
Central Nervous System Mold Infections in Children with Hematological Malignancies: Advances in Diagnosis and Treatment

 , and
, and 
Abstract
:1. Introduction
2. Epidemiology and Risk Groups
3. Pathogenesis
4. Clinical Presentation
5. Diagnostic Imaging
5.1. Fungal Sinus Disease
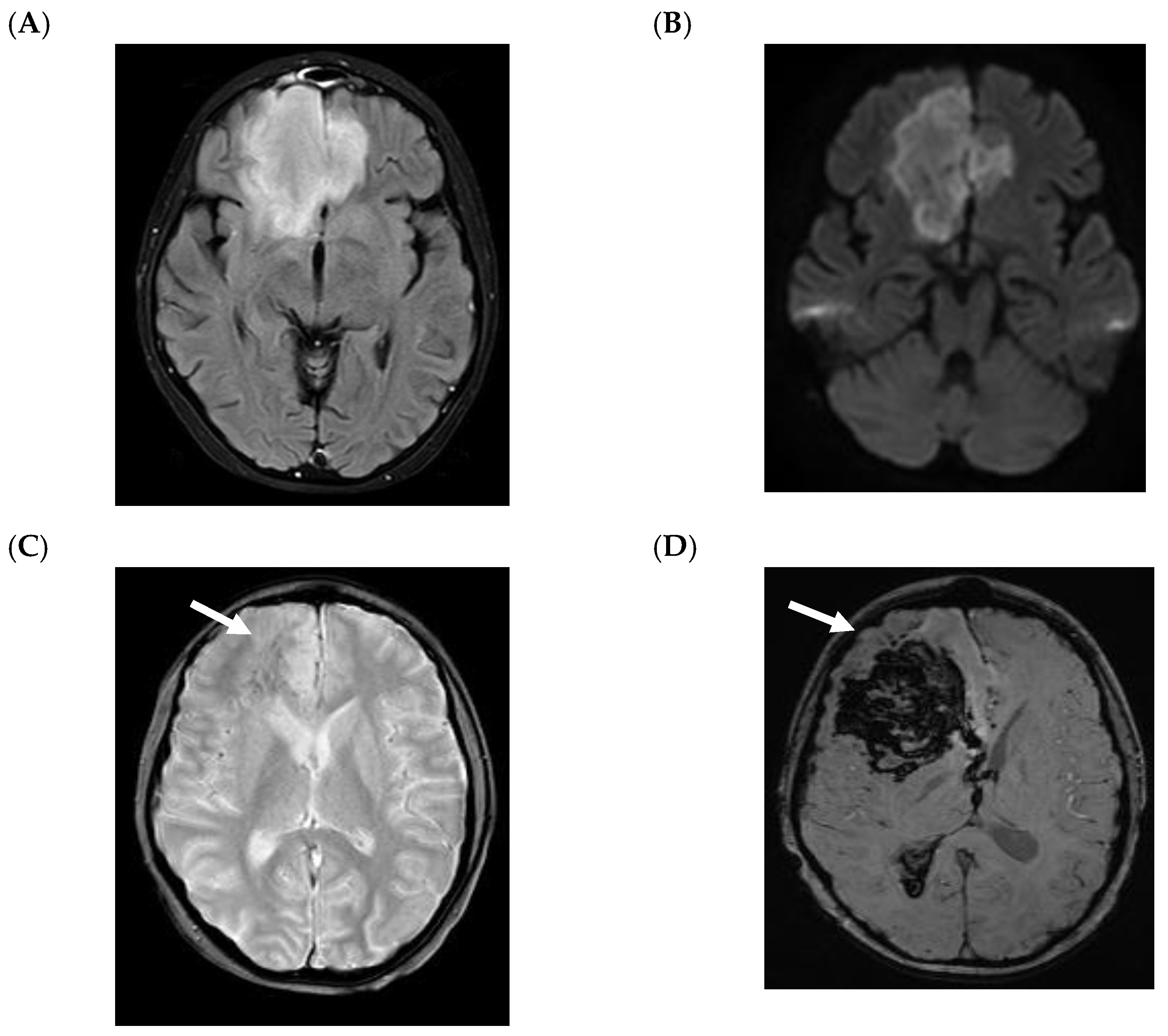
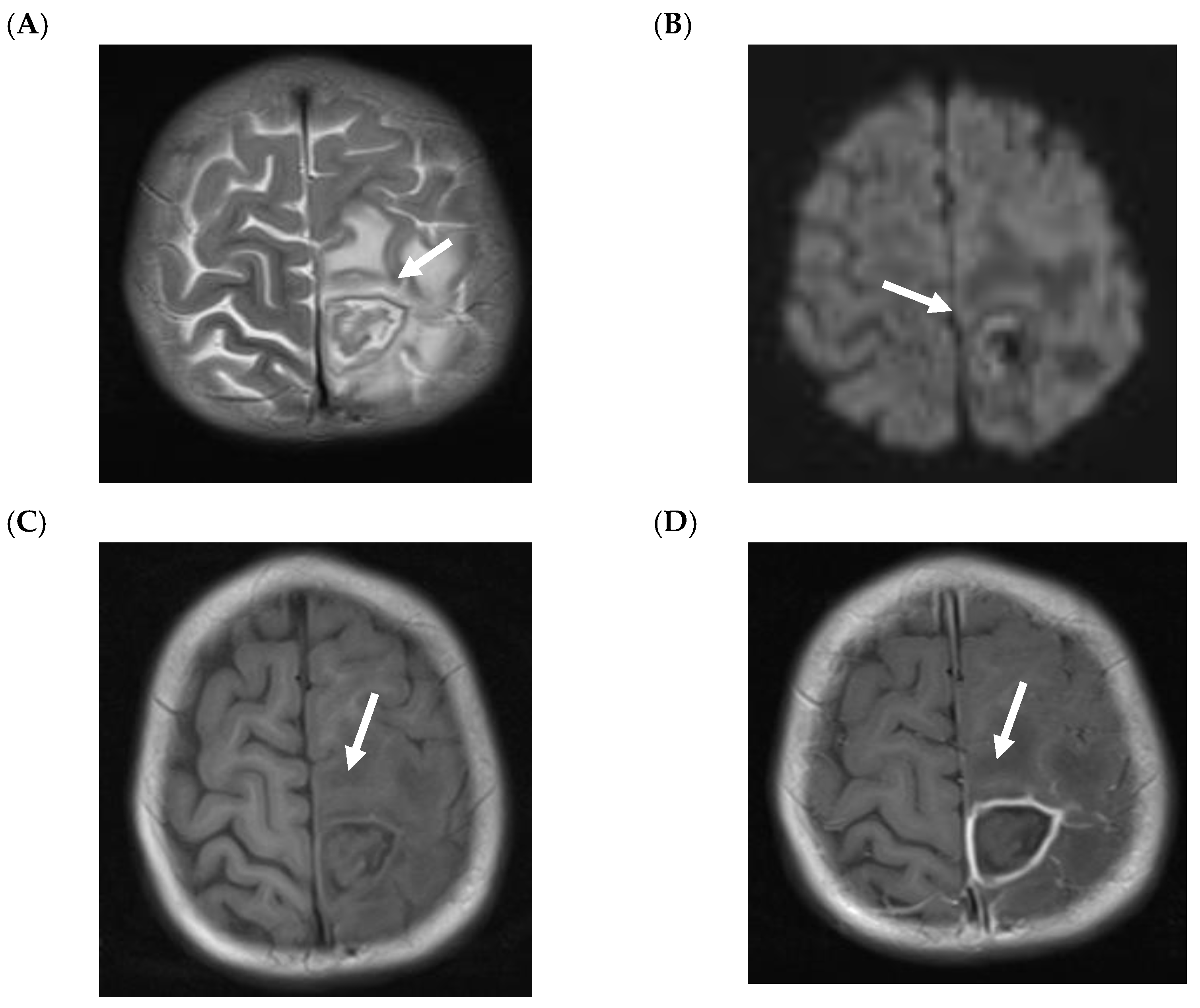
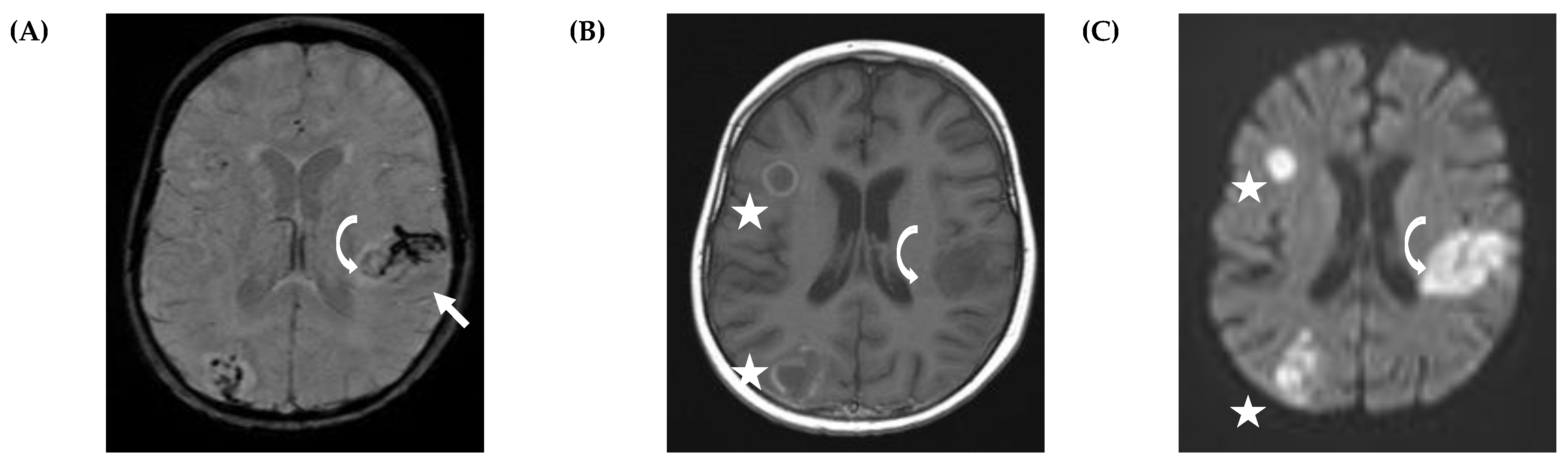
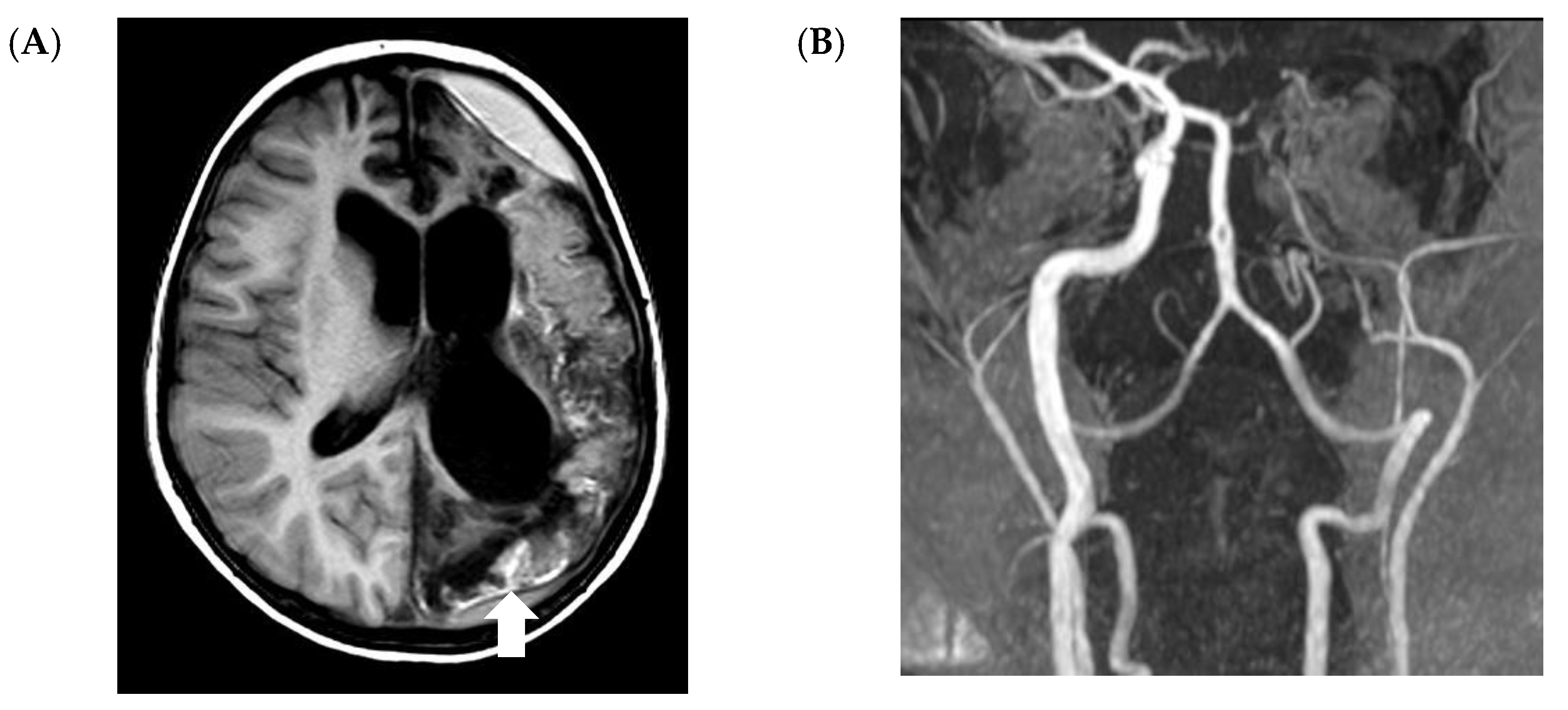
5.2. CNS Manifestations
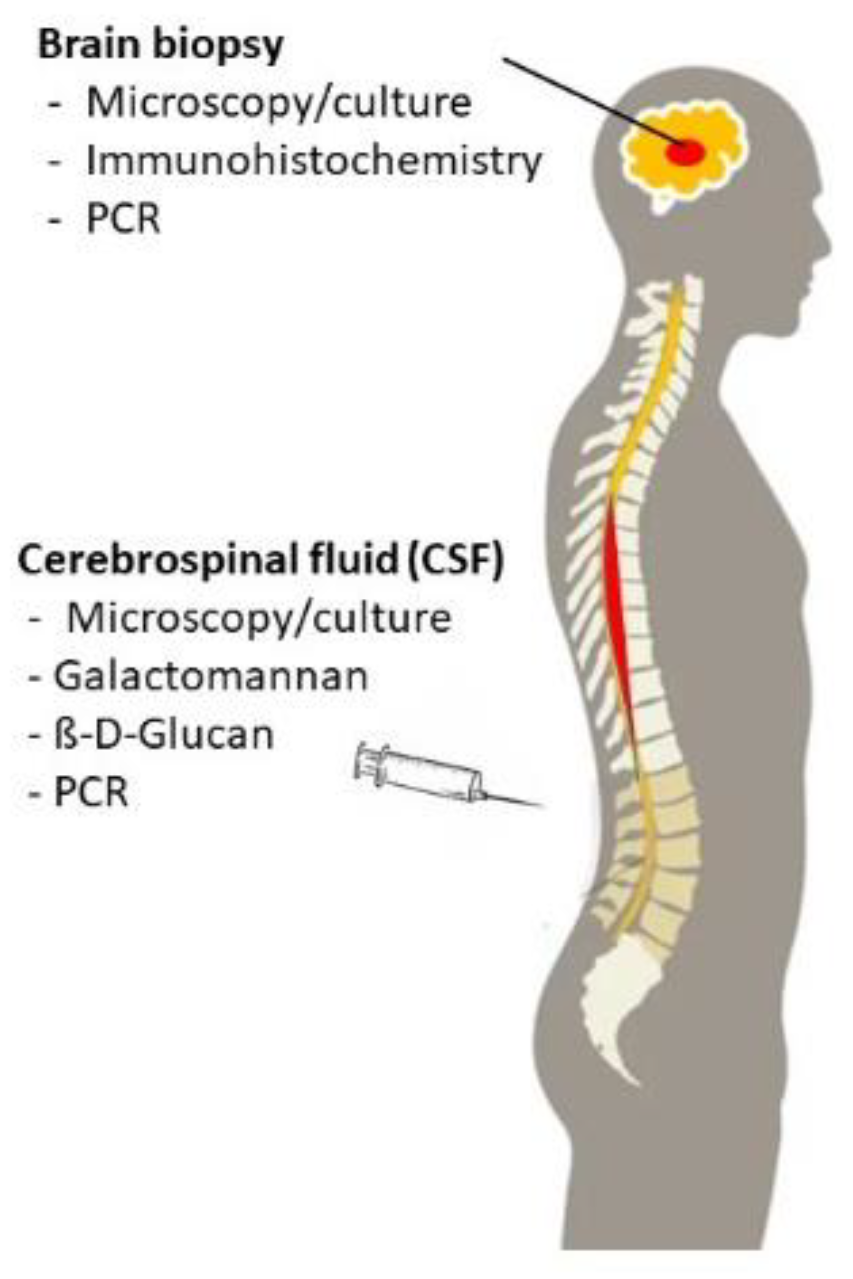
6. Microbiological Evaluation
6.1. Microscopy
6.2. Culturing Techniques
6.3. Non-Culture-Based Assays
6.4. Galactomannan
6.5. Beta-D-Glucan
6.6. Molecular Test Methods
6.7. MALDI-TOF Mass Spectrometry
7. Therapy and Outcome
8. Conclusions and Perspectives
Author Contributions
Funding
Conflicts of Interest
References
- Groll, A.H.; Shah, P.M.; Mentzel, C.; Schneider, M.; Just-Nuebling, G.; Huebner, K. Trends in the postmortem epidemiology of invasive fungal infections at a university hospital. J. Infect. 1996, 33, 23–32. [Google Scholar] [CrossRef]
- Lehrnbecher, T.; Frank, C.; Engels, K.; Kriener, S.; Groll, A.H.; Schwabe, D. Trends in the postmortem epidemiology of invasive fungal infections at a university hospital. J. Infect. 2010, 61, 259–265. [Google Scholar] [CrossRef]
- Dignani, M.C. Epidemiology of invasive fungal diseases on the basis of autopsy reports. F1000Prime Rep. 2014, 6, 81. [Google Scholar] [CrossRef]
- Zaoutis, T.E.; Heydon, K.; Chu, J.H.; Walsh, T.J.; Steinbach, W.J. Epidemiology, outcomes, and costs of invasive aspergillosis in immunocompromised children in the United States, 2000. Pediatrics 2006, 117, e711–e716. [Google Scholar] [CrossRef] [PubMed]
- Cesaro, S.; Tridello, G.; Castagnola, E.; Calore, E.; Carraro, F.; Mariotti, I.; Colombini, A.; Perruccio, K.; Decembrino, N.; Russo, G.; et al. Retrospective study on the incidence and outcome of proven and probable invasive fungal infections in high-risk pediatric onco-hematological patients. Eur. J. Haematol. 2017, 99, 240–248. [Google Scholar] [CrossRef] [PubMed]
- Lehrnbecher, T.; Schoning, S.; Poyer, F.; Georg, J.; Becker, A.; Gordon, K.; Attarbaschi, A.; Groll, A.H. Incidence and Outcome of Invasive Fungal Diseases in Children With Hematological Malignancies and/or Allogeneic Hematopoietic Stem Cell Transplantation: Results of a Prospective Multicenter Study. Front. Microbiol. 2019, 10, 681. [Google Scholar] [CrossRef] [PubMed]
- Fisher, B.T.; Robinson, P.D.; Lehrnbecher, T.; Steinbach, W.J.; Zaoutis, T.E.; Phillips, B.; Sung, L. Risk Factors for Invasive Fungal Disease in Pediatric Cancer and Hematopoietic Stem Cell Transplantation: A Systematic Review. J. Pediatric Infect. Dis. Soc. 2018, 7, 191–198. [Google Scholar] [CrossRef] [PubMed]
- Prakash, H.; Chakrabarti, A. Global Epidemiology of Mucormycosis. J. Fungi 2019, 5, 26. [Google Scholar] [CrossRef] [Green Version]
- Schwartz, S.; Kontoyiannis, D.P.; Harrison, T.; Ruhnke, M. Advances in the diagnosis and treatment of fungal infections of the CNS. Lancet Neurol. 2018, 17, 362–372. [Google Scholar] [CrossRef]
- Montagna, M.T.; Lovero, G.; Coretti, C.; Martinelli, D.; Delia, M.; De Giglio, O.; Caira, M.; Puntillo, F.; D’Antonio, D.; Venditti, M.; et al. SIMIFF study: Italian fungal registry of mold infections in hematological and non-hematological patients. Infection 2014, 42, 141–151. [Google Scholar] [CrossRef]
- Elitzur, S.; Arad-Cohen, N.; Barg, A.; Litichever, N.; Bielorai, B.; Elhasid, R.; Fischer, S.; Fruchtman, Y.; Gilad, G.; Kapelushnik, J.; et al. Mucormycosis in children with haematological malignancies is a salvageable disease: A report from the Israeli Study Group of Childhood Leukemia. Br. J. Haematol. 2020, 189, 339–350. [Google Scholar] [CrossRef]
- Candoni, A.; Facchin, G.; Busca, A.; Lazzarotto, D.; Cattaneo, C.; Nadali, G.; Klimko, N.; Del Principe, M.I.; Castagnola, C.; Verga, L.; et al. Central nervous system fungal infections in allogeneic stem cell transplantation. Outcome of 24 recent cases and literature review. Eur. J. Haematol. 2020, 104, 148–150. [Google Scholar] [CrossRef]
- McCarthy, M.; Rosengart, A.; Schuetz, A.N.; Kontoyiannis, D.P.; Walsh, T.J. Mold infections of the central nervous system. N. Engl. J. Med. 2014, 371, 150–160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miceli, M.H. Central Nervous System Infections Due to Aspergillus and Other Hyaline Molds. J. Fungi 2019, 5, 79. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shi, M.; Mody, C.H. Fungal Infection in the Brain: What We Learned from Intravital Imaging. Front. Immunol. 2016, 7, 292. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patel, R.; Hossain, M.A.; German, N.; Al-Ahmad, A.J. Gliotoxin penetrates and impairs the integrity of the human blood-brain barrier in vitro. Mycotoxin Res. 2018, 34, 257–268. [Google Scholar] [CrossRef]
- Santiago-Tirado, F.H.; Onken, M.D.; Cooper, J.A.; Klein, R.S.; Doering, T.L. Trojan Horse Transit Contributes to Blood-Brain Barrier Crossing of a Eukaryotic Pathogen. mBio 2017, 8, e02183-16. [Google Scholar] [CrossRef] [Green Version]
- Koutsouras, G.W.; Ramos, R.L.; Martinez, L.R. Role of microglia in fungal infections of the central nervous system. Virulence 2017, 8, 705–718. [Google Scholar] [CrossRef] [Green Version]
- Lewis, R.E.; Wiederhold, N.P.; Chi, J.; Han, X.Y.; Komanduri, K.V.; Kontoyiannis, D.P.; Prince, R.A. Detection of gliotoxin in experimental and human aspergillosis. Infect. Immun. 2005, 73, 635–637. [Google Scholar] [CrossRef] [Green Version]
- Goralska, K.; Blaszkowska, J.; Dzikowiec, M. Neuroinfections caused by fungi. Infection 2018, 46, 443–459. [Google Scholar] [CrossRef] [Green Version]
- Hassler, A.; Porto, L.; Lehrnbecher, T. Cerebral Fungal Infection in Pediatric Cancer Patients. Curr. Fungal Infect. Rep. 2015, 9, 6–14. [Google Scholar] [CrossRef]
- Lauten, M.; Attarbaschi, A.; Cario, G.; Doring, M.; Moser, O.; Mucke, U.; Poyer, F.; Rieken, S.; Temme, C.; Voigt, S.; et al. Invasive mold disease of the central nervous system in children and adolescents with cancer or undergoing hematopoietic stem cell transplantation: Analysis of 29 contemporary patients. Pediatric Blood Cancer 2019, 66, e27806. [Google Scholar] [CrossRef] [PubMed]
- Groll, A.H.; Pana, D.; Lanternier, F.; Mesini, A.; Ammann, R.A.; Averbuch, B.; Castagnola, E.; Cesaro, S.; Engelhard, D.; Garcia-Vidal, C.; et al. Eighth European Conference on Infections in Leukaemia (ECIL-8): 2020 Updated Guidelines for Diagnosis, Prevention and Treatment of Invasive Fungal Diseases in Paediatric Patients with Cancer or Allogeneic Haematopoietic Cell Transplantation. Lancet Oncol. 2021, in press. [Google Scholar]
- Porto, L.; You, S.J.; Attarbaschi, A.; Cario, G.; Doring, M.; Moser, O.; Mucke, U.; Poyer, F.; Temme, C.; Voigt, S.; et al. Invasive Mold Infection of the Central Nervous System in Immunocompromised Children. J. Fungi 2020, 6, 226. [Google Scholar] [CrossRef] [PubMed]
- Nickerson, J.P.; Richner, B.; Santy, K.; Lequin, M.H.; Poretti, A.; Filippi, C.G.; Huisman, T.A. Neuroimaging of pediatric intracranial infection--part 2: TORCH, viral, fungal, and parasitic infections. J. Neuroimaging 2012, 22, e52–e63. [Google Scholar] [CrossRef] [PubMed]
- Gavito-Higuera, J.; Mullins, C.B.; Ramos-Duran, L.; Olivas Chacon, C.I.; Hakim, N.; Palacios, E. Fungal Infections of the Central Nervous System: A Pictorial Review. J. Clin. Imaging Sci. 2016, 6, 24. [Google Scholar] [CrossRef]
- Ashdown, B.C.; Tien, R.D.; Felsberg, G.J. Aspergillosis of the brain and paranasal sinuses in immunocompromised patients: CT and MR imaging findings. AJR Am. J. Roentgenol. 1994, 162, 155–159. [Google Scholar] [CrossRef]
- Aribandi, M.; McCoy, V.A.; Bazan, C., 3rd. Imaging features of invasive and noninvasive fungal sinusitis: A review. Radiographics 2007, 27, 1283–1296. [Google Scholar] [CrossRef]
- Middlebrooks, E.H.; Frost, C.J.; De Jesus, R.O.; Massini, T.C.; Schmalfuss, I.M.; Mancuso, A.A. Acute Invasive Fungal Rhinosinusitis: A Comprehensive Update of CT Findings and Design of an Effective Diagnostic Imaging Model. AJNR Am. J. Neuroradiol. 2015, 36, 1529–1535. [Google Scholar] [CrossRef] [Green Version]
- Antulov, R.; Dolic, K.; Fruehwald-Pallamar, J.; Miletic, D.; Thurnher, M.M. Differentiation of pyogenic and fungal brain abscesses with susceptibility-weighted MR sequences. Neuroradiology 2014, 56, 937–945. [Google Scholar] [CrossRef]
- Mathur, M.; Johnson, C.E.; Sze, G. Fungal infections of the central nervous system. Neuroimaging Clin. N. Am. 2012, 22, 609–632. [Google Scholar] [CrossRef]
- Britt, R.H.; Enzmann, D.R.; Placone, R.C., Jr.; Obana, W.G.; Yeager, A.S. Experimental anaerobic brain abscess. Computerized tomographic and neuropathological correlations. J. Neurosurg. 1984, 60, 1148–1159. [Google Scholar] [CrossRef] [PubMed]
- Lehrnbecher, T.; Becker, K.; Groll, A.H. Current Algorithms in Fungal Diagnosis in the Immunocompromised Host. Methods Mol. Biol. 2017, 1508, 67–84. [Google Scholar]
- Hayden, R.T.; Isotalo, P.A.; Parrett, T.; Wolk, D.M.; Qian, X.; Roberts, G.D.; Lloyd, R.V. In situ hybridization for the differentiation of Aspergillus, Fusarium, and Pseudallescheria species in tissue section. Diagn. Mol. Pathol. 2003, 12, 21–26. [Google Scholar] [CrossRef]
- Rickerts, V.; McCormick Smith, I.; Mousset, S.; Kommedal, O.; Fredricks, D.N. Deciphering the aetiology of a mixed fungal infection by broad-range PCR with sequencing and fluorescence in situ hybridisation. Mycoses 2013, 56, 681–686. [Google Scholar] [CrossRef] [PubMed]
- Ruhnke, M.; Bohme, A.; Buchheidt, D.; Cornely, O.; Donhuijsen, K.; Einsele, H.; Enzensberger, R.; Hebart, H.; Heussel, C.P.; Horger, M.; et al. Diagnosis of invasive fungal infections in hematology and oncology—Guidelines from the Infectious Diseases Working Party in Haematology and Oncology of the German Society for Haematology and Oncology (AGIHO). Ann. Oncol. 2012, 23, 823–833. [Google Scholar] [CrossRef] [PubMed]
- Schmalreck, A.F.; Lackner, M.; Becker, K.; Fegeler, W.; Czaika, V.; Ulmer, H.; Lass-Florl, C. Phylogenetic relationships matter: Antifungal susceptibility among clinically relevant yeasts. Antimicrob. Agents Chemother. 2014, 58, 1575–1585. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lamoth, F. Galactomannan and 1,3-beta-d-Glucan Testing for the Diagnosis of Invasive Aspergillosis. J. Fungi 2016, 2, 22. [Google Scholar] [CrossRef] [PubMed]
- Jenks, J.D.; Hoenigl, M. Point-of-care diagnostics for invasive aspergillosis: Nearing the finish line. Expert Rev. Mol. Diagn. 2020, 20, 1009–1017. [Google Scholar] [CrossRef]
- Donnelly, J.P.; Chen, S.C.; Kauffman, C.A.; Steinbach, W.J.; Baddley, J.W.; Verweij, P.E.; Clancy, C.J.; Wingard, J.R.; Lockhart, S.R.; Groll, A.H.; et al. Revision and Update of the Consensus Definitions of Invasive Fungal Disease From the European Organization for Research and Treatment of Cancer and the Mycoses Study Group Education and Research Consortium. Clin. Infect. Dis. 2020, 71, 1367–1376. [Google Scholar] [CrossRef] [Green Version]
- Lehrnbecher, T.; Robinson, P.D.; Fisher, B.T.; Castagnola, E.; Groll, A.H.; Steinbach, W.J.; Zaoutis, T.E.; Negeri, Z.F.; Beyene, J.; Phillips, B.; et al. Galactomannan, beta-D-Glucan, and Polymerase Chain Reaction-Based Assays for the Diagnosis of Invasive Fungal Disease in Pediatric Cancer and Hematopoietic Stem Cell Transplantation: A Systematic Review and Meta-Analysis. Clin. Infect. Dis. 2016, 63, 1340–1348. [Google Scholar] [CrossRef]
- Ullmann, A.J.; Aguado, J.M.; Arikan-Akdagli, S.; Denning, D.W.; Groll, A.H.; Lagrou, K.; Lass-Florl, C.; Lewis, R.E.; Munoz, P.; Verweij, P.E.; et al. Diagnosis and management of Aspergillus diseases: Executive summary of the 2017 ESCMID-ECMM-ERS guideline. Clin. Microbiol. Infect. 2018, 24 (Suppl. 1), e1–e38. [Google Scholar] [CrossRef] [Green Version]
- Calmettes, C.; Gabriel, F.; Blanchard, E.; Servant, V.; Bouchet, S.; Kabore, N.; Forcade, E.; Leroyer, C.; Bidet, A.; Latrabe, V.; et al. Breakthrough invasive aspergillosis and diagnostic accuracy of serum galactomannan enzyme immune assay during acute myeloid leukemia induction chemotherapy with posaconazole prophylaxis. Oncotarget 2018, 9, 26724–26736. [Google Scholar] [CrossRef] [PubMed]
- Kauffman, C.A.; Sexton, D.J.; Bond, S. Diagnosis of Invasive Aspergillosis. Available online: https://www.uptodate.com/contents/diagnosis-of-invasive-aspergillosis (accessed on 20 December 2020).
- Marchetti, O.; Lamoth, F.; Mikulska, M.; Viscoli, C.; Verweij, P.; Bretagne, S.; European Conference on Infections in Leukemia Laboratory Working Group. ECIL recommendations for the use of biological markers for the diagnosis of invasive fungal diseases in leukemic patients and hematopoietic SCT recipients. Bone Marrow Transplant 2012, 47, 846–854. [Google Scholar] [CrossRef] [Green Version]
- Desai, R.; Ross, L.A.; Hoffman, J.A. The role of bronchoalveolar lavage galactomannan in the diagnosis of pediatric invasive aspergillosis. Pediatr. Infect. Dis. J. 2009, 28, 283–286. [Google Scholar] [CrossRef]
- De Mol, M.; de Jongste, J.C.; van Westreenen, M.; Merkus, P.J.; de Vries, A.H.; Hop, W.C.; Warris, A.; Janssens, H.M. Diagnosis of invasive pulmonary aspergillosis in children with bronchoalveolar lavage galactomannan. Pediatric Pulmonol. 2013, 48, 789–796. [Google Scholar] [CrossRef] [PubMed]
- Chong, G.M.; Maertens, J.A.; Lagrou, K.; Driessen, G.J.; Cornelissen, J.J.; Rijnders, B.J. Diagnostic Performance of Galactomannan Antigen Testing in Cerebrospinal Fluid. J. Clin. Microbiol. 2016, 54, 428–431. [Google Scholar] [CrossRef] [Green Version]
- Lehrnbecher, T.; Rath, P.M.; Attarbaschi, A.; Cario, G.; Doring, M.; Moser, O.; Mucke, U.; Poyer, F.; Rieken, S.; Temme, C.; et al. Galactomannan and PCR in the Central Nervous System to Detect Invasive Mold Disease—A Retrospective Analysis in Immunocompromised Children. Sci. Rep. 2019, 9, 12950. [Google Scholar] [CrossRef] [PubMed]
- Linder, K.A.; Kauffman, C.A.; Zhou, S.; Richards, B.J.; Kleiboeker, S.; Miceli, M.H. Performance of the (1,3)-Beta-D-Glucan Assay on Bronchoalveolar Lavage Fluid for the Diagnosis of Invasive Pulmonary Aspergillosis. Mycopathologia 2020, 185, 925–929. [Google Scholar]
- Huppler, A.R.; Fisher, B.T.; Lehrnbecher, T.; Walsh, T.J.; Steinbach, W.J. Role of Molecular Biomarkers in the Diagnosis of Invasive Fungal Diseases in Children. J. Pediatr. Infect. Dis. Soc. 2017, 6, S32–S44. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, P.B.; Benjamin, D.K., Jr.; Alexander, B.D.; Johnson, M.D.; Finkelman, M.A.; Steinbach, W.J. Quantification of 1,3-beta-D-glucan levels in children: Preliminary data for diagnostic use of the beta-glucan assay in a pediatric setting. Clin. Vaccine Immunol. 2007, 14, 924–925. [Google Scholar] [CrossRef] [Green Version]
- Koltze, A.; Rath, P.; Schoning, S.; Steinmann, J.; Wichelhaus, T.A.; Bader, P.; Bochennek, K.; Lehrnbecher, T. Beta-D-Glucan Screening for the Detection of Invasive Fungal Disease in Children Undergoing Allogeneic Hematopoietic Stem Cell Transplantation. J. Clin. Microbiol. 2015, 53, 2605–2610. [Google Scholar] [CrossRef] [Green Version]
- White, S.K.; Schmidt, R.L.; Walker, B.S.; Hanson, K.E. (1→3)-beta-D-glucan testing for the detection of invasive fungal infections in immunocompromised or critically ill people. Cochrane Database Syst. Rev. 2020, 7, CD009833. [Google Scholar]
- Salvatore, C.M.; Chen, T.K.; Toussi, S.S.; DeLaMora, P.; Petraitiene, R.; Finkelman, M.A.; Walsh, T.J. (1→3)-beta-d-Glucan in Cerebrospinal Fluid as a Biomarker for Candida and Aspergillus Infections of the Central Nervous System in Pediatric Patients. J. Pediatric Infect. Dis. Soc. 2016, 5, 277–286. [Google Scholar] [CrossRef] [Green Version]
- Lyons, J.L.; Thakur, K.T.; Lee, R.; Watkins, T.; Pardo, C.A.; Carson, K.A.; Markley, B.; Finkelman, M.A.; Marr, K.A.; Roos, K.L.; et al. Utility of measuring (1,3)-beta-d-glucan in cerebrospinal fluid for diagnosis of fungal central nervous system infection. J. Clin. Microbiol. 2015, 53, 319–322. [Google Scholar] [CrossRef] [Green Version]
- Buchheidt, D.; Reinwald, M.; Spiess, B.; Boch, T.; Hofmann, W.K.; Groll, A.H.; Lehrnbecher, T.; Working Group “Infections in Hematology and Oncology”, German Paul-Ehrlich-Society. Biomarker-based diagnostic work-up of invasive pulmonary aspergillosis in immunocompromised paediatric patients—Is Aspergillus PCR appropriate? Mycoses 2016, 59, 67–74. [Google Scholar] [CrossRef] [PubMed]
- Barnes, R.A.; White, P.L.; Morton, C.O.; Rogers, T.R.; Cruciani, M.; Loeffler, J.; Donnelly, J.P. Diagnosis of aspergillosis by PCR: Clinical considerations and technical tips. Med. Mycol. 2018, 56, 60–72. [Google Scholar] [CrossRef] [PubMed]
- White, P.L.; Wingard, J.R.; Bretagne, S.; Loffler, J.; Patterson, T.F.; Slavin, M.A.; Barnes, R.A.; Pappas, P.G.; Donnelly, J.P. Aspergillus Polymerase Chain Reaction: Systematic Review of Evidence for Clinical Use in Comparison with Antigen Testing. Clin. Infect. Dis. 2015, 61, 1293–1303. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cruciani, M.; White, P.L.; Mengoli, C.; Loffler, J.; Morton, C.O.; Klingspor, L.; Buchheidt, D.; Maertens, J.; Heinz, W.J.; Rogers, T.R.; et al. The impact of anti-mould prophylaxis on Aspergillus PCR blood testing for the diagnosis of invasive aspergillosis. J. Antimicrob. Chemother. 2021, 76, 635–638. [Google Scholar] [CrossRef]
- Loeffler, J.; Hafner, J.; Mengoli, C.; Wirth, C.; Heussel, C.P.; Loffler, C.; White, P.L.; Ullmann, A.J.; Michel, D.; Wiegering, V.; et al. Prospective Biomarker Screening for Diagnosis of Invasive Aspergillosis in High-Risk Pediatric Patients. J. Clin. Microbiol. 2017, 55, 101–109. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heng, S.C.; Chen, S.C.; Morrissey, C.O.; Thursky, K.; Manser, R.L.; De Silva, H.D.; Halliday, C.L.; Seymour, J.F.; Nation, R.L.; Kong, D.C.; et al. Clinical utility of Aspergillus galactomannan and PCR in bronchoalveolar lavage fluid for the diagnosis of invasive pulmonary aspergillosis in patients with haematological malignancies. Diagn. Microbiol. Infect. Dis. 2014, 79, 322–327. [Google Scholar] [CrossRef]
- Hoenigl, M.; Prattes, J.; Spiess, B.; Wagner, J.; Prueller, F.; Raggam, R.B.; Posch, V.; Duettmann, W.; Hoenigl, K.; Wolfler, A.; et al. Performance of galactomannan, beta-d-glucan, Aspergillus lateral-flow device, conventional culture, and PCR tests with bronchoalveolar lavage fluid for diagnosis of invasive pulmonary aspergillosis. J. Clin. Microbiol. 2014, 52, 2039–2045. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- White, P.L.; Parr, C.; Barnes, R.A. Predicting Invasive Aspergillosis in Hematology Patients by Combining Clinical and Genetic Risk Factors with Early Diagnostic Biomarkers. J. Clin. Microbiol. 2018, 56, e01122. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buitrago, M.J.; Bernal-Martinez, L.; Castelli, M.V.; Rodriguez-Tudela, J.L.; Cuenca-Estrella, M. Performance of panfungal—And specific-PCR-based procedures for etiological diagnosis of invasive fungal diseases on tissue biopsy specimens with proven infection: A 7-year retrospective analysis from a reference laboratory. J. Clin. Microbiol. 2014, 52, 1737–1740. [Google Scholar] [CrossRef] [Green Version]
- Moncada, P.A.; Budvytiene, I.; Ho, D.Y.; Deresinski, S.C.; Montoya, J.G.; Banaei, N. Utility of DNA sequencing for direct identification of invasive fungi from fresh and formalin-fixed specimens. Am. J. Clin. Pathol. 2013, 140, 203–208. [Google Scholar] [CrossRef] [Green Version]
- Reinwald, M.; Buchheidt, D.; Hummel, M.; Duerken, M.; Bertz, H.; Schwerdtfeger, R.; Reuter, S.; Kiehl, M.G.; Barreto-Miranda, M.; Hofmann, W.K.; et al. Diagnostic performance of an Aspergillus-specific nested PCR assay in cerebrospinal fluid samples of immunocompromised patients for detection of central nervous system aspergillosis. PLoS ONE 2013, 8, e56706. [Google Scholar] [CrossRef] [PubMed]
- Bader, O. Fungal Species Identification by MALDI-ToF Mass Spectrometry. Methods Mol. Biol. 2017, 1508, 323–337. [Google Scholar]
- Sung, L.; Phillips, R.; Lehrnbecher, T. Time for paediatric febrile neutropenia guidelines—Children are not little adults. Eur. J. Cancer 2011, 47, 811–813. [Google Scholar] [CrossRef] [PubMed]
- Nau, R.; Sorgel, F.; Eiffert, H. Penetration of drugs through the blood-cerebrospinal fluid/blood-brain barrier for treatment of central nervous system infections. Clin. Microbiol. Rev. 2010, 23, 858–883. [Google Scholar] [CrossRef] [Green Version]
- Verweij, P.E.; Te Dorsthorst, D.T.; Janssen, W.H.; Meis, J.F.; Mouton, J.W. In vitro activities at pH 5.0 and pH 7.0 and in vivo efficacy of flucytosine against Aspergillus fumigatus. Antimicrob. Agents Chemother. 2008, 52, 4483–4485. [Google Scholar] [CrossRef] [Green Version]
- Cornely, O.A.; Maertens, J.; Winston, D.J.; Perfect, J.; Ullmann, A.J.; Walsh, T.J.; Helfgott, D.; Holowiecki, J.; Stockelberg, D.; Goh, Y.T.; et al. Posaconazole vs. fluconazole or itraconazole prophylaxis in patients with neutropenia. N. Engl. J. Med. 2007, 356, 348–359. [Google Scholar] [CrossRef] [Green Version]
- Ullmann, A.J.; Lipton, J.H.; Vesole, D.H.; Chandrasekar, P.; Langston, A.; Tarantolo, S.R.; Greinix, H.; Morais de Azevedo, W.; Reddy, V.; Boparai, N.; et al. Posaconazole or fluconazole for prophylaxis in severe graft-versus-host disease. N. Engl. J. Med. 2007, 356, 335–347. [Google Scholar] [CrossRef] [PubMed]
- Arrieta, A.C.; Sung, L.; Bradley, J.S.; Zwaan, C.M.; Gates, D.; Waskin, H.; Carmelitano, P.; Groll, A.H.; Lehrnbecher, T.; Mangin, E.; et al. A non-randomized trial to assess the safety, tolerability, and pharmacokinetics of posaconazole oral suspension in immunocompromised children with neutropenia. PLoS ONE 2019, 14, e0212837. [Google Scholar] [CrossRef] [PubMed]
- Groll, A.H.; Abdel-Azim, H.; Lehrnbecher, T.; Steinbach, W.J.; Paschke, A.; Mangin, E.; Winchell, G.A.; Waskin, H.; Bruno, C.J. Pharmacokinetics and safety of posaconazole intravenous solution and powder for oral suspension in children with neutropenia: An open-label, sequential dose-escalation trial. Int. J. Antimicrob. Agents 2020, 56, 106084. [Google Scholar] [CrossRef]
- Schwartz, S.; Cornely, O.A.; Hamed, K.; Marty, F.M.; Maertens, J.; Rahav, G.; Herbrecht, R.; Heinz, W.J. Isavuconazole for the treatment of patients with invasive fungal diseases involving the central nervous system. Med. Mycol. 2020, 58, 417–424. [Google Scholar] [CrossRef] [Green Version]
- Decembrino, N.; Perruccio, K.; Zecca, M.; Colombini, A.; Calore, E.; Muggeo, P.; Soncini, E.; Comelli, A.; Molinaro, M.; Goffredo, B.M.; et al. A Case Series and Literature Review of Isavuconazole Use in Pediatric Patients with Hemato-oncologic Diseases and Hematopoietic Stem Cell Transplantation. Antimicrob. Agents Chemother. 2020, 64, e01783. [Google Scholar] [CrossRef]
- Tortorano, A.M.; Prigitano, A.; Esposto, M.C.; Arsic Arsenijevic, V.; Kolarovic, J.; Ivanovic, D.; Paripovic, L.; Klingspor, L.; Nordoy, I.; Hamal, P.; et al. European Confederation of Medical Mycology (ECMM) epidemiological survey on invasive infections due to Fusarium species in Europe. Eur. J. Clin. Microbiol. Infect. Dis. 2014, 33, 1623–1630. [Google Scholar] [CrossRef]
- Jensen, T.S.R.; Arendrup, M.C.; von Buchvald, C.; Frandsen, T.L.; Juhler, M.; Nygaard, U. Successful Treatment of Rhino-Orbital-Cerebral Mucormycosis in a Child with Leukemia. J. Pediatric Hematol. Oncol. 2017, 39, e211–e215. [Google Scholar] [CrossRef] [PubMed]
- Dworsky, Z.D.; Bradley, J.S.; Brigger, M.T.; Pong, A.L.; Kuo, D.J. Multimodal Treatment of Rhinocerebral Mucormycosis in a Pediatric Patient with Relapsed Pre-B Acute Lymphoblastic Leukemia. Pediatric Infect. Dis. J. 2018, 37, 555–558. [Google Scholar] [CrossRef]
- Chitasombat, M.N.; Kontoyiannis, D.P. Treatment of mucormycosis in transplant patients: Role of surgery and of old and new antifungal agents. Curr. Opin. Infect. Dis. 2016, 29, 340–345. [Google Scholar] [CrossRef]
- Middelhof, C.A.; Loudon, W.G.; Muhonen, M.D.; Xavier, C.; Greene, C.S., Jr. Improved survival in central nervous system aspergillosis: A series of immunocompromised children with leukemia undergoing stereotactic resection of aspergillomas. Report of four cases. J. Neurosurg. 2005, 103, 374–378. [Google Scholar] [CrossRef] [PubMed]
- Dotis, J.; Iosifidis, E.; Roilides, E. Central nervous system aspergillosis in children: A systematic review of reported cases. Int. J. Infect. Dis. 2007, 11, 381–393. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gunzer, M.; Thornton, C.R.; Beziere, N. Advances in the In Vivo Molecular Imaging of Invasive Aspergillosis. J. Fungi 2020, 6, 338. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Compound (Formulation) | Pediatric Approval | Pediatric Dosage | Comments |
|---|---|---|---|
| Liposomal amphotericin B (iv) | Children of all ages | 3 mg/kg per day in one dose Mucormycosis: 5–10 mg/kg per day in one dose | Less nephrotoxic than amphotericin B deoxycholate |
| Amphotericin B lipid complex (iv) | Children ≥ 1 month | 5 mg/kg per day in one dose | Infusion-related toxicity similar, but less nephrotoxic than amphotericin B deoxycholate |
| Voriconazole (iv and oral) | Children ≥ 2 years | Children aged 2–<12 years or 12–14 years and weighing <50 kg: 8 mg/kg (day 1, 9 mg/kg) twice daily intravenously or 9 mg/kg twice daily orally; children aged ≥15 years or 12–14 years and weighing ≥50 kg: 4 mg/kg (day 1, 6 mg/kg) twice daily intravenously or 200 mg twice daily orally | TDM recommended First choice in CNS aspergillosis Not active against mucormycetes |
| Posaconazole (iv and oral) | EU: no US: ≥13 years (prophylaxis) | Patients ≥13 years: Delayed release tablets, 300 mg/d in one dose (day 1: 300 mg twice); patients from 1 month to 12 years: oral suspension, starting dose 6 mg/kg three times daily + TDM | Problems with absorption with the oral suspension Most likely limited activity in CNS |
| Isavuconazole (iv and oral) | No | 10 mg/kg per day in one dose, maximal dose of 372 mg isavuconazonium sulfate (d 1 and 2: three times daily) | Suggested dose corresponds to that investigated in a pediatric phase II trial (part of the Pediatric Investigation Plan) |
| Caspofungin (iv) | Children of all ages | 50 mg/m2 per day (day 1, 70 mg/m2) in one dose (maximum dose 70 mg per day) | Limited penetration to the CNS |
| Micafungin (iv) | Children of all ages | 2–4 mg/kg per day (in children weighing ≥50 kg, 100–200 mg) in one dose | Limited penetration to the CNS |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Luckowitsch, M.; Rudolph, H.; Bochennek, K.; Porto, L.; Lehrnbecher, T. Central Nervous System Mold Infections in Children with Hematological Malignancies: Advances in Diagnosis and Treatment. J. Fungi 2021, 7, 168. https://0-doi-org.brum.beds.ac.uk/10.3390/jof7030168
Luckowitsch M, Rudolph H, Bochennek K, Porto L, Lehrnbecher T. Central Nervous System Mold Infections in Children with Hematological Malignancies: Advances in Diagnosis and Treatment. Journal of Fungi. 2021; 7(3):168. https://0-doi-org.brum.beds.ac.uk/10.3390/jof7030168
Chicago/Turabian StyleLuckowitsch, Marie, Henriette Rudolph, Konrad Bochennek, Luciana Porto, and Thomas Lehrnbecher. 2021. "Central Nervous System Mold Infections in Children with Hematological Malignancies: Advances in Diagnosis and Treatment" Journal of Fungi 7, no. 3: 168. https://0-doi-org.brum.beds.ac.uk/10.3390/jof7030168