
Altered Heart Rate Turbulence and Variability Parameters Predict 1-Year Mortality in Heart Failure with Preserved Ejection Fraction

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
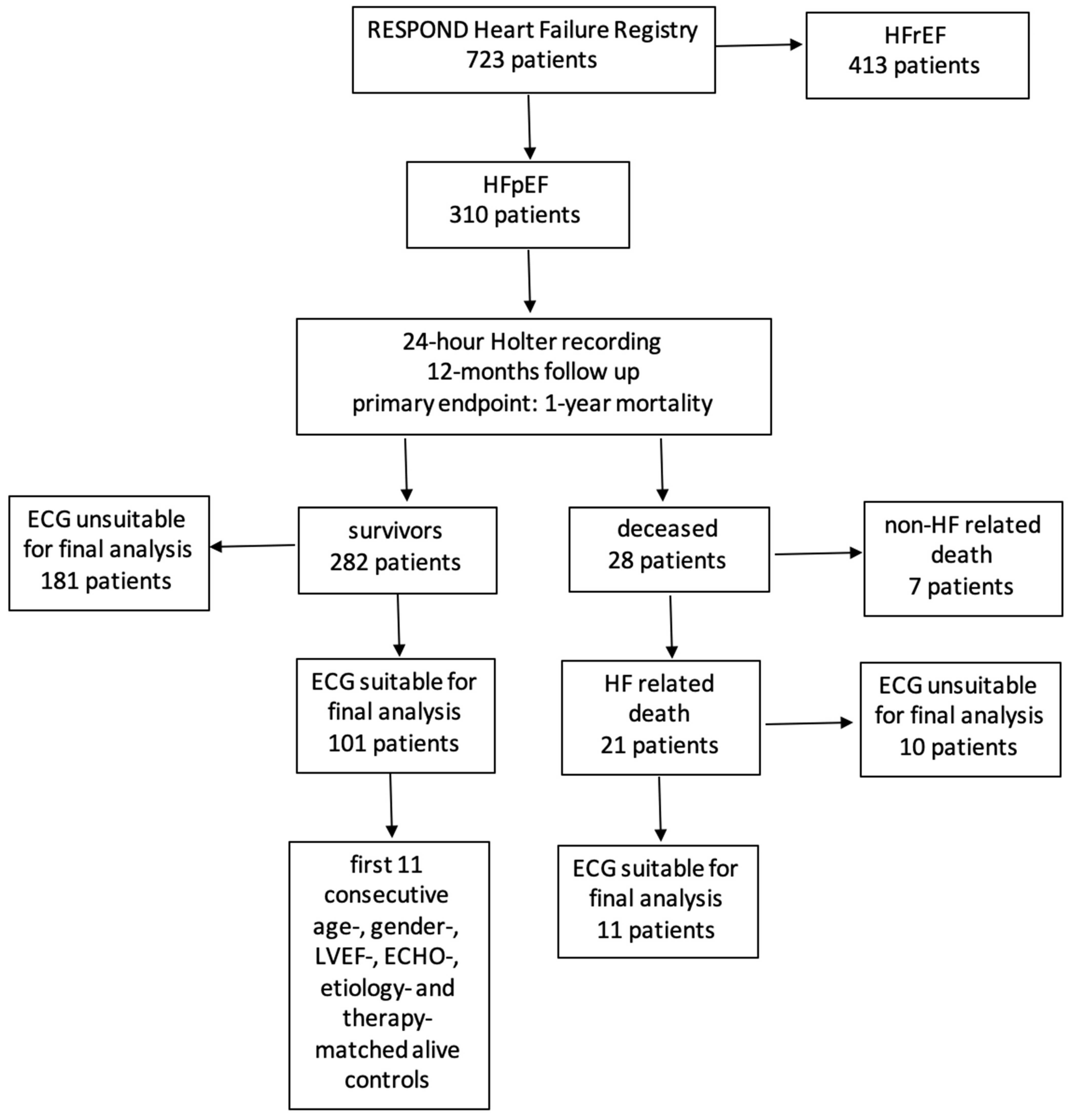
2.1. Patient Population
2.2. Study Design
2.3. HRT Analysis
2.4. HRV Analysis
2.5. Statistical Analysis
3. Results
3.1. Study Population
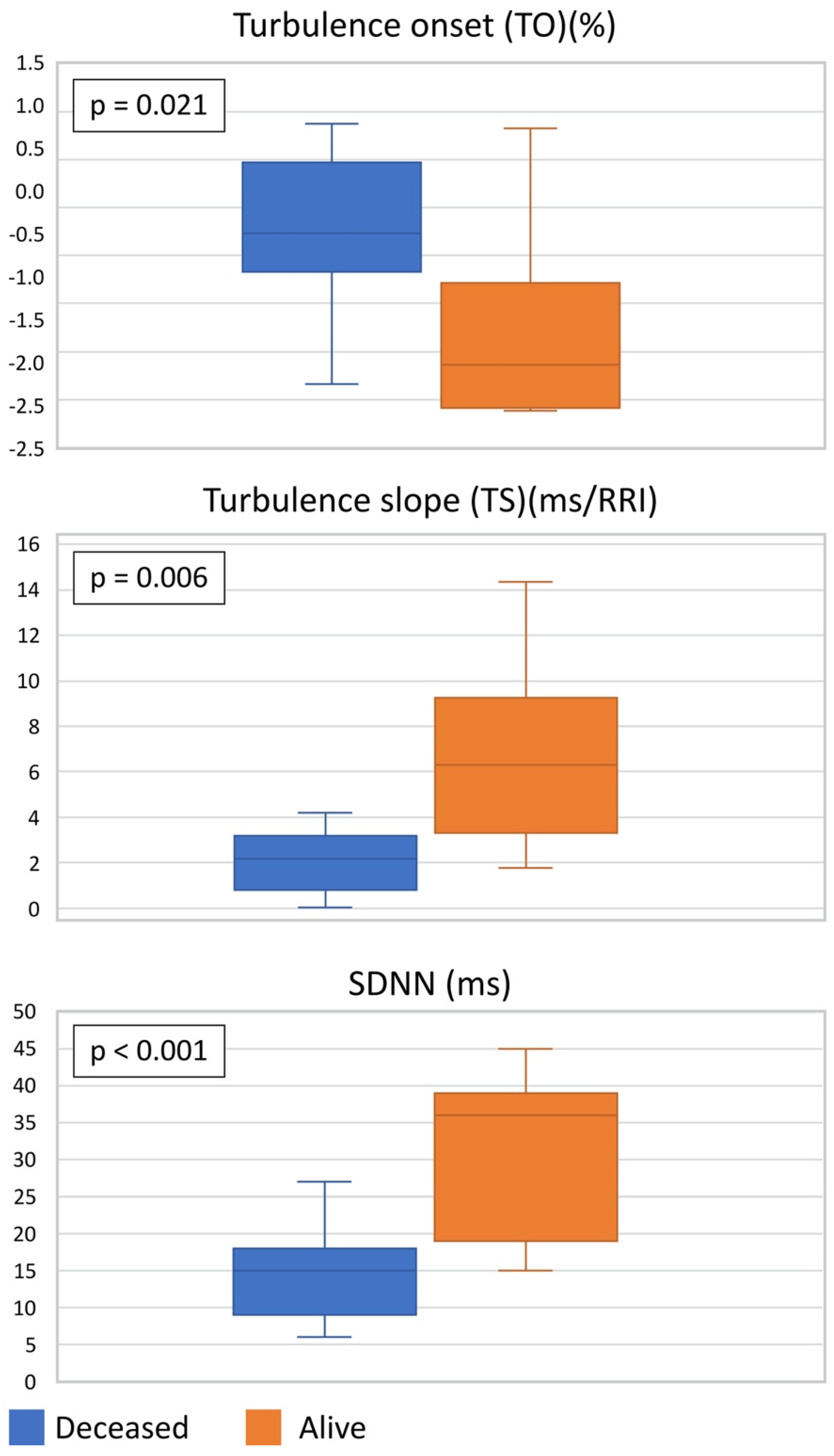
3.2. HRT and HRV Values in Case–Control Population
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Louridas, G.E.; Lourida, K.G. Heart failure in patients with preserved ejection fraction: Questions concerning clinical progression. J. Cardiovasc. Dev. Dis. 2016, 3, 27. [Google Scholar] [CrossRef] [PubMed]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Celutkiene, J.; Chioncel, O.; et al. 2021 ESC guidelines for the diagnosis and treatment of acute and chronic heart failure: Developed by the task force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. Heart J. 2021, 36, 3599–3726. [Google Scholar] [CrossRef]
- Chioncel, O.; Lainscak, M.; Seferovic, P.M.; Anker, S.D.; Crespo-Leiro, M.G.; Harjola, V.P.; Parissis, J.; Laroche, C.; Piepoli, M.F.; Fonseca, C.; et al. Epidemiology and one-year outcomes in patients with chronic heart failure and preserved, mid-range and reduced ejection fraction: An analysis of the ESC Heart Failure Long-Term Registry. Eur. J. Heart Fail. 2017, 19, 1574–1585. [Google Scholar] [CrossRef] [PubMed]
- Anker, S.D.; Butler, J.; Filippatos, G.; Ferreira, J.P.; Bocchi, E.; Böhm, M.; Brunner-La Rocca, H.P.; Choio, D.J.; Chopra, V.; Chuquiure-Valenzuela, E.; et al. Empagliflozin in Heart Failure with a Preserved Ejection Fraction. N. Engl. J. Med. 2021, 385, 1451–1461. [Google Scholar] [CrossRef]
- Liao, L.; Jollis, J.G.; Anstrom, K.J.; Whellan, D.J.; Kitzman, D.W.; Aurigemma, G.P.; Mark, D.B.; Schulman, K.A.; Gottdiener, J.S. Costs for Heart Failure With Normal vs Reduced Ejection Fraction. Arch. Intern. Med. 2006, 166, 112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Savic-Radojevic, A.; Pljesa-Ercegovac, M.; Matic, M.; Simic, D.; Radovanovic, S.; Simic, T. Novel biomarkers of heart failure. Adv. Clin. Chem. 2017, 79, 93–152. [Google Scholar] [CrossRef] [PubMed]
- Borlaug, B.A.; Redfield, M.M.; Melenovsky, V.; Kane, G.C.; Karon, B.L.; Jacobsen, S.J.; Rodeheffer, R.J. Longitudinal changes in left ventricular stiffness: A community-based study. Circ. Heart Fail. 2013, 6, 944–952. [Google Scholar] [CrossRef] [Green Version]
- Ksela, J.; Avbelj, V.; Kalisnik, J.M. Multifractality in heartbeat dynamics in patients undergoing beating-heart myocardial revascularization. Comput. Biol. Med. 2015, 60, 66–73. [Google Scholar] [CrossRef]
- Berezin, E.A.; Berezin, A.A.; Lichtenauer, M. Myokines and heart failure: Challenging role in adverse cardiac remodelling, mypothy, and clinical oputcomes. Dis. Markers 2021, 2021, 6644631. [Google Scholar] [CrossRef]
- Liu, L.; Wu, Q.; Yan, H.; Chen, B.; Zheng, X.; Zhou, Q. Association between Cardiac Autonomic Neuropathy and Coronary Artery Lesions in Patients with Type 2 Diabetes. Dis. Markers 2020, 2020, 6659166. [Google Scholar] [CrossRef]
- Grässler, B.; Thielmann, B.; Böckelmann, I.; Hökelmann, A. Effects of different exercise interventjons on cardiac autonomic control and secondary health factors in middle-aged adults: A systematic review. J. Cardiovasc. Dev. Dis. 2021, 8, 94. [Google Scholar] [CrossRef] [PubMed]
- Cygankiewicz, I. Heart rate turbulence. Prog. Cardiovasc. Dis. 2013, 56, 160–171. [Google Scholar] [CrossRef] [PubMed]
- Pinnacchio, G.; Lanza, G.A.; Stazi, A.; Careri, G.; Coviello, I.; Mollo, R.; Crea, F. Determinants of heart rate turbulence in individuals without apparent heart disease and in patients with stable coronary artery disease. Europace 2015, 17, 1855–1861. [Google Scholar] [CrossRef] [PubMed]
- Marynissen, T.; Flore, V.; Heidbuchel, H.; Nuyens, D.; Ector, J.; Willems, R. Heart rate turbulence predicts ICD-resistant mortality in ischaemic heart disease. Europace 2014, 16, 1069–1077. [Google Scholar] [CrossRef]
- Traxler, D.; Lainscak, M.; Simader, E.; Ankersmit, H.J.; Jug, B. Heat shock protein 27 acts as a predictor of prognosis in chronic heart failure patients. Clin. Chim. Acta 2017, 473, 127–132. [Google Scholar] [CrossRef]
- Kosir, G.; Jug, B.; Novakovic, M.; Bozic Mijovski, M.; Ksela, J. Endocan Is an Independent Predictor of Heart Failure-Related Mortality and Hospitalizations in Patients with Chronic Stable Heart Failure. Dis. Markers 2019, 2019, 9134096. [Google Scholar] [CrossRef] [Green Version]
- Jansen, C.; Al-Kassou, B.; Lehmann, J.; Pohlmann, A.; Chang, J.; Praktiknjo, M.; Nickenig, G.; Strassburg, C.P.; Schrickel, J.W.; Andrie, R.; et al. Severe abnormal Heart Rate Turbulence Onset is associated with deterioration of liver cirrhosis. PLoS ONE 2018, 13, e0195631. [Google Scholar] [CrossRef]
- Özkeçeci, G.; Ünlü, B.S.; Dursun, H.; Akci, Ö.; Köken, G.; Onrat, E.; Avsar, A. Heart rate variability and heart rate turbulence in patients with polycystic ovary syndrome. Anatol. J. Cardiol. 2016, 16, 323–327. [Google Scholar] [CrossRef] [Green Version]
- Yu, Y.; Xu, Y.; Zhang, M.; Wang, Y.; Zou, W.; Gu, Y. Value of Assessing Autonomic Nervous Function by Heart Rate Variability and Heart Rate Turbulence in Hypertensive Patients. Int. J. Hypertens. 2018, 2018, 4067601. [Google Scholar] [CrossRef]
- Schmidt, G.; Malik, M.; Barthel, P.; Schneider, R.; Ulm, K.; Rolnitzky, L.; Camm, A.J.; Bigger, J.T.; Schömig, A. Heart-rate turbulence after ventricular premature beats as a predictor of mortality after acute myocardial infarction. Lancet 1999, 353, 1390–1396. [Google Scholar] [CrossRef] [Green Version]
- Bauer, A.; Malik, M.; Barthel, P.; Schneider, R.; Watanabe, M.A.; Camm, A.J.; Schömig, A.; Schmidt, G. Turbulence dynamics: An independent predictor of late mortality after acute myocardial infarction. Int. J. Cardiol. 2006, 107, 42–47. [Google Scholar] [CrossRef] [PubMed]
- Grimm, W.; Sharkova, J.; Christ, M.; Schneider, R.; Schmidt, G.; Maisch, B. Heart Rate Turbulence following Ventricular Premature Beats in Healthy Controls. Ann. Noninvasive Electrocardiol. 2003, 8, 127–131. [Google Scholar] [CrossRef] [PubMed]
- D’Addio, G.; Cesarelli, M.; Corbi, G.; Romano, M.; Furgi, G.; Ferrara, N.; Rengo, F. Reproducibility of heart rate turbulence indexes in heart failure patients. Annu. Int. Conf. IEEE Eng. Med. Biol. Soc. 2010, 2010, 2573–2576. [Google Scholar] [CrossRef] [PubMed]
- Blesius, V.; Schölzel, C.; Ernst, G.; Dominik, A. HRT assessment reviewed: A systematic review of heart rate turbulence methodology. Physiol. Meas. 2020, 41, 08TR01. [Google Scholar] [CrossRef]
- Heart rate variability: Standards of measurement, physiological interpretation and clinical use. Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology. Circulation 1996, 93, 1043–1065. [CrossRef] [Green Version]
- Cygankiewicz, I.; Zareba, W. Heart rate variability. Handb. Clin. Neurol. 2013, 117, 379–393. [Google Scholar] [CrossRef]
- Xhyheri, B.; Manfrini, O.; Mazzolini, M.; Pizzi, C.; Bugiardini, R. Heart rate variability today. Prog. Cardiovasc. Dis. 2012, 55, 321–331. [Google Scholar] [CrossRef]
- Nolan, J.; Batin, P.D.; Andrews, R.; Lindsay, S.J.; Brooksby, P.; Mullen, M.; Baig, W.; Flapan, A.D.; Cowley, A.; Prescott, R.J.; et al. Prospective study of heart rate variability and mortality in chronic heart failure: Results of the United Kingdom heart failure evaluation and assessment of risk trial (UK-heart). Circulation 1998, 98, 1510–1516. [Google Scholar] [CrossRef] [Green Version]
- Hernando, D.; Roca, S.; Sancho, J.; Alesanco, A.; Bailon, R. Validation of the Apple Watch for Heart Rate Variability Measurements during Relax and Mental Stress in Healthy Subjects. Sensors 2018, 18, 2619. [Google Scholar] [CrossRef] [Green Version]
- Solomon, S.D.; McMurray, J.J.V.; Anand, I.S.; Ge, J.; Lam, C.S.P.; Maggioni, A.P.; Martinez, F.; Packer, M.; Pfeffer, M.A.; Pieske, B.; et al. Angiotensin-Neprilysin Inhibition in Heart Failure with Preserved Ejection Fraction. N. Engl. J. Med. 2019, 381, 1609–1620. [Google Scholar] [CrossRef] [Green Version]
- Silverman, D.N.; Plante, T.B.; Infeld, M.; Callas, P.W.; Juraschek, S.P.; Dougherty, G.B.; Meyer, M. Association of β-Blocker Use With Heart Failure Hospitalizations and Cardiovascular Disease Mortality Among Patients With Heart Failure With a Preserved Ejection Fraction: A Secondary Analysis of the TOPCAT Trial. JAMA Netw. Open 2019, 2, e1916598. [Google Scholar] [CrossRef] [PubMed]
- Gorre, F.; Vandekerckhove, H. Beta-blockers: Focus on mechanism of action. Which beta-blocker, when and why? Acta Cardiol. 2010, 65, 565–570. [Google Scholar] [CrossRef] [PubMed]
- Crespo-Leiro, M.G.; Anker, S.D.; Maggioni, A.P.; Coats, A.J.; Filippatos, G.; Ruschitzka, F.; Ferrari, R.; Piepoli, M.F.; Delgado Jimenez, J.F.; Metra, M.; et al. European Society of Cardiology Heart Failure Long-Term Registry (ESC-HF-LT): 1-year follow-up outcomes and differences across regions. Eur. J. Heart Fail. 2016, 18, 613–625. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Badreldin, H.A.; Aldosari, N.; Alnashwan, L.; Almutairi, T.; Yousif, N.; Alsulaiman, K.; Aljuhani, O.; Hafiz, A.; Alshaya, O. What the near future holds for sacubitril/valsartan: A summary of major ongoing studies. J. Cardiovasc. Dev. Dis. 2022, 9, 54. [Google Scholar] [CrossRef]
- Harper, A.R.; Patel, H.C.; Lyon, A.R. Heart failure with preserved ejection fraction. Clin. Med. 2018, 18 (Suppl. S2), s24–s29. [Google Scholar] [CrossRef]
- Meta-analysis Global Group in Chronic Heart Failure (MAGGIC). The survival of patients with heart failure with preserved or reduced left ventricular ejection fraction: An individual patient data meta-analysis. Eur. Heart J. 2012, 33, 1750–1757. [Google Scholar] [CrossRef] [Green Version]
- Nandini, N. Epidemiology and pathogenesis of heart failure with preserved ejection fraction. Rev. Cardiovasc. Med. 2020, 21, 531–540. [Google Scholar] [CrossRef]
- Toschi-Dias, E.; Rondon, M.U.P.B.; Cogliati, C.; Paolocci, N.; Tobaldini, E.; Montano, N. Contribution of Autonomic Reflexes to the Hyperadrenergic State in Heart Failure. Front. Neurosci. 2017, 11, 162. [Google Scholar] [CrossRef]
- Florea, V.G.; Cohn, J.N. The Autonomic Nervous System and Heart Failure. Circ. Res. 2014, 114, 1815–1826. [Google Scholar] [CrossRef] [Green Version]
- Filgueiras-Rama, D. Sympathetic Innervation and Cardiac Arrhythmias. In Cardiac Electrophysiology: From Cell to Bedside, 7th ed.; Zipes, D.P., Jalife, J., Stevenson, W.G., Eds.; Elsevier: Amsterdam, The Netherlands, 2018; pp. 387–395. [Google Scholar] [CrossRef]
- Barthel, P.; Schneider, R.; Bauer, A.; Ulm, K.; Schmitt, C.; Schömig, A.; Schmidt, G. Risk stratification after acute myocardial infarction by heart rate turbulence. Circulation 2003, 108, 1221–1226. [Google Scholar] [CrossRef] [Green Version]
- Makikallio, T.H.; Barthel, P.; Schneider, R.; Bauer, A.; Tapanainen, J.M.; Tulppo, M.P.; Schmidt, G.; Huikuri, H.V. Prediction of sudden cardiac death after acute myocardial infarction: Role of Holter monitoring in the modern treatment era. Eur. Heart J. 2005, 26, 762–769. [Google Scholar] [CrossRef] [PubMed]
- Bauer, A.; Barthel, P.; Schneider, R.; Ulm, K.; Müller, A.; Joeining, A.; Stich, R.; Kiviniemi, A.; Hnatkova, K.; Huikuri, H.; et al. Improved Stratification of Autonomic Regulation for risk prediction in post-infarction patients with preserved left ventricular function (ISAR-Risk). Eur. Heart J. 2009, 30, 576–583. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bauer, A.; Barthel, P.; Müller, A.; Ulm, K.; Huikuri, H.; Malik, M.; Schmidt, G. Risk prediction by heart rate turbulence and deceleration capacity in postinfarction patients with preserved left ventricular function retrospective analysis of 4 independent trials. J. Electrocardiol. 2009, 42, 597–601. [Google Scholar] [CrossRef] [PubMed]
- Cygankiewicz, I.; Zareba, W.; Vazquez, R.; Bayes-Genis, A.; Pascual, D.; Macaya, C.; Almendral, J.; Fiol, M.; Bardaji, A.; Gonzalez-Juanatey, J.R.; et al. Risk stratification of mortality in patients with heart failure and left ventricular ejection fraction >35%. Am. J. Cardiol. 2009, 103, 1003–1010. [Google Scholar] [CrossRef]
- La Rovere, M.T.; Pinna, G.D.; Maestri, R.; Barlera, S.; Bernardinangeli, M.; Veniani, M.; Nicolosi, G.L.; Marchioli, R.; Tavazzi, L. Autonomic markers and cardiovascular and arrhythmic events in heart failure patients: Still a place in prognostication? Data from the GISSI-HF trial. Eur. J. Heart Fail. 2012, 14, 1410–1419. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristic | All Patients (n = 22) | Deceased (n = 11) | Alive Controls (n = 11) | p-Value |
|---|---|---|---|---|
| Age (years) | 80 ± 7 | 80 ± 6 | 80 ± 7 | 0.872 |
| Gender, female (%) | 4 (18) | 2 (18) | 2 (18) | 1.000 |
| NYHA class ≥ III (%) | 6 (27) | 3 (27) | 3 (27) | 1.000 |
| Therapy | ||||
| ACEi/ARB (%) | 16 (73) | 8 (73) | 8 (73) | 1.000 |
| Spironolactone (%) | 5 (23) | 3 (27) | 2 (18) | 0.611 |
| Diuretics (%) | 7 (32) | 3 (27) | 4 (36) | 0.647 |
| Beta-blockers (%) | 12 (55) | 6 (55) | 6 (55) | 1.000 |
| LVEF | ||||
| Mean | 63 ± 6 | 63 ± 2 | 64 ± 1 | 0.735 |
| 50–60% (%) | 11 (50) | 6 (55) | 5 (45) | 0.669 |
| 60–70% (%) | 6 (27) | 3 (27) | 3 (27) | 1.000 |
| >70% (%) | 5 (23) | 2 (18) | 3 (27) | 0.611 |
| HF Aetiology | ||||
| ischemic (%) | 10 (45) | 5 (45) | 5 (45) | 0.669 |
| non-ischemic (%) | 12 (55) | 6 (55) | 6 (55) | 0.669 |
| Diastolic Dysfunction | ||||
| Grade I (%) | 12 (55) | 6 (55) | 6 (55) | 1.000 |
| Grade II (%) | 8 (36) | 4 (36) | 4 (36) | 1.000 |
| Grade III (%) | 2 (9) | 1 (9) | 1 (9) | 1.000 |
| LV Hypertrophy | 15 (68) | 8 (72) | 7 (64) | 0.476 |
| LA Enlargement | 13 (59) | 7 (64) | 6 (55) | 0.603 |
| E/A Ratio | 0.8 ± 0.2 | 0.7 ± 0.3 | 0.8 ± 0.1 | 0.729 |
| E/e’ Ratio | 10 ± 4 | 10 ± 0.2 | 9 ± 3 | 0.579 |
| TR Vmax | 2.7 ± 0.6 | 2.6 ± 0.7 | 2.8 ± 0.4 | 0.638 |
| Heart Rate (beats/minute) | 79.6 ± 5.3 | 79.4 ± 4.9 | 80.1 ± 5.8 | 0.454 |
| Deceased (n = 11) | Alive Controls (n = 11) | p-Value | |
|---|---|---|---|
| Number of PVCs (median, IQR) | 17 [13–19] | 14 [11–19] | n/a |
| TO (%) (median, IQR) | −0.27 [−0.54–0.34] | −1.64 [−1.99–−1.01] | 0.021 |
| TS (ms/RRI) | 2.17 [0.80–3.08] | 6.29 [4.20–8.02] | 0.006 |
| SDNN (ms) | 14.73 ± 6.97 | 30.55 ± 11.15 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ksela, J.; Rupert, L.; Djordjevic, A.; Antonic, M.; Avbelj, V.; Jug, B. Altered Heart Rate Turbulence and Variability Parameters Predict 1-Year Mortality in Heart Failure with Preserved Ejection Fraction. J. Cardiovasc. Dev. Dis. 2022, 9, 213. https://0-doi-org.brum.beds.ac.uk/10.3390/jcdd9070213
Ksela J, Rupert L, Djordjevic A, Antonic M, Avbelj V, Jug B. Altered Heart Rate Turbulence and Variability Parameters Predict 1-Year Mortality in Heart Failure with Preserved Ejection Fraction. Journal of Cardiovascular Development and Disease. 2022; 9(7):213. https://0-doi-org.brum.beds.ac.uk/10.3390/jcdd9070213
Chicago/Turabian StyleKsela, Jus, Lea Rupert, Anze Djordjevic, Miha Antonic, Viktor Avbelj, and Borut Jug. 2022. "Altered Heart Rate Turbulence and Variability Parameters Predict 1-Year Mortality in Heart Failure with Preserved Ejection Fraction" Journal of Cardiovascular Development and Disease 9, no. 7: 213. https://0-doi-org.brum.beds.ac.uk/10.3390/jcdd9070213