
Diagnostic Accuracy of the Overlapping Infinity Loops, Wire Cube, and Clock Drawing Tests in Subjective Cognitive Decline, Mild Cognitive Impairment and Dementia

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participant Recruitment
2.2. Clinical Diagnosis
2.3. Control Group
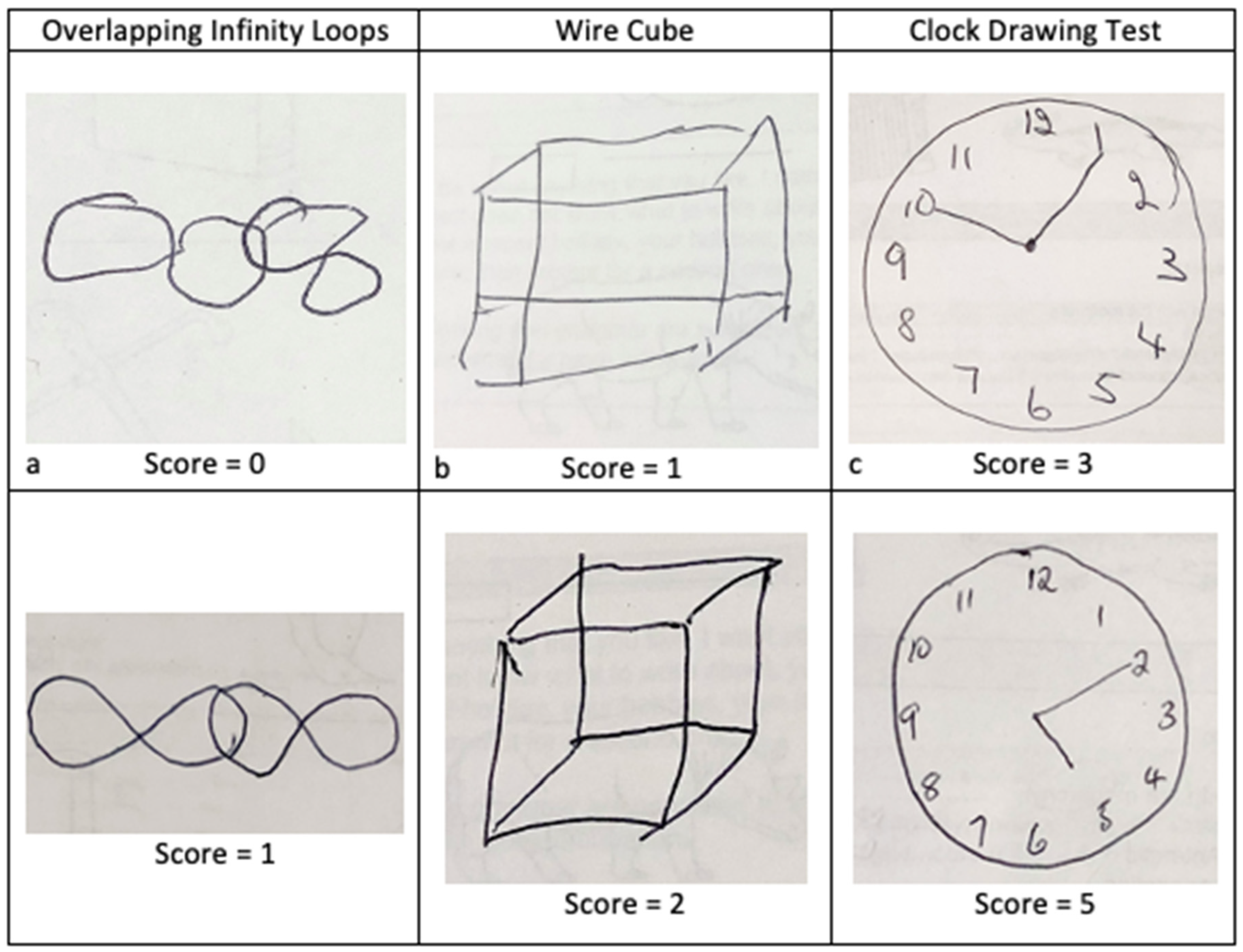
2.4. Figure Drawing Tests
2.5. Statistical Analysis
3. Results
3.1. Participant Demographics and Clinical Diagnosis
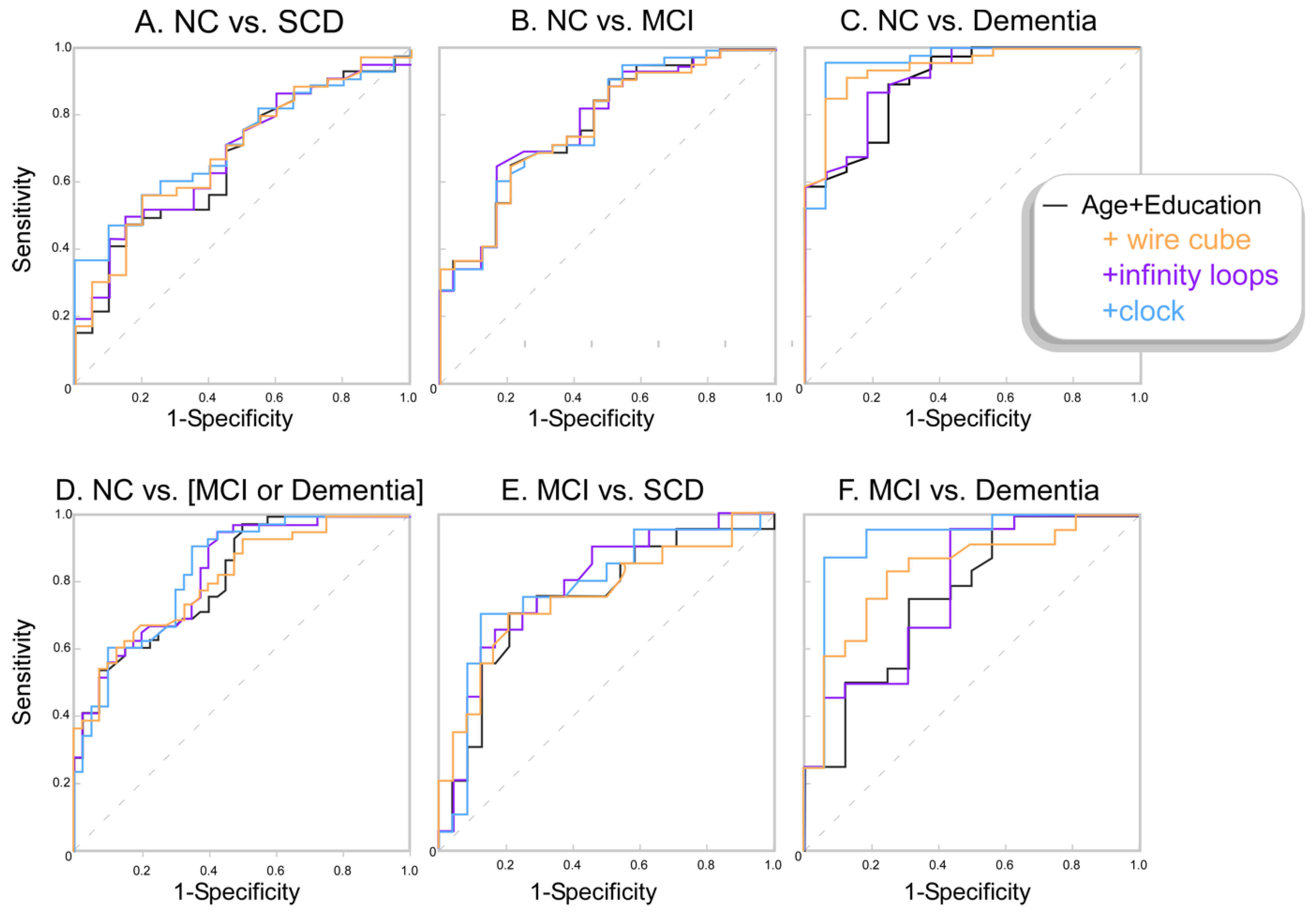
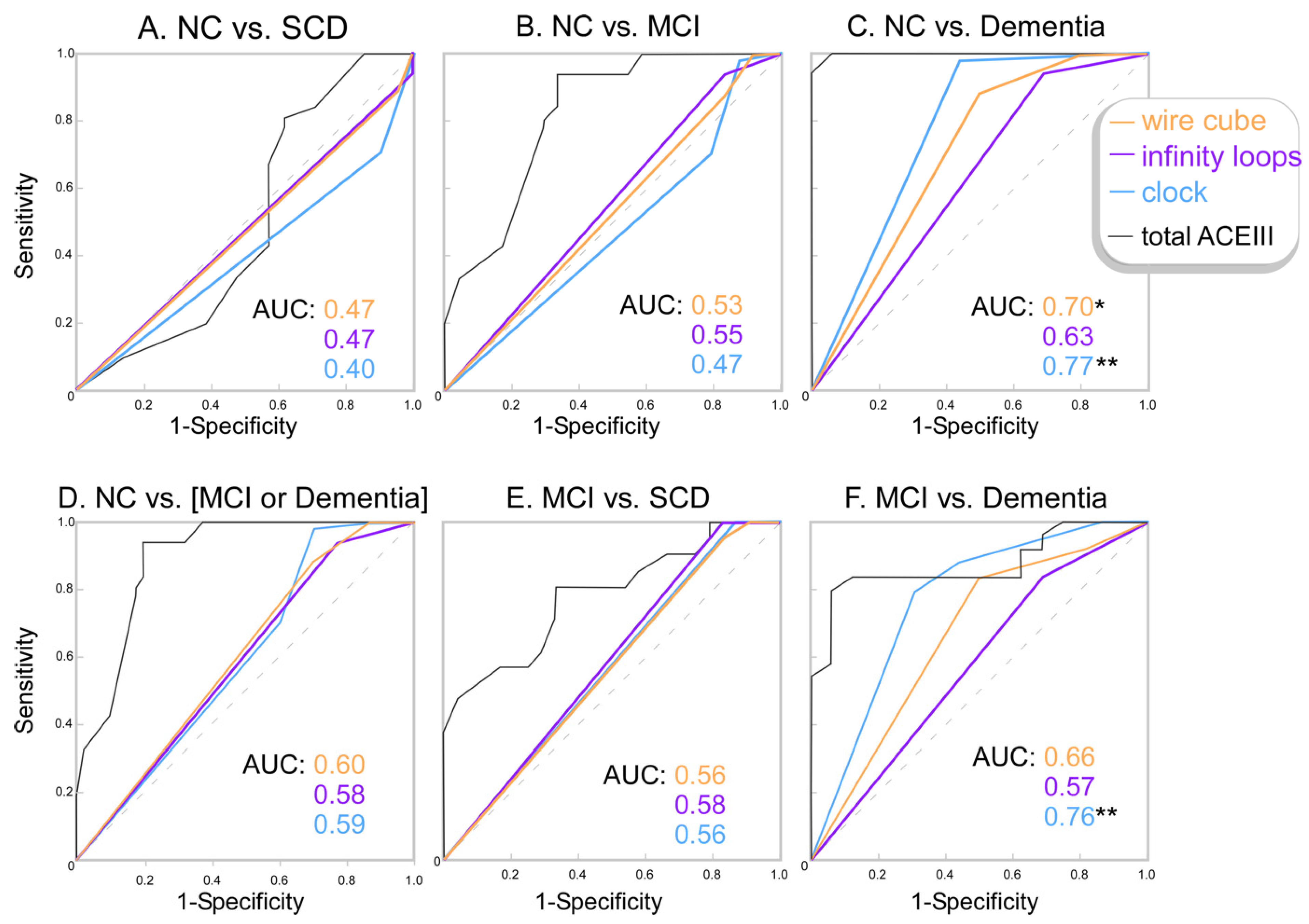
3.2. Figure Drawing Task Discriminatory Capacity
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bruno, D.; Schurmann Vignaga, S. Addenbrooke’s cognitive examination III in the diagnosis of dementia: A critical review. Neuropsychiatr. Dis. Treat. 2019, 15, 441–447. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Talwar, N.A.; Churchill, N.W.; Hird, M.A.; Pshonyak, I.; Tam, F.; Fischer, C.E.; Graham, S.J.; Schweizer, T.A. The neural correlates of the clock-drawing test in healthy aging. Front. Hum. Neurosci. 2019, 13, 25. [Google Scholar] [CrossRef] [PubMed]
- Salimi, S.; Irish, M.; Foxe, D.; Hodges, J.R.; Piguet, O.; Burrell, J.R. Can visuospatial measures improve the diagnosis of Alzheimer’s disease? Alzheimer Dement. Diagn. Assess. Dis. Monit. 2017, 6, 66–74. [Google Scholar] [CrossRef]
- Ahmed, S.; Brennan, L.; Eppig, J.; Price, C.C.; Lamar, M.; Delano-Wood, L.; Bangen, K.J.; Edmonds, E.C.; Clark, L.; Nation, D.A.; et al. Visuoconstructional impairment in subtypes of mild cognitive impairment. Appl. Neuropsychol. Adult 2016, 23, 43–52. [Google Scholar] [CrossRef] [Green Version]
- Buckner, R.L.; Snyder, A.Z.; Shannon, B.J.; LaRossa, G.; Sachs, R.; Fotenos, A.F.; Sheline, Y.I.; Klunk, W.; Mathis, C.A.; Morris, J.C.; et al. Molecular, structural and functional characterization of Alzheimer’s disease: Evidence for a relationship between default activity, amyloid and memory. J. Neurosci. 2005, 24, 7709–7717. [Google Scholar] [CrossRef] [Green Version]
- Jagust, W.J.; Eberling, J.L.; Reed, B.R.; Mathis, C.A.; Budinger, T.F. Clinical studies of cerebral blood flow in Alzheimer’s disease. Ann. N. Y. Acad. Sci. 1997, 26, 254–262. [Google Scholar] [CrossRef]
- Bat, B.K.; Chan, J.Y.; Chan, T.K.; Huo, Z.; Yip, B.H.; Wong, M.C.; Tsoi, K.K. Comparing drawing under instructions with image copying for mild cognitive impairment (MCI) or dementia screening: A meta-analysis of 92 diagnostic studies. Aging Ment. Health 2022, 26, 1019–1026. [Google Scholar] [CrossRef]
- Chan, J.Y.C.; Bat, B.K.K.; Wong, A.; Chan, T.K.; Huo, Z.; Yip, B.H.K.; Kowk, T.C.Y.; Tsoi, K.K.F. Evaluation of digital drawing tests and paper-and-pencil drawing tests for the screening of mild cognitive impairment and dementia: A systematic review and meta-analysis of diagnostic studies. Neuropsychol. Rev. 2021. [Google Scholar] [CrossRef]
- Charernboon, T. Diagnostic accuracy of the overlapping infinity loops, wire cube, and clock drawing tests for cognitive impairment in mild cognitive impairment and dementia. Int. J. Alzheime. Dis. 2017, 2017, 5289239. [Google Scholar] [CrossRef] [Green Version]
- Jessen, F.; Amariglio, R.E.; van Boxtel, M.; Breteler, M.; Ceccaldi, M.; Chételat, G.; Dubois, B.; Dufouil, C.; Ellis, K.A.; van der Flier, W.M.; et al. A conceptual framework for research on subjective cognitive decline in preclinical Alzheimer’s disease. Alzheime. Dement. 2014, 10, 844–852. [Google Scholar] [CrossRef] [Green Version]
- Seo, E.H.; Kim, H.; Choi, K.Y.; Lee, K.H.; Choo, I.H. Pre-mild cognitive impairment: Can visual memory predict who rapidly convert to mild cognitive impairment? Psychiatry Investig. 2018, 15, 869–875. [Google Scholar] [CrossRef] [PubMed]
- Mathuranath, P.S.; Nestor, P.J.; Berrios, G.E.; Rakowicz, W.; Hodges, J.R. A brief cognitive test battery to differentiate Alzheimer’s disease and frontotemporal dementia. Neurology 2000, 55, 1613–1620. [Google Scholar] [CrossRef] [PubMed]
- Alty, J.E.; Cosgrove, J.; Jamieson, S.; Smith, S.L.; Possin, K.L. Which figure copy test is more sensitive to cognitive impairment in Parkinson’s disease: Wire cube or interlocking pentagons? Clin. Neurol. Neurosurg. 2015, 139, 244–246. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, S.; Chen, L.; Jin, X.; Yan, J.; Xu, S.; Xu, Y.; Liu, C.; Jin, Y. Effects of age and education on clock-drawing performance by elderly adults in China. Clin. Neuropsychol. 2019, 33, 96–105. [Google Scholar] [CrossRef]
- Gaestel, Y.; Amieva, H.; Letenneur, L.; Dartigues, J.-F.; Fabrigoule, C. Cube drawing performance in normal ageing and Alzheimer’s disease: Data from the PAQUID elderly population-based cohort. Dement. Geriatr. Cogn. Disord. 2006, 21, 22–32. [Google Scholar] [CrossRef]
- Yoshimura, T.; Osawa, A.; Maeshima, S. Assessment of cube-copying among community-dwelling elderly living in Japan using the vertex criterion and parallelism. Psychogeriatrics 2021, 21, 722–729. [Google Scholar] [CrossRef]
- Winblad, B.; Palmer, K.; Kivipelto, M.; Jelic, V.; Fratiglioni, L.; Wahlund, L.-O.; Nordberg, A.; Backman, L.J.; Albert, M.S.; Almkvist, O.; et al. Mild cognitive impairment—Beyond controversies, towards a consensus: Report of the International Working Group on mild cognitive impairment. J. Intern. Med. 2004, 256, 240–246. [Google Scholar] [CrossRef]
- McKhann, G.M.; Knopman, D.S.; Chertkow, H.; Hyman, B.T.; Jack, C.R., Jr.; Kawas, C.H.; Klunk, W.E.; Koroshetz, W.J.; Manly, J.J.; Mayeux, R.; et al. The diagnosis of dementia due to Alzheimer’s disease: Recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheime. Dement. 2011, 7, 263–269. [Google Scholar] [CrossRef] [Green Version]
- Bartlett, L.; Doherty, K.; Farrow, M.; Kim, S.; Hill, E.; King, A.; Alty, J.; Eccleston, C.; Kitsos, A.; Bindoff, A.; et al. Island study linking aging and neurodegenerative disease (ISLAND) targeting dementia risk reduction: Protocol for a prospective web-based cohort study. JMIR Res. Protoc. 2022, 11, e34688. [Google Scholar] [CrossRef]
- Zarantonello, L.; Schiff, S.; Amodio, P.; Bisiacchi, P. The effect of age, educational level, gender and cognitive reserve on visuospatial working memory performance across adult life span. Neuropsychol. Dev. Cogn. B Aging Neuropsychol. Cogn. 2020, 27, 302–319. [Google Scholar] [CrossRef]
- Ferguson, H.J.; Brunsdon, V.E.A.; Bradford, E.E.F. The developmental trajectories of executive function from adolescence to old age. Sci Rep. 2021, 11, 1382. [Google Scholar] [CrossRef] [PubMed]
- Seidler, R.D.; Bernard, J.A.; Burutolu, T.B.; Fling, B.W.; Gordon, M.T.; Gwin, J.T.; Kwak, Y.; Lipps, D.B. Motor control and aging: Links to age-related brain structural, functional, and biochemical effects. Neurosci. Biobehav. Rev. 2010, 34, 721–733. [Google Scholar] [CrossRef] [Green Version]
- Maher, C.; Calia, C. The effect of illiteracy on performance in screening tools for dementia: A meta-analysis. J. Clin. Exp. Neuropsychol. 2021, 43, 945–966. [Google Scholar] [CrossRef] [PubMed]
- Stern, Y. Cognitive reserve. Neuropsychologia 2009, 47, 2015–2028. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.; Chey, J. Effects of education, literacy, and dementia on the clock drawing test performance. J. Int. Neuropsychol. Soc. 2010, 16, 1138–1146. [Google Scholar] [CrossRef]
- Ehreke, L.; Luck, T.; Luppa, M.; König, H.-H.; Villringer, A.; Riedel-Heller, S.G. Clock drawing test—Screening utility for mild cognitive impairment according to different scoring systems: Results of the Leipzig Longitudinal Study of the Aged (LEILA 75+). Int. Psychogeriatr. 2011, 23, 1592–1601. [Google Scholar] [CrossRef]
- Ehreke, L.; Luppa, M.; König, H.-H.; Riedel-Heller, S.G. Is the clock drawing test a screening tool for the diagnosis of mild cognitive impairment? A systematic review. Int. Psychogeriatr. 2009, 22, 56–63. [Google Scholar] [CrossRef]
- Amodeo, S.; Mainland, B.J.; Herrmann, N.; Shulman, K.I. The times they are a-changin’: Clock drawing and prediction of dementia. J. Geriatr. Psychiatry Neurol. 2015, 28, 145–155. [Google Scholar] [CrossRef]
- Pike, K.E.; Cavuoto, M.G.; Li, L.; Wright, B.J.; Kinsella, G.J. Subjective cognitive decline: Level of risk for future dementia and mild cognitive impairment, a meta-analysis of longitudinal studies. Neuropsychol. Rev. 2021. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| NC | SCD | MCI | Dementia | p-Value | |
|---|---|---|---|---|---|
| n | 51 | 21 | 24 | 16 | |
| Age (years): mean (SD) | 67.47 (7.63) | 65.48 (9.38) | 68.50 (10.24) | 77.25 (7.38) # | <0.01 |
| Male (%) | 25.49 | 28.57 | 41.67 | 31.25 | 0.56 |
| Total years of education: mean (SD) | 16.24 (3.80) | 15.05 (3.73) | 12.33 (3.16) * | 10.56 (2.56) * | <0.01 |
| Total ACE-III score: mean (SD) [range] | 95.98 (2.87) [89–100] | 95.05 (5.06) [84–100] | 88.00 (8.72) # [69–98] | 73.38 (9.00) # [56–89] | <0.01 |
| Letters score: mean (SD) [range] | 5.98 (1.29) [2–7] | 5.95 (1.43) [1–7] | 5.46 (1.69) [0–7] | 3.73 (2.02) # [0–7] | 0.01 |
| Animals score: mean (SD) [range] | 6.18 (0.95) [4–7] | 6.24 (1.14) [2–7] | 5.08 (2.06) [0–7] | 3.80 (1.61) # [0–6] | <0.01 |
| Dot counting score: mean (SD) [range] | 3.94 (0.24) [3,4] | 4.00 (0) [0] | 3.92 (0.28) [3,4] | 3.80 (0.56) [2–4] | 0.23 |
| Letter identification score: mean (SD) [range] | 4.00 (0) [0] | 4.00 (0) [0] | 4.00 (0) [0] | 4.00 (0) [0] | NA |
| % correctly completing infinity loops | 94.12 | 100.00 | 83.33 | 68.75 | |
| % correctly completing wire cube | 88.24 | 95.24 | 83.34 | 50.00 | |
| % correctly completing CDT | 70.59 | 90.48 | 79.17 | 31.25 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Costa, S.; St George, R.J.; McDonald, J.S.; Wang, X.; Alty, J. Diagnostic Accuracy of the Overlapping Infinity Loops, Wire Cube, and Clock Drawing Tests in Subjective Cognitive Decline, Mild Cognitive Impairment and Dementia. Geriatrics 2022, 7, 72. https://0-doi-org.brum.beds.ac.uk/10.3390/geriatrics7040072
Costa S, St George RJ, McDonald JS, Wang X, Alty J. Diagnostic Accuracy of the Overlapping Infinity Loops, Wire Cube, and Clock Drawing Tests in Subjective Cognitive Decline, Mild Cognitive Impairment and Dementia. Geriatrics. 2022; 7(4):72. https://0-doi-org.brum.beds.ac.uk/10.3390/geriatrics7040072
Chicago/Turabian StyleCosta, Sigourney, Rebecca J. St George, James Scott McDonald, Xinyi Wang, and Jane Alty. 2022. "Diagnostic Accuracy of the Overlapping Infinity Loops, Wire Cube, and Clock Drawing Tests in Subjective Cognitive Decline, Mild Cognitive Impairment and Dementia" Geriatrics 7, no. 4: 72. https://0-doi-org.brum.beds.ac.uk/10.3390/geriatrics7040072