
Myocardial Bridging Leading to Cardiac Collapse in a Marathon Runner

 ,
,  , , ,
, , , {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Case Report
2.1. History of Presentation
2.2. Past Medical History
2.3. Differential Diagnosis
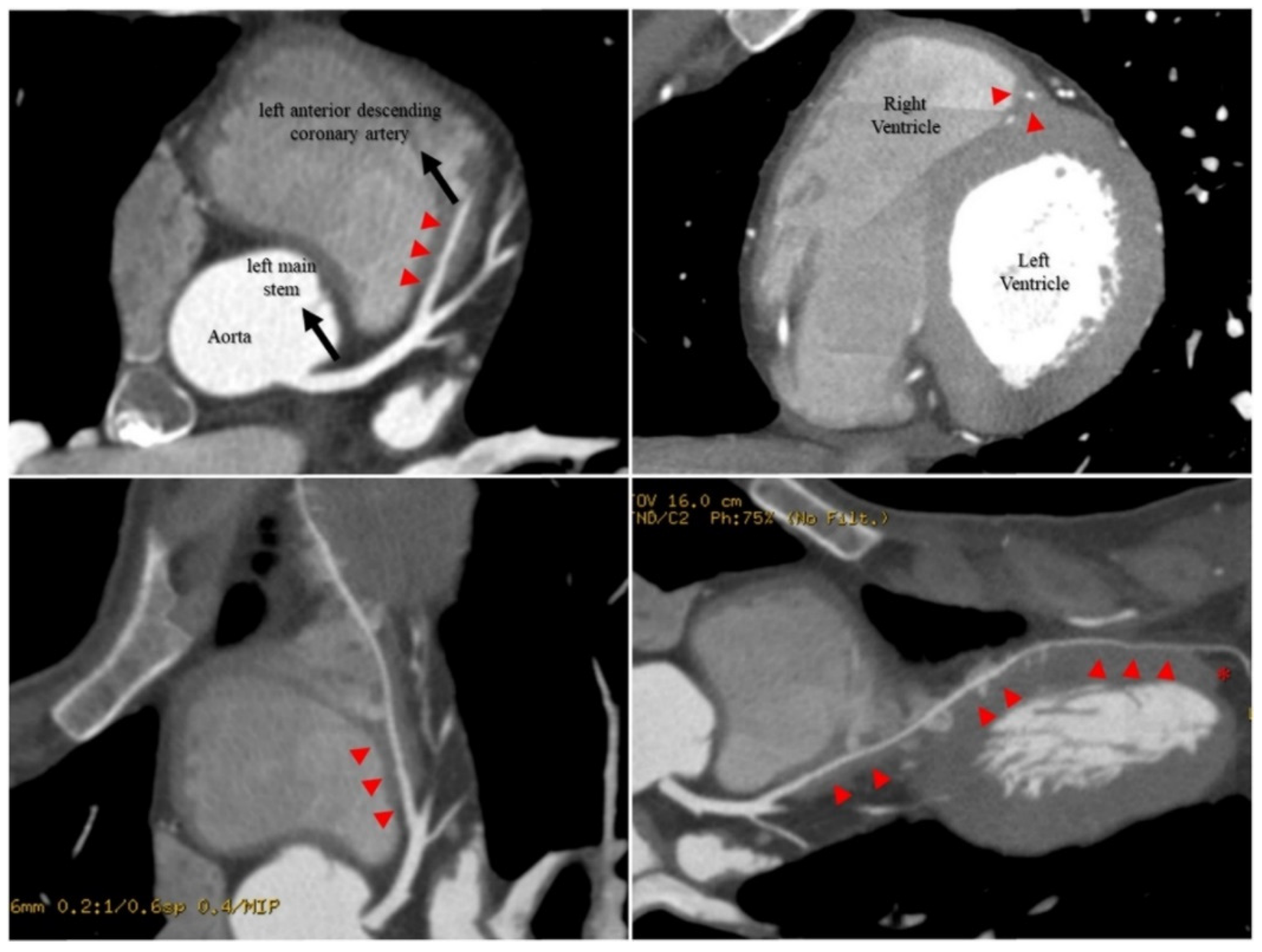
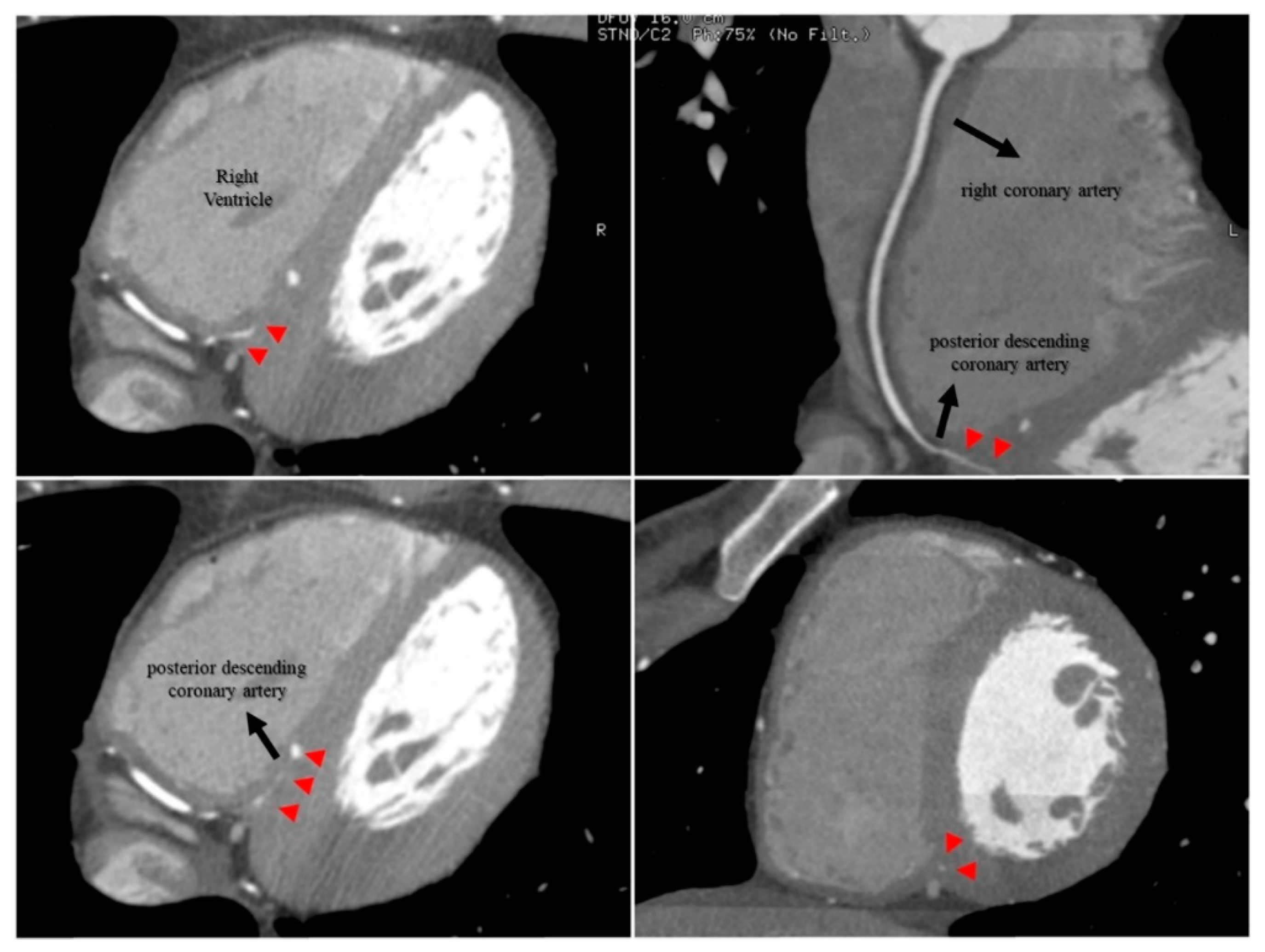
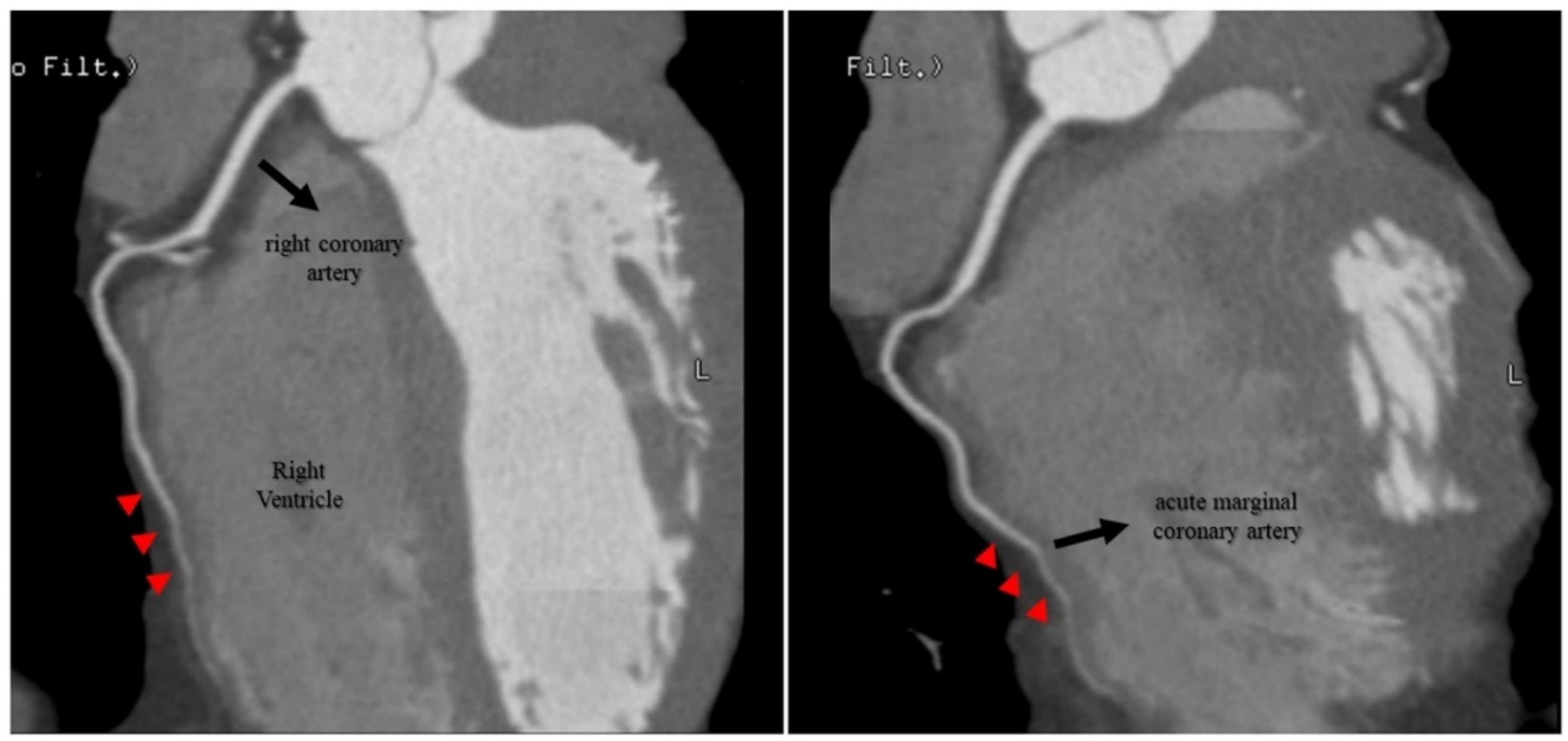
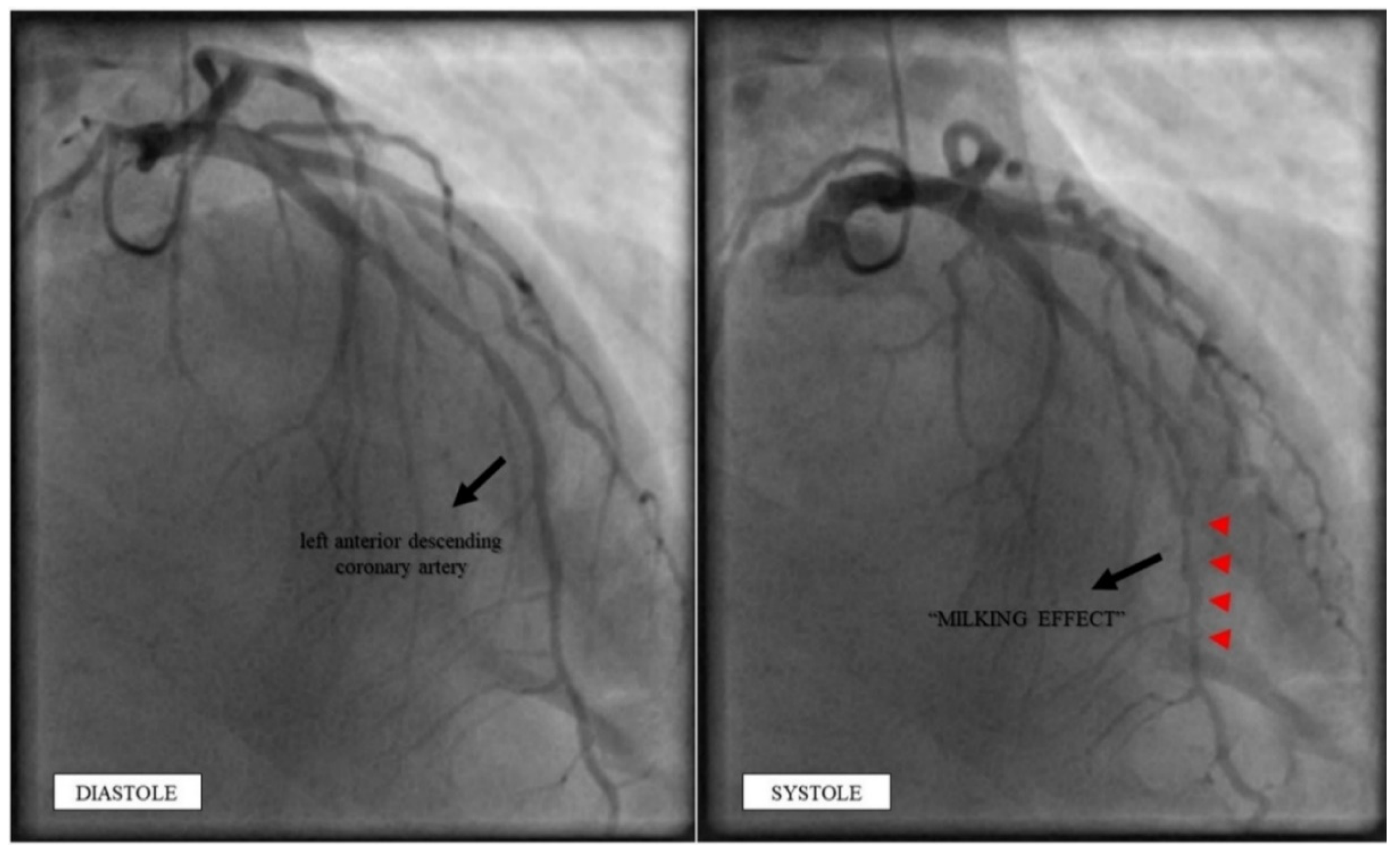
2.4. Investigations
2.5. Management
2.6. Follow-Up
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sternheim, D.; Power, D.A.; Samtani, R.; Kini, A.; Fuster, V.; Sharma, S. Myocardial Bridging: Diagnosis, Functional Assessment, and Management: JACC State-of-the-Art Review. J. Am. Coll. Cardiol. 2021, 78, 2196–2212. [Google Scholar] [CrossRef] [PubMed]
- Gowd, B.M.; Thompson, P.D. Isolated myocardial bridging and exercise-related cardiac events. Int. J. Sports Med. 2014, 35, 1145–1150. [Google Scholar] [CrossRef]
- Zerbo, S.; Lanzarone, A.; Raimondi, M.; Martino, L.; Malta, G.; Cappello, F.; Argo, A. Myocardial bridge pathology and preventable accidents during physical activity of healthy subjects: A case report and a literature review. Med. Leg. J. 2020, 88, 209–214. [Google Scholar] [CrossRef] [PubMed]
- Corban, M.T.; Hung, O.Y.; Eshtehardi, P.; Rasoul-Arzrumly, E.; McDaniel, M.; Mekonnen, G.; Timmins, L.H.; Lutz, J.; Guyton, R.A.; Samady, H. Myocardial bridging: Contemporary understanding of pathophysiology with implications for diagnostic and therapeutic strategies. J. Am. Coll. Cardiol. 2014, 63, 2346–2355. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vicent, L.; Ariza-Sole, A.; Gonzalez-Juanatey, J.R.; Uribarri, A.; Ortiz, J.; Lopez de Sa, E.; Sans-Rosello, J.; Querol, C.T.; Codina, P.; Sousa-Casasnovas, I.; et al. Exercise-related severe cardiac events. Scand. J. Med. Sci. Sports 2018, 28, 1404–1411. [Google Scholar] [CrossRef]
- Salvo, G.D.; Pergola, V.; Fadel, B.; Bulbul, Z.A.; Caso, P. Strain Echocardiography and Myocardial Mechanics: From Basics to Clinical Applications. J. Cardiovasc. Echogr. 2015, 25, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hemmati, P.; Schaff, H.V.; Dearani, J.A.; Daly, R.C.; Lahr, B.D.; Lerman, A. Clinical Outcomes of Surgical Unroofing of Myocardial Bridging in Symptomatic Patients. Ann. Thorac. Surg. 2020, 109, 452–457. [Google Scholar] [CrossRef]
- Sanchez, L.D.; Pereira, J.; Berkoff, D.J. The evaluation of cardiac complaints in marathon runners. J. Emerg. Med. 2009, 36, 369–376. [Google Scholar] [CrossRef] [PubMed]
- Brancaccio, M.; Mennitti, C.; Cesaro, A.; Monda, E.; D’Argenio, V.; Casaburi, G.; Mazzaccara, C.; Ranieri, A.; Fimiani, F.; Barretta, F.; et al. Multidisciplinary in-Depth Investigation in a Young Athlete Suffering from Syncope Caused by Myocardial Bridge. Diagnostics 2021, 11, 2144. [Google Scholar] [CrossRef]





Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alexandre, A.; Vieira, P.; Dias-Frias, A.; Pereira, A.; Campinas, A.; Sá-Couto, D.; Brochado, B.; Sá, I.; Silveira, J.; Torres, S. Myocardial Bridging Leading to Cardiac Collapse in a Marathon Runner. J. Cardiovasc. Dev. Dis. 2022, 9, 200. https://0-doi-org.brum.beds.ac.uk/10.3390/jcdd9070200
Alexandre A, Vieira P, Dias-Frias A, Pereira A, Campinas A, Sá-Couto D, Brochado B, Sá I, Silveira J, Torres S. Myocardial Bridging Leading to Cardiac Collapse in a Marathon Runner. Journal of Cardiovascular Development and Disease. 2022; 9(7):200. https://0-doi-org.brum.beds.ac.uk/10.3390/jcdd9070200
Chicago/Turabian StyleAlexandre, André, Pinheiro Vieira, André Dias-Frias, Anaisa Pereira, Andreia Campinas, David Sá-Couto, Bruno Brochado, Isabel Sá, João Silveira, and Severo Torres. 2022. "Myocardial Bridging Leading to Cardiac Collapse in a Marathon Runner" Journal of Cardiovascular Development and Disease 9, no. 7: 200. https://0-doi-org.brum.beds.ac.uk/10.3390/jcdd9070200