
Biventricular versus Conduction System Pacing after Atrioventricular Node Ablation in Heart Failure Patients with Atrial Fibrillation


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Population
- (a)
- severely symptomatic AF/atrial flutter with rapid ventricular rate, refractory to pharmacological rate or rhythm control, unsuitable for catheter ablation or in which ablation had failed;
- (b)
- tachycardia-induced cardiomyopathy without other identifiable cause of reduced ejection fraction;
- (c)
- ejection fraction LVEF < 50%;
- (d)
- New York Heart Association (NYHA) class II–IV;
- (e)
- narrow QRS complex ≤ 120 ms;
- (f)
- the patient has provided written informed consent and was 18 years or older.
2.2. Procedures
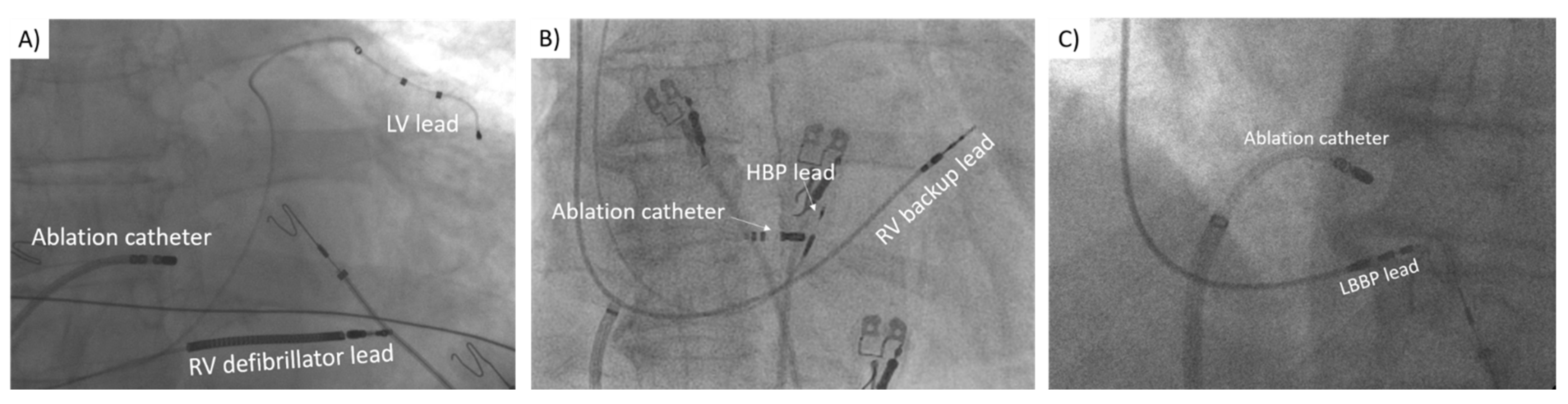
2.2.1. Biventricular Pacing
2.2.2. His Bundle Pacing
2.2.3. Left Bundle Branch Pacing
2.2.4. Atrioventricular Node Ablation
2.3. Outcomes and Follow-Up
2.4. Statistical Analyses
3. Results
3.1. Patient Characteristics
3.2. Procedural Outcomes
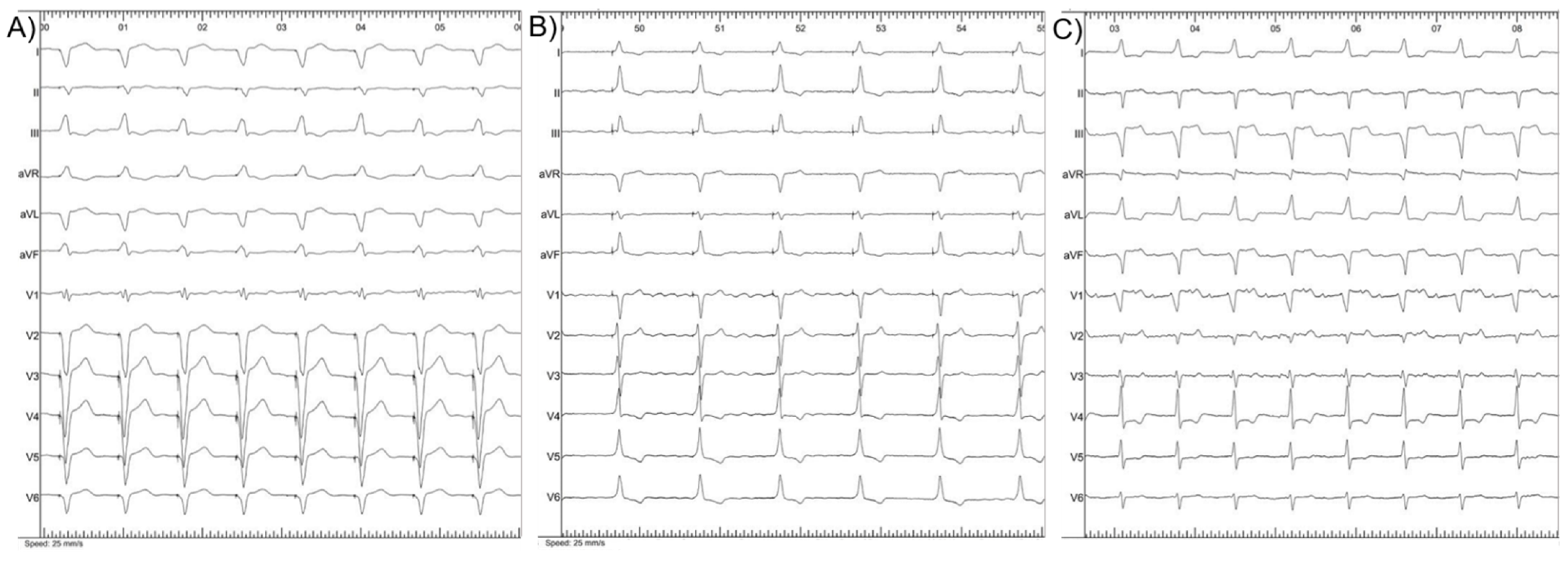
3.3. Electrical Parameters
3.4. Clinical Outcomes
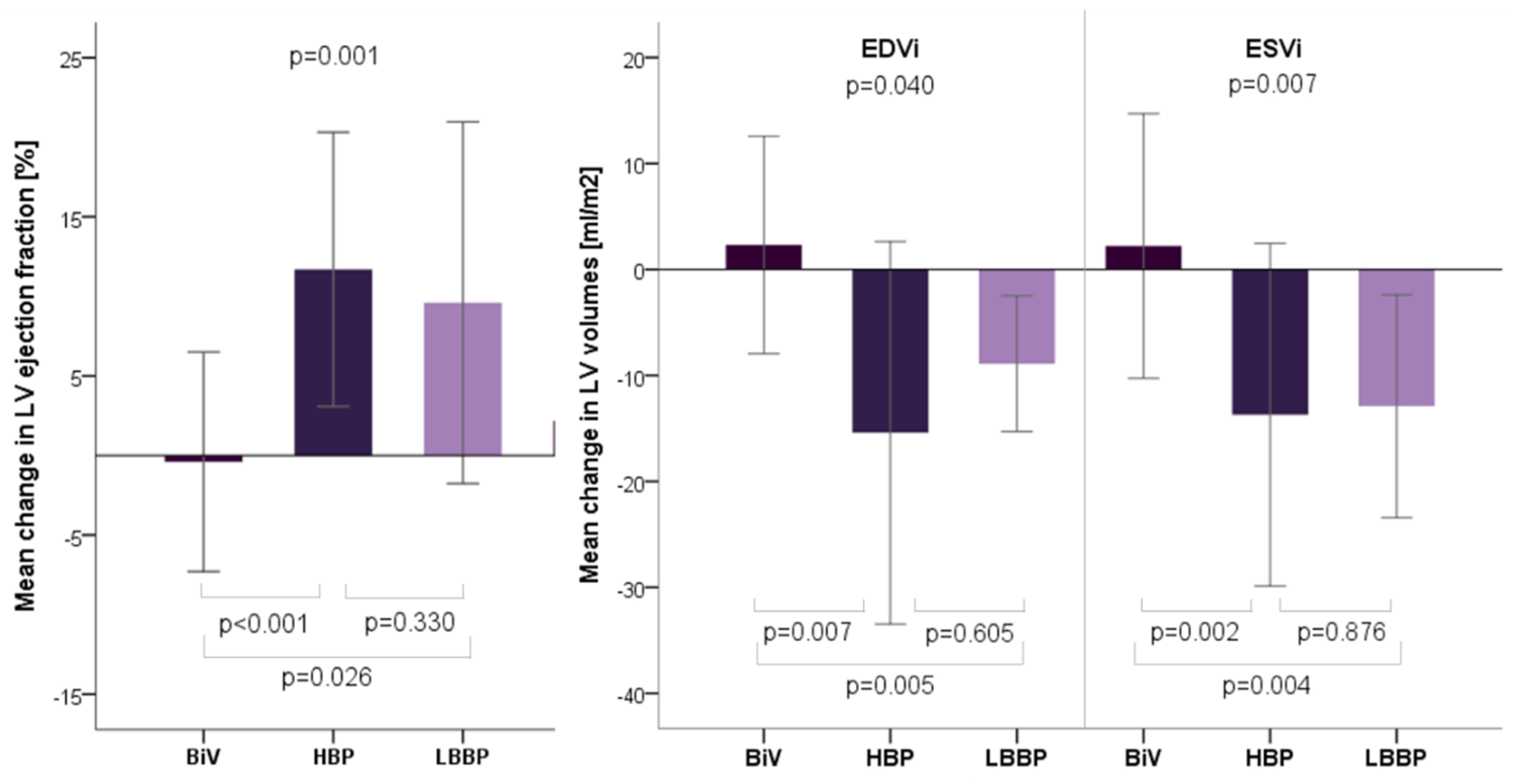
3.5. Echocardiographic Outcomes
4. Discussion
4.1. Procedures Assessment
4.2. Electocardiographic and Echocardiographic Outcomes
4.3. Clinical Outcomes
4.4. Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| CSP | conduction system pacing |
| HBP | His-bundle pacing |
| LBBP | left bundle branch pacing |
| BiV | biventricular |
| RV | right ventricle |
| LV | left ventricle |
| AVNA | atrioventricular node ablation |
| AF | atrial fibrillation |
| HF | heart failure |
| ESC | European Society of Cardiology |
| LVEF | left ventricle ejection fraction |
| LAVI | left atrial volume index |
| LVEDVi | LV end dyastolic volume index |
| LVESVi | LV end systolic volume index |
| NYHA | New York Heart Association |
| ICD | implantable cardioverter-defibrillator |
| ECG | electrocardiogram |
| NT-proBNP | N-terminal prohormone of brain natriuretic peptid (NT-proBNP) |
| GFR | glomerular filtration rate |
References
- Tan, E.; Rienstra, M.; Wiesfeld, A.; Schoonderwoerd, B.A.; Hobbel, H.H.; Van Gelder, I.C. Long-term outcome of the atrioventricular node ablation and pacemaker implantation for symptomatic refractory atrial fibrillation. Europace 2008, 10, 412–418. [Google Scholar] [CrossRef] [PubMed]
- Huang, W.; Su, L.; Wu, S. Pacing treatment of atrial fibrillation patients with heart failure: His bundle pacing combined with atrioventricular node ablation. Card. Electrophysiol. Clin. 2018, 10, 519–535. [Google Scholar] [CrossRef] [PubMed]
- Kay, G.N.; Ellenbogen, K.A.; Giudici, M.; Redfield, M.M.; Jenkins, L.S.; Mianulli, M.; Wilkoff, B. The Ablate and Pace Trial: A prospective study of catheter ablation of the AV conduction system and permanent pacemaker implantation for treatment of atrial fibrillation. APT Investigators. J. Interv. Card. Electrophysiol. 1998, 2, 121–135. [Google Scholar] [CrossRef] [PubMed]
- Tops, L.F.; Schalij, M.J.; Holman, E.R.; van Erven, L.; van der Wall, E.E.; Bax, J.J. Right ventricular pacing can induce ventricular dyssynchrony in patients with atrial fibrillation after atrioventricular node ablation. J. Am. Coll. Cardiol. 2006, 48, 1642–1648. [Google Scholar] [CrossRef]
- Stavrakis, S.; Garabelli, P.; Reynolds, D.W. Cardiac resynchronization therapy after atrioventricular junction ablation for symptomatic atrial fibrillation: A meta-analysis. Europace 2012, 14, 1490–1497. [Google Scholar] [CrossRef]
- Chatterjee, N.A.; Upadhyay, G.A.; Ellenbogen, K.A.; Palmisano, P.; Chieffo, E.; Occhetta, E.; Quartieri, F.; Calò, L.; Ungar, A.; Mont, L.; et al. Atrioventricular nodal ablation in atrial fibrillation: A meta-analysis of biventricular vs. right ventricular pacing mode. Eur. J. Heart Fail. 2012, 14, 661–667. [Google Scholar] [CrossRef] [Green Version]
- Brignole, M.; Botto, G.; Mont, L.; Iacopino, S.; De Marchi, G.; Oddone, D.; Luzi, M.; Tolosana, J.M.; Navazio, A.; Menozzi, C. Cardiac resynchronization therapy in patients undergoing atrioventricular junction ablation for permanent atrial fibrillation: A randomized trial. Eur. Heart J. 2011, 32, 2420–2429. [Google Scholar] [CrossRef] [Green Version]
- Brignole, M.; Pokushalov, E.; Pentimalli, F.; Palmisano, P.; Chieffo, E.; Occhetta, E.; Quartieri, F.; Calò, L.; Ungar, A.; Mont, L.; et al. A randomized controlled trial of atrioventricular junction ablation and cardiac resynchronization therapy in patients with permanent atrial fibrillation and narrow QRS. Eur. Heart J. 2018, 39, 3999–4008. [Google Scholar] [CrossRef]
- Brignole, M.; Pentimalli, F.; Palmisano, P.; Landolina, M.; Quartieri, F.; Occhetta, E.; Calò, L.; Mascia, G.; Mont, L.; Vernooy, K.; et al. APAF-CRT Trial Investigators. AV junction ablation and cardiac resynchronization for patients with permanent atrial fibrillation and narrow QRS: The APAF-CRT mortality trial. Eur. Heart J. 2021, 42, 4731–4739. [Google Scholar] [CrossRef]
- Deshmukh, P.; Casavant, D.A.; Romanyshyn, M.; Anderson, K. Permanent, direct His-bundle pacing: A novel approach to cardiac pacing in patients with normal His-Purkinje activation. Circulation 2000, 101, 869–877. [Google Scholar] [CrossRef] [Green Version]
- Vijayaraman, P.; Subzposh, F.A.; Naperkowski, A. Atrioventricular node ablation and His bundle pacing. Europace 2017, 19, iv10–iv16. [Google Scholar] [CrossRef]
- Huang, W.; Su, L.; Wu, S.; Xu, L.; Xiao, F.; Zhou, X.; Ellenbogen, K.A. Benefits of permanent His bundle pacing combined with a-trioventricular node ablation in atrial fibrillation patients with heart failure with both preserved and reduced left ventricular ejection fraction. J Am. Heart Assoc. 2017, 6, e005309. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, W.; Su, L.; Wu, S.; Xu, L.; Xiao, F.; Zhou, X.; Ellenbogen, K.A. A novel pacing strategy with low and stable output: Pacing the left bundle branch immediately beyond the conduction block. Can. J. Cardiol. 2017, 33, 1736.e1–1736.e3. [Google Scholar] [CrossRef] [PubMed]
- Occhetta, E.; Bortnik, M.; Magnani, A.; Francalacci, G.; Piccinino, C.; Plebani, L.; Marino, P. Prevention of ventricular desynchronization by permanent para-Hisian pacing after atrioventricular node ablation in chronic atrial fibrillation: A crossover, blinded, randomized study versus apical right ventricular pacing. J. Am. Coll. Cardiol. 2006, 47, 1938–1945. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muthumala, A.; Vijayaraman, P. His-Purkinje conduction system pacing and atrioventricular node ablation. Herzschrittmacherther. Elektrophysiol. 2020, 31, 117–123. [Google Scholar] [CrossRef]
- Padala, S.K.; Ellenbogen, K.A. Pacing of Specialized Conduction System. Card. Electrophysiol. Clin. 2021, 13, 755–784. [Google Scholar] [CrossRef]
- Wang, S.; Wu, S.; Xu, L.; Xiao, F.; Whinnett, Z.I.; Vijayaraman, P.; Su, L.; Huang, W. Feasibility and efficacy of His bundle pacing or left bundle pacing combined with atrioventricular node ablation in patients with persistent atrial fibrillation and implantable cardioverter-defibrillator therapy. J. Am. Heart Assoc. 2019, 8, e014253. [Google Scholar] [CrossRef] [PubMed]
- Brugada, J.; Katritsis, D.G.; Arbelo, E.; Arribas, F.; Bax, J.J.; Blomström-Lundqvist, C.; Calkins, H.; Corrado, D.; Deftereos, S.G.; Diller, G.-P.; et al. 2019 ESC Guidelines for the management of patients with supraventricular tachycardia The Task Force for the management of patients with supraventricular tachycardia of the European Society of Cardiology (ESC). Eur. Heart J. 2020, 41, 655–720. [Google Scholar] [CrossRef] [Green Version]
- Žižek, D.; Antolič, B.; Mežnar, A.Z.; Zavrl-Džananović, D.; Jan, M.; Štublar, J.; Pernat, A. Biventricular versus His bundle pacing after atrioventricular node ablation in heart failure patients with narrow QRS. Acta Cardiol. 2021, 2, 1–9. [Google Scholar] [CrossRef]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: Developed by the Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). With the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. J. Heart Fail. 2022, 24, 4–131. [Google Scholar]
- Vijayaraman, P.; Dandamudi, G. Anatomical approach to permanent His bundle pacing: Optimizing His bundle capture. J. Electrocardiol. 2016, 49, 649–657. [Google Scholar] [CrossRef] [PubMed]
- Gu, M.; Hu, Y.; Hua, W.; Niu, H.; Chen, X.; Cai, M.; Zhang, N.; Li, H.; Zhou, X.; Zhang, S. Visualization of tricuspid valve annulus for implantation of His bundle pacing in patients with symptomatic bradycardia. J Cardiovasc Electrophysiol. 2019, 30, 2164–2169. [Google Scholar] [CrossRef] [PubMed]
- Huang, W.; Chen, X.; Su, L.; Wu, S.; Xia, X.; Vijayaraman, P. A beginner’s guide to permanent left bundle branch pacing. Heart Rhythm. 2019, 16, 1791–1796. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhuo, W.; Zhong, X.; Liu, H.; Yu, j.; Chen, Q.; Hu, J.; Xiong, Q.; Hong, K. Pacing Characteristics of His Bundle Pacing vs. Left Bundle Branch Pacing: A Systematic Review and Meta-Analysis. Front. Cardiovasc. Med. 2022, 9, 849143. [Google Scholar] [CrossRef]
- Yuan, Z.; Cheng, L.; Wu, Y. Meta-Analysis Comparing Safety and Efficacy of Left Bundle Branch Area Pacing Versus His Bundle Pacing. Am. J. Cardiol. 2022, 164, 64–72. [Google Scholar] [CrossRef] [PubMed]
- Shah, R.M.; Patel, D.; Molnar, J.; Ellenbogen, K.A.; Koneru, J.N. Cardiac-resynchronization therapy in patients with systolic heart failure and QRS interval ≤130 ms: Insights from a meta-analysis. Europace 2015, 17, 267–273. [Google Scholar] [CrossRef]
- Khan, M.N.; Jaïs, P.; Cummings, J.; Di Biase, L.; Sanders, P.; Martin, D.O.; Kautzner, J.; Hao, S.; Themistoclakis, S.; Fanelli, R.; et al. PABA-CHF Investigators. Pulmonary-vein isolation for atrial fibrillation in patients with heart failure. N. Engl. J. Med. 2008, 359, 1778–1785. [Google Scholar] [CrossRef] [Green Version]
- Su, L.; Wang, S.; Wu, S.; Xu, L.; Huang, Z.; Chen, X.; Zheng, R.; Jiang, L.; Ellenbogen, K.A.; Whinnett, Z.I.; et al. Long-Term Safety and Feasibility of Left Bundle Branch Pacing in a Large Single-Center Study. Circ Arrhythm. Electrophysiol. 2021, 14, e009261. [Google Scholar] [CrossRef]
- Moriña-Vázquez, P.; Moraleda-Salas, M.T.; Arce-León, Á.; Venegas-Gamero, J.; Fernández-Gómez, J.M.; Díaz-Fernández, J.F. Effectiveness and safety of AV node ablation after His bundle pacing in patients with uncontrolled atrial arrhythmias. Pacing Clin. Electrophysiol. 2021, 44, 1004–1009. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| BiV (n = 13) | HBP (n = 27) | LBBP (n = 10) | p Value | |
|---|---|---|---|---|
| Characteristics | ||||
| Age [years] | 70 (67–73.5) | 71 (62–75) | 69 (67–78) | 0.888 |
| Male sex | 7 (53.8%) | 10 (37.0%) | 7 (70.0%) | 0.196 |
| QRS [ms] | 98 (±7) | 100 (±13) | 105 (±15) | 0.145 |
| Heart rate [bpm] | 128 (113–137) | 133 (123–141) | 127 (97–132) | 0.278 |
| Atrial flutter | 2 (15.4%) | 6 (22.2%) | 3 (30.0%) | 0.815 |
| LVEF [%] | 38 (35–40) | 39 (30–45) | 28 (20–42) | 0.135 |
| LAVI [mL/m2] | 55 (±11) | 55 (±11) | 59 (±14) | 0.975 |
| Initial median NYHA class | 3 | 3 | 3 | 0.175 |
| Comorbidities | ||||
| AH | 9 (69.2%) | 17 (63.0%) | 8 (80.0%) | 0.665 |
| Diabetes | 3 (23.1%) | 8 (29.6%) | 2 (20.0%) | 0.914 |
| CAD | 6 (46.2%) | 6 (22.2%) | 4 (40.0%) | 0.260 |
| Medication | ||||
| ACEi/ARB/ARNI | 9 (69.2%) | 20 (74.1%) | 6 (60.0%) | 0.716 |
| MRA | 7 (53.8%) | 9 (33.3%) | 5 (50.0%) | 0.434 |
| BB | 13 (100%) | 25 (92.6%) | 9 (90.0%) | 0.767 |
| Digoxin | 5 (38.5%) | 7 (25.9%) | 2 (20.0%) | 0.640 |
| Amiodarone | 2 (15.4%) | 6 (22.2%) | 1 (10.0%) | 0.887 |
| Anticoagulation | 13 (100%) | 25 (92.6%) | 10 (100%) | 1 |
| Loop diuretic | 7 (53.8%) | 17 (63.0%) | 7 (70.0%) | 0.794 |
| BiV (n = 13) | HBP (n = 27) | LBBP (n = 10) | p Value | |
|---|---|---|---|---|
| Electrocardiographic characteristics | ||||
| Baseline QRS [ms] | 98 (±7) | 100 (±13) | 98 (±7) | 0.145 |
| Post-implant QRS [ms] | 172 (±13) | 105 (±17)) | 127 (±13) | <0.001 |
| Lead measurements | ||||
| Initial CSP/LV threshold [V] | 1.4 (1.1–1.75) | 1.25 (1–2) | 0.8 (0.5–1.1) | 0.006 |
| Initial CSP/LV impedance [ohm] | 760 (±229) | 526 (±87) | 750 (±77) | <0.001 |
| BiV (n = 13) | HBP (n = 25) * | LBBP (n = 10) | |
|---|---|---|---|
| Initial CSP/LV threshold [V] | 1.4 (1.1–1.75) | 1.25 (0.875–1.9) | 0.8 (0.5–1.1) |
| Follow-up CSP/LV threshold [V] | 1.5 (1–1.625) | 0.75 (0.5–1.875) | 0.8 (0.5–1) |
| p value: initial vs. follow-up | 0.765 | 0.370 | 0.799 |
| Initial CSP/LV impedance [ohm] | 760 (±229) | 526 (±90) | 749 (±77) |
| Follow-up CSP/LV impedance [ohm] | 682 (±161) | 465 (±72) | 594 (±137) |
| p value: initial vs. follow-up | 0.142 | 0.008 | 0.002 |
| BiV (n = 13) | HBP (n = 25) | LBBP (n = 10) | p Value—Comparing Groups | |
|---|---|---|---|---|
| NYHA class | ||||
| Initial median NYHA class | 3 | 3 | 3 | 0.175 |
| Nb. in NYHA class 2 | 1 (7.7%) | 2 (8.0%) | 4 (40.0%) | |
| Nb. in NYHA class 3 | 11 (84.6%) | 18 (72.0%) | 5 (50.0%) | |
| Nb. in NYHA class 4 | 1 (7.7%) | 5 (20.0%) | 1 (10.0%) | |
| Follow-up median NYHA class | 3 | 2 | 2 | 0.059 |
| Nb. in NYHA class 1 | 0 | 5 (20.0%) | 4 (40.0%) | |
| Nb. in NYHA class 2 | 6 (46.2%) | 15 (60,0%) | 5 (50.0%) | |
| Nb. in NYHA class 3 | 6 (46.2%) | 5 (20.0%) | 1 (10.0%) | |
| Nb. in NYHA class 4 | 1 (7.7%) | 0 | 0 | |
| p value: initial vs. follow-up | 0.096 | <0.001 | 0.008 | |
| Loop diuretics | ||||
| Initial | 7 (53.8%) | 17 (63.0%) | 7 (70.0%) | 0.8 |
| Follow-up | 6 (46.2%) | 9 (33.3%) | 6 (60.0%) | 0.403 |
| p value: initial vs. follow-up | 0.564 | 0.014 | 0.564 | |
| NT-proBNP [pg/mL] | ||||
| Initial | 1908 (1215–2825) | 2800 (1257–5977) | 2689 (1603–5710) | 0.339 |
| Follow-up | 1856 (1195–2505) | 1472 (904–2113) | 1632 (861–5028) | 0.599 |
| p value: initial vs. follow-up | 0.311 | 0.001 | 0.047 | |
| eGFR [mL/min/1.73 m2] | ||||
| Initial | 58 (51–62) | 52 (45–61) | 66 (35–84) | 0.240 |
| Follow-up | 60 (49–66) | 67 (55–73) | 79 (41–90) | 0.214 |
| p value: initial vs. follow-up | 0.349 | 0.001 | 0.033 | |
| BiV (n = 13) | HBP (n = 25) * | LBBP (n = 10) | |
|---|---|---|---|
| Initial LVEF [%] | 38 (35–40) | 39 (31–46) | 28 (20–43) |
| Follow-up LVEF [%] | 37 (35–41) | 49 (42–58) | 40 (31–44) |
| p value: initial vs. follow-up | 0.916 | <0.001 | 0.041 |
| Initial LVEDVi [mL/m2] | 82 (±17) | 72 (±21) | 89 (±22) |
| Follow-up LVEDVi [mL/m2] | 84 (±19) | 61 (±18) | 81 (±21) |
| p value: initial vs. follow-up | 0.509 | 0.006 | 0.002 |
| Initial LVESVi [mL/m2] | 51 (±12) | 45 (±18) | 63 (±21) |
| Follow-up LVESVi [mL/m2] | 53 (±14) | 32 (±13) | 50 (±18) |
| p value: initial vs. follow-up | 0.551 | <0.001 | 0.004 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ivanovski, M.; Mrak, M.; Mežnar, A.Z.; Žižek, D. Biventricular versus Conduction System Pacing after Atrioventricular Node Ablation in Heart Failure Patients with Atrial Fibrillation. J. Cardiovasc. Dev. Dis. 2022, 9, 209. https://0-doi-org.brum.beds.ac.uk/10.3390/jcdd9070209
Ivanovski M, Mrak M, Mežnar AZ, Žižek D. Biventricular versus Conduction System Pacing after Atrioventricular Node Ablation in Heart Failure Patients with Atrial Fibrillation. Journal of Cardiovascular Development and Disease. 2022; 9(7):209. https://0-doi-org.brum.beds.ac.uk/10.3390/jcdd9070209
Chicago/Turabian StyleIvanovski, Maja, Miha Mrak, Anja Zupan Mežnar, and David Žižek. 2022. "Biventricular versus Conduction System Pacing after Atrioventricular Node Ablation in Heart Failure Patients with Atrial Fibrillation" Journal of Cardiovascular Development and Disease 9, no. 7: 209. https://0-doi-org.brum.beds.ac.uk/10.3390/jcdd9070209