Comparison of DNA Extracted from Pediatric Saliva, Gingival Crevicular Fluid and Site-Specific Biofilm Samples


Abstract
:1. Introduction
2. Methods
2.1. Study Approval
2.2. Original Sample Collection
2.3. DNA Isolation
2.4. DNA Analysis
2.5. qPCR Screening
- (Nucleotide = nt; Tm = melting temperature)
- Bacterial 16S rRNA
- Forward 16S rRNA universal primer, 5′-ACGCGTCGACAGAGTTTGATCCTGGCT-3′
- 27 nt, 56% GC, Tm 76 °C
- Reverse 16S rRNA universal primer, 5′-GGGACTACCAGGGTATCTAAT-3′
- 21 nt, 48% GC, Tm 62 °C
- 16S probe: (6-FAM)-5′-CGTATTACCGCGGCTGCTGGCAC-3′-(TAMRA)
- 23 nt, 65% GC, Tm 76 °C
- Forward primer-GAPDH, 5′-ATCTTCCAGGAGCGAGATCC-3′
- 20 nt, 55% GC, Tm 66 °C
- Reverse primer-GAPDH, 5′- ACCACTGACACGTTGGCAGT-3′
- 20 nt, 55% GC, Tm 70 °C
- GAPDH probe: (6-FAM)-5′-CCTCTACTGGCGCTGCCAAGGCT-3′-(TAMRA)
- 23 nt, 65% GC, Tm 77 °C
2.6. qPCR Analysis
2.7. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Buzalaf, M.A.R.; Ortiz, A.C.; Carvalho, T.S.; Fideles, S.O.M.; Araújo, T.T.; Moraes, S.M.; Buzalaf, N.R.; Reis, F.N. Saliva as a diagnostic tool for dental caries, periodontal disease and cancer: Is there a need for more biomarkers? Expert Rev. Mol. Diagn. 2020, 30, 543–555. [Google Scholar] [CrossRef] [PubMed]
- Sereno, D.; Akhoundi, M.; Sayehmri, K.; Mirzaei, A.; Holzmuller, P.; Lejon, V.; Waleckx, E. Noninvasive biological samples to detect and diagnose infections due to trypanosomatidae parasites: A systematic review and meta-analysis. Int. J. Mol. Sci. 2020, 21, 1684. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martina, E.; Campanati, A.; Diotallevi, F.; Offidani, A. Saliva and oral diseases. J. Clin. Med. 2020, 9, 466. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bostanci, N.; Bao, K.; Greenwood, D.; Silbereisen, A.; Belibasakis, G.N. Periodontal disease: From the lenses of light microscopy to the specs of proteomics and next-generation sequencing. Adv. Clin. Chem. 2019, 93, 263–290. [Google Scholar] [CrossRef]
- Arias-Bujanda, N.; Regueira-Iglesias, A.; Balsa-Castro, C.; Nibali, L.; Donos, N.; Tomás, I. Accuracy of single molecular biomarkers in saliva for the diagnosis of periodontitis: A systematic review and meta-analysis. J. Clin. Periodontol. 2020, 47, 2–18. [Google Scholar] [CrossRef]
- Esteves, C.V.; Campos, W.G.; Souza, M.M.; Lourenço, S.V.; Siqueira, W.L.; Lemos-Júnior, C.A. Diagnostic potential of saliva proteome analysis: A review and guide to clinical practice. Braz. Oral Res. 2019, 33, e043. [Google Scholar] [CrossRef] [Green Version]
- Zhang, L.; Sun, T.; Zhu, P.; Sun, Z.; Li, S.; Li, F.; Zhang, Y.; Tan, K.; Lu, J.; Yuan, R.; et al. Quantitative analysis of salivary oral bacteria associated with severe early childhood caries and construction of caries assessment model. Sci. Rep. 2020, 10, 6365. [Google Scholar] [CrossRef] [Green Version]
- Nagel, A.; Dimitrakopoulou, E.; Teig, N.; Kern, P.; Lücke, T.; Michna, D.; Korn, K.; Steininger, P.; Shahada, K.; Neumann, K.; et al. Characterization of a universal screening approach for congenital CMV infection based on a highly-sensitive, quantitative, multiplex real-time PCR assay. PLoS ONE 2020, 15, e0227143. [Google Scholar] [CrossRef]
- Santigli, E.; Koller, M.; Klug, B. Oral biofilm sampling for microbiome analysis in healthy children. J. Vis. Exp. 2017, 130, e56320. [Google Scholar] [CrossRef] [Green Version]
- Papagerakis, P.; Zheng, L.; Kim, D.; Said, R.; Ehlert, A.A.; Chung, K.K.M.; Papagerakis, S. Saliva and gingival crevicular fluid (GCF) collection for biomarker screening. Methods Mol Biol. 2019, 1922, 549–562. [Google Scholar] [CrossRef]
- Carr, G.; Alexander, A.; Dionisio, K.; Kingsley, K. Quantitative comparison of oral site-specific DNA isolates reveals differential outcomes. J. Adv. Biol. Biotechnol. 2019, 22, 1–7. [Google Scholar] [CrossRef]
- Kommerein, N.; Stumpp, S.N.; Müsken, M.; Ehlert, N.; Winkel, A.; Häussler, S.; Behrens, P.; Buettner, F.F.; Stiesch, M. An oral multispecies biofilm model for high content screening applications. PLoS ONE 2017, 12, e0173973. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Verma, D.; Garg, P.K.; Dubey, A.K. Insights into the human oral microbiome. Arch. Microbiol. 2018, 200, 525–540. [Google Scholar] [CrossRef]
- Mosaddad, S.A.; Tahmasebi, E.; Yazdanian, A.; Rezvani, M.B.; Seifalian, A.; Yazdanian, M.; Tebyanian, H. Oral microbial biofilms: An update. Eur. J. Clin. Microbiol. Infect. Dis. 2019, 38, 2005–2019. [Google Scholar] [CrossRef] [PubMed]
- Bowen, W.H.; Burne, R.A.; Wu, H.; Koo, H. Oral biofilms: Pathogens, matrix, and polymicrobial interactions in microenvironments. Trends Microbiol. 2018, 26, 229–242. [Google Scholar] [CrossRef]
- Mira, A. Oral microbiome studies: Potential diagnostic and therapeutic implications. Adv. Dent. Res. 2018, 29, 71–77. [Google Scholar] [CrossRef]
- Larsen, T.; Fiehn, N.E. Dental biofilm infections—An update. APMIS 2017, 125, 376–384. [Google Scholar] [CrossRef]
- McDaniel, S.; McDaniel, J.; Tam, A.; Kingsley KHoward, K.M. Oral microbial ecology of selenemonas noxia and scardovia wiggsiae. Microbiol. Res. J. Int. 2017, 21, 1–8. [Google Scholar] [CrossRef]
- McDaniel, J.; McDaniel, S.; Tam, A.; Kingsley, K.; Howard, K.M. Screening a saliva repository for scardovia wiggsiae and streptococcus mutans: A Pilot Study. J. Adv. Microbiol. 2017, 5, 1–8. [Google Scholar] [CrossRef]
- Divaris, K.; Shungin, D.; Rodríguez-Cortés, A.; Basta, P.V.; Roach, J.; Cho, H.; Wu, D.; Ferreira Zandoná, A.G.; Ginnis, J.; Ramamoorthy, S.; et al. The supragingival biofilm in early childhood caries: Clinical and laboratory protocols and bioinformatics pipelines supporting metagenomics, metatranscriptomics, and metabolomics studies of the oral microbiome. Methods Mol. Biol. 2019, 1922, 525–548. [Google Scholar] [CrossRef] [PubMed]
- Agler, C.S.; Shungin, D.; Ferreira Zandoná, A.G.; Schmadeke, P.; Basta, P.V.; Luo, J.; Cantrell, J.; Pahel, T.D.; Meyer, B.D., Jr.; Shaffer, J.R.; et al. Protocols, methods, and tools for genome-wide association studies (GWAS) of dental traits. Methods Mol. Biol. 2019, 1922, 493–509. [Google Scholar] [CrossRef] [PubMed]
- Rupf, S.; Laczny, C.C.; Galata, V.; Backes, C.; Keller, A.; Umanskaya, N.; Erol, A.; Tierling, S.; Lo Porto, C.; Walter, J.; et al. Comparison of initial oral microbiomes of young adults with and without cavitated dentin caries lesions using an in situ biofilm model. Sci. Rep. 2018, 8, 14010. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paiva, M.F.; Delbem, A.C.B.; Danelon, M.; Nagata, M.E.; Moraes, F.R.N.; Coclete, G.E.G.; Cunha, R.F.; Buzalaf, M.A.R.; Pessan, J.P. Fluoride concentration and amount of dentifrice influence enamel demineralization in situ. J. Dent. 2017, 66, 18–22. [Google Scholar] [CrossRef] [PubMed]
- Diaz, P.I.; Valm, A.M. Microbial interactions in oral communities mediate emergent biofilm properties. J. Dent. Res. 2020, 99, 18–25. [Google Scholar] [CrossRef]
- Miller, D.P.; Fitzsimonds, Z.R.; Lamont, R.J. Metabolic signaling and spatial interactions in the oral polymicrobial community. J. Dent. Res. 2019, 98, 1308–1314. [Google Scholar] [CrossRef]
- Kreth, J.; Ferracane, J.L.; Pfeifer, C.S.; Khajotia, S.; Merritt, J. At the interface of materials and microbiology: A call for the development of standardized approaches to assay biomaterial-biofilm interactions. J. Dent. Res. 2019, 98, 850–852. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
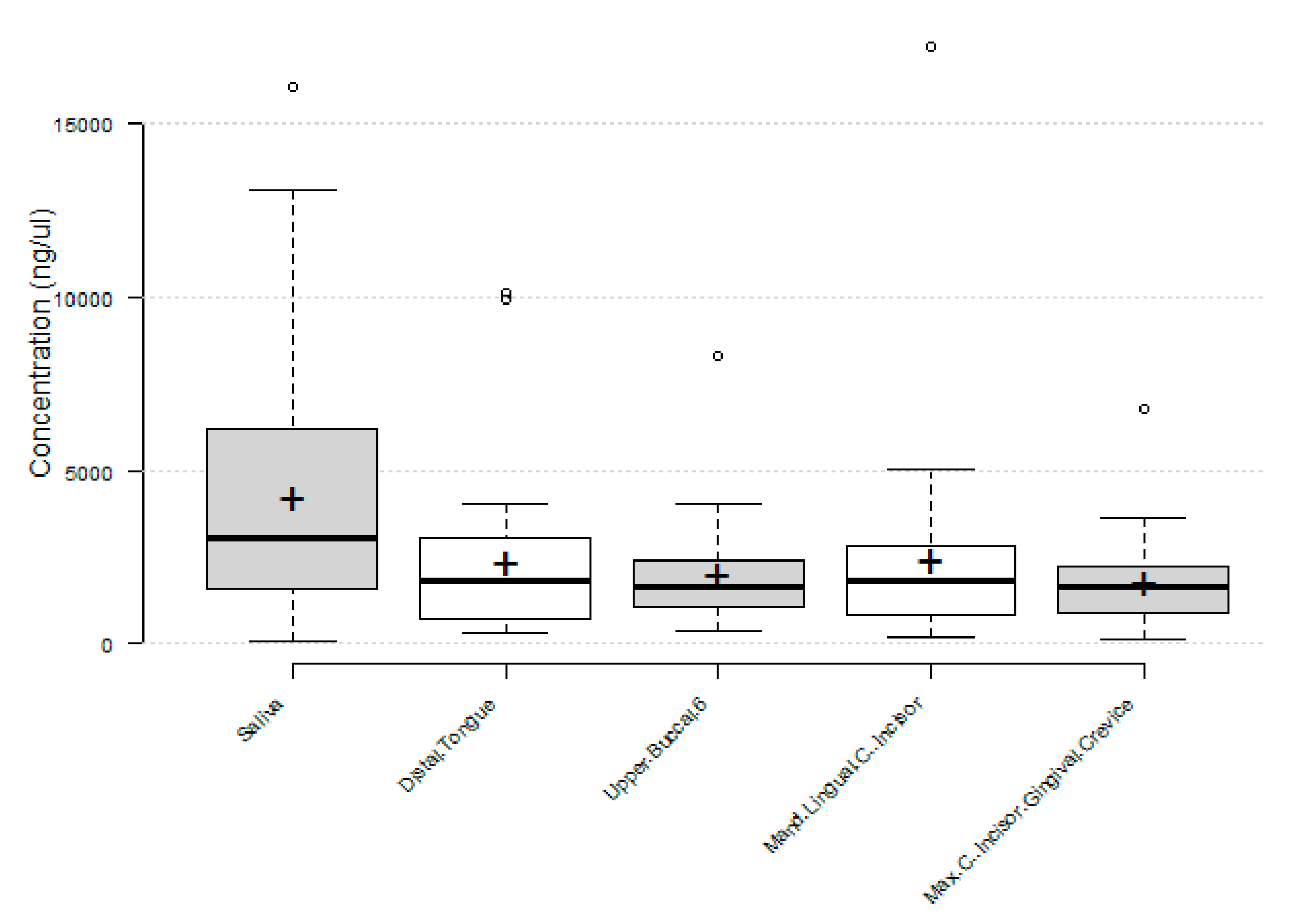
| Site | Concentration Mean ± SEM | Concentration Median | Statistical Analysis | Purity (A260:A280) Mean ± SEM (Range) | Contamination (A260:A230) Mean ± SEM (Range) |
|---|---|---|---|---|---|
| Saliva (n = 47) | 4264.1 ± 742.2 ng/μL | 3038.3 ng/μL | p = 0.0348 | 1.74 ± 0.22 (range: 1.56–2.02) | 1.92 ± 0.13 (range: 1.88–2.02) |
| Dorsum tongue (n = 47) | 2382.4 ± 445.1 ng/μL | 1797.9 ng/μL | 1.79 ± 0.19 (range: 1.64–1.99) | 1.99 ± 0.17 (range: 1.81–2.13) | |
| Upper buccal (n = 47) | 2048.4 ± 302.4 ng/μL | 1618.3 ng/μL | p = 0.5376 | 1.77 ± 0.26 (range: 1.63–2.11) | 1.98 ± 0.11 (range: 1.85–2.06) |
| Mandibular lingual (n = 47) | 2428.6 ± 576.5 ng/μL | 1795.8 ng/μL | 1.82 ± 0.31 (range: 1.55–1.95) | 2.01 ± 0.16 (range: 1.90–2.13) | |
| Gingival crevicular fluid (GCF) (n = 47) | 1771.5 ± 245.9 ng/μL | 1669.2 ng/μL | p = 0.4805 | 1.71 ± 0.22 (range: 1.60–1.98) | 1.96 ± 0.08 (range: 1.89–2.05) |
| Demographic | Study Sample | Clinic | Statistical Analysis |
|---|---|---|---|
| Sex | |||
| Female | n = 17/47 (36.2%) | 52.8% | Χ2 = 110.571, d.f. = 1 |
| Male | n = 30/47 (63.8%) | 47.2% | p = 0.0012 |
| Race/Ethnicity | |||
| White (non-Minority) | n = 2/47 (4.25%) | 24.7% | Χ2 = 223.753, d.f. = 1 |
| Minority | n = 45/47 (95.75%) | 75.3% | p = 0.00018 |
| Hispanic | n = 35/47 (74.5%) | 52.1% | |
| Black | n = 8/47 (17%) | 11.8% | |
| Asian/Other | n = 2/47 (4.25%) | 11.4% | |
| Age | |||
| Average age | 10.26 years | 11.34 years | |
| Age range | 5—15 years | 0—18 years |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Emett, J.; David, R.; McDaniel, J.; McDaniel, S.; Kingsley, K. Comparison of DNA Extracted from Pediatric Saliva, Gingival Crevicular Fluid and Site-Specific Biofilm Samples. Methods Protoc. 2020, 3, 48. https://0-doi-org.brum.beds.ac.uk/10.3390/mps3030048
Emett J, David R, McDaniel J, McDaniel S, Kingsley K. Comparison of DNA Extracted from Pediatric Saliva, Gingival Crevicular Fluid and Site-Specific Biofilm Samples. Methods and Protocols. 2020; 3(3):48. https://0-doi-org.brum.beds.ac.uk/10.3390/mps3030048
Chicago/Turabian StyleEmett, Jason, Roxanne David, Jaydene McDaniel, Steven McDaniel, and Karl Kingsley. 2020. "Comparison of DNA Extracted from Pediatric Saliva, Gingival Crevicular Fluid and Site-Specific Biofilm Samples" Methods and Protocols 3, no. 3: 48. https://0-doi-org.brum.beds.ac.uk/10.3390/mps3030048