
Anaplastic Mammary Carcinoma in Cat




CIISA, Faculdade de Medicina Veterinária, Universidade de Lisboa, Av. da Universidade Técnica, 1300-477 Lisboa, Portugal
*
Author to whom correspondence should be addressed.
†
Present address: Faculdade de Medicina Veterinária, Universidade Lusófona de Humanidades e Tecnologia, Campo Grande 376, 1749-024 Lisboa, Portugal.
Vet. Sci. 2021, 8(5), 77; https://doi.org/10.3390/vetsci8050077
Submission received: 21 April 2021
/
Revised: 27 April 2021
/
Accepted: 2 May 2021
/
Published: 4 May 2021
(This article belongs to the Special Issue Advances in Feline Internal Medicine)
Abstract
:Clinical, pathological, and immunohistochemical findings related to a feline mammary tumor with similar features to canine anaplastic mammary carcinoma are herein described for the first time. A female cat was presented for clinical evaluation with gastrointestinal signs, oedema, erythema, and painful lesion in the right inguinal region. Three weeks later, the mass had doubled in size and radiographic revaluation of the thoracic cavity revealed a metastatic pattern. Due to the poor prognosis and decline of the clinical status the owners decided for euthanasia. Post-mortem examination exposed a mammary tumoral mass with subcutaneous oedema, an enlargement of the right inguinal lymph node, and nodules in several organs. Histological analysis confirmed the presence of large pleomorphic epithelial cells, often grouped in small clusters with bizarre nuclei. Immunohistochemical study of the different lesions was performed and both primary tumor and regional metastasis showed tumor cells to be negative estrogen receptor alpha, positive progesterone receptor, positive HER-2, and positive pan-cytokeratin. Given that the clinical history was compatible with an inflammatory mammary carcinoma, the cyclooxygenase-2 expression levels were evaluated and presented a weak immunoreactivity. Regarding the distant metastatic lesions, tumor cells were negative for ER-α and PR and, positive both for HER-2 and pan-cytokeratin.
1. Introduction
Feline mammary carcinoma shows a high incidence, being the third most common tumor in this species [1]. Notwithstanding, feline anaplastic mammary carcinoma (AMC) was only briefly described by Della Salda et al. (1993) [2] and so far, no additional reports were published.
In dogs, the AMC is considered the most aggressive type of mammary tumor, showing a low frequency (4%) and being associated with a short survival time (less than 20 weeks) [3,4,5]. This histologic presentation is characterized by a diffuse infiltrating neoplasm composed of large, pleomorphic and multinucleated giant cells, frequently showing acidophilic cytoplasm and dispersed nuclear chromatin [2]. Lymphocytes, plasm cells, mast cells, neutrophils, eosinophils and macrophages may be presented among the tumor cells and in the stroma [6].
To the best of our knowledge, this is the first report that fully describes the clinical and molecular features of an AMC in a female cat.
2. Case Presentation
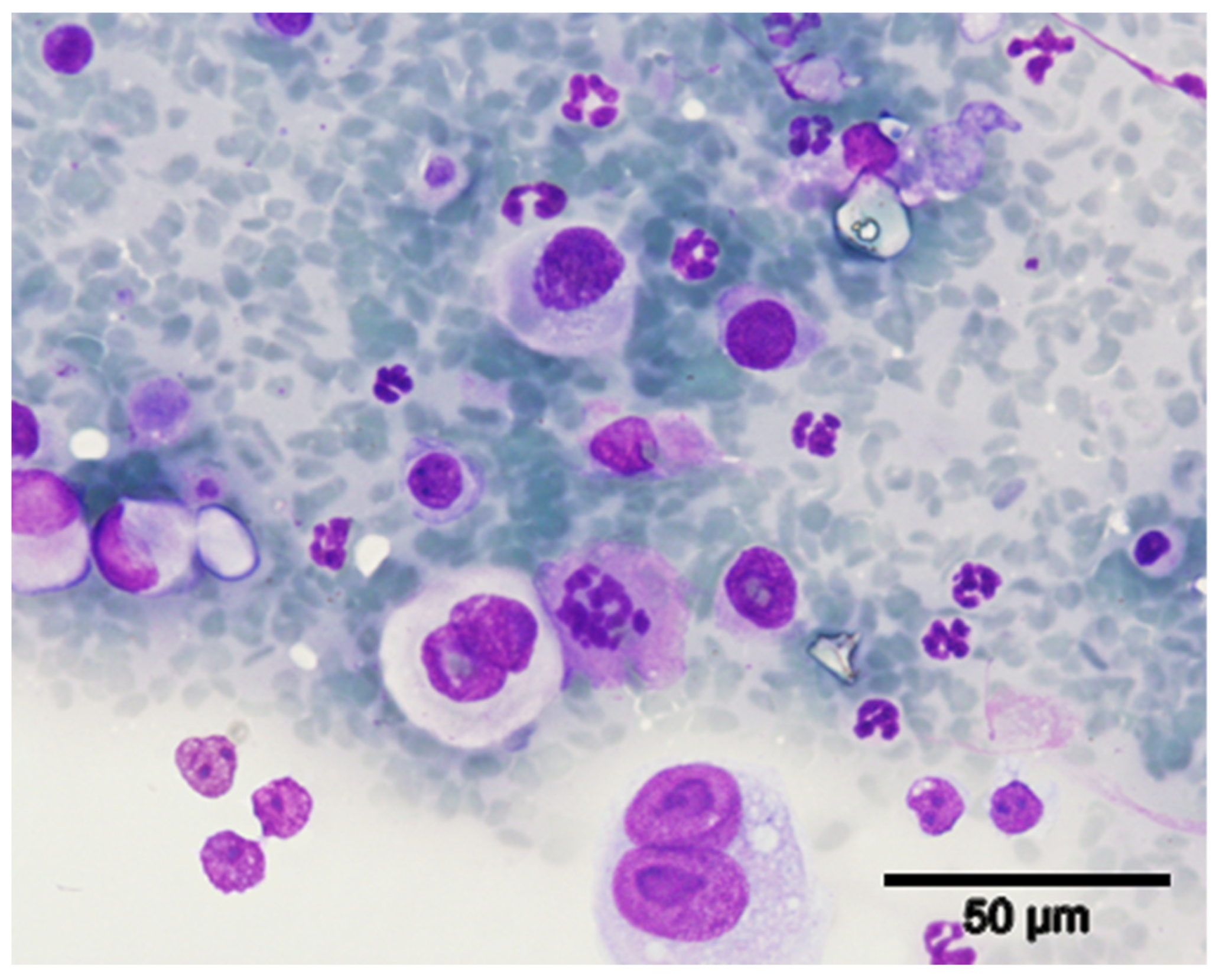
A 9-year-old spayed female cat of the European shorthair breed with vaccination and deworming overdue was presented at the Teaching Hospital of the Veterinary Medicine Faculty of Lisbon University with signs of vomit and melena. Physical examination revealed a non-pruritic, small nodule (<1 cm), surrounding the nipple of the inguinal right mammary gland. Regional pain was noted during palpation, and the subcutis was firm. The mass was subjected to a fine needle aspiration biopsy for cytological study and a mammary carcinoma was diagnosed based on the presence of cellular aggregates with neoplastic features, such as pleomorphic cells with bizarre nuclei and multinucleated cells, suggesting a high degree of malignancy (Figure 1).
Disease staging was based on the radiological evaluation of the thoracic cavity, with no signs of lung metastases, and hematological and biochemical profiles, neither presenting abnormal values. A radical mastectomy was then advised. In a period of three weeks, the clinical status of the animal rapidly deteriorated and the tumoral mass grew exuberantly (3 cm in diameter). Surgery could not be performed because animal developed anorexia, dehydration, tachypnea, abdominal distension (secondary to aerophagia due to the dyspnea), a weak femoral artery pulse, and lymphadenopathy of both the axillary and inguinal lymph regions. A systemic inflammatory reaction was diagnosed due to leucocytosis (31,400 cells/µL, reference values: 5500–19,500 cells/µL), and neutrophilia (28,260 cells/µL, reference values 2500–12,500 cells/µL) [7]. A radiographic thoracic re-evaluation showed a nodular interstitial lung pattern suggestive of a recent metastatic process. The abdominal ultrasound exam revealed enlargement of both mesenteric and colic lymph nodes (7 mm in diameter), although a normal biochemical profile was maintained.
Given the rapid evolution of a neoplastic disease of poor prognosis and attending the owners’ will, the animal was humanely euthanized. A thorough necropsy was performed, with subsequent histopathological analysis of various organs and tissues.
The following gross modifications were observed: (1) thickening of the skin with underlying subcutaneous oedema in the right inguinal area, (2) nonencapsulated mass with 3 cm in diameter at the right inguinal mammary gland, confined to the subcutaneous tissue (hypodermis), without showing dermic infiltration or into the underlying skeletal muscle (microscopically, the mass showed three smaller nodular lesions), and (3) homolateral inguinal and axillary lymph node enlargement. Moderate hemothorax and hemopericardium were observed, while scattered multifocal, small, nodular lesions could be observed throughout the lung parenchyma (and had a diameter of approximately 1 mm). Multiple nodular-shaped lesions (with a diameter of approximately 3–6 mm) were also observed in the liver, pancreas, right kidney, adrenal glands, cerebellum, brain, and several muscles. No other significant changes could be detected in the remaining organs.
3. Material and Methods
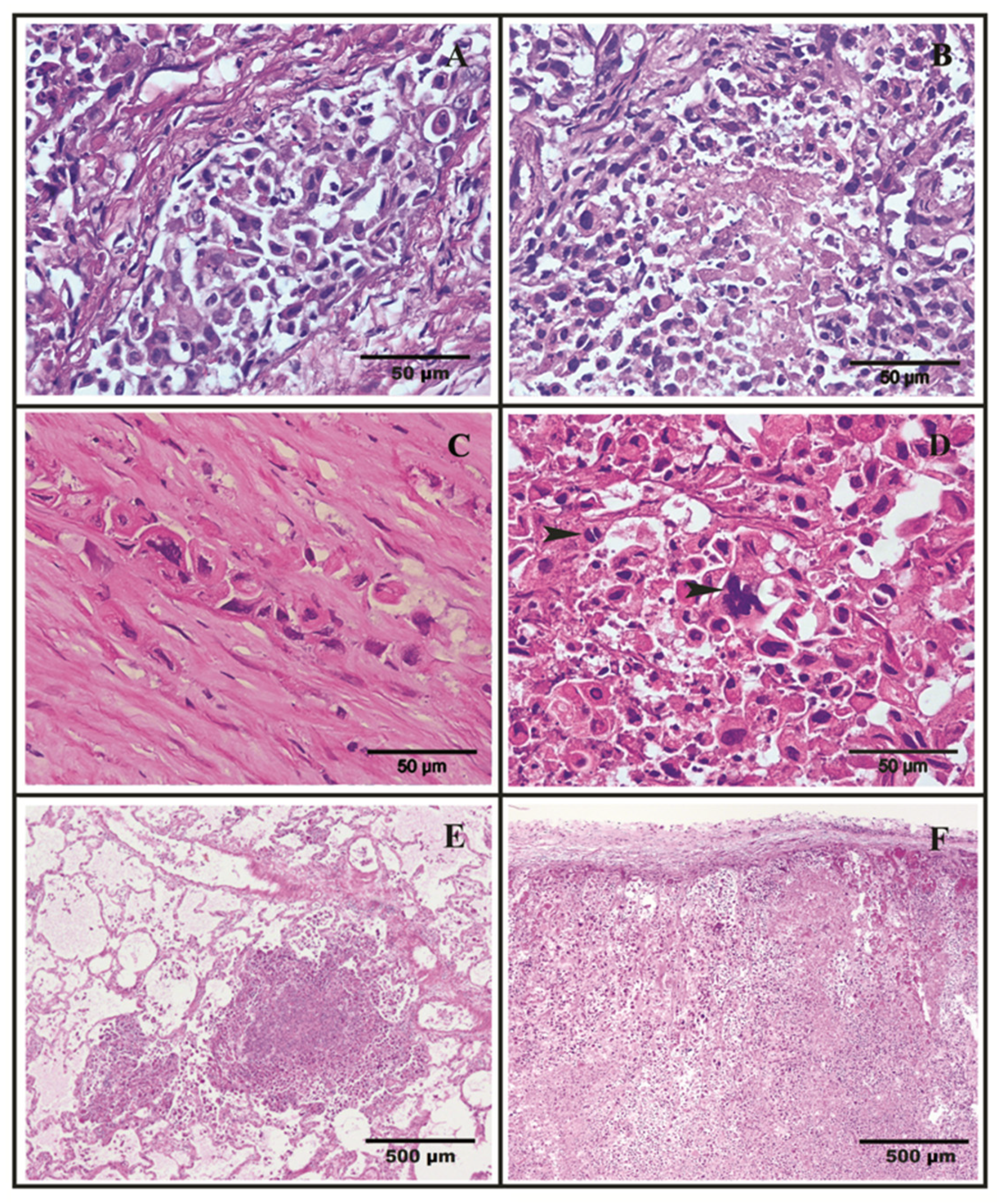
Tissue samples from several of the aforementioned lesions were collected and fixed in 10% buffered formalin for 24 h prior to routine histological processing. Histological examination of the lesions, including the mammary mass from which the cytological sample had been taken, revealed an epithelial malignant tumor. The primary tumor corresponded to a round mass of epithelial cells arranged in sheets separated by wide trabeculae of connective tissue, displaying a strong vascular invasion by neoplastic cells (Figure 2A). Extensive necrotic areas were visible (Figure 2B). Neoplastic cells were frequently individualized or arranged in small nests (Figure 2C), often surrounded by collagen fibers (desmoplasia). Small and rare areas of tubular differentiation can be identified. The predominant tumor cells are round or deformed due to close contact. The cytoplasm is acidophilic, and the large nucleus is very often deformed, hyperchromatic, with the nucleolus rarely identified. Giant cells are frequent, both macro and multinucleated (Figure 2D). The metastases (Figure 2E,F) in general showed cellular organization and morphology similar to the primitive tumor, with only small areas of tubular differentiation. According to Misdorp grade system this tumor was classified as highly malignant mammary carcinoma (grade III) [8].
Considering that tumor cells were poorly differentiated and that both anaplastic carcinomas and anaplastic sarcomas display this feature, pan-cytokeratin immunostaining was performed to verify the epithelial nature of the tumor and to help discriminate between these tumor types [9]. Moreover, the proliferation rate of the tumor was determined by calculating the Ki-67 index. Accordingly, the Ki-67 proliferation index was assessed by analyzing the percentage of Ki-67-positive tumor cell nuclei in 1000 tumor cells [10]. For molecular tumor classification, the expression levels of estrogen receptor alpha (ER-α) and the progesterone receptor (PR) were examined in addition to the HER-2 transmembrane receptor status. The antibodies used in this study were previously tested in feline mammary tissues [11,12], being discriminated in Table 1 with the immunohistochemistry protocols. Positive and negative controls were used for each antigen evaluated: a normal tonsil tissue sample for pan-cytokeratin and Ki-67 [10,13]; human mammary carcinomas tissue sample with known positive/negative status for the estrogen receptor alpha (ER-α), progesterone receptor (PR) and HER2 assessment [14], and feline uterus with cystic endometrial hyperplasia-pyometra complex positive for cyclooxygenase-2 (COX-2) [15].
4. Results
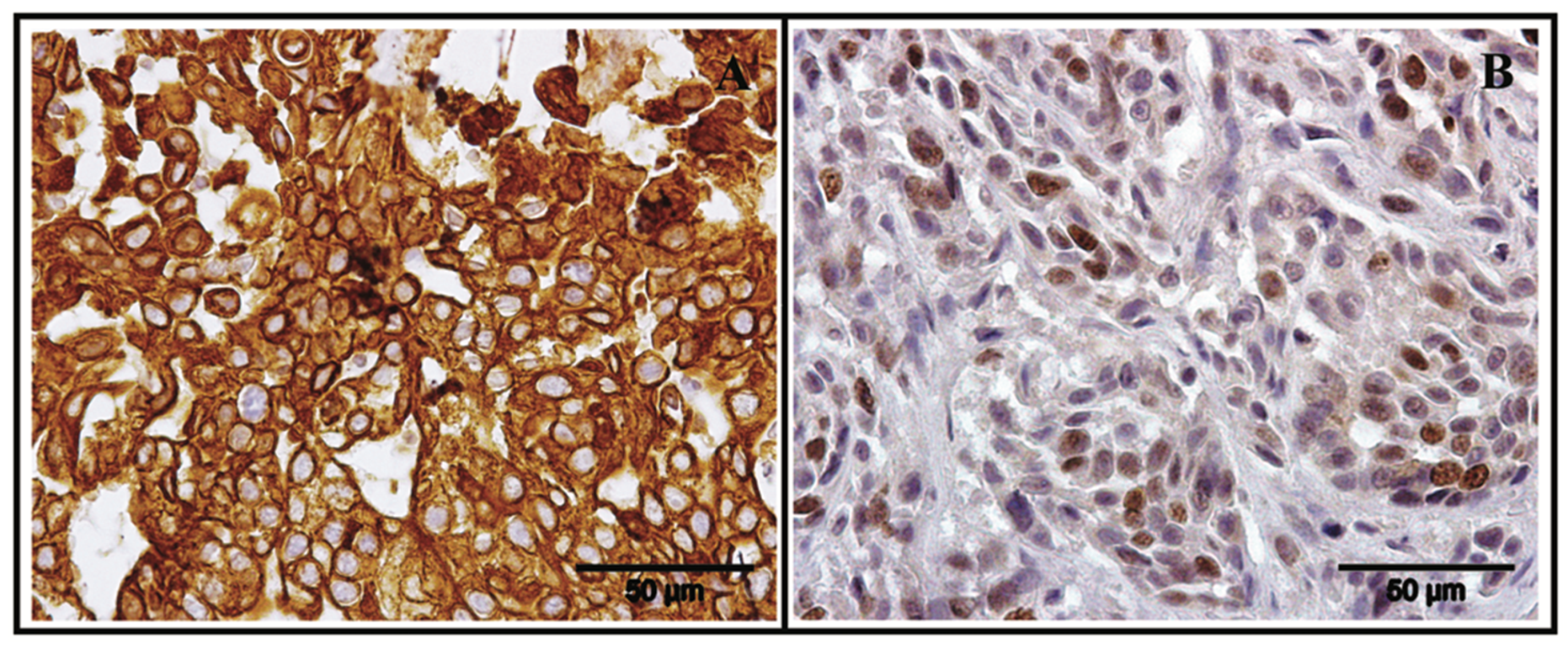
Strong staining for pan-cytokeratin in the cell membrane confirmed the epithelial nature of the tumor cells (Figure 3A), while a 0.19 Ki-67 value indicated a fast rate of cell growth and confirmed the aggressive nature of the tumor [16] (Figure 3B).
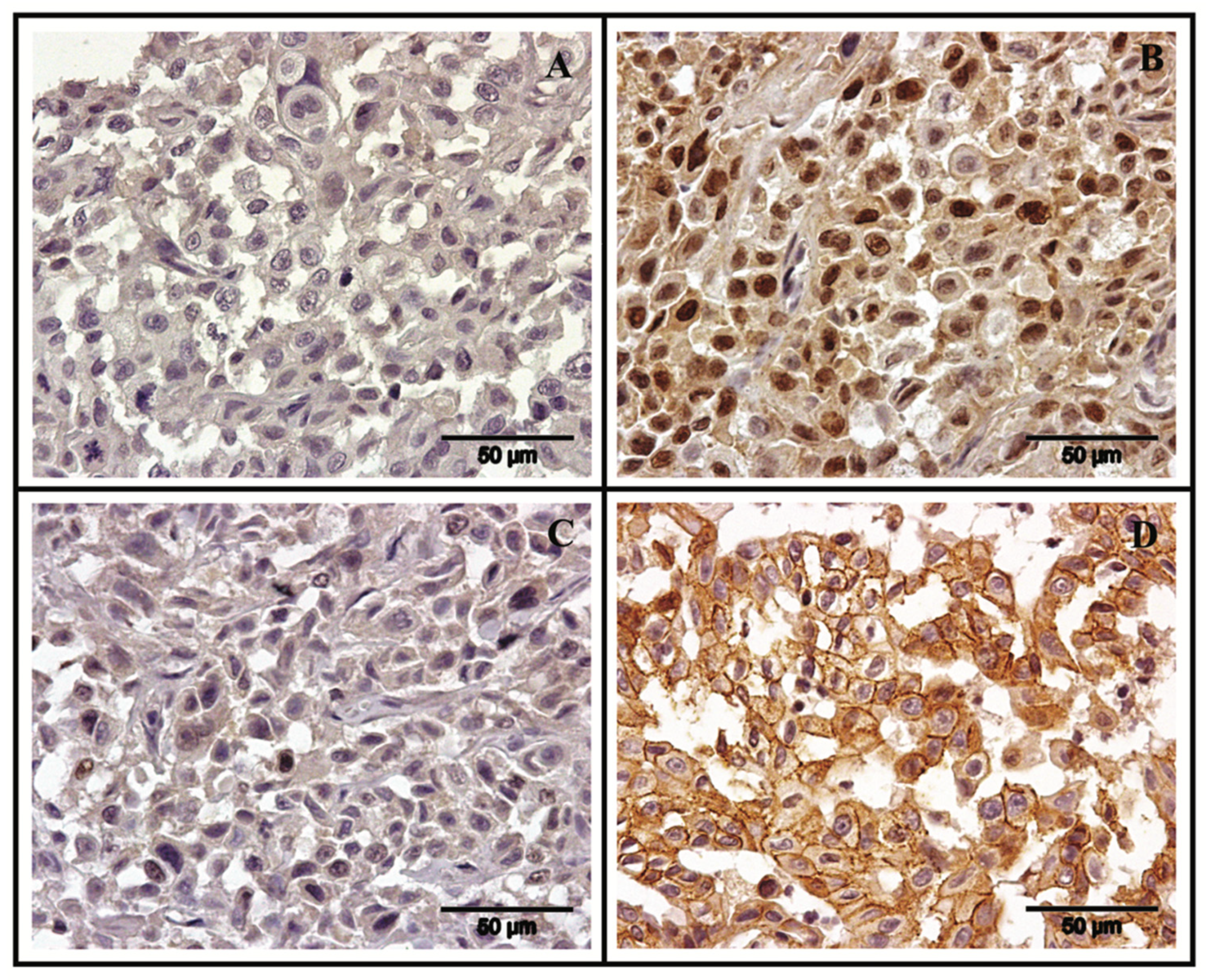
Regarding the immunohistochemistry results, the primary tumor and the regional metastatic lesions were negative for ER-α and positive for PR (Figure 4A,B), while the distant metastasis (pancreas, lung, right kidney and right suprascapular muscle) were negative for both hormone receptors (Figure 4C), according to the American Society of Clinical Oncology (ASCO) guidelines [17]. Concerning HER-2 expression, primary and metastatic lesions showed a strong and complete membrane staining in more than 30% of tumor cells (Figure 4D), scored as 2+ in accordance with the guidelines of the ASCO [18]. The COX-2 expression in the primary mass was scored as 1+ (cytoplasmic staining in < 10% of tumor cells) corresponding to a weak immunoreactivity [14].
5. Discussion
Based on the clinical evolution and the histopathological exam, the tumor herein described was considered compatible with an anaplastic mammary carcinoma (AMC). In the dog, its main features include high infiltrative capacity associated with frequent lymphatic vessels invasion, leading to regional lymph node and lung metastasis [19,20], with radiographic evaluation usually detecting an interstitial lung pattern [19], as reported in this case. Moreover, the AMC type is characterized by the presence of multinucleated cells together with large, pleomorphic cells with bizarre nuclei varying in size and usually chromatin enriched. Both anisokaryosis and anisocytosis were observed, and mitoses were common events (8–10 dividing-cells were observed per each high magnification field, 40×). Frequently, the neoplastic cells are both presented individually and grouped in small nests and the tumor tissues can be infiltrated by lymphocytes, plasma cells, mast cells, neutrophils, eosinophils and macrophages [19,20,21]. All the above anaplastic mammary carcinoma features are very similar to those reported in the presented case. Additionally, the tumor was poorly differentiated, which is frequently observed in this type of neoplasm and often requires the evaluation of protein markers, like cytokeratins, to prove the epithelial cellular origin.
In human oncology, determination of ER-α, PR and HER2 status is routinely performed, and has an important prognostic and predictive value together with the Ki-67 index. The expression of ER-α and PR are usually associated with a better prognosis, and patients whose biopsies show positive staining for these receptors are eligible for hormonal therapy. In contrast, human breast HER2-positive tumors, usually negative for ER-α and PR expressions are correlated with a worse prognosis, and have a specific target therapy with an anti-HER2 monoclonal antibody [22]. In veterinary oncology, the significance of this classification is not well defined, but HER2 status has been associated with a shorter overall survival lifespan in feline mammary carcinoma cases [23]. Regarding the presented case and considering the high cellular proliferation index and the HER-2 overexpression, this tumor also showed morphologic and immunohistochemical characteristics usually associated with an aggressive tumor behavior with poor outcome [22,23]. Moreover, we have identified a different molecular pattern in the tumor cells of the distant metastases, namely a loss of PR staining, which is also reported in human cases as being correlated with a less favorable prognosis [2]. Accordingly, previous studies in canine and feline medicine described a progressive down expression of hormone receptors in metastases [24,25,26].
Finally, the tumor described in this case report could have been classified as inflammatory, like mammary carcinoma because of the clinical presentation, such as the fulminant clinical course, the oedema, erythema, firmness, and hyperthermia of the mammary glands. However, the inflammatory carcinoma differs from other carcinomas due to repeated tumor embolization in the lymphatic vessels considered a specific hallmark of this mammary tumor type [27,28]. In fact, massive embolization of neoplastic cells in the dermal lymphatic vessels was not observed. Additionally, it was considered relevant to analyze the expression of COX-2 (that showed a 1+ score), a feature that needs to be evaluated in future AMC studies.
6. Conclusions
In our opinion, this report emphasizes the importance of using both histopathological and molecular markers to correctly establish the diagnosis and the prognosis, providing new information concerning feline mammary carcinomas. Although feline AMC is rare, we consider that the increase in the longevity will lead to higher incidence of this tumor type. Therefore, clinical veterinarians must be aware of the possible occurrence of this tumor, suspecting it in cases of neoplasms with extremely rapid growth and with evident signs of high malignancy, such as skin ulceration, adhesion to surrounded tissues (skin and muscle) and development of depressed central zone due to tumor necrosis. In case of suspecting an AMC, the clinical veterinarian should start the treatment urgently and perform an adequate chemotherapy protocol for this aggressive cancer.
Author Contributions
Conceptualization, M.S., J.C. and F.F.; methodology, M.S. and J.C.; investigation, M.S. and J.C.; writing—original draft preparation, M.S., J.C. and F.F.; writing—review and editing, M.S., J.C., C.N. and F.F.; supervision, F.F.; project administration, F.F.; funding acquisition, F.F. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by Fundação para a Ciência e a Tecnologia (Portugal), through the projects PTDC/CVT-EPI/3638/2014 and UIDB/00276/2020. C.N. is receipt of a PhD fellowship from University of Lisbon (ref.C00191r). Presentation at Meetings: A poster of this work was presented at the 30th Meeting of the European Society of Veterinary Pathology and Annual Meeting of the European College of Veterinary Pathologists (ESVP/ECVP) 2012 Congress, León, Spain, on 5–8 September 2012.
Institutional Review Board Statement
Ethical review and approval were waived for this study, as there was no interference with animal well-being.
Informed Consent Statement
Not applicable.
Data Availability Statement
Data sharing not applicable.
Conflicts of Interest
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results.
References
- Soares, M.; Madeira, S.; Correia, J.; Peleteiro, M.; Cardoso, F.; Ferreira, F. Molecular based subtyping of feline mammary carcinomas and clinicopathological characterization. Breast 2016, 27, 44–51. [Google Scholar] [CrossRef]
- Della Salda, L.; Sarli, G.; Benazzi, C.; Marcato, P.S. Giant Cells in anaplastic mammary carcinoma of the dog and cat. J. Comp. Pathol. 1993, 109, 345–360. [Google Scholar] [CrossRef]
- Bostock, D.E.; Moriarty, J.; Crocker, J. Correlation between Histologic Diagnosis Mean Nucleolar Organizer Region Count and Prognosis in Canine Mammary Tumors. Vet. Pathol. 1992, 29, 381–385. [Google Scholar] [CrossRef]
- Bostock, D.E. Canine and Feline Mammary Neoplasms. Br. Vet. J. 1986, 142, 506–515. [Google Scholar] [CrossRef]
- Brearley, M. Mammary gland tumours in the dog. Practice 1989, 11, 248–253. [Google Scholar] [CrossRef]
- Meuten, D. Tumors in Domestic Animals, 5th ed.; John Wiley & Sons Inc.: Ames, IA, USA, 2017. [Google Scholar]
- Cowell, R.L.; Tyler, R.D.; Meinkoth, J.H.; DeNicola, D.B. Diagnostic Cytology and Hematology of the Dog and Cat, 3rd ed.; Elsevier Health Sciences: St Louis, MO, USA, 2007. [Google Scholar]
- Misdorp, W. Tumors of the mammary gland. In Tumors in Domestic Animals, 4th ed.; Iowa State Press: Ames, IA, USA, 2002. [Google Scholar]
- Misdorp, W. Histological classification of mammary tumors of the dog and the cat. In World Health Organization International Histological Classification of Tumours of Domestic Animals, 2nd ed.; Armed Force Institute of Pathology: Washington, DC, USA; World Health Organization: Geneva, Switzerland, 1999; Volume 7, pp. 11–27. [Google Scholar]
- Soares, M.; Ribeiro, R.; Carvalho, S.; Peleteiro, M.; Correia, J.; Ferreira, F. Ki-67 as a Prognostic Factor in Feline Mammary Carcinoma: What Is the Optimal Cutoff Value? Vet. Pathol. 2016, 53, 37–43. [Google Scholar] [CrossRef] [Green Version]
- Burrai, G.P.; Mohammed, S.I.; Miller, M.A.; Marras, V.; Pirino, S.; Addis, M.F.; Uzzau, S.; Antuofermo, E. Spontaneous feline mammary intraepithelial lesions as a model for human estrogen receptor- and progesterone receptor-negative breast lesions. BMC Cancer 2010, 10, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soares, M.; Correia, J.; Rodrigues, P.; Simões, M.; Matos, A.; Ferreira, F. Feline HER2 Protein Expression Levels and Gene Status in Feline Mammary Carcinoma: Optimization of Immunohistochemistry (IHC) and In Situ Hybridization (ISH). Microsc. Microanal. 2013, 19, 876–882. [Google Scholar] [CrossRef] [PubMed]
- Matos, A.J.F.; Faustino, A.M.R.; Lopes, C.; Rutteman, G.R.; Gärtner, F. Detection of lymph node micrometastases malignant mammary tumours in dogs by cytokeratin immunostaining. Vet. Rec. 2006, 158, 626–630. [Google Scholar] [CrossRef]
- Millanta, F.; Citi, S.; Della Santa, D.; Porciani, M.; Poli, A. COX-2 expression in canine and feline invasive mammary carcinomas: Correlation with clinicopathological features and prognostic fmolecular markers. Breast Cancer Res. Treat. 2006, 98, 115–120. [Google Scholar] [CrossRef] [PubMed]
- Veiga, G.A.L.; Miziara, R.H.; Angrimani, D.S.R.; Papa, P.C.; Cogliati, B.; Vannucchi, C.I. Cystic endometrial hyperplasia-pyometra syndrome in bitches: Identification of hemodynamic, inflammatory, and cell proliferation changes. Biol. Reprod. 2017, 96, 58–69. [Google Scholar]
- Yerushalmi, R.; Woods, R.; Ravdin, P.M.; Hayes, M.M.; Gelmon, K.A. Ki67 in breast cancer: Prognostic and predictive potential. Lancet Oncol. 2010, 11, 174–183. [Google Scholar] [CrossRef]
- Hammond, M.E.H.; Hayes, D.F.; Wolff, A.C.; Mangu, P.B.; Temin, S. American Society of Clinical Oncology/College of American Pathologists guideline recommendations for immunohistochemical testing of estrogen and progesterone receptors in breast cancer. J. Oncol. Pract. 2010, 6, 195–197. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wolff, A.C.; Hammond, M.E.H.; Schwartz, J.N.; Hagerty, K.L.; Allred, D.C.; Cote, R.J.; Dowsett, M.; Fitzgibbons, P.L.; Hanna, W.M.; Langer, A.; et al. American Society of Clinical Oncology/College of American Pathologists guideline recommendations for human epidermal growth factor receptor 2 testing in breast cancer. J. Clin. Oncol. 2007, 25, 118–145. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goldschmidt, M.H.; Peña, L.; Rasotto, R.; Zappulli, V. Classification and grading of canine mammary tumors. Vet. Pathol. 2011, 48, 117–131. [Google Scholar] [CrossRef]
- Losco, P.E. Local and Peripheral Eosinophilia in a Dog with Anaplastic Mammary Carcinoma. Vet. Pathol. 1986, 23, 536–538. [Google Scholar] [CrossRef]
- Eroles, P.; Bosch, A.; Alejandro Pérez-Fidalgo, J.; Lluch, A. Molecular biology in breast cancer: Intrinsic subtypes and signaling pathways. Cancer Treat. Rev. 2012, 38, 698–707. [Google Scholar] [CrossRef]
- Millanta, F.; Calandrella, M.; Citi, S.; Della Santa, D.; Poli, A. Overexpression of HER-2 in feline invasive mammary carcinomas: An immunohistochemical survey and evaluation of its prognostic potential. Vet. Pathol. 2005, 42, 30–34. [Google Scholar] [CrossRef]
- Bogina, G.; Bortesi, L.; Marconi, M.; Venturini, M.; Lunardi, G.; Coati, F.; Massocco, A.; Manfrin, E.; Pegoraro, C.; Zamboni, G. Comparison of hormonal receptor and HER-2 status between breast primary tumours and relapsing tumours: Clinical implications of progesterone receptor loss. Virchows Arch. 2011, 459, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beha, G.; Muscatello, L.V.; Brunetti, B.; Asproni, P.; Millanta, F.; Poli, A.; Benazzi, C.; Sarli, G. Molecular phenotype of primary mammary tumours and distant metastases in female dogs and cats. J. Comp. Pathol. 2014, 150, 194–197. [Google Scholar] [CrossRef]
- Brunetti, B.; Asproni, P.; Beha, G.; Muscatello, L.V.; Millanta, F.; Poli, A.; Benazzi, C.; Sarli, G. Molecular Phenotype in Mammary Tumours of Queens: Correlation between Primary Tumour and Lymph Node Metastasis. J. Comp. Pathol. 2013, 148, 206–213. [Google Scholar] [CrossRef] [PubMed]
- Beha, G.; Brunetti, B.; Asproni, P.; Muscatello, L.V.; Millanta, F.; Poli, A.; Sarli, G.; Benazzi, C. Molecular portrait-based correlation between primary canine mammary tumor and its lymph node metastasis: Possible prognostic-predictive models and/or stronghold for specific treatments? BMC Vet. Res. 2012, 8, 219. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pérez-Alenza, M.D.; Jiménez, A.; Nieto, A.I.; Peña, L. First description of feline inflammatory mammary carcinoma: Clinicopathological and immunohistochemical characteristics of three cases. Breast Cancer Res. 2004, 6, 300–307. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Millanta, F.; Verin, R.; Asproni, P.; Giannetti, G.; Poli, A. A case of feline primary inflammatory mammary carcinoma: Clinicopathological and immunohistochemical findings. J. Feline Med. Surg. 2012, 14, 420–423. [Google Scholar] [CrossRef]
Figure 1.
Fine needle aspiration cytology of the right inguinal mammary lesion. The tumor cells were frequently multinucleated and showed marked anisocytosis, anisokaryosis and multiple prominent nucleoli, indicating a high degree of malignancy. Inflammatory cells, particularly neutrophils and lymphocytes, were frequently observed (Giemsa counterstain, 40×).
Figure 1.
Fine needle aspiration cytology of the right inguinal mammary lesion. The tumor cells were frequently multinucleated and showed marked anisocytosis, anisokaryosis and multiple prominent nucleoli, indicating a high degree of malignancy. Inflammatory cells, particularly neutrophils and lymphocytes, were frequently observed (Giemsa counterstain, 40×).

Figure 2.
(A) Primary mammary tumor tissue with vascular invasion by neoplastic cells (H&E staining, 40×); (B) Necrosis affecting large areas of the tumor (H&E, 40×); (C) Neoplastic cells are frequently individualized or arranged in small nests surrounded by dense and abundant collagen fibers (desmoplasia) (H&E staining, 40×); (D) Giant and multinucleated cells (arrowheads) were frequently present, and severe anisokaryosis and anisocytosis were common. The nuclei were irregularly shaped with occasional indentations or convolutions present and had coarsely stippled chromatin (H&E, 40×). (E) Lung and (F) supra renal metastases of primary mammary tumor (H&E staining, 4×).
Figure 2.
(A) Primary mammary tumor tissue with vascular invasion by neoplastic cells (H&E staining, 40×); (B) Necrosis affecting large areas of the tumor (H&E, 40×); (C) Neoplastic cells are frequently individualized or arranged in small nests surrounded by dense and abundant collagen fibers (desmoplasia) (H&E staining, 40×); (D) Giant and multinucleated cells (arrowheads) were frequently present, and severe anisokaryosis and anisocytosis were common. The nuclei were irregularly shaped with occasional indentations or convolutions present and had coarsely stippled chromatin (H&E, 40×). (E) Lung and (F) supra renal metastases of primary mammary tumor (H&E staining, 4×).

Figure 3.
(A) Intense membrane pan-cytokeratin immunostaining in the primary mammary mass (chromogen diaminobenzidine, Mayer’s hematoxylin counterstain, 40× magnification); (B) Nuclear Ki-67 immunostaining (0.19 index) (chromogen diaminobenzidine, Mayer’s hematoxylin counterstain, 40×).
Figure 3.
(A) Intense membrane pan-cytokeratin immunostaining in the primary mammary mass (chromogen diaminobenzidine, Mayer’s hematoxylin counterstain, 40× magnification); (B) Nuclear Ki-67 immunostaining (0.19 index) (chromogen diaminobenzidine, Mayer’s hematoxylin counterstain, 40×).

Figure 4.
Primary and metastatic tumor immunophenotyping (chromogen diaminobenzidine, Mayer’s hematoxylin counterstain, 40×). (A) Primary tumor stained negative for ER; (B) PR positive staining was observed in more than 10% of tumor cells present in a metastatic lesion of the regional inguinal lymph node; (C) Negative immunostaining for PR expression in distant metastases (suprascapular muscle); (D) HER-2 positive immunostaining (scored 2+) is shown. A moderate, complete membrane staining pattern of non-uniform intensity was observed in more than 10% of the tumor cells in the primary tumor.
Figure 4.
Primary and metastatic tumor immunophenotyping (chromogen diaminobenzidine, Mayer’s hematoxylin counterstain, 40×). (A) Primary tumor stained negative for ER; (B) PR positive staining was observed in more than 10% of tumor cells present in a metastatic lesion of the regional inguinal lymph node; (C) Negative immunostaining for PR expression in distant metastases (suprascapular muscle); (D) HER-2 positive immunostaining (scored 2+) is shown. A moderate, complete membrane staining pattern of non-uniform intensity was observed in more than 10% of the tumor cells in the primary tumor.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
Primary antibodies and immunostaining protocols used.
| Antigen | Primary Antibody | Dilution | Incubation | Antigen Retrieval Method |
|---|---|---|---|---|
| Cytokeratins | clone AE1/AE3 (DAKO) | 1:100 | 60 min, RT | Microwave 900 W 5′ + 600 W 15′ with buffer solution at pH 9,0 (Tris EDTA pH 9.0, Novocastra™ Epitope Retrieval Solution) |
| Ki-67 | clone MM1 (Leica) | 1:100 | 60 min, RT | Pressure chamber (2 atm during 2 min), citrate buffer solution (pH 6.0) |
| ER-α | clone SP1 (Ventana) | 1:150 | 16 h, 4 °C | |
| HER-2 | clone A0485 (DAKO) | 1:300 | 60 min, RT | Boiling water bath (95 °C, 60 min), citrate buffer solution (pH 6.0) |
| PR | clone 1E2 (Ventana) | RTU | 16 h, 4 °C | |
| COX-2 | clone SP21 (Biocare Medical) | 1:75 | 16 h, 4 °C | Pressure chamber (2 atm during 2 min), citrate buffer solution (pH 6.0) |
RT, Room temperature; RTU, ready-to-use.
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Soares, M.; Correia, J.; Nascimento, C.; Ferreira, F. Anaplastic Mammary Carcinoma in Cat. Vet. Sci. 2021, 8, 77. https://0-doi-org.brum.beds.ac.uk/10.3390/vetsci8050077
AMA Style
Soares M, Correia J, Nascimento C, Ferreira F. Anaplastic Mammary Carcinoma in Cat. Veterinary Sciences. 2021; 8(5):77. https://0-doi-org.brum.beds.ac.uk/10.3390/vetsci8050077
Chicago/Turabian StyleSoares, Maria, Jorge Correia, Catarina Nascimento, and Fernando Ferreira. 2021. "Anaplastic Mammary Carcinoma in Cat" Veterinary Sciences 8, no. 5: 77. https://0-doi-org.brum.beds.ac.uk/10.3390/vetsci8050077
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.