
A New Protocol to Treat Abdominal Subcutaneous Fat Combining Microwaves and Flat magnetic stimulation

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Experimental Protocol
2.2. Objective and Patients’ Assessments
2.3. Statistical Analyses
3. Results
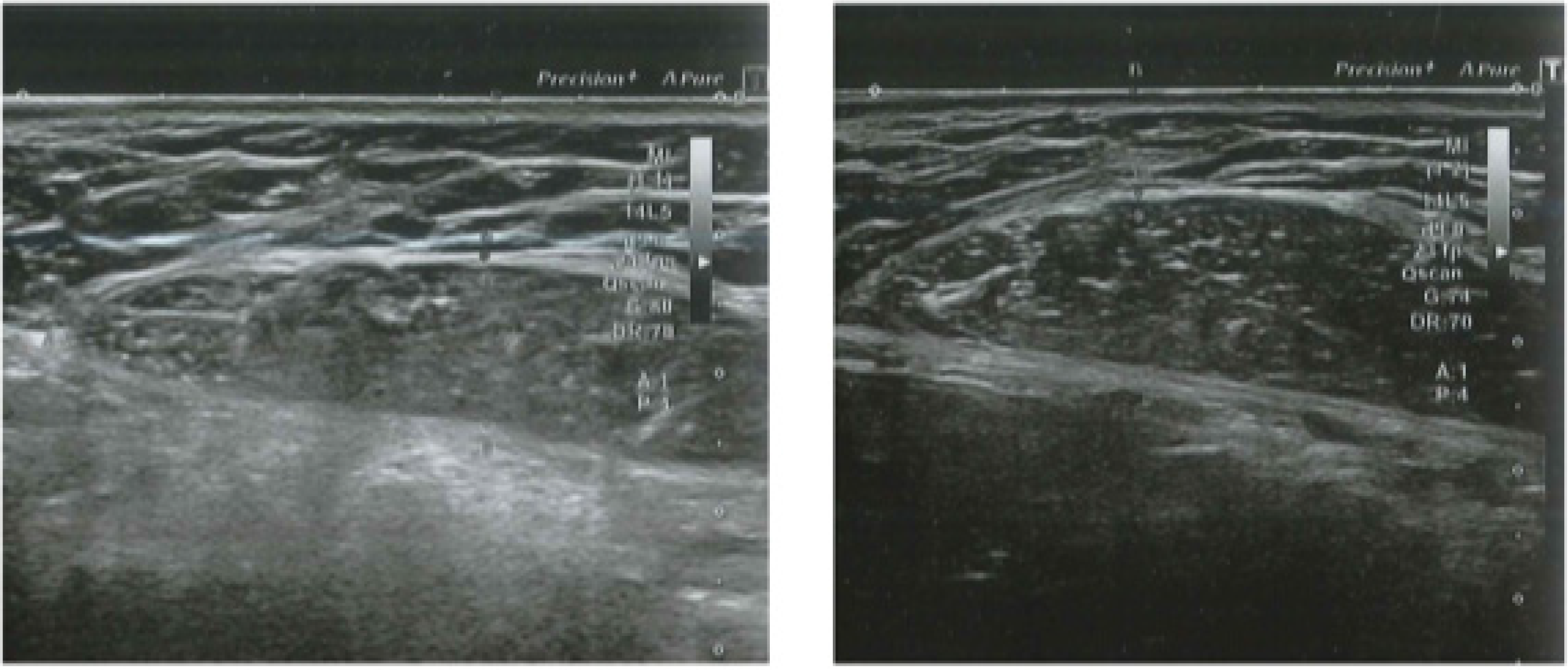
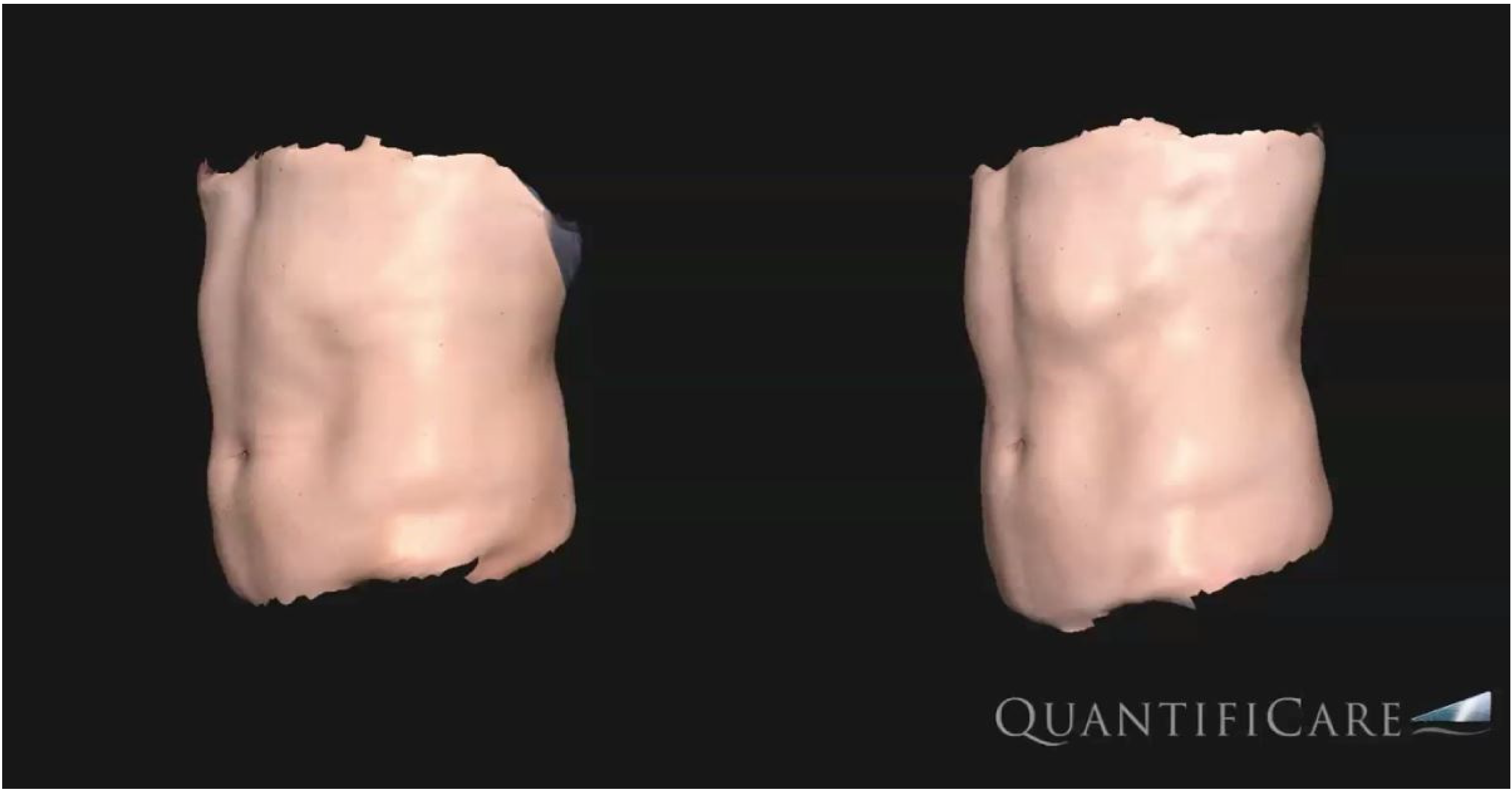
3.1. Objective Measurements
3.2. Blood Examination
3.3. Patients’ Assessments and Side Effects
4. Discussion
Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Friedmann, D.P.; Avram, M.M.; Cohen, S.R.; Duncan, D.I.; Goldman, M.P.; Weiss, E.T.; Young, L. An evaluation of the patient population for aesthetic treatments targeting abdominal subcutaneous adipose tissue. J. Cosmet. Dermatol. 2014, 13, 119–124. [Google Scholar] [CrossRef]
- Friedmann, D.P. A review of the aesthetic treatment of abdominal subcutaneous adipose tissue: Background, implications, and therapeutic options. Dermatol. Surg. 2015, 41, 18–34. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, J.; Verne, S.; Griffith, R.; Falto-Aizpurua, L.; Nouri, K. Non-invasive subcutaneous fat reduction: A review. J. Eur. Acad. Dermatol. Venereol. 2015, 29, 1679–1688. [Google Scholar] [CrossRef] [PubMed]
- Saedi, N.; Kaminer, M. New waves for fat reduction: High-intensity focused ultrasound. Semin. Cutan. Med. Surg. 2013, 32, 26–30. [Google Scholar] [PubMed]
- Jewell, M.L.; Solish, N.J.; Desilets, C.S. Non-invasive body sculpting technologies with an emphasis on high-intensity focused ultrasound. Aesthetic Plast. Surg. 2011, 35, 901–912. [Google Scholar] [CrossRef] [PubMed]
- Bennardo, L.; Fusco, I.; Cuciti, C.; Sicilia, C.; Salsi, B.; Cannarozzo, G.; Hoffmann, K.; Nisticò, S.P. Microwave Therapy for Cellulite: An Effective Non-Invasive Treatment. J. Clin. Med. 2022, 11, 515. [Google Scholar] [CrossRef] [PubMed]
- Bonan, P.; Verdelli, A. Combined microwaves and fractional microablative CO2 laser treatment for postpartum abdominal laxity. J. Cosmet. Dermatol. 2021, 20, 124–131. [Google Scholar] [CrossRef]
- Mozaffarian, D. Dietary and Policy Priorities for Cardiovascular Disease, Diabetes, and Obesity: A Comprehensive Review. Circulation 2016, 133, 187–225. [Google Scholar] [CrossRef]
- Mezzana, P.; Pieri, L.; Leone, A.; Fusco, I. Schwarzy: The new system for muscle toning and body shaping. J. Cosmet. Dermatol. 2021, 20, 2678–2680. [Google Scholar] [CrossRef] [PubMed]
- Hoeffelin, H.; Jacquemin, D.; Defaweux, V.; Nizet, J.L. A methodological evaluation of volumetric measurement techniques including three-dimensional imaging in breast surgery. Biomed. Res. Int. 2014, 2014, 573249. [Google Scholar] [CrossRef]
- Tsuka, T.; Okamoto, Y.; Sunden, Y.; Morita, T.; Yamashita, M.; Osaki, T.; Azuma, K.; Amaha, T.; Ito, N.; Murahata, Y.; et al. Ultrasonography of sudden swollen tongue in a calf. BMC Vet. Res. 2020, 16, 200. [Google Scholar] [CrossRef] [PubMed]
- Alizadeh, Z.; Halabchi, F.; Mazaheri, R.; Abolhasani, M.; Tabesh, M. Review of the Mechanisms and Effects of Noninvasive Body Contouring Devices on Cellulite and Subcutaneous Fat. Int. J. Endocrinol. Metab. 2016, 14, e36727. [Google Scholar] [CrossRef] [Green Version]
- Pahlavani, N.; Nattagh-Eshtivani, E.; Amanollahi, A.; Ransbar, G. Effects of microwave technology on the subcutaneous abdominal fat and anthropometric indices of overweight adults: A clinical trial. J. Cosmet. Dermatol. 2021, 21, 1482–1488. [Google Scholar] [CrossRef] [PubMed]
- Foster, K.R.; Ziskin, M.C.; Balzano, Q. Thermal Response of Human Skin to Microwave Energy: A Critical Review. Health Phys. 2016, 111, 528–541. [Google Scholar] [CrossRef]
- Zerbinati, N.; d’Este, E.; Farina, A.; Cornaglia, A.I.; Jafferany, M.; Golubovic, M.; Binic, I.; Sigova, J.; Van Thuong, N.; Tirant, M.; et al. Remodeling of collagen constituting interlobular septa of subcutaneous adipose tissue following microwaves application. Dermatol. Ther. 2020, 33, e13362. [Google Scholar] [CrossRef]
- Jacob, C.I.; Paskova, K. Safety and efficacy of a novel high-intensity focused electromagnetic technology device for non-invasive abdominal body shaping. J. Cosmet. Dermatol. 2018, 17, 783–787. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goldberg, D.J.; Enright, K.M.; Goldfarb, R.; Katz, B.; Gold, M. The role and clinical benefits of high-intensity focused electromagnetic devices for non-invasive lipolysis and beyond: A narrative review and position paper. J. Cosmet. Dermatol. 2021, 20, 2096–2101. [Google Scholar] [CrossRef]
- Giesse, S. A German Prospective Study of the Safety and Efficacy of a Non-Invasive, High-intensity, Electromagnetic Abdomen and Buttock Contouring Device. J. Clin. Aesthet. Dermatol. 2021, 14, 30–33. [Google Scholar] [PubMed]
- Jacob, C.I.; Rank, B. Abdominal Remodeling in Postpartum Women by Using a High-intensity Focused Electromagnetic (HIFEM) Procedure: An Investigational Magnetic Resonance Imaging (MRI) Pilot Study. J. Clin. Aesthet. Dermatol. 2020, 13 (Suppl. 1), S16–S20. [Google Scholar] [PubMed]
- Duncan, D.; Dinev, I. Noninvasive Induction of Muscle Fiber Hypertrophy and Hyperplasia: Effects of High-Intensity Focused Electromagnetic Field Evaluated in an In-Vivo Porcine Model: A Pilot Study. Aesthet. Surg. J. 2020, 40, 568–574. [Google Scholar] [CrossRef] [PubMed]
- Weiss, R.A.; Bernardy, J.; Tichy, F. Simultaneous Application of High-Intensity Focused Electromagnetic and Synchronized Radiofrequency for Fat Disruption: Histological and Electron Microscopy Porcine Model Study. Dermatol. Surg. 2021, 47, 1059–1064. [Google Scholar] [CrossRef] [PubMed]
- Goldberg, D.J. Deletion of adipocytes induced by a novel device simultaneously delivering synchronized radiofrequency and hifem: Human histological study. J. Cosmet. Dermatol. 2021, 20, 1104–1109. [Google Scholar] [CrossRef]
- Kinney, B.M.; Lozanova, P. High intensity focused electromagnetic therapy evaluated by magnetic resonance imaging: Safety and efficacy study of a dual tissue effect based non-invasive abdominal body shaping. Lasers Surg. Med. 2019, 51, 40–46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kent, D.E.; Kinney, B.M. The effect of high-intensity focused electromagnetic procedure on visceral adipose tissue: Retrospective assessment of computed tomography scans. J. Cosmet. Dermatol. 2021, 20, 757–762. [Google Scholar] [CrossRef] [PubMed]
- Kranendonk, M.E.; Visseren, F.L.; van Balkom, B.W.; Nolte-‘t Hoen, E.N.; van Herwaarden, J.A.; de Jager, W.; Schipper, H.S.; Brenkman, A.B.; Verhaar, M.C.; Wauben, M.H.; et al. Human adipocyte extracellular vesicles in reciprocal signaling between adipocytes and macrophages. Obesity 2014, 22, 1296–1308. [Google Scholar] [CrossRef] [PubMed]
- Cinti, S.; Mitchell, G.; Barbatelli, G.; Murano, I.; Ceresi, E.; Faloia, E.; Wang, S.; Fortier, M.; Greenberg, A.S.; Obin, M.S. Adipocyte death defines macrophage localization and function in adipose tissue of obese mice and humans. J. Lipid Res. 2005, 46, 2347–2355. [Google Scholar] [CrossRef] [Green Version]
- Frank, K.; Hamade, H.; Casabona, G.; Gotkin, R.H.; Kaye, K.O.; Tiryaki, T.; Freytag, D.L.; Bialowas, C.; Koban, K.C.; Cotofana, S. Influences of Age, Gender, and Body Mass Index on the Thickness of the Abdominal Fatty Layers and its Relevance for Abdominal Liposuction and Abdominoplasty. Aesthet. Surg. J. 2019, 39, 1085–1093. [Google Scholar] [CrossRef] [PubMed]
- Nistico, S.P.; Silvestri, M.; Zingoni, T.; Tamburi, F.; Bennardo, L.; Cannarozzo, G. Combination of Fractional CO2 Laser and Rhodamine-Intense Pulsed Light in Facial Rejuvenation: A Randomized Controlled Trial. Photobiomodul. Photomed. Laser Surg. 2021, 39, 113–117. [Google Scholar] [CrossRef] [PubMed]
- Cannarozzo, G.; Fazia, G.; Bennardo, L.; Tamburi, F.; Amoruso, G.F.; Del Duca, E.; Nistico, S.P. A New 675 nm Laser Device in the Treatment of Facial Aging: A Prospective Observational Study. Photobiomodul. Photomed. Laser Surg. 2021, 39, 118–122. [Google Scholar] [CrossRef] [PubMed]
- Leone, A.; Piccolo, D.; Conforti, C.; Pieri, L.; Fusco, I. Evaluation of safety and efficacy of a new device for muscle toning and body shaping. J. Cosmet. Dermatol. 2021, 20, 3863–3870. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| 1st Month | First Day of the Week | Third Day of the Week |
|---|---|---|
| 1st week | Onda + Schwarzy (Massage) | Schwarzy (Massage) |
| 2nd week | Schwarzy (Massage) | Schwarzy (Massage) |
| 3th week | Schwarzy (Shaping/Strenght) | Schwarzy (Shaping/Strenght) |
| 4th week | Schwarzy (Shaping/Strenght) | Schwarzy (Shaping/Strenght) |
| 2nd month | First day of the week | |
| 1st week | Onda + Schwarzy (Massage) | Schwarzy (Massage) |
| 2nd week | Schwarzy (Massage) | |
| 3th week | Schwarzy (Shaping/Strenght) | |
| 4th week | Schwarzy (Shaping/Strenght) |
| Baseline | 3-Month Follow-Up | |
|---|---|---|
| Mean WC (cm) | 98.2 ± 7.4 | 94.0 ± 6.6 |
| Abdominal muscle tissue thicknesses: upper abdomen (mm) | 9.5 ± 3.0 | 12.0 ± 1.1 |
| Abdominal muscle tissue thicknesses: lower abdomen (mm) | 10.3 ± 2.4 | 14.1 ± 2.1 |
| Abdominal muscle tissue thicknesses: lateral abdomen (mm) | 10.1 ± 2.0 | 13.2 ± 3.3 |
| Rectus abdominis diastasis (mm) | 24.1 ± 4.1 | 22.1 ± 3.8 |
| Thickness of the adipose tissue (mm) | 9.8 ± 2.4 | 8.0 ± 2.1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nisticò, S.P.; Bonan, P.; Coli, F.; Verdelli, A.; Fusco, I.; Gratteri, F.; Sicilia, C.; Cantisani, C.; Pellacani, G.; Bennardo, L.; et al. A New Protocol to Treat Abdominal Subcutaneous Fat Combining Microwaves and Flat magnetic stimulation. Bioengineering 2022, 9, 182. https://0-doi-org.brum.beds.ac.uk/10.3390/bioengineering9050182
Nisticò SP, Bonan P, Coli F, Verdelli A, Fusco I, Gratteri F, Sicilia C, Cantisani C, Pellacani G, Bennardo L, et al. A New Protocol to Treat Abdominal Subcutaneous Fat Combining Microwaves and Flat magnetic stimulation. Bioengineering. 2022; 9(5):182. https://0-doi-org.brum.beds.ac.uk/10.3390/bioengineering9050182
Chicago/Turabian StyleNisticò, Steven Paul, Paolo Bonan, Federica Coli, Alice Verdelli, Irene Fusco, Francesco Gratteri, Claudia Sicilia, Carmen Cantisani, Giovanni Pellacani, Luigi Bennardo, and et al. 2022. "A New Protocol to Treat Abdominal Subcutaneous Fat Combining Microwaves and Flat magnetic stimulation" Bioengineering 9, no. 5: 182. https://0-doi-org.brum.beds.ac.uk/10.3390/bioengineering9050182