
Cardiotoxicity of Chemical Substances: An Emerging Hazard Class

 , , ,
, , ,  and
and 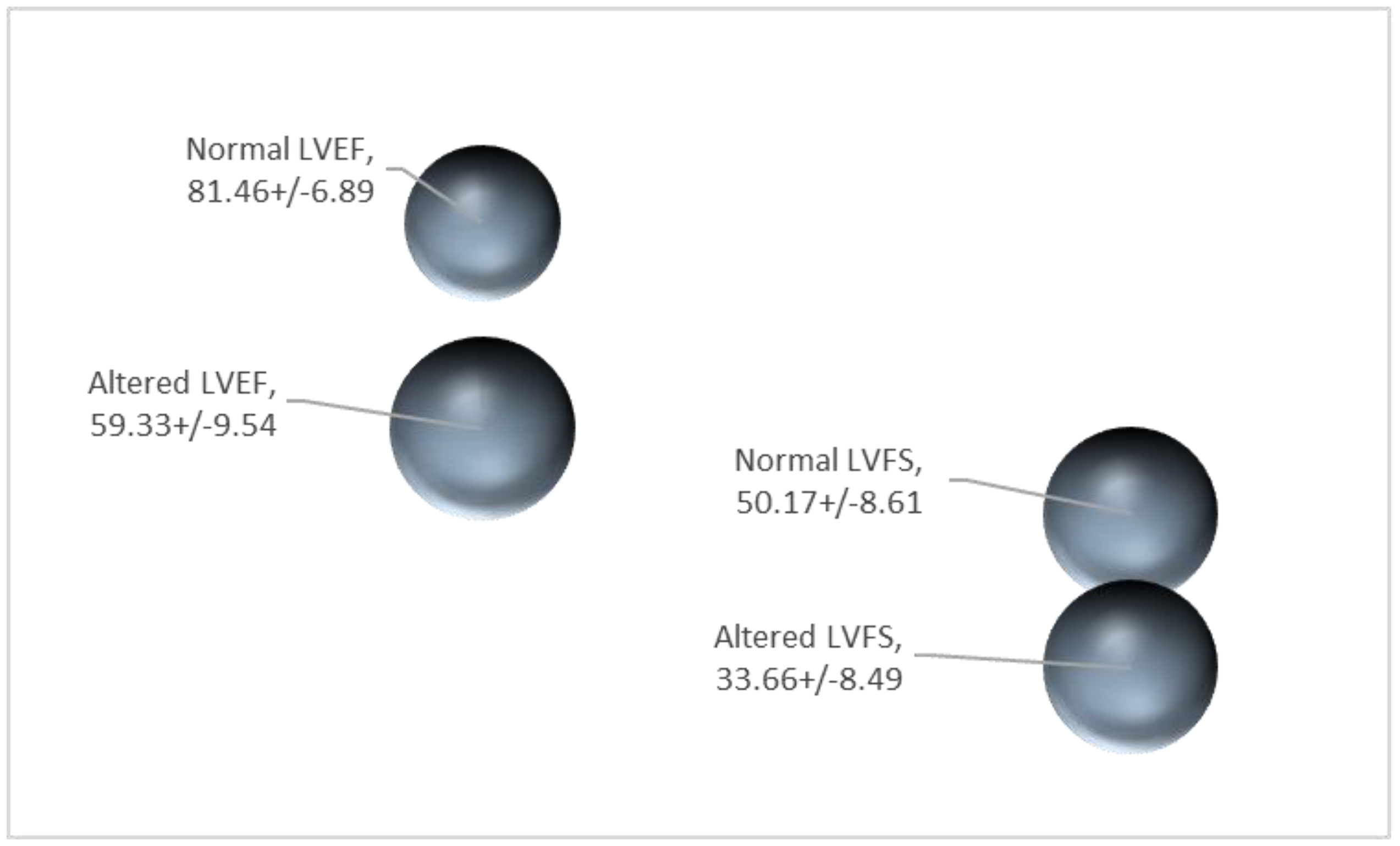{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
- ○
- Acute toxicity (oral, dermal, inhalation);
- ○
- Skin corrosion/skin irritation;
- ○
- Serious eye damage/eye irritation;
- ○
- Respiratory sensitization;
- ○
- Skin sensitization;
- ○
- Mutagenicity;
- ○
- Carcinogenicity;
- ○
- Toxicity for reproduction;
- ○
- Specific target organ toxicity (STOT) (single exposure, SE);
- ○
- Specific target organ toxicity (STOT) (repeated exposure, RE);
- ○
- Aspiration hazard.
- Anatomical and histopathological data;
- Echocardiographic data on contractility (e.g., LVEF, LVFS), documentation of cardiac frequency and/or implementation of other cardiac imaging modalities (e.g., MRI);
- Biochemical data, of generic nature (e.g., circulating oxidative stress markers), of more specific nature (e.g., oxidative stress markers of the cardiac tissue) and heart specific biomarkers (e.g., cardiac enzymes);
- Identification of pathways and mode of actions, which modulate the changes observed in different parameters after exposure to chemicals;
- In silico data, such as adverse outcome pathways (AOPs), omics, in vitro, organs on a chip, physiologically based pharmacokinetic models (PBPK), etc.
2. Current Definition of Cardiotoxicity
3. Roadmap for Identifying Regulatory Criteria on Cardiotoxicity Based on Animal Studies
4. Evaluation of Preliminary Results in Order to Identify Classification Criteria
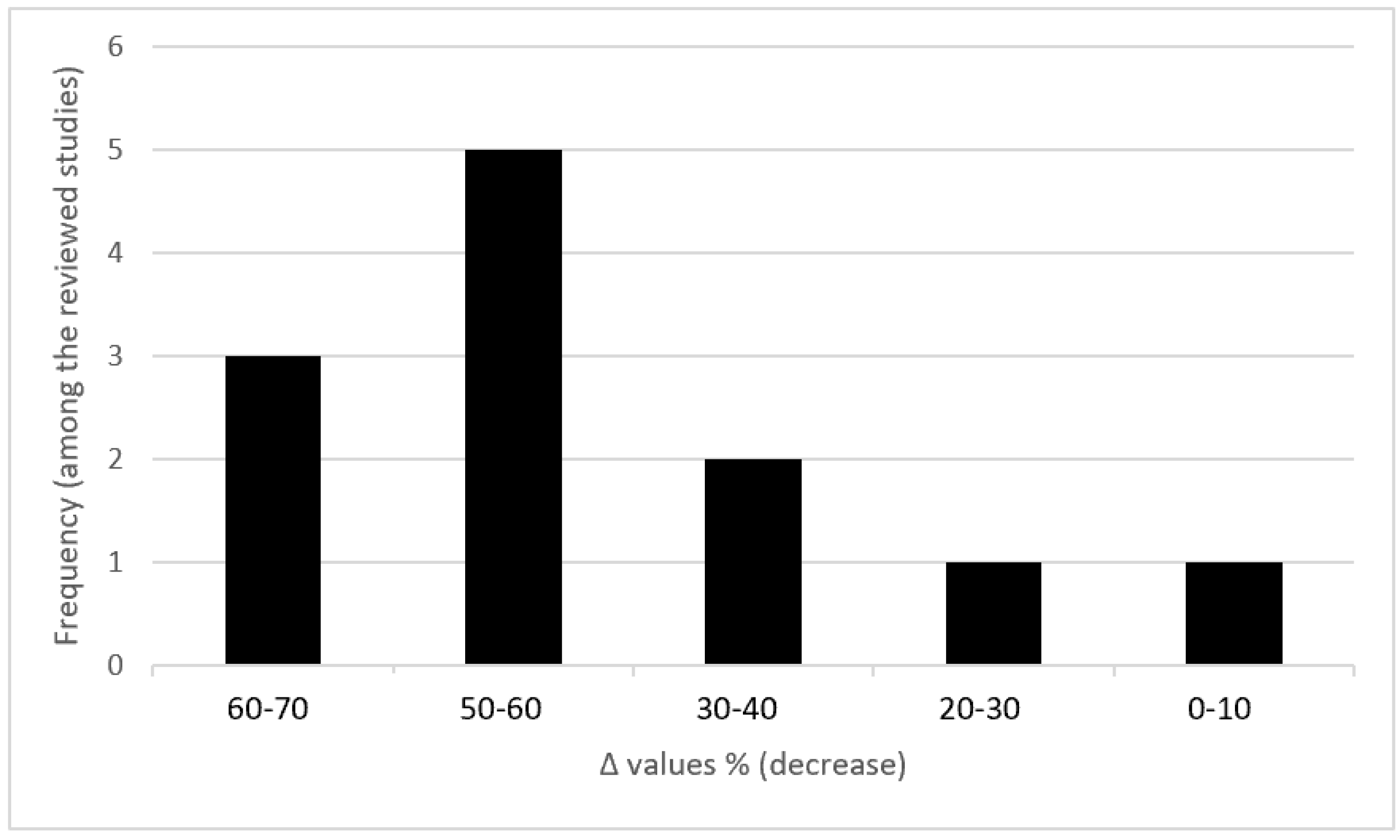
4.1. Echocardiography Indices
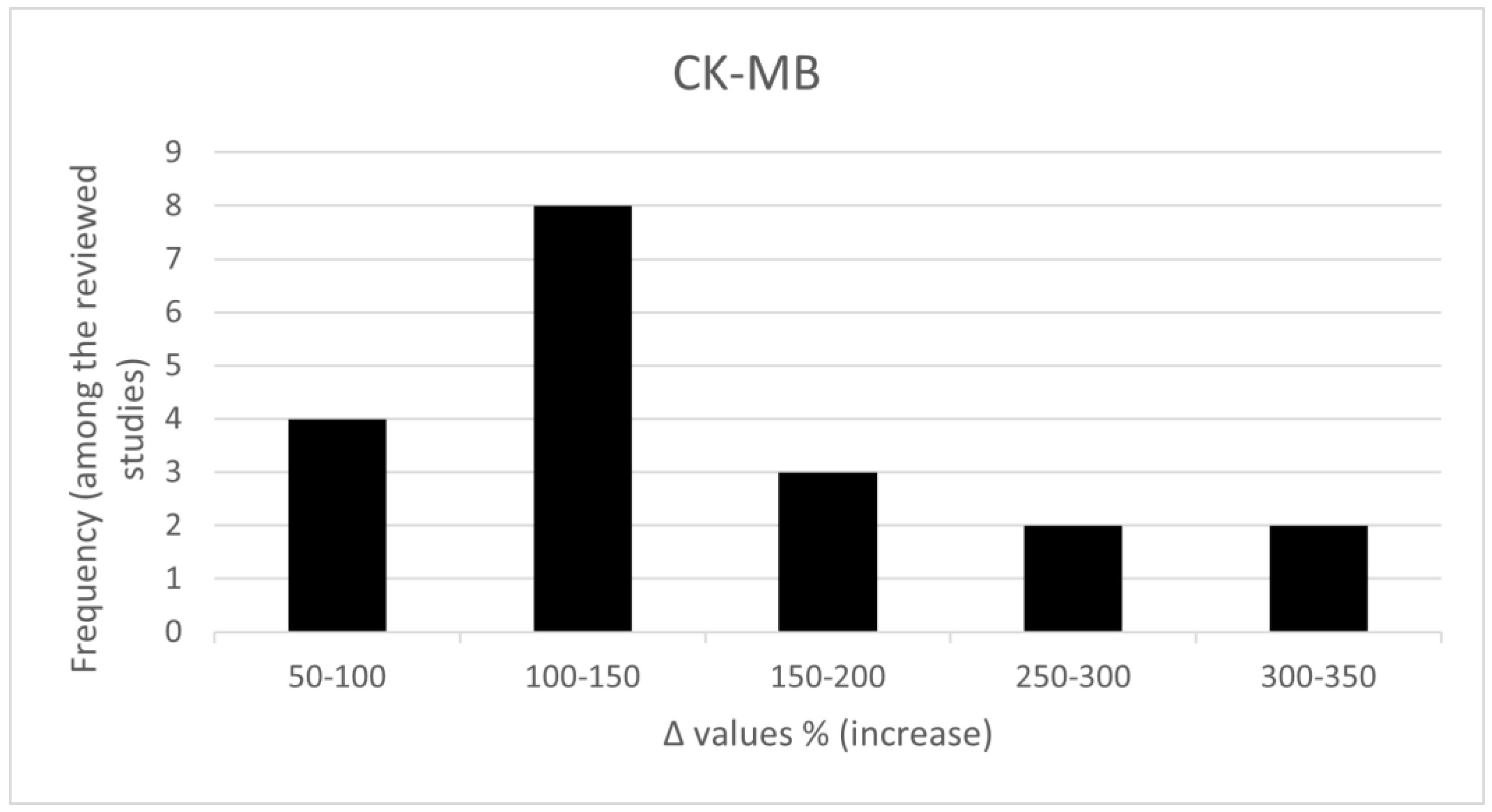
4.2. Biochemical Biomarkers
- Catalase (CAT)
- Malondialdehyde (MDA)
- Reactive oxygen species (ROS)
- Superoxide dismutase (SOD)
- Total antioxidant capacity (TAC)
- Total Oxidant Status (TOS)
- Glutathione (GSH)
- Glutathione peroxidase (GSH-Px)
- Lipid hydroperoxide (LH)
- Lactate dehydrogenase (LDH)
- Creatine kinase (CK)
- Creatine kinase-myocardial band isoenzyme (CK-MB)
- Cardiac troponin I (cTnI)
- Cardiac troponin T (cTnT)
- Atrial natriuretic peptide (ANP)
- Brain natriuretic peptide (BNP)
- Interleukin-1 family members (IL-1)
- TNF alpha
5. Future Perspectives and Reflections
- Identification of the appropriate animal species and strain;
- Identification of the lines of scientific evidence (e.g., histopathological, biochemical, echocardiographic indices etc.) from animal studies with relevance to humans;
- Meta-analysis of each line of scientific evidence recognized by animal species after exposure to well-established cardiotoxicants to humans (e.g., anthracyclines) in order to identify threshold values or range of normal and/ or altered values due to exposure;
- Validation of the above described evidence in animals exposed to other alleged cardiotoxic substances (e.g., AAS and pesticides);
- Establishment of mechanisms of action based on information either of known or alleged cardiotoxicants and association thereof with the parameters introduced as scientific evidence in the development of classification criteria;
- Discussion and introduction of novel indices and in silico methods.
Author Contributions
Funding
Conflicts of Interest
Abbreviations
References
- Sirenko, O.; Grimm, F.A.; Ryan, K.R.; Iwata, Y.; Chiu, W.A.; Parham, F.; Wignall, J.A.; Anson, B.; Cromwell, E.F.; Behl, M.; et al. In Vitro cardiotoxicity assessment of environmental chemicals using an organotypic human induced pluripotent stem cell-derived model. Toxicol. Appl. Pharmacol. 2017, 322, 60–74. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berardi, R.; Caramanti, M.; Savini, A.; Chiorrini, S.; Pierantoni, C.; Onofri, A.; Ballatore, Z.; De Lisa, M.; Mazzanti, P.; Cascinu, S. State of the art for cardiotoxicity due to chemotherapy and to targeted therapies: A literature review. Crit. Rev. Oncol./Hematol. 2013, 88, 75–86. [Google Scholar] [CrossRef] [PubMed]
- Germanakis, I.; Tsarouhas, K.; Fragkiadaki, P.; Tsitsimpikou, C.; Goutzourelas, N.; Champsas, M.C.; Stagos, D.; Rentoukas, E.; Tsatsakis, A.M. Oxidative stress and myocardial dysfunction in young rabbits after short term anabolic steroids administration. Food Chem. Toxicol. 2013, 61, 101–105. [Google Scholar] [CrossRef] [PubMed]
- Madeddu, C.; Deidda, M.; Piras, A.; Cadeddu, C.; Demurtas, L.; Puzzoni, M.; Piscopo, G.; Scartozzi, M.; Mercuro, G. Pathophysiology of cardiotoxicity induced by nonanthracycline chemotherapy. J. Cardiovasc. Med. 2016, 17 (Suppl. 1), e12–e18. [Google Scholar] [CrossRef] [PubMed]
- Vasilaki, F.; Tsitsimpikou, C.; Tsarouhas, K.; Germanakis, I.; Tzardi, M.; Kavvalakis, M.; Ozcagli, E.; Kouretas, D.; Tsatsakis, A.M. Cardiotoxicity in rabbits after long-term nandrolone decanoate administration. Toxicol. Lett. 2016, 241, 143–151. [Google Scholar] [CrossRef]
- Baggish, A.L.; Weiner, R.B.; Kanayama, G.; Hudson, J.I.; Lu, M.T.; Hoffmann, U.; Pope, H.G., Jr. Cardiovascular Toxicity of Illicit Anabolic-Androgenic Steroid Use. Circulation 2017, 135, 1991–2002. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sobczuk, P.; Czerwinska, M.; Kleibert, M.; Cudnoch-Jedrzejewska, A. Anthracycline-induced cardiotoxicity and renin-angiotensin-aldosterone system-from molecular mechanisms to therapeutic applications. Heart Fail. Rev. 2022, 27, 295–319. [Google Scholar] [CrossRef] [PubMed]
- Hashemzaei, M.; Karami, S.; Delaramifar, A.; Sheidary, A.; Tabrizian, K.; Rezaee, R.; Shahsavand, S.; Arsene, A.; Tsatsakis, A.; Taghdisi, S.M. Anticancer effects of co-administration of daunorubicin and resveratrol in MOLT-4, U266 B1 and Raji cell lines. Farmacia 2016, 64, 36–42. [Google Scholar]
- Iranshahi, M.; Barthomeuf, C.; Bayet-Robert, M.; Chollet, P.; Davoodi, D.; Piacente, S.; Rezaee, R.; Sahebkar, A. Drimane-Type Sesquiterpene Coumarins from Ferula gummosa Fruits Enhance Doxorubicin Uptake in Doxorubicin-Resistant Human Breast Cancer Cell Line. J. Tradit. Complement. Med. 2014, 4, 118–125. [Google Scholar] [CrossRef] [Green Version]
- Schwarz, E.R.; Pollick, C.; Dow, J.; Patterson, M.; Birnbaum, Y.; Kloner, R.A. A small animal model of non-ischemic cardiomyopathy and its evaluation by transthoracic echocardiography. Cardiovasc. Res. 1998, 39, 216–223. [Google Scholar] [CrossRef] [Green Version]
- Varga, Z.V.; Ferdinandy, P.; Liaudet, L.; Pacher, P. Drug-induced mitochondrial dysfunction and cardiotoxicity. Am. J. Physiol.-Heart Circ. Physiol. 2015, 309, H1453–H1467. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zamorano, J.L.; Lancellotti, P.; Rodriguez Munoz, D.; Aboyans, V.; Asteggiano, R.; Galderisi, M.; Habib, G.; Lenihan, D.J.; Lip, G.Y.H.; Lyon, A.R.; et al. 2016 ESC Position Paper on cancer treatments and cardiovascular toxicity developed under the auspices of the ESC Committee for Practice Guidelines: The Task Force for cancer treatments and cardiovascular toxicity of the European Society of Cardiology (ESC). Eur. Heart J. 2016, 37, 2768–2801. [Google Scholar] [CrossRef] [PubMed]
- Plana, J.C.; Galderisi, M.; Barac, A.; Ewer, M.S.; Ky, B.; Scherrer-Crosbie, M.; Ganame, J.; Sebag, I.A.; Agler, D.A.; Badano, L.P.; et al. Expert consensus for multimodality imaging evaluation of adult patients during and after cancer therapy: A report from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J Am. Soc. Echocardiogr. 2014, 27, 911–939. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pardo Sanz, A.; Zamorano, J.L. ‘Cardiotoxicity’: Time to define new targets? Eur. Heart J. 2020, 41, 1730–1732. [Google Scholar] [CrossRef] [PubMed]
- Braam, S.R.; Tertoolen, L.; van de Stolpe, A.; Meyer, T.; Passier, R.; Mummery, C.L. Prediction of drug-induced cardiotoxicity using human embryonic stem cell-derived cardiomyocytes. Stem Cell Res. 2010, 4, 107–116. [Google Scholar] [CrossRef] [Green Version]
- Robert, J. Preclinical assessment of anthracycline cardiotoxicity in laboratory animals: Predictiveness and pitfalls. Cell Biol. Toxicol. 2007, 23, 27–37. [Google Scholar] [CrossRef]
- Georgiadis, N.; Tsarouhas, K.; Rezaee, R.; Nepka, H.; Kass, G.E.N.; Dorne, J.C.M.; Stagkos, D.; Toutouzas, K.; Spandidos, D.A.; Kouretas, D.; et al. What is considered cardiotoxicity of anthracyclines in animal studies. Oncol. Rep. 2020, 44, 798–818. [Google Scholar] [CrossRef]
- Tsarouhas, K.; Kochiadakis, G.E.; Docea, A.O. Chapter 23—Current and emerging concepts of cardiotoxicity. In Toxicological Risk Assessment and Multi-System Health Impacts from Exposure; Tsatsakis, A.M., Ed.; Academic Press-Elsevier: Cambridge, MA, USA, 2021; pp. 269–274. [Google Scholar]
- Georgiadis, N.; Tsarouhas, K.; Tsitsimpikou, C.; Vardavas, A.; Rezaee, R.; Germanakis, I.; Tsatsakis, A.; Stagos, D.; Kouretas, D. Pesticides and cardiotoxicity. Where do we stand? Toxicol. Appl. Pharmacol. 2018, 353, 1–14. [Google Scholar] [CrossRef]
- Bostan, H.B.; Rezaee, R.; Valokala, M.G.; Tsarouhas, K.; Golokhvast, K.; Tsatsakis, A.M.; Karimi, G. Cardiotoxicity of nano-particles. Life Sci. 2016, 165, 91–99. [Google Scholar] [CrossRef]
- Kim, K.W.; Won, Y.L.; Ko, K.S.; Heo, K.H.; Chung, Y.H. The effects of hazardous chemical exposure on cardiovascular disease in chemical products manufacturing workers. Toxicol. Res. 2012, 28, 269–277. [Google Scholar] [CrossRef] [Green Version]
- Jackstadt, R.; Hermeking, H. MicroRNAs as regulators and mediators of c-MYC function. Biochim. Biophys. Acta (BBA)-Gene Regul. Mech. Acta 2015, 1849, 544–553. [Google Scholar] [CrossRef] [PubMed]
- Gomez de Cedron, M.; Ramirez de Molina, A. Microtargeting cancer metabolism: Opening new therapeutic windows based on lipid metabolism. J. Lipid. Res. 2016, 57, 193–206. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schraml, E.; Hackl, M.; Grillari, J. MicroRNAs and toxicology: A love marriage. Toxicol. Rep. 2017, 4, 634–636. [Google Scholar] [CrossRef]
- Mikaelian, I.; Scicchitano, M.; Mendes, O.; Thomas, R.A.; Leroy, B.E. Frontiers in preclinical safety biomarkers: MicroRNAs and messenger RNAs. Toxicol. Pathol. 2013, 41, 18–31. [Google Scholar] [CrossRef] [Green Version]
- French, D.; Wu, A.H.B. Chapter 9.12—Cardiac Markers. In The Immunoassay Handbook, 4th ed.; Wild, D., Ed.; Elsevier: Amsterdam, The Netherlands; Oxford, UK, 2013; pp. 817–831. [Google Scholar]
- Yuan, M.; Zang, L.; Xu, A.; Gong, M.; Liu, Q.; Huo, B.; Wang, J.; Fu, H.; Tse, G.; Roever, L.; et al. Dynamic Changes of Serum Heart Type-Fatty Acid Binding Protein in Cancer Patients Treated with Immune Checkpoint Inhibitors. Front. Pharmacol. 2021, 12, 748677. [Google Scholar] [CrossRef] [PubMed]
- Manrique, C.; Park, M.; Tiwari, N.; Plana, J.C.; Garcia, M. Diagnostic Strategies for Early Recognition of Cancer Therapeutics-Related Cardiac Dysfunction. Clin. Med. Insights Cardiol. 2017, 11, 1179546817697983. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, E.; Lee, M.; Onwuanyi, A. Monitoring of chemotherapy induced left ventricular systolic dysfunction in breast cancer patients. J. Am. Coll. Cardiol. 2021, 77 (Suppl. 1), 3326. [Google Scholar] [CrossRef]
- Zafiropoulos, A.; Tsarouhas, K.; Tsitsimpikou, C.; Fragkiadaki, P.; Germanakis, I.; Tsardi, M.; Maravgakis, G.; Goutzourelas, N.; Vasilaki, F.; Kouretas, D.; et al. Cardiotoxicity in rabbits after a low-level exposure to diazinon, propoxur, and chlorpyrifos. Hum. Exp. Toxicol. 2014, 33, 1241–1252. [Google Scholar] [CrossRef]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Georgiadis, N.; Tsarouhas, K.; Dorne, J.-L.C.M.; Kass, G.E.N.; Laspa, P.; Toutouzas, K.; Koulaouzidou, E.A.; Kouretas, D.; Tsitsimpikou, C. Cardiotoxicity of Chemical Substances: An Emerging Hazard Class. J. Cardiovasc. Dev. Dis. 2022, 9, 226. https://0-doi-org.brum.beds.ac.uk/10.3390/jcdd9070226
Georgiadis N, Tsarouhas K, Dorne J-LCM, Kass GEN, Laspa P, Toutouzas K, Koulaouzidou EA, Kouretas D, Tsitsimpikou C. Cardiotoxicity of Chemical Substances: An Emerging Hazard Class. Journal of Cardiovascular Development and Disease. 2022; 9(7):226. https://0-doi-org.brum.beds.ac.uk/10.3390/jcdd9070226
Chicago/Turabian StyleGeorgiadis, Nikolaos, Konstantinos Tsarouhas, Jean-Lou C. M. Dorne, George E. N. Kass, Petroula Laspa, Konstantinos Toutouzas, Elisabeth A. Koulaouzidou, Dimitrios Kouretas, and Christina Tsitsimpikou. 2022. "Cardiotoxicity of Chemical Substances: An Emerging Hazard Class" Journal of Cardiovascular Development and Disease 9, no. 7: 226. https://0-doi-org.brum.beds.ac.uk/10.3390/jcdd9070226