Predictors of Fatal Pulmonary Haemorrhage in Dogs Affected by Leptospirosis Approaching Haemodialysis

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Klopfleisch, R.; Kohn, B.; Plog, S.; Weingart, C.; Nockler, K.; Mayer-Scholl, A.; Gruber, A.D. An emerging pulmonary haemorrhagic syndrome in dogs similar to the human leptospiral pulmonary haemorrhagic syndrome? Vet. Med. Int. 2010, 27, 928541. [Google Scholar] [CrossRef] [PubMed]
- Schuller, S.; Francey, T.; Hartmann, K.; Hugonnard, M.; Kohn, B.; Nally, J.E.; Sykes, J. European consensus statement on leptospirosis in dogs and cats. J. Small Anim. Pract. 2015, 56, 159–179. [Google Scholar] [CrossRef] [PubMed]
- Sykes, J.E.; Hartmann, K.F.; Lunn, K.F.; Moore, G.E.; Stoddard, R.A.; Goldstein, R.E. 2010 ACVIM Small Animal Consensus Statement on Leptospirosis: Diagnosis, epidemiology, treatment, and prevention. J. Vet. Intern. Med. 2011, 25, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Arean, V.M.; Sarasin, G.; Green, J.H. The pathogenesis of leptospirosis: Toxin production by leptospira icterohaemorrhagiae. Am. J. Vet. Res. 1964, 25, 836–843. [Google Scholar]
- Croda, J.; Ramos, J.G.R.; Matsunaga, J.; Queiroz, A.; Homma, A.; Riley, L.W.; Haake, D.A.; Reis, M.G.; Ko, A.I. Leptospira immunoglobulin-like proteins as a serodiagnostic marker for acute leptospirosis. J. Clin. Microbiol. 2007, 45, 1528–1534. [Google Scholar] [CrossRef] [Green Version]
- Martinez Garcia, M.A.; De Diego Damia, A.; Villaneuva, R.M.; Lopez Hontagas, J.L. Pulmonary involvement in Leptospirosis. Eur. J. Clin. Microbiol. Inf. Dis. 2000, 19, 471–474. [Google Scholar] [CrossRef] [PubMed]
- Herath, N.; Uluwattage, W.; Weliwitiya, T.; Karunanayake, L.; Lekamwasam, S.; Ratnatunga, N.; Karunanayake, P.; Wickramasinghe, S.; Patabendi, S.; Senaviratne, S.; et al. Sequel and therapeutic modalities of leptospirosis associated severe pulmonary haemorrhagic syndrome (SPHS); a Sri Lankan experience. BMC Infect Dis. 2019, 19, 451. [Google Scholar] [CrossRef] [PubMed]
- Marchiori, E.; Lourenco, S.; Setubal, S.; Zanetti, G.; Davaus Gasparetto, T.; Hochhegger, B. Clinical and imaging manifestations of hemorrhagic pulmonary Leptospirosis: A state of the art review. Lung 2011, 189, 1–9. [Google Scholar] [CrossRef]
- Segev, G.; Kass, P.H.; Francey, T.; Cowgill, L.D. A novel clinical scoring system for outcome prediction in dogs with acute kidney injury managed by hemodialysis. J. Vet. Intern. Med. 2008, 22, 301–308. [Google Scholar] [CrossRef]
- Knopfler, S.; Mayer-Scholl, A.; Luge, E.; Klopfleisch, R.; Gruber, A.D.; Nockler, K.; Kohn, B. Evaluation of clinical, laboratory, imaging findings and outcome in 99 dogs with leptospirosis. J. Small Anim. Pract. 2017, 58, 582–588. [Google Scholar] [CrossRef]
- Kohn, B.; Steinicke, K.; Arndt, G.; Gruber, A.D.; Guerra, B.; Jansen, A.; Kaser-Hotz, B.; Klopfleisch, R.; Lotz, F.; Luge, E.; et al. Pulmonary abnormalities in dogs with leptospirosis. J. Vet. Intern. Med. 2010, 24, 1277–1282. [Google Scholar] [CrossRef]
- Major, A.; Schweighauser, A.; Francey, T. Increasing incidence of canine leptospirosis in Switzerland. Int. J. Environ. Res. Public Health 2014, 11, 7242–7260. [Google Scholar] [CrossRef] [Green Version]
- Ross, S. Anticoagulation in intermittent hemodialysis: Pathways, protocols and pittfalls. Vet. Clin. N. Am. Small Anim. Pract. 2011, 41, 163–175. [Google Scholar] [CrossRef] [PubMed]
- Andrade, L.; Cleto, S.; Seguro, A.C. Door to dialysis time and daily hemodialysis in patients with leptospirosis: Impact on mortality. Clin. J. Am. Soc. Nephrol. 2007, 2, 739–744. [Google Scholar] [CrossRef]
- Maissen-Villinger, C.A.; Schweinghauser, A.; Van Dorland, A.; Morel, C.; Bruckmaier, R.M.; Zurbriggen, A.; Francey, T. Expression profile of cytokines and enzymes mRNA in blood leukocytes of dogs with Leptospirosis and its associated pulmonary haemorrhage syndrome. PLoS ONE 2016, 11, e0148029. [Google Scholar]
- Schuller, S.; Callanan, J.J.; Worrall, S.; Francey, T.; Schweighauser, A.; Kohn, B.; Klopfleisch, R.; Posthaus, H.; Nally, J.E. Immunohistochemical detection of IgM and IgG in lung tissue of dogs with leptospiral pulmonary haemorrhage syndrome. Comp. Immunol. Microbiol. Infect Dis. 2015, 40, 47–53. [Google Scholar] [CrossRef] [PubMed]
- Fraga, T.R.; Barbosa, A.S.; Isaac, L. Leptospirosis: Aspects of innate immunity, immunopathogenesis and immune evasion from the complement system. Scand. J. Immunol. 2011, 73, 408–419. [Google Scholar] [CrossRef] [PubMed]
- Pereira, M.; Valerio-Bolas, A.; Saraiva-Marques, C.; Alexandre-Pires, G.; Pereira da Fonseca, I.; Santos-Gomes, G. Development of dog immune system: From in uterus to elderly. Vet. Sci. 2019, 6, 83. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spichler, A.S.; Villaca, P.J.; Athanazio, D.A.; Albuquerque, J.O.M.; Buzzar, M.; Castro, B.; Seguro, A.; Vinetz, J.M. Predictors of lethality in severe Leptospirosis in urban Brazil. Am. J. Trop. Med. Hyg. 2008, 79, 911–914. [Google Scholar] [CrossRef] [Green Version]
- De Francesco Daher, E.; Soares de Abreu, K.L.; da Silva Junior, G.B. Leptospirosis-associated acute kidney injury. J. Bras Nefrol. 2010, 32, 400–407. [Google Scholar]
- Tantitanawat, S.; Tanjatham, S. Prognostic factors associated with severe leptospirosis. J. Med. Assoc. Thai 2003, 86, 925–931. [Google Scholar] [PubMed]
- Esen, S.; Sunbul, M.; Leblebicioglu, H.; Eroglu, C.; Turan, D. Impact of clinical and laboratory findings on prognosis in leptospirosis. Swiss Med. Wkly. 2004, 134, 347–352. [Google Scholar]
- Baumann, D.; Fluckiger, M. Radiographic findings in the thorax of dogs with leptospiral infection. Vet. Radiol. Ultrasound 2001, 42, 305–307. [Google Scholar] [CrossRef] [PubMed]
- Barthelemy, A.; Magnin, M.; Pouzot-Nevoret, C.; Bonnet-Garin, J.M.; Hugonnard, M.; Goy-Thollot, I. Hemorrhagic, hemostatic, and thromboelastometric disorders in 35 dogs with a clinical diagnosis of Leptospirosis: A prospective study. J. Vet. Intern. Med. 2017, 31, 69–80. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marotto, P.C.; Ko, A.I.; Murta-Nascimento, C.; Seguro, A.C.; Prado, R.R.; Barbosa, M.C.; Cleto, S.A.; Eluf-Neto, J. Early identification of leptospirosis-associated pulmonary haemorrhage syndrome by use of a validated prediction model. J. Infect. 2010, 60, 218–223. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variables | Reference Range | PH (n = 10) Mean ± SD; Median (min-max) | nPH (n = 37) Mean ± SD; Median (min-max) | p Value |
|---|---|---|---|---|
| Creatinine | 0.6–1.5 mg/dL | 9.8 (8.0–22.0) | 8.7 (2.3–21.1) | 0.075 |
| Urea | 15–55 mg/dL | 349.5 (266–611) | 347 (109–626) | 0.603 |
| Calcium | 8.7–11.8 mg/dL | 9.6 ± 1.3 | 10.4 ± 2.4 | 0.325 |
| Phosphate | 2.5–5 mg/dL | 14.4 (10.0–22.0) | 13.9 (5.4–59.0) | 0.795 |
| HCO3 | 21–31 mEq/L | 11.0 (6.0–16.0) | 14.0 (5.0–29.0) | 0.254 |
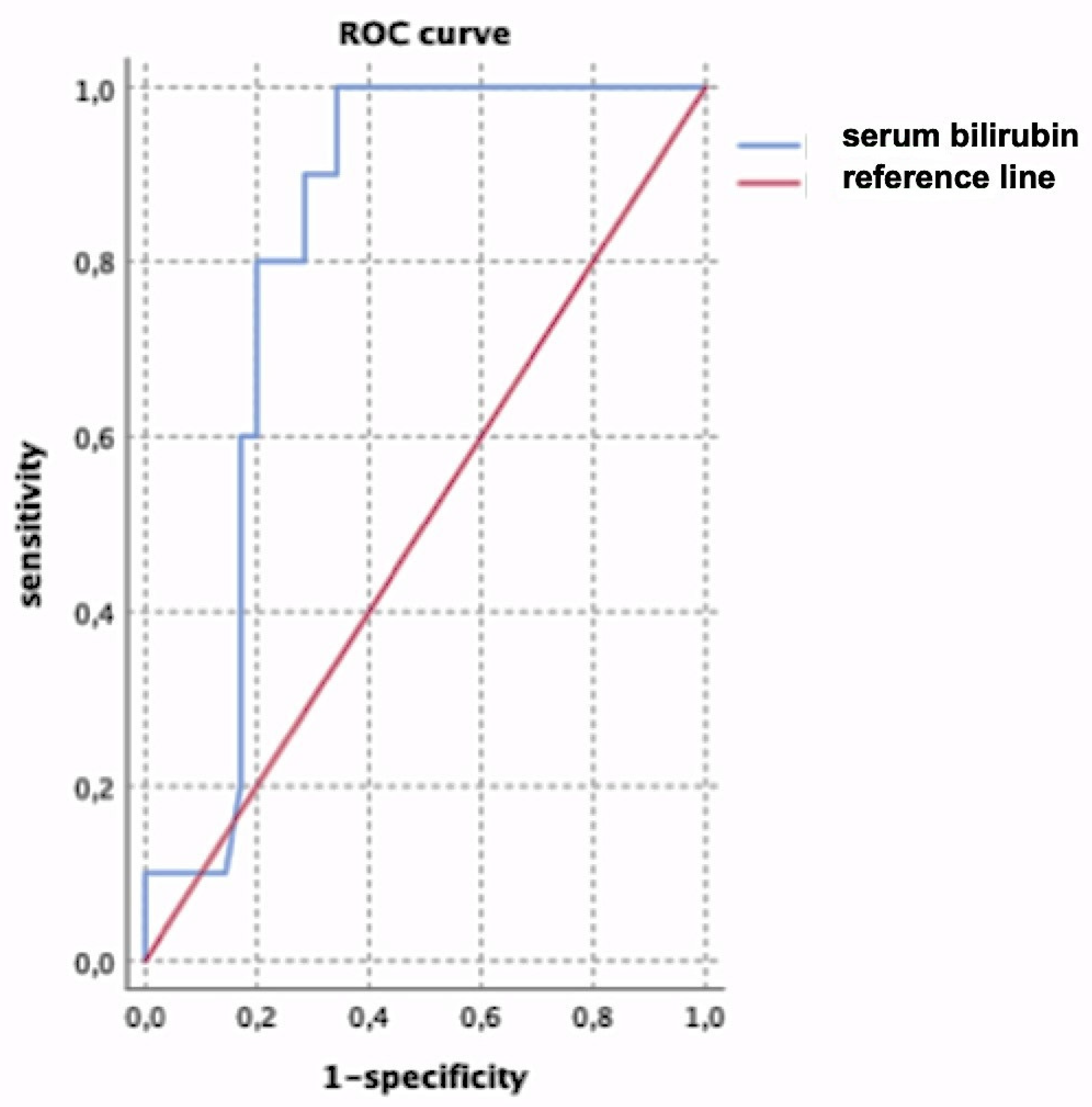
| Bilirubin | 0.07–0.3 mg/dL | 17.2 ± 13.3 | 5.6 ± 8.5 | 0.002 * |
| AST | 15–40 U/L | 204.7 ± 96.0 | 115.6 ± 127.1 | 0.04 * |
| ALT | 20–70 U/L | 176.7 ± 45.9 | 100.7 ± 87.0 | 0.012 * |
| ALKP | 45–250 U/L | 1600.0 (1024.0–3541.0) | 563.5 (53.0–5050.0) | 0.002 * |
| Total Protein | 5.8–7.8 g/dL | 5.0 (4.0–6.8) | 5.8 (4.0–9.0) | 0.102 |
| Albumin | 2.6–4.1 g/dL | 2.5 (2.0–2.8) | 2.4 (1.3–3.7) | 0.948 |
| Glycaemia | 80–125 mg/dL | 83.0 (66–106) | 104.5 (60–171) | 0.014 * |
| CRP | 0–0.30 mg/dL | 1.6 (0.3–2.5) | 1.5 (0.3–5.2) | 0.557 |
| GGT | 2–11 U/L | 14.7 ± 7.6 | 11.0 ± 10.5 | 0.420 |
| Na | 146–156 mEq/L | 145.0 (139.0–155.0) | 146.0 (135.0–163.0) | 0.222 |
| K | 3.9–5.5 mEq/L | 5.8 (5.0–7.0) | 4.7 (2.8–8.6) | 0.089 |
| RBC | 5.65–8.87 M/μL | 4.8 (1.5–6.6) | 4.7 (1.3–8.2) | 0.761 |
| HCT | 37.3–61.7% | 35 (9–39) | 28 (9–53) | 0.187 |
| Hgb | 13.1–20.5 g/dL | 12.5 (3.5–15.0) | 10.0 (4.0–19.0) | 0.237 |
| WBC | 5.05–16.76 K/μL | 18.0 (7.6–28.8) | 18.3 (7.6–49.0) | 0.720 |
| Neutrophils | 2.95–11.64 K/μL | 16.5 ± 2.7 | 15.5 ± 6.3 | 0.587 |
| Eosinophils | 0.06–1.23 K/μL | 0.11 ± 0.17 | 0.10 ± 0.13 | 0.862 |
| Basophils | 0–0.10 K/μL | 0.03 ± 0.03 | 0.03 ± 0.04 | 0.852 |
| Lymphocytes | 1.05–5.10 K/μL | 1.0 (0.1–4.8) | 1.7 (0.5–8.8) | 0.604 |
| Monocytes | 0.16–1.12 K/μL | 2.3 (1.0–7.6) | 2.0 (0.2–4.1) | 0.426 |
| PLT | 148–484 K/μL | 72.3 ± 47.8 | 225.1 ± 173.3 | 0.04 * |
| PT | 5.5–11.4 sec | 27.6 ± 45.4 | 10.6 ± 17.0 | 0.126 |
| aPTT | 10.6–19.9 sec | 19.9 ± 2.4 | 21.6 ± 16.8 | 0.820 |
| Fibrinogen | 125–335 mg/dL | 621.0 (296.0–999.0) | 660.0 (103.0–2376.0) | 0.688 |
| BW | Kg | 30.0 (9.0–43.0) | 16.0 (5.0–43.0) | 0.052 |
| Age | Years | 4.5 (2.0–10.0) | 3.0 (0.3–13.0) | 0.150 |
| Icterus | 8/10 (80%) | 22/37 (59%) | 0.230 Phi: 0.175 | |
| Spontaneous bleeding | 6/10 (60%) | 12/37 (32%) | 0.112 Phi: 0.232 | |
| Respirtaory distress | 7/10 (70%) | 5/37 (13%) | 0.002 * Phi: 0.457 | |
| Radiological abnormalities | 6/10 (60%) | 17/37 (46%) | 0.177 Phi: 0.211 | |
| Radiological pattern Alveolar pattern Interstial-alveolar pattern Unstructured interstitial | 2/6 (33%) 3/6 (50%) 1/6 (17%) | 3/17 (18%) 5/17 (29%) 9/17 (53%) | 0.225 Phi: 0.325 | |
| Radiological pattern distribution Cranial Caudal Diffuse | 1/6 (17%) 1/6 (17%) 4/6 (66%) | 1/17 (6%) 11/17 (65%) 5/17 (29%) | 0.193 Phi: 0.340 | |
| Pleural effusion Present Absent | 1/10 (10%) 9/10 (90%) | 3/37 (8%) 34/37 (92%) | 0.849 Phi: 0.02 | |
| Variables | Logistic Regression Analysis | ||
|---|---|---|---|
| p | Odds Ratio | 95% CI | |
| Bilirubin | 0.013 * | 1.156 | 1.031–1.295 |
| AST | 0.380 | 0.993 | 0.978–1.009 |
| ALT | 0.324 | 1.016 | 0.985–1.048 |
| ALKP | 0.515 | 1.000 | 0.999–1.002 |
| PLT | 0.752 | 0.965 | 0.774–1.203 |
| Glycaemia | 0.172 | 0.926 | 0.828–1.034 |
| Respiratory distress | 0.003 * | 40.986 | 3.648–460.479 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lippi, I.; Puccinelli, C.; Perondi, F.; Ceccherini, G.; Pierini, A.; Marchetti, V.; Citi, S. Predictors of Fatal Pulmonary Haemorrhage in Dogs Affected by Leptospirosis Approaching Haemodialysis. Vet. Sci. 2021, 8, 25. https://0-doi-org.brum.beds.ac.uk/10.3390/vetsci8020025
Lippi I, Puccinelli C, Perondi F, Ceccherini G, Pierini A, Marchetti V, Citi S. Predictors of Fatal Pulmonary Haemorrhage in Dogs Affected by Leptospirosis Approaching Haemodialysis. Veterinary Sciences. 2021; 8(2):25. https://0-doi-org.brum.beds.ac.uk/10.3390/vetsci8020025
Chicago/Turabian StyleLippi, Ilaria, Caterina Puccinelli, Francesca Perondi, Gianila Ceccherini, Alessio Pierini, Veronica Marchetti, and Simonetta Citi. 2021. "Predictors of Fatal Pulmonary Haemorrhage in Dogs Affected by Leptospirosis Approaching Haemodialysis" Veterinary Sciences 8, no. 2: 25. https://0-doi-org.brum.beds.ac.uk/10.3390/vetsci8020025