
A Comparative Study on Surgical Treatment of Valvular Heart Disease between High-Volume Cardiac Centers in China and STS Data

Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source
2.2. Patients
2.3. Statistical Analysis
3. Results
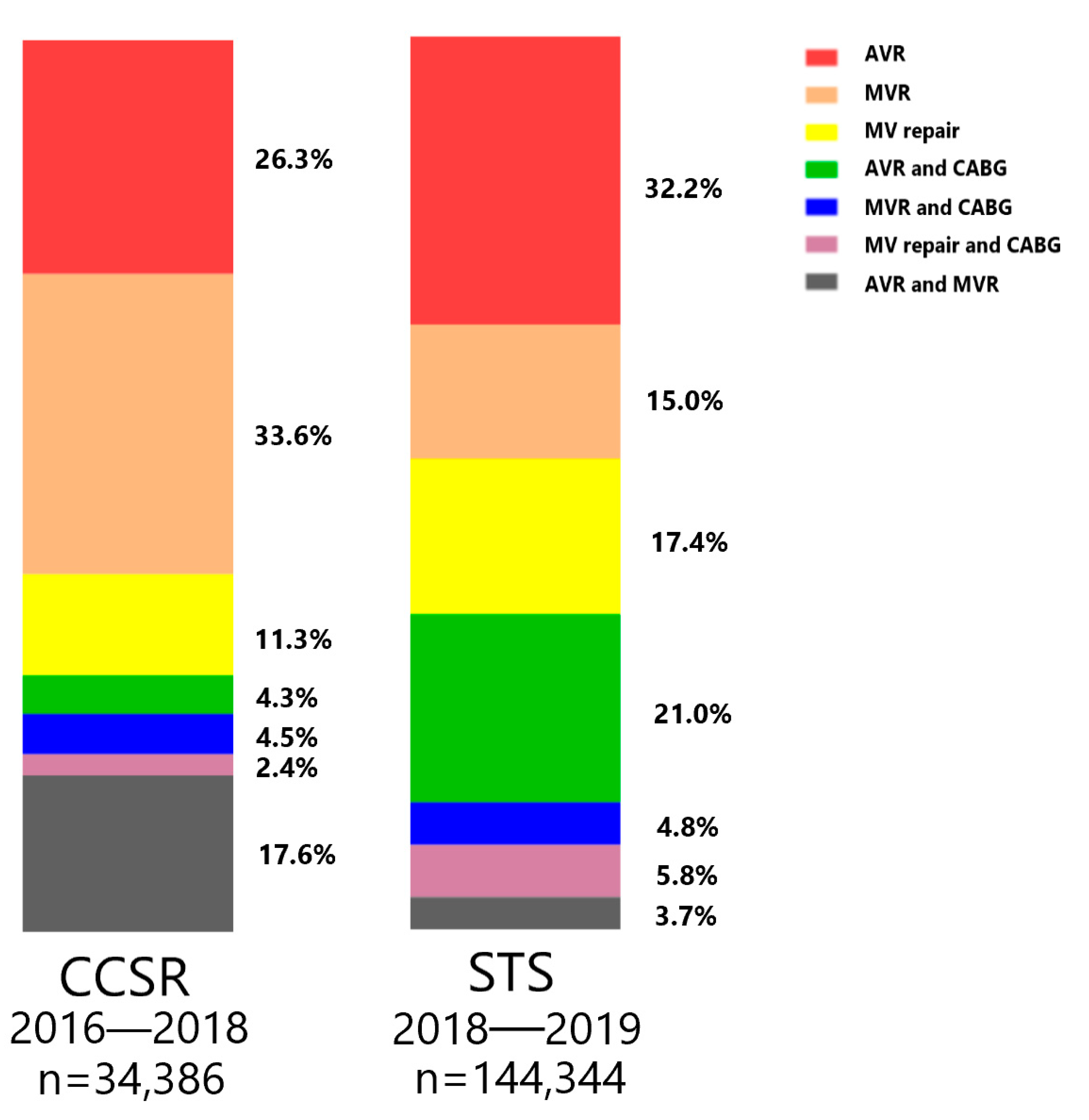
3.1. Proportions of More Commonly Performed VHD Surgeries
3.2. Trends in VHD Surgical Procedures
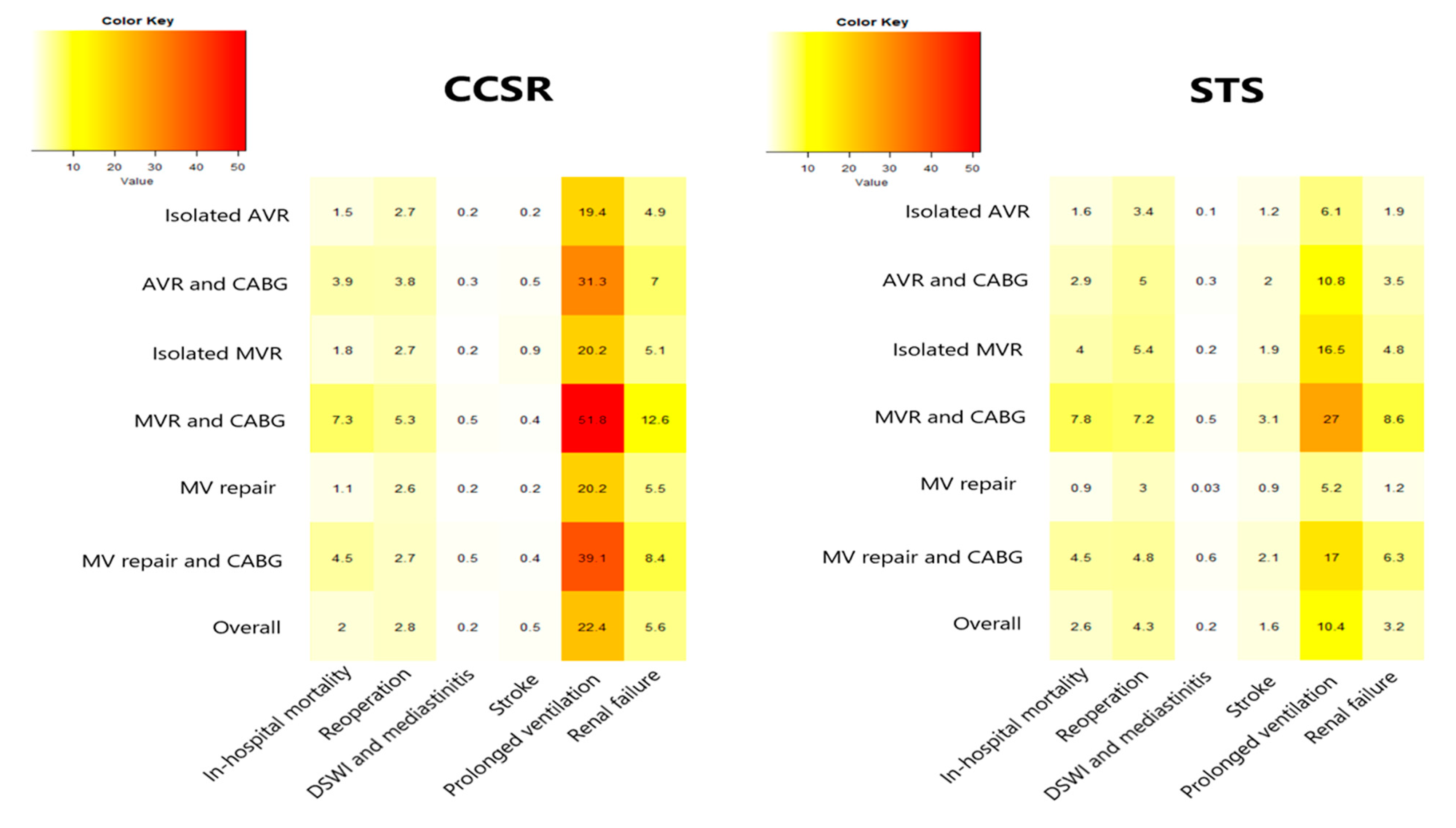
3.3. Distribution of In-Hospital Mortality and Other Major Complications Rates in Different Procedures
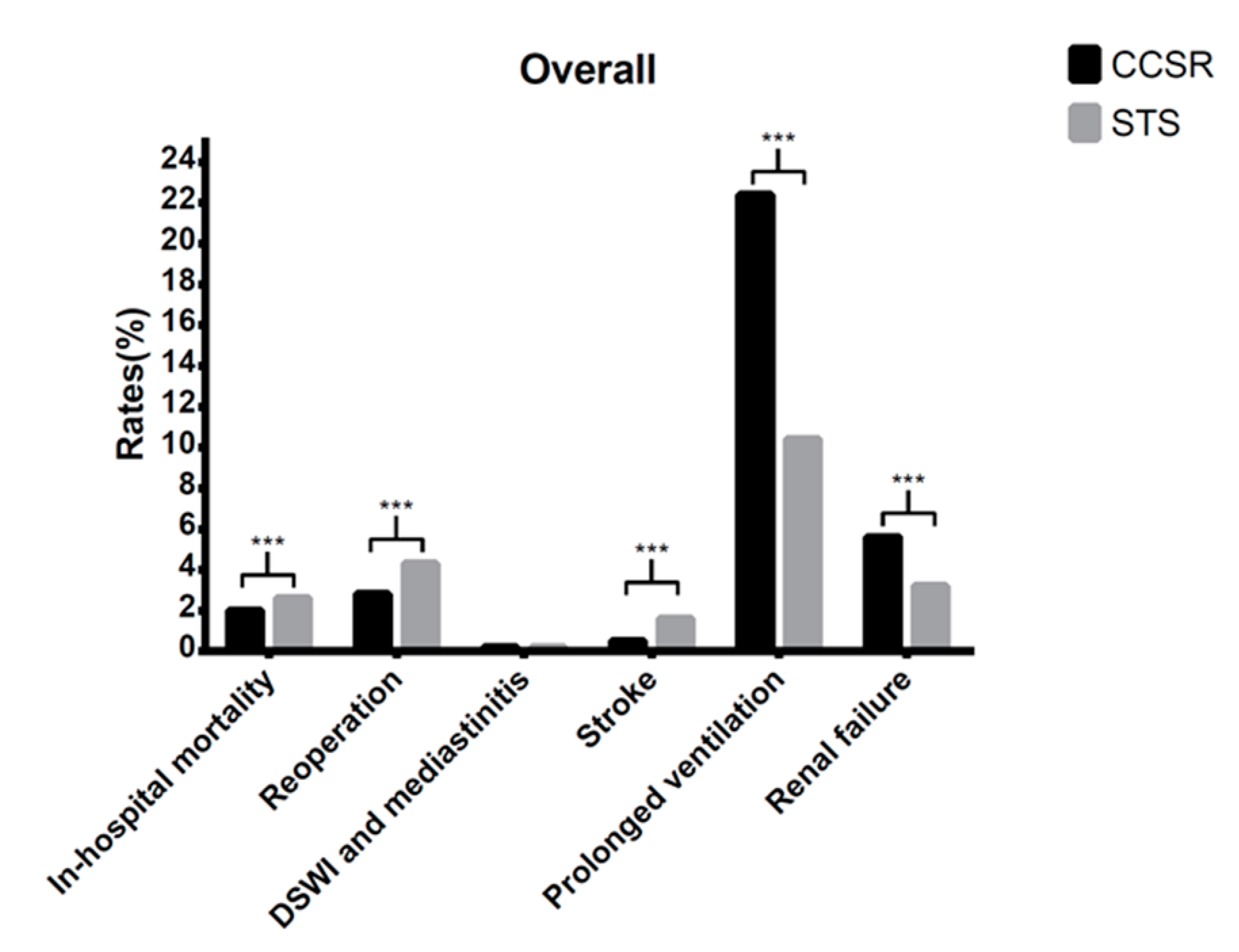
3.4. Comparison of Outcomes in the Whole Cohort between CCSR and STS data
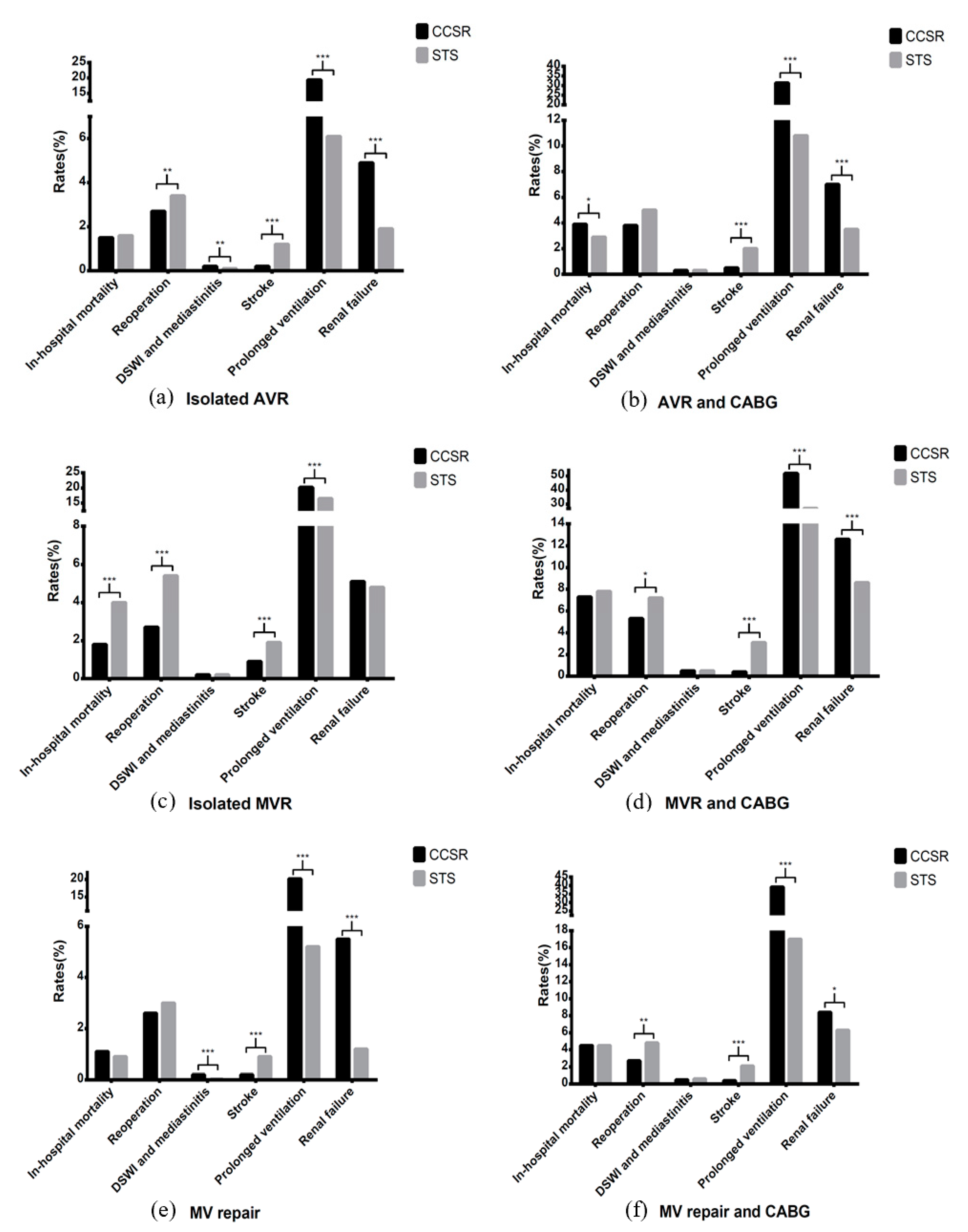
3.5. Comparison of Outcomes in Different Procedures between CCSR and STS data
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Liu, S.; Li, Y.; Zeng, X.; Wang, H.; Zhou, M. Burden of Cardiovascular Diseases in China, 1990–2016: Findings from the 2016 Global Burden of Disease Study. JAMA Cardiol. 2019, 4, 342–352. [Google Scholar] [CrossRef] [PubMed]
- Timmis, A.; Vardas, P.; Townsend, N.; Torbica, A.; Katus, H.; De Smedt, D.; Gale, C.P.; Maggioni, A.P.; Petersen, S.E.; Huculeci, R.; et al. European Society of Cardiology: Cardiovascular disease statistics 2021. Eur. Heart J. 2022, 43, 716–799. [Google Scholar] [CrossRef]
- Coffey, S.; Roberts-Thomson, R.; Brown, A.; Carapetis, J.; Chen, M.; Enriquez-Sarano, M.; Zühlke, L.; Prendergast, B.D. Global epidemiology of valvular heart disease. Nat. Rev. Cardiol. 2021, 18, 853–864. [Google Scholar] [CrossRef] [PubMed]
- Bowdish, M.E.; D’Agostino, R.S.; Thourani, V.H.; Schwann, T.A.; Krohn, C.; Desai, N.; Shahian, D.M.; Fernandez, F.G.; Badhwar, V. STS Adult Cardiac Surgery Database: 2021 Update on Outcomes, Quality, and Research. Ann. Thorac. Surg. 2021, 111, 1770–1780. [Google Scholar] [CrossRef] [PubMed]
- Marijon, E.; Mocumbi, A.; Narayanan, K.; Jouven, X.; Celermajer, D.S. Persisting burden and challenges of rheumatic heart disease. Eur. Heart J. 2021, 42, 3338–3348. [Google Scholar] [CrossRef] [PubMed]
- Rao, C.; Zhang, H.; Gao, H.; Zhao, Y.; Yuan, X.; Hua, K.; Hu, S.; Zheng, Z. The Chinese Cardiac Surgery Registry: Design and Data Audit. Ann. Thorac. Surg. 2016, 101, 1514–1520. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Brien, S.M.; Feng, L.; He, X.; Xian, Y.; Jacobs, J.P.; Badhwar, V.; Kurlansky, P.A.; Furnary, A.P.; Cleveland, J.C., Jr.; Lobdell, K.W.; et al. The Society of Thoracic Surgeons 2018 Adult Cardiac Surgery Risk Models: Part 2-Statistical Methods and Results. Ann. Thorac. Surg. 2018, 105, 1419–1428. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bellomo, R.; Ronco, C.; Kellum, J.A.; Mehta, R.L.; Palevsky, P. Acute renal failure-Definition, outcome measures, animal models, fluid therapy and information technology needs: The Second International Consensus Conference of the Acute Dialysis Quality Initiative (ADQI) Group. Crit. Care 2004, 8, R204–R212. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iung, B.; Delgado, V.; Rosenhek, R.; Price, S.; Prendergast, B.; Wendler, O.; De Bonis, M.; Tribouilloy, C.; Evangelista, A.; Bogachev-Prokophiev, A.; et al. Contemporary Presentation and Management of Valvular Heart Disease: The EURObservational Research Programme Valvular Heart Disease II Survey. Circulation 2019, 140, 1156–1169. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Wang, Z.; Chen, Z.; Wang, X.; Zhang, L.; Li, S.; Zheng, C.; Kang, Y.; Jiang, L.; Zhu, Z.; et al. Current status and etiology of valvular heart disease in China: A population-based survey. BMC Cardiovasc. Disord. 2021, 21, 339. [Google Scholar] [CrossRef] [PubMed]
- Huang, X.; Dhruva, S.S.; Yuan, X.; Bai, X.; Lu, Y.; Yan, X.; Liu, J.; Li, W.; Hu, D.; Ji, R.; et al. Characteristics, interventions and outcomes of patients with valvular heart disease hospitalised in China: A cross-sectional study. BMJ Open 2021, 11, e052946. [Google Scholar] [CrossRef] [PubMed]
- Liu, F.Z.; Xue, Y.M.; Liao, H.T.; Zhan, X.Z.; Guo, H.M.; Huang, H.L.; Fang, X.H.; Wei, W.; Rao, F.; Deng, H.; et al. Five-year epidemiological survey of valvular heart disease: Changes in morbidity, etiological spectrum and management in a cardiovascular center of Southern China. J. Thorac. Dis. 2014, 6, 1724–1730. [Google Scholar] [PubMed]
- Hu, P.; Liu, X.B.; Liang, J.; Zhu, Q.F.; Pu, C.X.; Tang, M.Y.; Wang, J.A. A hospital-based survey of patients with severe valvular heart disease in China. Int. J. Cardiol. 2017, 231, 244–247. [Google Scholar] [CrossRef] [PubMed]
- DiBardino, D.J.; ElBardissi, A.W.; McClure, R.S.; Razo-Vasquez, O.A.; Kelly, N.E.; Cohn, L.H. Four decades of experience with mitral valve repair: Analysis of differential indications, technical evolution, and long-term outcome. J. Thorac. Cardiovasc. Surg. 2010, 139, 76–83, Discussion-4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Waikittipong, S. Mitral valve repair for rheumatic mitral regurgitation: Mid-term results. Asian Cardiovasc. Thorac. Ann. 2015, 23, 658–664. [Google Scholar] [CrossRef] [PubMed]
- Vervoort, D.; Ouzounian, M.; Yanagawa, B. Mitral valve surgery for rheumatic heart disease: Replace, repair, retrain? Curr. Opin. Cardiol. 2021, 36, 179–185. [Google Scholar] [CrossRef] [PubMed]
- Vervoort, D.; Nguyen, D.H.; Nguyen, T.C. When Culture Dictates Practice: Adoption of Minimally Invasive Mitral Valve Surgery. Innovations 2020, 15, 406–409. [Google Scholar] [CrossRef] [PubMed]
- Carroll, J.D.; Mack, M.J.; Vemulapalli, S.; Herrmann, H.C.; Gleason, T.G.; Hanzel, G.; Deeb, G.M.; Thourani, V.H.; Cohen, D.J.; Desai, N.; et al. STS-ACC TVT Registry of Transcatheter Aortic Valve Replacement. J. Am. Coll. Cardiol. 2020, 76, 2492–2516. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.M.; Xiong, T.Y.; Xu, K.; Fang, Z.F.; Jiang, L.; Jin, J.; He, S.H.; Yang, Y.N.; He, J.J.; Jia, Y.H.; et al. Characteristics and outcomes following transcatheter aortic valve replacement in China: A report from China aortic valve transcatheter replacement registry (CARRY). Chin. Med. J. 2021, 134, 2678–2684. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Procedure | CCSR 2016 | CCSR 2018 | CCSR Change: 2016 to 2018 (%) | STS 2018 | STS 2019 | STS Change: 2018 to 2019 (%) |
|---|---|---|---|---|---|---|
| Overall | 11,850 | 12,044 | 1.6 ↑ | 75,597 | 68,747 | −9.1 ↓ |
| Isolated AVR | 3033 | 3395 | 11.9 ↑ | 25,646 | 20,965 | −18.3 ↓ |
| Isolated MVR | 4042 | 3876 | −4.1 ↓ | 10,823 | 10,748 | −0.7 ↓ |
| MV repair | 1231 | 1429 | 16.1 ↑ | 12,608 | 12,570 | −0.3 ↓ |
| AVR and CABG | 493 | 547 | 11.0 ↑ | 16,100 | 12,246 | −11.5 ↓ |
| MVR and CABG | 486 | 512 | 5.3 ↑ | 3554 | 3441 | −3.2 ↓ |
| MV repair and CABG | 271 | 291 | 7.4 ↑ | 4151 | 4153 | 0.0 |
| AVR and MVR | 2294 | 1994 | −13.1 ↓ | 2715 | 2624 | −3.4 ↓ |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, H.; Gong, J.; Wu, Y.; Zheng, Z.; Hou, J. A Comparative Study on Surgical Treatment of Valvular Heart Disease between High-Volume Cardiac Centers in China and STS Data. J. Cardiovasc. Dev. Dis. 2022, 9, 212. https://0-doi-org.brum.beds.ac.uk/10.3390/jcdd9070212
Lin H, Gong J, Wu Y, Zheng Z, Hou J. A Comparative Study on Surgical Treatment of Valvular Heart Disease between High-Volume Cardiac Centers in China and STS Data. Journal of Cardiovascular Development and Disease. 2022; 9(7):212. https://0-doi-org.brum.beds.ac.uk/10.3390/jcdd9070212
Chicago/Turabian StyleLin, Hongyuan, Jiamiao Gong, Yongjian Wu, Zhe Zheng, and Jianfeng Hou. 2022. "A Comparative Study on Surgical Treatment of Valvular Heart Disease between High-Volume Cardiac Centers in China and STS Data" Journal of Cardiovascular Development and Disease 9, no. 7: 212. https://0-doi-org.brum.beds.ac.uk/10.3390/jcdd9070212