
The Role of Cognitive Performance and Physical Functions in the Association between Age and Gait Speed: A Mediation Study

 ,
,  , , ,
, , ,  and
and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Design and Participants
2.2. Data Collection
2.2.1. Demographics and Clinical Data
2.2.2. Cognitive Assessment
2.2.3. Physical Functions
2.2.4. Gait
2.2.5. Covariates
2.3. Statistical Analysis
3. Results
3.1. Main Characteristics of the Participants
3.2. Associations between CP and PF with GS
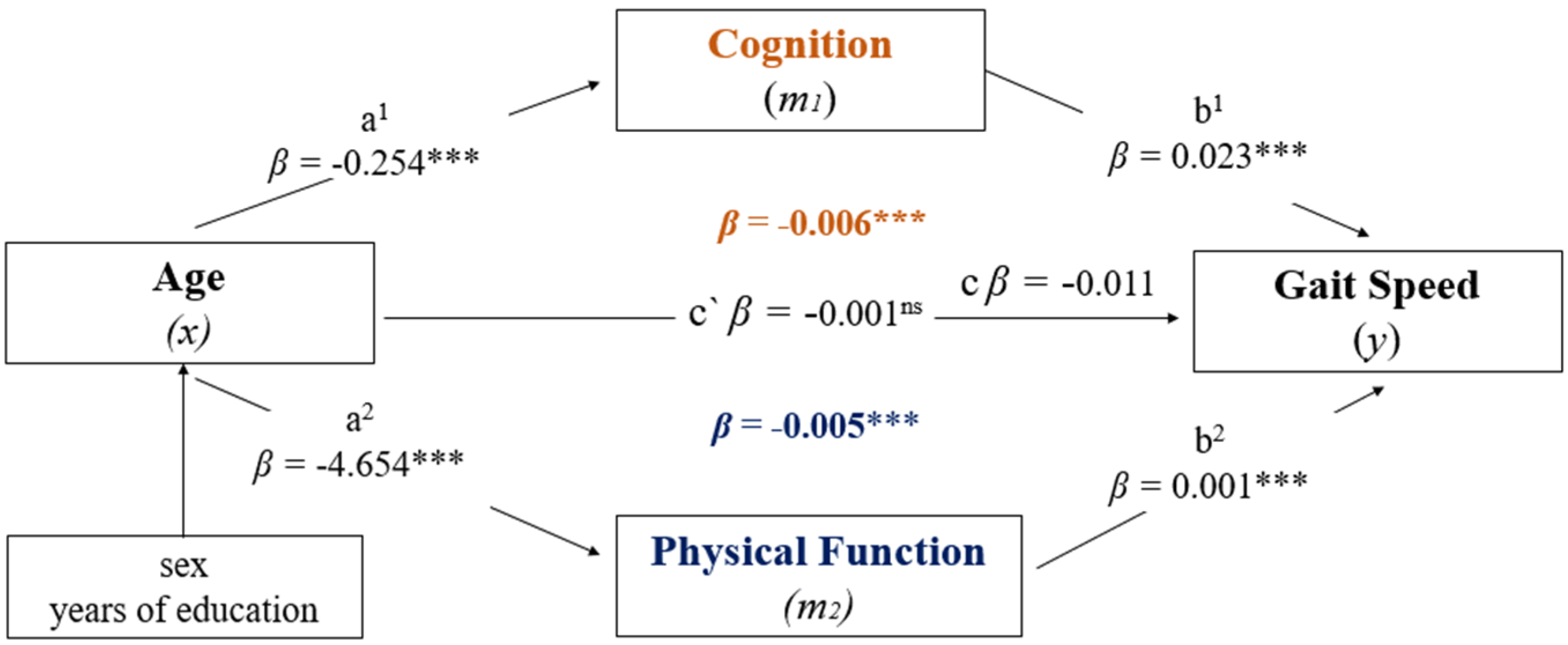
3.3. Mediation Analysis: CP and PF in the Relationship between Age and GS
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cromwell, R.L.; Newton, R.A. Relationship between Balance and Gait Stability in Healthy Older Adults. J. Aging Phys. Act. 2004, 12, 90–100. [Google Scholar] [CrossRef] [PubMed]
- Herssens, N.; Verbecque, E.; Hallemans, A.; Vereeck, L.; Van Rompaey, V.; Saeys, W. Do spatiotemporal parameters and gait variability differ across the lifespan of healthy adults? A systematic review. Gait Posture 2018, 64, 181–190. [Google Scholar] [CrossRef] [PubMed]
- Fitzpatrick, A.L.; Buchanan, C.K.; Nahin, R.L.; Dekosky, S.T.; Atkinson, H.H.; Carlson, M.C.; Williamson, J.D. Associations of gait speed and other measures of physical function with cognition in a healthy cohort of elderly persons. J. Gerontol. A Biol. Sci. Med. Sci. 2007, 62, 1244–1251. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rogers, H.L.; Cromwell, R.L.; Grady, J.L. Adaptive Changes in Gait of Older and Younger Adults as Responses to Challenges to Dynamic Balance. J. Aging Phys. Act. 2008, 16, 85–96. [Google Scholar] [CrossRef]
- Danion, F.; Varraine, E.; Bonnard, M.; Pailhous, J. Stride variability in human gait: The effect of stride frequency and stride length. Gait Posture 2003, 18, 69–77. [Google Scholar] [CrossRef]
- Kirkwood, R.N.; Araújo, P.A.; Dias, C.S. Biomecânica da marcha em idosos caidores e não caidores: Uma revisão da literatura. Rev. Bras. Ciênc. Mov. 2006, 14, 103–110. [Google Scholar]
- Martin, K.L.; Blizzard, L.; Wood, A.G.; Srikanth, V.; Thomson, R.; Sanders, L.M.; Callisaya, M.L. Cognitive Function, Gait, and Gait Variability in Older People: A Population-Based Study. J. Gerontol. Ser. A 2013, 68, 726–732. [Google Scholar] [CrossRef]
- Holtzer, R.; Verghese, J.; Xue, X.; Lipton, R.B. Cognitive processes related to gait velocity: Results from the Einstein aging study. Neuropsychology 2006, 20, 215–223. [Google Scholar] [CrossRef]
- Montero-Odasso, M.M.; Barnes, B.; Speechley, M.; Muir Hunter, S.W.; Doherty, T.J.; Duque, G.; Gopaul, K.; Sposato, L.A.; Casas-Herrero, A.; Borrie, M.J.; et al. Disentangling Cognitive-Frailty: Results From the Gait and Brain Study. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2016, 71, 1476–1482. [Google Scholar] [CrossRef] [Green Version]
- Perez-Sousa, M.A.; Venegas-Sanabria, L.C.; Chavarro-Carvajal, D.A.; Cano-Gutierrez, C.A.; Izquierdo, M.; Correa-Bautista, J.E.; Ramírez-Vélez, R. Gait speed as a mediator of the effect of sarcopenia on dependency in activities of daily living. J. Cachexia Sarcopenia Muscle 2019, 10, 1009–1015. [Google Scholar] [CrossRef] [Green Version]
- Peel, N.M.; Alapatt, L.J.; Jones, L.V.; Hubbard, R.E. The association between gait speed and cognitive status in community-dwelling older people: A systematic review and meta-analysis. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2019, 74, 943–948. [Google Scholar] [CrossRef] [PubMed]
- Rasmussen, L.J.H.; Caspi, A.; Ambler, A.; Broadbent, J.M.; Cohen, H.J.; D’Arbeloff, T.; Elliott, M.; Hancox, R.J.; Harrington, H.; Hogan, S.; et al. Association of Neurocognitive and Physical Function With Gait Speed in Midlife. JAMA Netw. Open 2019, 2, e1913123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Verlinden, V.J.A.; van der Geest, J.N.; Hofman, A.; Ikram, M.A. Cognition and gait show a distinct pattern of association in the general population. Alzheimers Dement. 2014, 10, 328–335. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fritz, S.; Lusardi, M. White Paper: “Walking Speed: The Sixth Vital Sign.”. J. Geriatr. Phys. Ther. 2009, 32, 2–5. [Google Scholar] [CrossRef] [Green Version]
- Annweiler, C.; Beauchet, O.; Bartha, R.; Wells, J.L.; Borrie, M.J.; Hachinski, V.; Montero-Odasso, M. Motor cortex and gait in mild cognitive impairment: A magnetic resonance spectroscopy and volumetric imaging study. Brain 2013, 136, 859–871. [Google Scholar] [CrossRef] [Green Version]
- Pérez-Sousa, M.Á.; del Pozo-Cruz, J.; Olivares, P.R.; Cano-Gutiérrez, C.A.; Izquierdo, M.; Ramírez-Vélez, R. Role for Physical Fitness in the Association between Age and Cognitive Function in Older Adults: A Mediation Analysis of the SABE Colombia Study. Int. J. Environ. Res. Public Health 2021, 18, 751. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J.A.; Verghese, J.; Zwerling, J.L. Cognition and gait in older people. Maturitas 2016, 93, 73–77. [Google Scholar] [CrossRef]
- Kasović, M.; Štefan, L.; Zvonař, M. Domain-Specific and Total Sedentary Behavior Associated with Gait Velocity in Older Adults: The Mediating Role of Physical Fitness. Int. J. Environ. Res. Public Health 2020, 17, 593. [Google Scholar] [CrossRef] [Green Version]
- Cesari, M.; Onder, G.; Zamboni, V.; Manini, T.; Shorr, R.I.; Russo, A.; Bernabei, R.; Pahor, M.; Landi, F. Physical function and self-rated health status as predictors of mortality: Results from longitudinal analysis in the ilSIRENTE study. BMC Geriatr. 2008, 8, 34. [Google Scholar] [CrossRef] [Green Version]
- Hardy, S.E.; Perera, S.; Roumani, Y.F.; Chandler, J.M.; Studenski, S.A. Improvement in Usual Gait Speed Predicts Better Survival in Older Adults. J. Am. Geriatr. Soc. 2007, 55, 1727–1734. [Google Scholar] [CrossRef]
- Studenski, S.; Faulkner, K.; Inzitari, M.; Brach, J.; Chandler, J.; Cawthon, P.; Connor, E.B.; Kritchevsky, S.; Badinelli, S.; Harris, T.; et al. Gait Speed and Survival in Older Adults. JAMA J. Am. Med. Assoc. 2015, 305, 50–58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Veronese, N.; Stubbs, B.; Volpato, S.; Zuliani, G.; Maggi, S.; Cesari, M.; Lipnicki, D.M.; Smith, L.; Schofield, P.; Firth, J.; et al. Association Between Gait Speed With Mortality, Cardiovascular Disease and Cancer: A Systematic Review and Meta-analysis of Prospective Cohort Studies. J. Am. Med. Dir. Assoc. 2018, 19, 981–988.e7. [Google Scholar] [CrossRef] [PubMed]
- Karunananthan, S.; Moodie, E.E.M.; Bergman, H.; Payette, H.; Diehr, P.H.; Wolfson, C. Physical Function and Survival in Older Adults: A longitudinal study accounting for time-varying effects. Arch. Gerontol. Geriatr. 2021, 96, 104440. [Google Scholar] [CrossRef] [PubMed]
- Osoba, M.Y.; Rao, A.K.; Agrawal, S.K.; Lalwani, A.K. Balance and gait in the elderly: A contemporary review. Laryngoscope Investig. Otolaryngol. 2019, 4, 143–153. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davis, J.C.; Robertson, M.C.; Ashe, M.C.; Liu-Ambrose, T.; Khan, K.M.; Marra, C.A. International comparison of cost of falls in older adults living in the community: A systematic review. Osteoporos. Int. 2010, 21, 1295–1306. [Google Scholar] [CrossRef]
- Weijer, R.H.A.; Hoozemans, M.J.M.; van Dieën, J.H.; Pijnappels, M. Self-perceived gait stability modulates the effect of daily life gait quality on prospective falls in older adults. Gait Posture 2018, 62, 475–479. [Google Scholar] [CrossRef] [Green Version]
- Steckhan, G.M.A.; Fleig, L.; Schwarzer, R.; Warner, L.M. Perceived Physical Functioning and Gait Speed as Mediators in the Association Between Fear of Falling and Quality of Life in Old Age. J. Appl. Gerontol. 2020, 41, 421–429. [Google Scholar] [CrossRef]
- Van Schooten, K.S.; Pijnappels, M.; Lord, S.R.; van Dieën, J.H. Quality of Daily-Life Gait: Novel Outcome for Trials that Focus on Balance, Mobility, and Falls. Sensors 2019, 19, 4388. [Google Scholar] [CrossRef] [Green Version]
- Beauchet, O.; Allali, G.; Launay, C.; Herrmann, F.R.; Annweiler, C. Gait variability at fast-pace walking speed: A biomarker of mild cognitive impairment? J. Nutr. Health Aging 2013, 17, 235–239. [Google Scholar] [CrossRef]
- Montero-Odasso, M.; Verghese, J.; Beauchet, O.; Hausdorff, J.M. Gait and Cognition: A Complementary Approach to Understanding Brain Function and the Risk of Falling. J. Am. Geriatr. Soc. 2012, 60, 2127–2136. [Google Scholar] [CrossRef] [Green Version]
- Taniguchi, Y.; Yoshida, H.; Fujiwara, Y.; Motohashi, Y.; Shinkai, S. A Prospective Study of Gait Performance and Subsequent Cognitive Decline in a General Population of Older Japanese. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2012, 67, 796–803. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morris, R.; Lord, S.; Bunce, J.; Burn, D.; Rochester, L. Gait and cognition: Mapping the global and discrete relationships in ageing and neurodegenerative disease. Neurosci. Biobehav. Rev. 2016, 64, 326–345. [Google Scholar] [CrossRef] [PubMed]
- Verghese, J.; Wang, C.; Lipton, R.B.; Holtzer, R. Motoric Cognitive Risk Syndrome and the Risk of Dementia. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2013, 68, 412–418. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jaroslawska, A.J.; Gathercole, S.E.; Holmes, J. Following instructions in a dual-task paradigm: Evidence for a temporary motor store in working memory. Q. J. Exp. Psychol. 2018, 71, 2439–2449. [Google Scholar] [CrossRef]
- Falbo, S.; Condello, G.; Capranica, L.; Forte, R.; Pesce, C. Effects of Physical-Cognitive Dual Task Training on Executive Function and Gait Performance in Older Adults: A Randomized Controlled Trial. BioMed Res. Int. 2016, 2016, 5812092. [Google Scholar] [CrossRef] [Green Version]
- Wrightson, J.G.; Ross, E.Z.; Smeeton, N.J. The effect of cognitive-task type and walking speed on dual-task gait in healthy adults. Mot. Control 2016, 20, 109–121. [Google Scholar] [CrossRef]
- Allali, G.; Montembeault, M.; Brambati, S.M.; Bherer, L.; Blumen, H.M.; Launay, C.P.; Liu-Ambrose, T.; Helbostad, J.L.; Verghese, J.; Beauchet, O. Brain structure covariance associated with gait control in aging. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2019, 74, 705–713. [Google Scholar] [CrossRef]
- Tian, Q.; An, Y.; Resnick, S.M.; Studenski, S. The relative temporal sequence of decline in mobility and cognition among initially unimpaired older adults: Results from the Baltimore Longitudinal Study of Aging. Age Ageing 2016, 46, 445–451. [Google Scholar] [CrossRef] [Green Version]
- Watson, N.L.; Rosano, C.; Boudreau, R.M.; Simonsick, E.M.; Ferrucci, L.; Sutton-Tyrrell, K.; Hardy, S.E.; Atkinson, H.H.; Yaffe, K.; Satterfield, S.; et al. Executive Function, Memory, and Gait Speed Decline in Well-Functioning Older Adults. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2010, 65A, 1093–1100. [Google Scholar] [CrossRef] [Green Version]
- Murray, E.A.; Wise, S.P. Interactions between orbital prefrontal cortex and amygdala: Advanced cognition, learned responses and instinctive behaviors. Curr. Opin. Neurobiol. 2010, 20, 212–220. [Google Scholar] [CrossRef] [Green Version]
- Montero-Odasso, M. Gait as a biomarker of cognitive impairment and dementia syndromes. Quo vadis? Eur. J. Neurol. 2016, 23, 437–438. [Google Scholar] [CrossRef] [PubMed]
- Li, C.; Verghese, J.; Holtzer, R. A comparison of two walking while talking paradigms in aging. Gait Posture 2014, 40, 415–419. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taraldsen, K.; Helbostad, J.L.; Follestad, T.; Bergh, S.; Selbæk, G.; Saltvedt, I. Gait, physical function, and physical activity in three groups of home-dwelling older adults with different severity of cognitive impairment—A cross-sectional study. BMC Geriatr. 2021, 21, 670. [Google Scholar] [CrossRef]
- Garcia-Cifuentes, E.; Márquez, I.; Vasquez, D.; Aguillon, D.; Borda, M.G.; Lopera, F.; Cano-Gutierrez, C. The Role of Gait Speed in Dementia: A Secondary Analysis from the SABE Colombia Study. Dement. Geriatr. Cogn. Disord. 2020, 49, 565–572. [Google Scholar] [CrossRef] [PubMed]
- Creavin, S.T.; Noel-Storr, A.H.; Smailagic, N.; Giannakou, A.; Ewins, E.; Wisniewski, S.; Cullum, S. Mini-Mental State Examination (MMSE) for the detection of Alzheimer’s dementia and other dementias in asymptomatic and previously clinically unevaluated people aged over 65 years in community and primary care populations. In Cochrane Database of Systematic Reviews; Creavin, S.T., Ed.; John Wiley & Sons, Ltd: Chichester, UK, 2016. [Google Scholar]
- Rose, D.J. Fallproof!: A Comprehensive Balance and Mobility Training Program, 2nd ed.; Human Kinetics: Champaign, IL, USA, 2010; ISBN 978-0-7360-6747-8. [Google Scholar]
- Kliegel, M.; Martin, M.; Jäger, T. Development and Validation of the Cognitive Telephone Screening Instrument (COGTEL) for the Assessment of Cognitive Function Across Adulthood. J. Psychol. 2007, 141, 147–170. [Google Scholar] [CrossRef] [PubMed]
- Ihle, A.; Gouveia, É.R.; Gouveia, B.R.; Kliegel, M. The Cognitive Telephone Screening Instrument (COGTEL): A Brief, Reliable, and Valid Tool for Capturing Interindividual Differences in Cognitive Functioning in Epidemiological and Aging Studies. Dement. Geriatr. Cogn. Dis. Extra 2017, 7, 339–345. [Google Scholar] [CrossRef]
- Rikli, R.E.; Jones, C.J. Development and Validation of Criterion-Referenced Clinically Relevant Fitness Standards for Maintaining Physical Independence in Later Years. Gerontologist 2013, 53, 255–267. [Google Scholar] [CrossRef] [PubMed]
- Bischkopf, J.; Busse, A.; Mc, A. Mild cognitive impairment 1—A review of prevalence, incidence and outcome according to current approaches. Acta Psychiatr. Scand. 2002, 106, 403–414. [Google Scholar] [CrossRef] [Green Version]
- Preacher, K.J.; Rucker, D.D.; Hayes, A.F. Addressing Moderated Mediation Hypotheses: Theory, Methods, and Prescriptions. Multivar. Behav. Res. 2007, 42, 185–227. [Google Scholar] [CrossRef]
- Hayes, A.F.; Rockwood, N.J. Regression-based statistical mediation and moderation analysis in clinical research: Observations, recommendations, and implementation. Behav. Res. Ther. 2017, 98, 39–57. [Google Scholar] [CrossRef]
- Costa, T.B.; Neri, A.L. Associated factors with physical activity and social activity in a sample of Brazilian older adults: Data from the FIBRA Study. Rev. Bras. Epidemiol. 2019, 22, e190022. [Google Scholar] [CrossRef] [PubMed]
- De Asteasu, M.L.S.; Martínez-Velilla, N.; Zambom-Ferraresi, F.; Casas-Herrero, Á.; Izquierdo, M. Role of physical exercise on cognitive function in healthy older adults: A systematic review of randomized clinical trials. Ageing Res. Rev. 2017, 37, 117–134. [Google Scholar] [CrossRef]
- Pau, M.; Leban, B.; Collu, G.; Migliaccio, G.M. Effect of light and vigorous physical activity on balance and gait of older adults. Arch. Gerontol. Geriatr. 2014, 59, 568–573. [Google Scholar] [CrossRef]
- Gomez-Bruton, A.; Navarrete-Villanueva, D.; Pérez-Gómez, J.; Vila-Maldonado, S.; Gesteiro, E.; Gusi, N.; Villa-Vicente, J.G.; Espino, L.; Gonzalez-Gross, M.; Casajus, J.A.; et al. The Effects of Age, Organized Physical Activity and Sedentarism on Fitness in Older Adults: An 8-Year Longitudinal Study. Int. J. Environ. Res. Public Health 2020, 17, 4312. [Google Scholar] [CrossRef]
- Klenk, J.; Kerse, N.; Rapp, K.; Nikolaus, T.; Becker, C.; Rothenbacher, D.; Peter, R.; Denkinger, M.D. Physical Activity and Different Concepts of Fall Risk Estimation in Older People–Results of the ActiFE-Ulm Study. PLoS ONE 2015, 10, e0129098. [Google Scholar] [CrossRef] [PubMed]
- Ronthal, M. Gait Disorders and Falls in the Elderly. Med. Clin. N. Am. 2019, 103, 203–213. [Google Scholar] [CrossRef] [PubMed]
- Hu, K.; Zhou, Q.; Jiang, Y.; Shang, Z.; Mei, F.; Gao, Q.; Chen, F.; Zhao, L.; Jiang, M.; Ma, B. Association between Frailty and Mortality, Falls, and Hospitalization among Patients with Hypertension: A Systematic Review and Meta-Analysis. BioMed Res. Int. 2021, 2021, 2690296. [Google Scholar] [CrossRef]
- Asai, T.; Misu, S.; Sawa, R.; Doi, T.; Yamada, M. The association between fear of falling and smoothness of lower trunk oscillation in gait varies according to gait speed in community-dwelling older adults. J. Neuroeng. Rehabil. 2017, 14, 5. [Google Scholar] [CrossRef] [Green Version]
- Lavedán, A.; Viladrosa, M.; Jürschik, P.; Botigué, T.; Nuín, C.; Masot, O.; Lavedán, R. Fear of falling in community-dwelling older adults: A cause of falls, a consequence, or both? PLoS ONE 2018, 13, e0194967. [Google Scholar] [CrossRef]
- Hartholt, K.A.; Polinder, S.; Van der Cammen, T.J.M.; Panneman, M.J.M.; Van der Velde, N.; Van Lieshout, E.M.M.; Patka, P.; Van Beeck, E.F. Costs of falls in an ageing population: A nationwide study from the Netherlands (2007–2009). Injury 2012, 43, 1199–1203. [Google Scholar] [CrossRef] [Green Version]
- Florence, C.S.; Bergen, G.; Atherly, A.; Burns, E.; Stevens, J.; Drake, C. Medical Costs of Fatal and Nonfatal Falls in Older Adults. J. Am. Geriatr. Soc. 2018, 66, 693–698. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Larsson, L.; Degens, H.; Li, M.; Salviati, L.; Lee, Y.I.; Thompson, W.; Kirkland, J.L.; Sandri, M. Sarcopenia: Aging-Related Loss of Muscle Mass and Function. Physiol. Rev. 2019, 99, 427–511. [Google Scholar] [CrossRef] [PubMed]
- Noce Kirkwood, R.; de Souza Moreira, B.; Mingoti, S.A.; Faria, B.F.; Sampaio, R.F.; Alves Resende, R. The slowing down phenomenon: What is the age of major gait velocity decline? Maturitas 2018, 115, 31–36. [Google Scholar] [CrossRef] [PubMed]
- Pepera, G.K.; Sandercock, G.R.; Sloan, R.; Cleland, J.J.F.; Ingle, L.; Clark, A.L. Influence of step length on 6-minute walk test performance in patients with chronic heart failure. Physiotherapy 2012, 98, 325–329. [Google Scholar] [CrossRef]
- Callisaya, M.L.; Beare, R.; Phan, T.G.; Blizzard, L.; Thrift, A.G.; Chen, J.; Srikanth, V.K. Brain structural change and gait decline: A longitudinal population-based study. J. Am. Geriatr. Soc. 2013, 61, 1074–1079. [Google Scholar] [CrossRef]
- Kuo, H.-K.; Leveille, S.G.; Yu, Y.-H.; Milberg, W.P. Cognitive Function, Habitual Gait Speed, and Late-Life Disability in the National Health and Nutrition Examination Survey (NHANES) 1999–2002. Gerontology 2007, 53, 102–110. [Google Scholar] [CrossRef] [Green Version]
- Jones, N.R.; Roalfe, A.K.; Adoki, I.; Hobbs, F.D.R.; Taylor, C.J. Survival of patients with chronic heart failure in the community: A systematic review and meta-analysis. Eur. J. Heart Fail. 2019, 21, 1306–1325. [Google Scholar] [CrossRef]
- Woo, J.; Leung, J.; Kwok, T. BMI, Body Composition, and Physical Functioning in Older Adults*. Obesity 2007, 15, 1886–1894. [Google Scholar] [CrossRef]
- Gardener, H.; Caunca, M.; Dong, C.; Cheung, Y.K.; Rundek, T.; Elkind, M.S.V.; Wright, C.B.; Sacco, R.L. Obesity Measures in Relation to Cognition in the Northern Manhattan Study. J. Alzheimers Dis. 2020, 78, 1653–1660. [Google Scholar] [CrossRef]
- Gunstad, J.; Lhotsky, A.; Wendell, C.R.; Ferrucci, L.; Zonderman, A.B. Longitudinal Examination of Obesity and Cognitive Function: Results from the Baltimore Longitudinal Study of Aging. Neuroepidemiology 2010, 34, 222–229. [Google Scholar] [CrossRef] [Green Version]
- Ling, C.H.Y.; Meskers, C.G.M.; Maier, A.B. Can anthropometric measures be used as proxies for body composition and physical function in geriatric outpatients? Arch. Gerontol. Geriatr. 2021, 94, 104379. [Google Scholar] [CrossRef] [PubMed]
- Porter Starr, K.N.; McDonald, S.R.; Bales, C.W. Obesity and Physical Frailty in Older Adults: A Scoping Review of Lifestyle Intervention Trials. J. Am. Med. Dir. Assoc. 2014, 15, 240–250. [Google Scholar] [CrossRef] [Green Version]
- Aracaty, M.L.; de Souza Rojas, S.R. Índice de vulnerabilidade Social vulnerability index (IVS) of the metropolitan regions of Belém do Pará-PA (RMB) and Manaus-AM (RMM). Econ. Desenv. 2021, 33, 1. [Google Scholar]
- SBGG-Brazilian Society of Geriatrics and Gerontology Mais Idosos Poucos Geriátras [More Older Adult Few Geriatricians]. Available online: http://www.sbgg-sp.com.br/pub/mais-idosos-poucos-geriatras/ (accessed on 26 March 2019).
- Nascimento, M.D.M. Healthy aging in Brazil: Odyssey or strategy? Educ. Gerontol. 2021, 47, 419–431. [Google Scholar] [CrossRef]
- Sousa, N.F.; Medina, L.d.P.B.; Bastos, T.F.; Monteiro, C.N.; Lima, M.G.; Barros, M.B.D.A. Social inequalities in the prevalence of indicators of active aging in the Brazilian population: National Health Survey, 2013. Rev. Bras. Epidemiol. 2019, 22 (Suppl. 2), E190013. [Google Scholar]
- WHO-World Health Organization. Active Ageing: A Policy Framework, a Contribution of the World Health Organization to the Second United Nations World Assembly on Ageing; World Health Organization: Madrid, Spain; Geneva, Switzerland, 2002. [Google Scholar]
- Rowe, J.W.; Kahn, R.L. Successful Aging 2.0: Conceptual Expansions for the 21st Century. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 2015, 70, 593–596. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Variable | Full Sample (n = 697) | Cognitive Impairment (n = 336) | No Cognitive Impairment (n = 361) | p-Value |
|---|---|---|---|---|
| Age (years) | 70.35 ± 6.86 | 71.58 ± 7.47 | 69.23 ± 6.05 | <0.001 |
| Sex n (%) | 0.001 | |||
| Female | 430 (61.7) | 183 (55.3) | 247 (67.5) | |
| Male | 267 (38.3) | 148 (44.7) | 119 (32.5) | |
| Education (years) (n) | 5.35 ± 5.54 | 1.97 ± 2.90 | 8.40 ± 5.61 | <0.001 |
| Falls (n) | 0.59 ± 1.32 | 0.68 ± 1.66 | 0.51 ± 0.90 | 0.087 |
| MMSE (n) | 24.40 ± 4.23 | 22.12 ± 4.16 | 26.51 ± 3.03 | <0.001 |
| Cognition (n) | ||||
| COGTEL (score) | 18.95 ± 9.45 | 11.11 ± 4.59 | 26.17 ± 6.59 | <0.001 |
| Physical function (n) | ||||
| PF total (score) | 470.63 ± 96.16 | 461.09 ± 99.95 | 479.40 ± 91.81 | <0.001 |
| Gait (m/s) | ||||
| GS | 1.35 ± 0.47 | 1.12 ± 0.34 | 1.55 ± 0.48 | <0.001 |
| Variable | Model 1 OR 95% CI p-Value | Model 2 OR 95% CI p-Value | Model 3 OR 95% CI p-Value |
|---|---|---|---|
| Lower CP | 0.450 (0.359–0.484) <0.001 | 0.437 (0.347–0.473) <0.001 | 0.296 (0.128–0.302) <0.001 |
| Lower PF | 0.206 (0.125–0.261) <0.001 | 0.188 (0.105–0.247) <0.001 | 0.141 (0.091–0.198) <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nascimento, M.d.M.; Gouveia, É.R.; Gouveia, B.R.; Marques, A.; Marconcin, P.; França, C.; Ihle, A. The Role of Cognitive Performance and Physical Functions in the Association between Age and Gait Speed: A Mediation Study. Geriatrics 2022, 7, 73. https://0-doi-org.brum.beds.ac.uk/10.3390/geriatrics7040073
Nascimento MdM, Gouveia ÉR, Gouveia BR, Marques A, Marconcin P, França C, Ihle A. The Role of Cognitive Performance and Physical Functions in the Association between Age and Gait Speed: A Mediation Study. Geriatrics. 2022; 7(4):73. https://0-doi-org.brum.beds.ac.uk/10.3390/geriatrics7040073
Chicago/Turabian StyleNascimento, Marcelo de Maio, Élvio Rúbio Gouveia, Bruna R. Gouveia, Adilson Marques, Priscila Marconcin, Cíntia França, and Andreas Ihle. 2022. "The Role of Cognitive Performance and Physical Functions in the Association between Age and Gait Speed: A Mediation Study" Geriatrics 7, no. 4: 73. https://0-doi-org.brum.beds.ac.uk/10.3390/geriatrics7040073