
Systolic Blood Pressure Response to Exercise in Endurance Athletes in Relation to Oxygen Uptake, Work Rate and Normative Values

 ,
,
Abstract
:1. Introduction
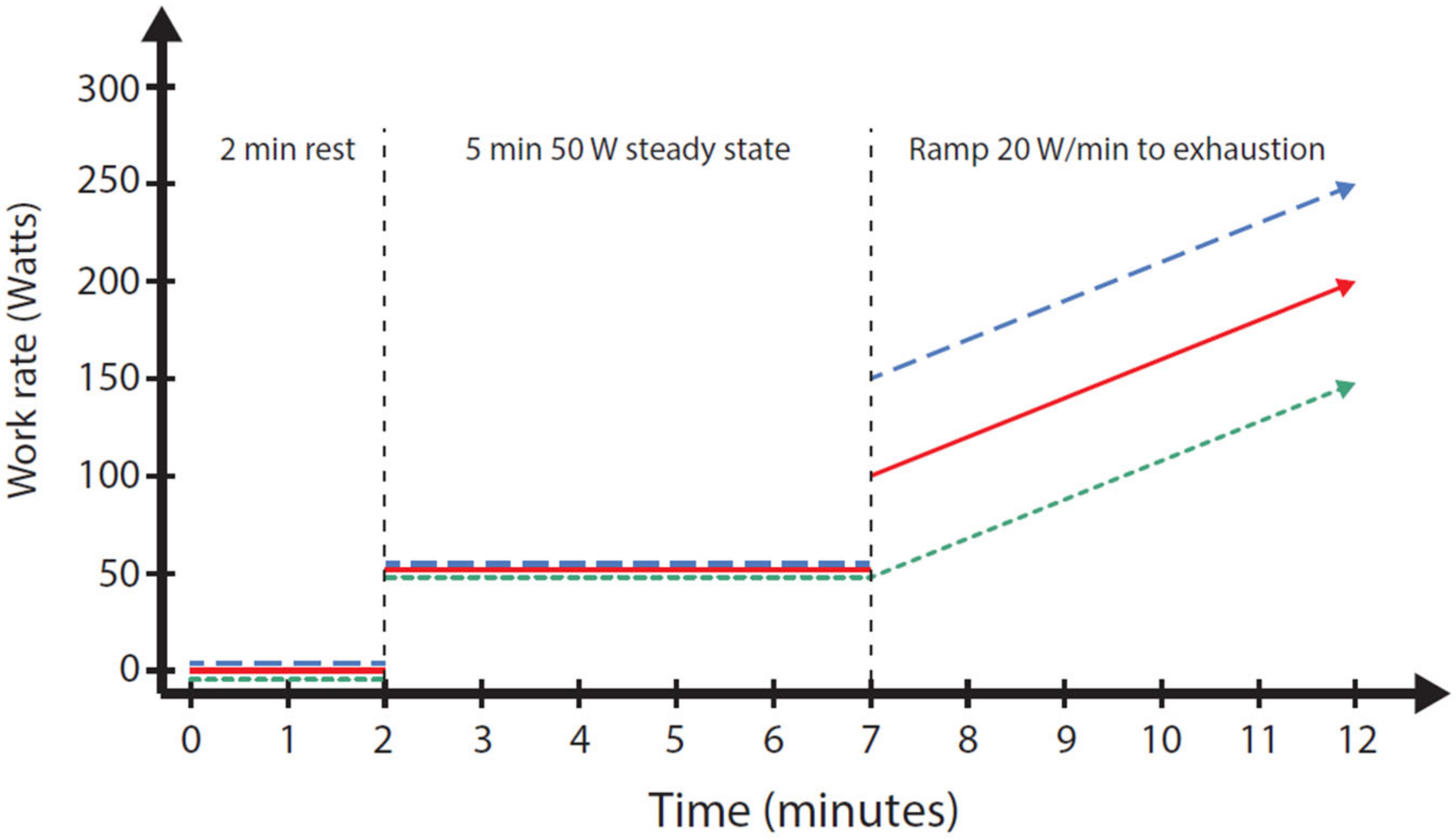
2. Materials and Methods
3. Results
3.1. Cohort Characteristics
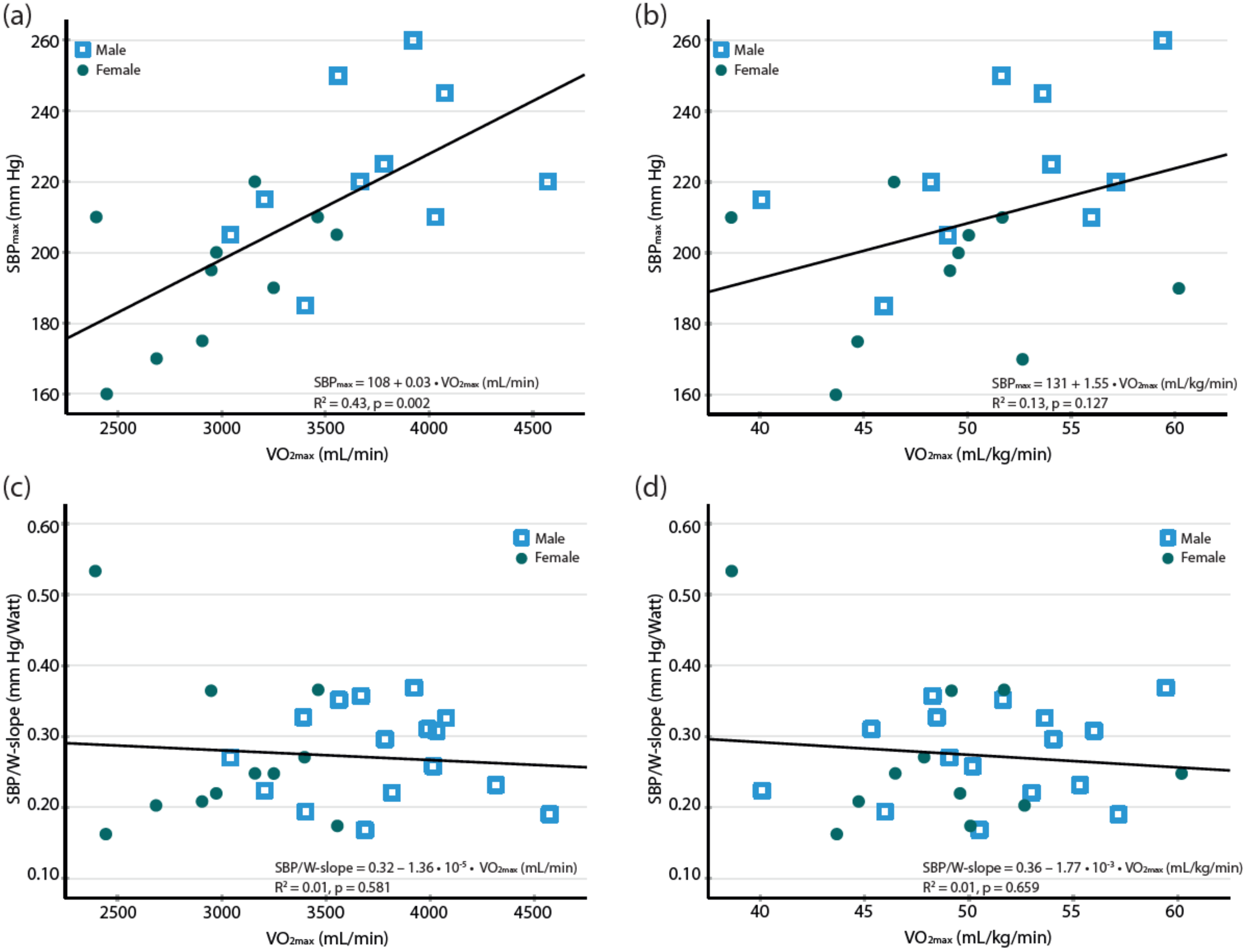
3.2. Blood Pressure Response to Exercise and Correlation to the Maximal Oxygen Uptake
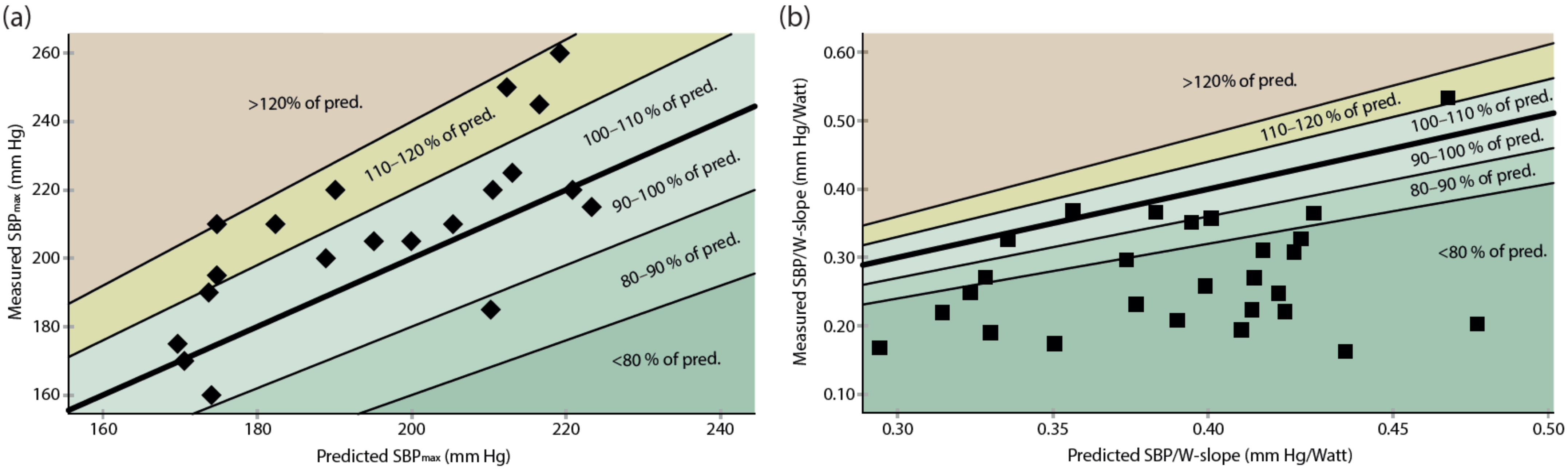
3.3. Comparison with the Suggested Thresholds and Reference Equations
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A


{kind=link}
{kind=link}
{kind=link}
| Outlier Included | Outlier Excluded | |
|---|---|---|
| SBP/VO2 slope in all athletes, mm Hg/L/min | 30.0 ± 10.2 | 28.4 ± 6.9 |
| SBP/VO2 slope in female athletes, mm Hg/L/min | 30.3 ± 14.5 | 26.5 ± 7.7 |
| SBP/W slope in all athletes, mm Hg | 0.27 ± 0.08 | 0.26 ± 0.07 |
| SBP/W slope in female athletes, mm Hg | 0.27 ± 0.11 | 0.25 ± 0.07 |
References
- Fletcher, G.F.; Ades, P.A.; Kligfield, P.; Arena, R.; Balady, G.J.; Bittner, V.A.; Coke, L.A.; Fleg, J.L.; Forman, D.E.; Gerber, T.C.; et al. Exercise standards for testing and training: A scientific statement from the American Heart Association. Circulation 2013, 128, 873–934. [Google Scholar] [CrossRef] [PubMed]
- Liguori, G. American College of Sports Medicine: Guidelines for Exercise Testing and Prescription, 11th ed.; Lippincott Williams: Philadelphia, PA, USA, 2021. [Google Scholar]
- Bevegård, S.; Freyschuss, U.; Strandell, T. Circulatory adaptation to arm and leg exercise in supine and sitting position. J. Appl. Physiol. 1966, 21, 37–46. [Google Scholar] [CrossRef] [PubMed]
- Astrand, P.O.; Cuddy, T.E.; Saltin, B.; Stenberg, J. Cardiac Output during Submaximal and Maximal Work. J. Appl. Physiol. 1964, 19, 268–274. [Google Scholar] [CrossRef]
- Zafrir, B.; Aker, A.; Asaf, Y.; Saliba, W. Blood pressure response during treadmill exercise testing and the risk for future cardiovascular events and new-onset hypertension. J. Hypertens. 2022, 40, 143–152. [Google Scholar] [CrossRef] [PubMed]
- Caselli, S.; Serdoz, A.; Mango, F.; Lemme, E.; Vaquer Segui, A.; Milan, A.; Attenhofer Jost, C.; Schmied, C.; Spataro, A.; Pelliccia, A. High blood pressure response to exercise predicts future development of hypertension in young athletes. Eur. Heart J. 2019, 40, 62–68. [Google Scholar] [CrossRef] [Green Version]
- Hedman, K.; Cauwenberghs, N.; Christle, J.W.; Kuznetsova, T.; Haddad, F.; Myers, J. Workload-indexed blood pressure response is superior to peak systolic blood pressure in predicting all-cause mortality. Eur. J. Prev. Cardiol. 2020, 27, 978–987. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Currie, K.D.; Floras, J.S.; La Gerche, A.; Goodman, J.M. Exercise Blood Pressure Guidelines: Time to Re-evaluate What is Normal and Exaggerated? Sports Med. 2018, 48, 1763–1771. [Google Scholar] [CrossRef] [PubMed]
- Hedman, K.; Lindow, T.; Elmberg, V.; Brudin, L.; Ekstrom, M. Age- and gender-specific upper limits and reference equations for workload-indexed systolic blood pressure response during bicycle ergometry. Eur. J. Prev. Cardiol. 2020, 28, 1360–1369. [Google Scholar] [CrossRef] [Green Version]
- Bauer, P.; Kraushaar, L.; Dorr, O.; Nef, H.; Hamm, C.W.; Most, A. Sex differences in workload-indexed blood pressure response and vascular function among professional athletes and their utility for clinical exercise testing. Eur. J. Appl. Physiol. 2021, 121, 1859–1869. [Google Scholar] [CrossRef]
- Bauer, P.; Kraushaar, L.; Hoelscher, S.; Weber, R.; Akdogan, E.; Keranov, S.; Dorr, O.; Nef, H.; Hamm, C.W.; Most, A. Blood Pressure Response and Vascular Function of Professional Athletes and Controls. Sports Med. Int. Open 2021, 5, E45–E52. [Google Scholar] [CrossRef]
- Petek, B.J.; Gustus, S.K.; Churchill, T.W.; Guseh, J.S.; Loomer, G.; VanAtta, C.; Baggish, A.L.; Wasfy, M.M. Sex-Based Differences in Peak Exercise Blood Pressure Indexed to Oxygen Consumption Among Competitive Athletes. Clin. Ther. 2021, 44, 11–22.e3. [Google Scholar] [CrossRef] [PubMed]
- Henry, W.L.; Gardin, J.M.; Ware, J.H. Echocardiographic measurements in normal subjects from infancy to old age. Circulation 1980, 62, 1054–1061. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for cardiac chamber quantification by echocardiography in adults: An update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. Eur. Heart J. Cardiovasc. Imaging 2015, 16, 233–270. [Google Scholar] [CrossRef] [PubMed]
- Vanoverschelde, J.J.; Essamri, B.; Vanbutsele, R.; d’Hondt, A.; Cosyns, J.R.; Detry, J.R.; Melin, J.A. Contribution of left ventricular diastolic function to exercise capacity in normal subjects. J. Appl. Physiol. 1993, 74, 2225–2233. [Google Scholar] [CrossRef] [PubMed]
- Hedman, K.; Tamas, E.; Henriksson, J.; Bjarnegard, N.; Brudin, L.; Nylander, E. Female athlete’s heart: Systolic and diastolic function related to circulatory dimensions. Scand. J. Med. Sci. Sports 2015, 25, 372–381. [Google Scholar] [CrossRef]
- Granfeldt, H.; Nylander, E. Use of vectorcardiography in determination of the left ventricular muscle mass. Clin. Physiol. 1987, 7, 209–216. [Google Scholar] [CrossRef]
- Brudin, L.; Jorfeldt, L.; Pahlm, O. Comparison of two commonly used reference materials for exercise bicycle tests with a Swedish clinical database of patients with normal outcome. Clin. Physiol. Funct. Imaging 2014, 34, 297–307. [Google Scholar] [CrossRef]
- Glaser, S.; Koch, B.; Ittermann, T.; Schaper, C.; Dorr, M.; Felix, S.B.; Volzke, H.; Ewert, R.; Hansen, J.E. Influence of age, sex, body size, smoking, and beta blockade on key gas exchange exercise parameters in an adult population. Eur. J. Cardiovasc. Prev. Rehabil. 2010, 17, 469–476. [Google Scholar] [CrossRef]
- Jetté, M.; Sidney, K.; Blümchen, G. Metabolic equivalents (METS) in exercise testing, exercise prescription, and evaluation of functional capacity. Clin. Cardiol. 1990, 13, 555–565. [Google Scholar] [CrossRef]
- Bauer, P.; Kraushaar, L.; Dorr, O.; Nef, H.; Hamm, C.W.; Most, A. Workload-indexed blood pressure response to a maximum exercise test among professional indoor athletes. Eur. J. Prev. Cardiol. 2020, 28, 1487–1494. [Google Scholar] [CrossRef]
- Hedman, K.; Moneghetti, K.J.; Christle, J.W.; Bagherzadeh, S.P.; Amsallem, M.; Ashley, E.; Froelicher, V.; Haddad, F. Blood pressure in athletic preparticipation evaluation and the implication for cardiac remodelling. Heart 2019, 105, 1223–1230. [Google Scholar] [CrossRef] [PubMed]
- Caselli, S.; Vaquer Sequi, A.; Lemme, E.; Quattrini, F.; Milan, A.; D’Ascenzi, F.; Spataro, A.; Pelliccia, A. Prevalence and Management of Systemic Hypertension in Athletes. Am. J. Cardiol. 2017, 119, 1616–1622. [Google Scholar] [CrossRef] [PubMed]
- Berger, A.; Grossman, E.; Katz, M.; Kivity, S.; Klempfner, R.; Segev, S.; Goldenberg, I.; Sidi, Y.; Maor, E. Exercise blood pressure and the risk for future hypertension among normotensive middle-aged adults. J. Am. Heart Assoc. 2015, 4, e001710. [Google Scholar] [CrossRef] [Green Version]
- Caselli, S.; Vaquer Segui, A.; Quattrini, F.; Di Gacinto, B.; Milan, A.; Assorgi, R.; Verdile, L.; Spataro, A.; Pelliccia, A. Upper normal values of blood pressure response to exercise in Olympic athletes. Am. Heart J. 2016, 177, 120–128. [Google Scholar] [CrossRef]
- Kim, Y.J.; Chun, H.; Kim, C.H. Exaggerated response of systolic blood pressure to cycle ergometer. Ann. Rehabil. Med. 2013, 37, 364–372. [Google Scholar] [CrossRef] [PubMed]
- Miyai, N.; Arita, M.; Morioka, I.; Miyashita, K.; Nishio, I.; Takeda, S. Exercise BP response in subjects with high-normal BP: Exaggerated blood pressure response to exercise and risk of future hypertension in subjects with high-normal blood pressure. J. Am. Coll. Cardiol. 2000, 36, 1626–1631. [Google Scholar] [CrossRef] [Green Version]


| All Subjects | Men | Women | p | |
|---|---|---|---|---|
| (n = 27) | (n = 16) | (n = 11) | ||
| Demographics | ||||
| Age (years) | 40 ± 10 | 45 ± 10 | 33 ± 6 | 0.002 |
| Weight (kg) | 69 ± 9 | 74 ± 6 | 62 ± 7 | <0.001 |
| Height (cm) | 176 ± 8 | 180 ± 7 | 170 ± 5 | <0.001 |
| BMI (kg/m2) | 22 ± 2 | 23 ± 1 | 22 ± 2 | 0.045 |
| Cardiopulmonary exercise test | ||||
| VO2max (L/min) | 3.5 ± 0.5 | 3.9 ± 0.4 | 3.0 ± 0.4 | <0.001 |
| VO2max (mL/kg/min) | 50 ± 5 | 51 ± 5 | 49 ± 6 | 0.23 |
| VO2max (% of predicted) | 155 ± 19 | 146 ± 13 | 169 ± 17 | <0.001 |
| METmax | 14 ± 2 | 15 ± 1 | 14 ± 2 | 0.23 |
| RPEmax (Borg RPE) | 19 (2) | 19 (2) | 17 (2) | 0.09 |
| Dyspneamax (Borg CR10) | 8 (2) | 9 (1) | 7 (2) | 0.034 |
| HRmax (beats/min) | 175 ± 10 | 175 ± 12 | 175 ± 9 | 0.89 |
| HRmax (% of age-predicted) | 97 ± 6 | 100 ± 6 | 94 ± 4 | 0.008 |
| Wmax | 315 ± 58 | 349 ± 42 | 266 ± 37 | <0.001 |
| Wmax (% of predicted) | 154 ± 19 | 146 ± 17 | 166 ± 16 | 0.004 |
| All subjects | Men | Women | p | |
|---|---|---|---|---|
| (n = 27) | (n = 16) | (n = 11) | ||
| At rest, before the test | ||||
| SBPlying (mm Hg) | 124 ± 12 | 128 ± 10 | 118 ± 11 | 0.022 |
| DBPlying (mm Hg) | 75 ± 8 | 75 ± 7 | 74 ± 8 | 0.68 |
| SBPsitting (mm Hg) | 125 ± 14 | 130 ± 11 | 118 ± 13 | 0.025 |
| During exercise | ||||
| SBPmax (mm Hg) 1 | 209 ± 26 | 224 ± 23 | 194 ± 20 | 0.005 |
| SBPpeak (mm Hg) | 211 ± 24 | 223 ± 20 | 193 ± 19 | <0.001 |
| SBP200 W (mm Hg) | 188 ± 18 | 190 ± 17 | 184 ± 20 | 0.35 |
| SBP50 W (mm Hg) | 145 ± 15 | 148 ± 15 | 140 ± 16 | 0.16 |
| Indexed to exercise intensity or work rate | ||||
| SBP/VO2 slope (mm Hg/L/min) | 29.8 ± 10.2 | 29.5 ± 6.4 | 30.3 ± 14.5 | 0.85 |
| SBP/MET slope (mm Hg/MET) 2 | 7.2 ± 2.4 | 7.6 ± 1.6 | 6.6 ± 3.3 | 0.30 |
| SBP/MET slope (mm Hg/MET) 3 | 6.8 ± 1.3 | 7.2 ± 1.0 | 6.3 ± 1.6 | 0.070 |
| SBP/W slope (mm Hg/W) | 0.27 ± 0.08 | 0.28 ± 0.06 | 0.27 ± 0.11 | 0.94 |
| VO2max (mL/min) | VO2max (mL/kg/min) | |
|---|---|---|
| SBPmax 1, r (p) | 0.654 (0.002) | 0.353 (0.13) |
| SBP/VO2 slope, r (p) | −0.205 (0.31) | −0.258 (0.19) |
| SBP/MET slope 2, r (p) | 0.066 (0.75) | −0.266 (0.18) |
| SBP/MET slope 3, r (p) | 0.140 (0.49) | −0.290 (0.14) |
| SBP/W slope, r (p) | −0.089 (0.66) | −0.111 (0.58) |
| SBP at 50 W, r (p) | 0.156 (0.44) | 0.005 (0.98) |
| SBP at 200 W, r (p) | 0.048 (0.81) | −0.050 (0.81) |
| Current Study | Bauer et al. | Petek et al. | |||||
|---|---|---|---|---|---|---|---|
| [11] | [10] | [12] | |||||
| Male endurance athletes | Female endurance athletes | Male handball players | Male handball players | Female football players | Male athletes | Female athletes | |
| Age (years) | 45 ± 10 | 33 ± 7 | 26 ± 5 | 22 ± 2 | 21 ± 2 | 38 ± 16 | 34 ± 15 |
| Height (cm) | 179 ± 7 | 170 ± 6 | 189 ± 7 | 189 ± 7 | 167 ± 5 | NA | NA |
| Weight (kg) | 73.7 ± 6.4 | 62.9 ± 6.9 | 91.5 ± 10.7 | 90.9 ± 12.3 | 60.8 ± 7.7 | NA | NA |
| BMI (kg/m2) | 22.9 ± 1.4 | 21.8 ± 1.8 | 25.7 ± 2 | 25.5 ± 2.4 | 21.7 ± 1.9 | NA | NA |
| Before the test, at rest | |||||||
| SBPsitting (mm Hg) | 130 ± 12 | 120 ± 14 | 123 ± 10 | 125 ± 10 | 120 ± 11 | 121 ± 9 | 110 ± 10 |
| At peak exercise | |||||||
| Wmax | 344 ± 39 | 269 ± 39 | 339 ± 64 | 342 ± 72 | 190 ± 32 | 344 ± 72 | 211 ± 48 |
| VO2max (mL/kg/min) | 51 ± 5 | 49 ± 6 | NA | NA | NA | 46 ± 10 | 37 ± 8 |
| HRmax (beats/min) | 174 ± 12 | 176 ± 9 | 179 ± 10 | 179 ± 12 | 184 ± 8 | 175 ± 16 | 175 ± 15 |
| HRmax (% predicted) | 100 ± 6 | 94 ± 3 | 94 ± 5 | NA | NA | NA | NA |
| SBP response to exercise | |||||||
| SBPmax (mm Hg) | 224 ± 24 | 194 ± 20 | 200 ± 20 | 202 ± 20 | 177 ± 15 | 186 ± 24 | 161 ± 15 |
| SBP/W slope (mm Hg/W) | 0.28 ± 0.06 | 0.27 ± 0.11 | 0.34 ± 0.13 | 0.34 ± 0.12 | 0.53 ± 0.19 | 0.20 ± 0.06 | 0.25 ± 0.08 |
| SBP200 W (mm Hg) | 191 ± 17 | 184 ± 22 | 169 ± 18 | NA | NA | NA | NA |
| SBP/VO2 slope (mm Hg/L/min) | 30 ± 6 | 30 ± 15 | NA | NA | NA | 21 ± 7 | 26 ± 7 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Carlén, A.; Eklund, G.; Andersson, A.; Carlhäll, C.-J.; Ekström, M.; Hedman, K. Systolic Blood Pressure Response to Exercise in Endurance Athletes in Relation to Oxygen Uptake, Work Rate and Normative Values. J. Cardiovasc. Dev. Dis. 2022, 9, 227. https://0-doi-org.brum.beds.ac.uk/10.3390/jcdd9070227
Carlén A, Eklund G, Andersson A, Carlhäll C-J, Ekström M, Hedman K. Systolic Blood Pressure Response to Exercise in Endurance Athletes in Relation to Oxygen Uptake, Work Rate and Normative Values. Journal of Cardiovascular Development and Disease. 2022; 9(7):227. https://0-doi-org.brum.beds.ac.uk/10.3390/jcdd9070227
Chicago/Turabian StyleCarlén, Anna, Gustaf Eklund, August Andersson, Carl-Johan Carlhäll, Magnus Ekström, and Kristofer Hedman. 2022. "Systolic Blood Pressure Response to Exercise in Endurance Athletes in Relation to Oxygen Uptake, Work Rate and Normative Values" Journal of Cardiovascular Development and Disease 9, no. 7: 227. https://0-doi-org.brum.beds.ac.uk/10.3390/jcdd9070227