical Fibre
3.2.3. Group 3—Nd:YAG Laser with Optical Fibre
3.3. Maximum Diameter of the Zone of Ablation
3.3.1. Group 1—Er:YAG Laser with Focusing Handpiece
3.3.2. Group 2—Er:YAG Laser with Optical Fibre
3.3.3. Group 3—Nd:YAG with Optical Fibre
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Schou, S.; Holmstrup, P.; Skovgaard, L.T.; Stoltze, K.; Hjorting-Hansen, E.; Wenzel, A.; Jørgensen, T. Implant surface preparation in the surgical treatment of experimental peri-implantitis with autogenous bone graft and ePTFE membrane in cynomolgus monkeys. Clin. Oral Implant. Res. 2003, 14, 412–422. [Google Scholar] [CrossRef] [PubMed]
- Schou, S.; Berglundh, T.; Lang, N.P. Surgical treatment of peri-implantitis. Int. J. Oral Maxillofac. Implant. 2004, 19, 140–149. [Google Scholar]
- Schwarz, F.; Sahm, N.; Iglhaut, G.; Becker, J. Impact of the method of surface debridement and decontamination on the clinical outcome following combined surgical therapy of peri-implantitis: A randomized controlled clinical study. J. Clin. Periodontol. 2011, 38, 276–284. [Google Scholar] [CrossRef] [PubMed]
- Karring, E.S.; Stavropoulos, A.; Ellegaard, B.; Karring, T. Treatment of peri-implantitis by the Vector system. Clin. Oral Implants Res. 2005, 16, 288–293. [Google Scholar] [CrossRef] [PubMed]
- Renvert, S.; Samuelsson, E.; Lindahl, C.; Persson, G.R. Mechanical non-surgical treatment of peri-implantitis: A double-blind randomized longitudinal clinical study. I: Clinical results. J. Clin. Periodontol. 2009, 36, 604–609. [Google Scholar] [CrossRef]
- Meyle, J. Mechanical, chemical and laser treatments of the implant surface in the presence of marginal bone loss around implants. Eur. J. Oral Implant. 2012, 5, 71–81. [Google Scholar]
- Del Amo, F.S.-L.; Yu, S.-H.; Wang, H.-L. Non-Surgical Therapy for Peri-Implant Diseases: A Systematic Review. J. Oral Maxillofac. Res. 2016, 7. [Google Scholar] [CrossRef]
- Deppe, H.; Horch, H.H. Laser applications in oral surgery and implant dentistry. Lasers Med. Sci. 2007, 22, 217–221. [Google Scholar] [CrossRef] [PubMed]
- Ruiz, R.A.D.; Romanos, G.E. Potential Causes of Titanium Particle and Ion Release in Implant Dentistry: A Systematic Review. Int. J. Mol. Sci. 2018, 19, 3585. [Google Scholar] [CrossRef] [Green Version]
- Ishikawa, I.; Aoki, A.; Takasaki, A.A. Clinical application of erbium:YAG laser in periodontology. J. Int. Acad. Periodontol. 2008, 10, 22–30. [Google Scholar]
- Miyazaki, A.; Yamaguchi, T.; Nishikata, J.; Okuda, K.; Suda, S.; Orima, K.; Kobayashi, T.; Yamazaki, K.; Yoshikawa, E.; Yoshie, H. Effects of Nd:YAG and CO2Laser Treatment and Ultrasonic Scaling on Periodontal Pockets of Chronic Periodontitis Patients. J. Periodontol. 2003, 74, 175–180. [Google Scholar] [CrossRef] [PubMed]
- Tomasi, C.; Schander, K.; Dahlén, G.; Wennström, J.L. Short-Term Clinical and Microbiologic Effects of Pocket Debridement With an Er:YAG Laser During Periodontal Maintenance. J. Periodontol. 2006, 77, 111–118. [Google Scholar] [CrossRef] [Green Version]
- Grzech-Leśniak, K.; Sculean, A.; Gašpirc, B. Laser reduction of specific microorganisms in the periodontal pocket using Er:YAG and Nd:YAG lasers: A randomized controlled clinical study. Lasers Med Sci. 2018, 33, 1461–1470. [Google Scholar] [CrossRef] [PubMed]
- Kelbauskiene, S.; Maciulskiene, V. A pilot study of Er,Cr:YSGG laser therapy used as an adjunct to scaling and root planing in patients with early and moderate periodontitis. Stomatologija 2007, 9, 21–26. [Google Scholar] [PubMed]
- Ting, C.-C.; Fukuda, M.; Watanabe, T.; Aoki, T.; Sanaoka, A.; Noguchi, T. Effects of Er,Cr:YSGG Laser Irradiation on the Root Surface: Morphologic Analysis and Efficiency of Calculus Removal. J. Periodontol. 2007, 78, 2156–2164. [Google Scholar] [CrossRef]
- Crespi, R.; Barone, A.; Covani, U. Histologic Evaluation of Three Methods of Periodontal Root Surface Treatment in Humans. J. Periodontol. 2005, 76, 476–481. [Google Scholar] [CrossRef] [Green Version]
- Kreisler, M.; Al Haj, H.; D’Hoedt, B. Clinical efficacy of semiconductor laser application as an adjunct to conventional scaling and root planing. Lasers Surg. Med. 2005, 37, 350–355. [Google Scholar] [CrossRef]
- Moritz, A.; Schoop, U.; Goharkhay, K.; Schauer, P.; Doertbudak, O.; Wernisch, J.; Sperr, W. Treatment of periodontal pockets with a diode laser. Lasers Surg. Med. 1998, 22, 302–311. [Google Scholar] [CrossRef]
- Schwarz, F.; Aoki, A.; Becker, J.; Sculean, A. Laser application in non-surgical periodontal therapy: A systematic review. J. Clin. Periodontol. 2008, 35, 29–44. [Google Scholar] [CrossRef]
- Ishikawa, I.; Aoki, A.; Takasaki, A.A. Potential applications of Erbium:YAG laser in periodontics. J. Periodontal Res. 2004, 39, 275–285. [Google Scholar] [CrossRef]
- Kreisler, M.; Kohnen, W.; Marinello, C.; Götz, H.; Duschner, H.; Jansen, B.; D’Hoedt, B. Bactericidal Effect of the Er:YAG Laser on Dental Implant Surfaces: An In Vitro Study. J. Periodontol. 2002, 73, 1292–1298. [Google Scholar] [CrossRef] [PubMed]
- Taniguchi, Y.; Aoki, A.; Mizutani, K.; Takeuchi, Y.; Ichinose, S.; Takasaki, A.A.; Schwarz, F.; Izumi, Y. Optimal Er:YAG laser irradiation parameters for debridement of microstructured fixture surfaces of titanium dental implants. Lasers Med. Sci. 2013, 28, 1057–1068. [Google Scholar] [CrossRef] [PubMed]
- Takagi, T.; Aoki, A.; Ichinose, S.; Taniguchi, Y.; Tachikawa, N.; Shinoki, T.; Meinzer, W.; Sculean, A.; Izumi, Y. Effective removal of calcified deposits on microstructured titanium fixture surfaces of dental implants with erbium lasers. J. Periodontol. 2018, 89, 680–690. [Google Scholar] [CrossRef] [PubMed]
- Shin, S.-I.; Min, H.-K.; Park, B.-H.; Kwon, Y.-H.; Park, J.-B.; Herr, Y.; Heo, S.-J.; Chung, J.-H. The effect of Er:YAG laser irradiation on the scanning electron microscopic structure and surface roughness of various implant surfaces: An in vitro study. Lasers Med Sci. 2010, 26, 767–776. [Google Scholar] [CrossRef]
- Kim, S.-W.; Kwon, Y.-H.; Chung, J.-H.; Shin, S.-I.; Herr, Y. The effect of Er:YAG laser irradiation on the surface microstructure and roughness of hydroxyapatite-coated implant. J. Periodontal Implant. Sci. 2010, 40, 276–282. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.-H.; Kwon, Y.-H.; Herr, Y.; Shin, S.-I.; Chung, J.-H. Effect of erbium-doped: Yttrium, aluminium and garnet laser irradiation on the surface microstructure and roughness of sand-blasted, large grit, acid-etched implants. J. Periodontal Implant. Sci. 2011, 41, 135–142. [Google Scholar] [CrossRef] [Green Version]
- Park, J.-H.; Heo, S.-J.; Koak, J.-Y.; Kim, S.-K.; Han, C.-H.; Lee, J.-H. Effects of laser irradiation on machined and anodized titanium disks. Int. J. Oral Maxillofac. Implant. 2012, 27, 265–272. [Google Scholar]
- Galli, C.; Macaluso, G.M.; Elezi, E.; Ravanetti, F.; Cacchioli, A.; Gualini, G.; Passeri, G. The effects of Er:YAG laser tretatment on titanium surface profile and osteoblastic cell activity: An in vitro study. J. Periodontol. 2011, 82, 1169–1177. [Google Scholar] [CrossRef]
- Verdaasdonk, R.M.; Van Swol, C.F.P. Laser light delivery systems for medical applications. Phys. Med. Biol. 1997, 42, 869–894. [Google Scholar] [CrossRef]
- Mir, M.; Meister, J.; Franzen, R.; Sabounchi, S.S.; Lampert, F.; Gutknecht, N. Influence of water-layer thickness on Er:YAG laser ablation of enamel of bovine anterior teeth. Lasers Med Sci. 2007, 23, 451–457. [Google Scholar] [CrossRef]
- Apel, C.; Gutknecht, N. Influence of the spatial beam profile on hard tissue ablation, Part II: Pulse energy and energy density distribution in simple beams. Lasers Med. Sci. 2004, 19, 112–118. [Google Scholar] [CrossRef]
- Stopp, S.; Svejdar, D.; Deppe, H.; Lueth, T.C. A new method for optimized laser treatment by laser focus navigation and distance visualization. In Proceedings of the 2007 29th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Lyon, France, 22–26 August 2007; IEEE: Piscataway, NJ, USA; pp. 1738–1741. [Google Scholar]
- Apel, C.; Franzen, R.; Meister, J.; Sarrafzadegan, H.; Thelen, S.; Gutknecht, N. Influence of the Pulse Duration of an Er:YAG Laser System on the Ablation Threshold of Dental Enamel. Lasers Med. Sci. 2002, 17, 253–257. [Google Scholar] [CrossRef]
- Matsuyama, T.; Aoki, A.; Oda, S.; Yoneyama, T.; Ishikawa, I. Effects of the Er:YAG Laser Irradiation on Titanium Implant Materials and Contaminated Implant Abutment Surfaces. J. Clin. Laser Med. Surg. 2003, 21, 7–17. [Google Scholar] [CrossRef] [PubMed]
- Kreisler, M.; Al Haj, H.; D’Hoedt, B. Temperature changes at the implant-bone interface during simulated surface decontamination with an Er:YAG laser. Int. J. Prosthodont. 2002, 15, 582–587. [Google Scholar]
- Colucci, V.; Amaral, F.L.B.D.; Pécora, J.D.; Palma-Dibb, R.G.; Corona, S.A.M. Water flow on erbium:yttrium–aluminum–garnet laser irradiation: Effects on dental tissues. Lasers Med. Sci. 2008, 24, 811–818. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.-E.; Jeoung, D.-J.; Kim, K.-S. Effects of Water Flow on Dental Hard Tissue Ablation Using Er:YAG Laser. J. Clin. Laser Med. Surg. 2003, 21, 139–144. [Google Scholar] [CrossRef] [PubMed]
- George, R.; Walsh, L.J. Performance assessment of novel side firing flexible optical fibers for dental applications. Lasers Surg. Med. 2009, 41, 214–221. [Google Scholar] [CrossRef] [PubMed]
- Geometric Product Specification (GPS). Surface Texture: Areal. Part 2: Terms, Definitions and Surface Texture Parameters. Geneva: Int. Org. Stand. Available online: https://www.iso.org/standard/42785.html (accessed on 6 August 2020).
- Palmquist, A.; Omar, O.M.; Esposito, M.; Lausmaa, J.; Thomsen, P. Titanium oral implants: Surface characteristics, interface biology and clinical outcome. J. R. Soc. Interface 2010, 7. [Google Scholar] [CrossRef]
- Albrektsson, T.; Wennerberg, A. Oral implant surfaces: Part 1--review focusing on topographic and chemical properties of different surfaces and in vivo responses to them. Int. J. Prosthodont. 2004, 17, 536–543. [Google Scholar]
- Romanos, D.G.E.; Everts, H.; Nentwig, G.H. Effects of Diode and Nd:YAG Laser Irradiation on Titanium Discs: A Scanning Electron Microscope Examination. J. Periodontol. 2000, 71, 810–815. [Google Scholar] [CrossRef]
- Kreisler, M.; Götz, H.; Duschner, H. Effect of Nd:YAG, Ho:YAG, Er:YAG, CO2, and GaAIAs laser irradiation on surface properties of endosseous dental implants. Int. J. Oral Maxillofac. Implant. 2002, 17, 202–211. [Google Scholar]
- Vassalli, M.; Giannelli, M. Effect of Nd: YAG laser on titanium dental implants studied by AFM. Ital. J. Anat. Embryol. = Arch. Ital. di Anat. ed embriologia 2004, 108, 195–203. [Google Scholar]
- Larsen, O.I.; Enersen, M.; Kristoffersen, A.K.; Wennerberg, A.; Bunæs, D.F.; Lie, S.A.; Leknes, K.N. Antimicrobial Effects of Three Different Treatment Modalities on Dental Implant Surfaces. J. Oral Implant. 2017, 43, 429–436. [Google Scholar] [CrossRef] [PubMed]
- Schwarz, F.; Sculean, A.; Romanos, G.; Herten, M.; Horn, N.; Scherbaum, W.; Becker, J. Influence of different treatment approaches on the removal of early plaque biofilms and the viability of SAOS2 osteoblasts grown on titanium implants. Clin. Oral Investig. 2005, 9, 111–117. [Google Scholar] [CrossRef] [PubMed]
- George, R.; Walsh, L.J. Factors Influencing the Ablating Potential of the Er: YAG Laser When Used to Ablate Radicular Dentine. J. Oral Laser Appl. 2008, 8, 33–41. [Google Scholar]
- Meister, J.; Apel, C.; Franzen, R.; Gutknecht, N. Influence of the spatial beam profile on hard tissue ablation Part I: Multimode emitting Er:YAG lasers. Lasers Med. Sci. 2003, 18, 112–118. [Google Scholar] [CrossRef]
- Vieiraalves, P.R.; Aranha, N.; Alfredo, E.; Marchesan, M.; Junior, A.B.; Sousa-Neto, M.D. Evaluation of Hollow Fiberoptic Tips for the Conduction of Er:YAG Laser. Photomed. Laser Surg. 2005, 23, 410–415. [Google Scholar] [CrossRef]
- George, R.; Walsh, L.J. Performance assessment of novel side firing safe tips for endodontic applications. J. Biomed. Opt. 2011, 16. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Panel Setting | Implant Surface and Fibre Tip Design Combinations | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Machined Surface | Micro-Roughened Surface | ||||||||
| Plain | Conical | Plain | Conical | ||||||
| Group 1 Er:YAG with fibre in 2062 handpiece | 400 mJ/1Hz 500 mJ/1Hz 600 mJ/1Hz | Wet | Dry | Wet | Dry | Wet | Dry | Wet | Dry |
| Group 2 Er:YAG 2060 Focusing handpiece | 200 mJ/1Hz 300 mJ/1Hz 400 mJ/1Hz 500 mJ/1Hz 600 mJ/1Hz | N/A | N/A | ||||||
| Group 3 Nd:YAG with fibre | 30mJ/10Hz 60 mJ/10Hz 90 mJ/10Hz 1W/20Hz 2W/20Hz 3W/20Hz | Wet | Dry | Wet | Dry | ||||
| Group 4 Control | Non-irradiated | N/A | N/A | N/A | N/A | ||||
| Panel Setting | Power Density (W/cm2) | ||
|---|---|---|---|
| Conical Fibre Tips | Plain Fibre Tips | ||
| Er:YAG fibre in 2062 handpiece | 400 mJ/1Hz 500 mJ/1Hz 600 mJ/1Hz | 5.40 6.45 7.60 | 11.50 13.25 15.45 |
| Er:YAG 2060 focusing handpiece | 200 mJ/1Hz 300 mJ/1Hz 400 mJ/1Hz 500 mJ/1Hz 600 mJ/1Hz | N/A | 6.75 8.55 11.35 14.65 18.45 |
| Nd:YAG | 30 mJ/10Hz 60 mJ/1Hz 90 mJ/1Hz 50 mJ/20Hz (1 W) 100 mJ/20Hz (2 W) 150 mJ/20Hz (3 W) | 9.90 16.50 25.00 29.50 59.00 81.00 | 12.00 23.00 34.00 38.00 75.00 109.00 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fenelon, T.; Bakr, M.M.; Walsh, L.J.; George, R. Effects of Lasers and Their Delivery Characteristics on Machined and Micro-Roughened Titanium Dental Implant Surfaces. Bioengineering 2020, 7, 93. https://0-doi-org.brum.beds.ac.uk/10.3390/bioengineering7030093
Fenelon T, Bakr MM, Walsh LJ, George R. Effects of Lasers and Their Delivery Characteristics on Machined and Micro-Roughened Titanium Dental Implant Surfaces. Bioengineering. 2020; 7(3):93. https://0-doi-org.brum.beds.ac.uk/10.3390/bioengineering7030093
Chicago/Turabian StyleFenelon, Thomas, Mahmoud M. Bakr, Laurence J. Walsh, and Roy George. 2020. "Effects of Lasers and Their Delivery Characteristics on Machined and Micro-Roughened Titanium Dental Implant Surfaces" Bioengineering 7, no. 3: 93. https://0-doi-org.brum.beds.ac.uk/10.3390/bioengineering7030093