
Difference in Movement between Superficial and Deep Parts of the Infrapatellar Fat Pad during Knee Extension
 , ,
, ,
Abstract
:1. Introduction
2. Methods
2.1. Procedures
2.2. Reliability
2.3. Statistical Analysis
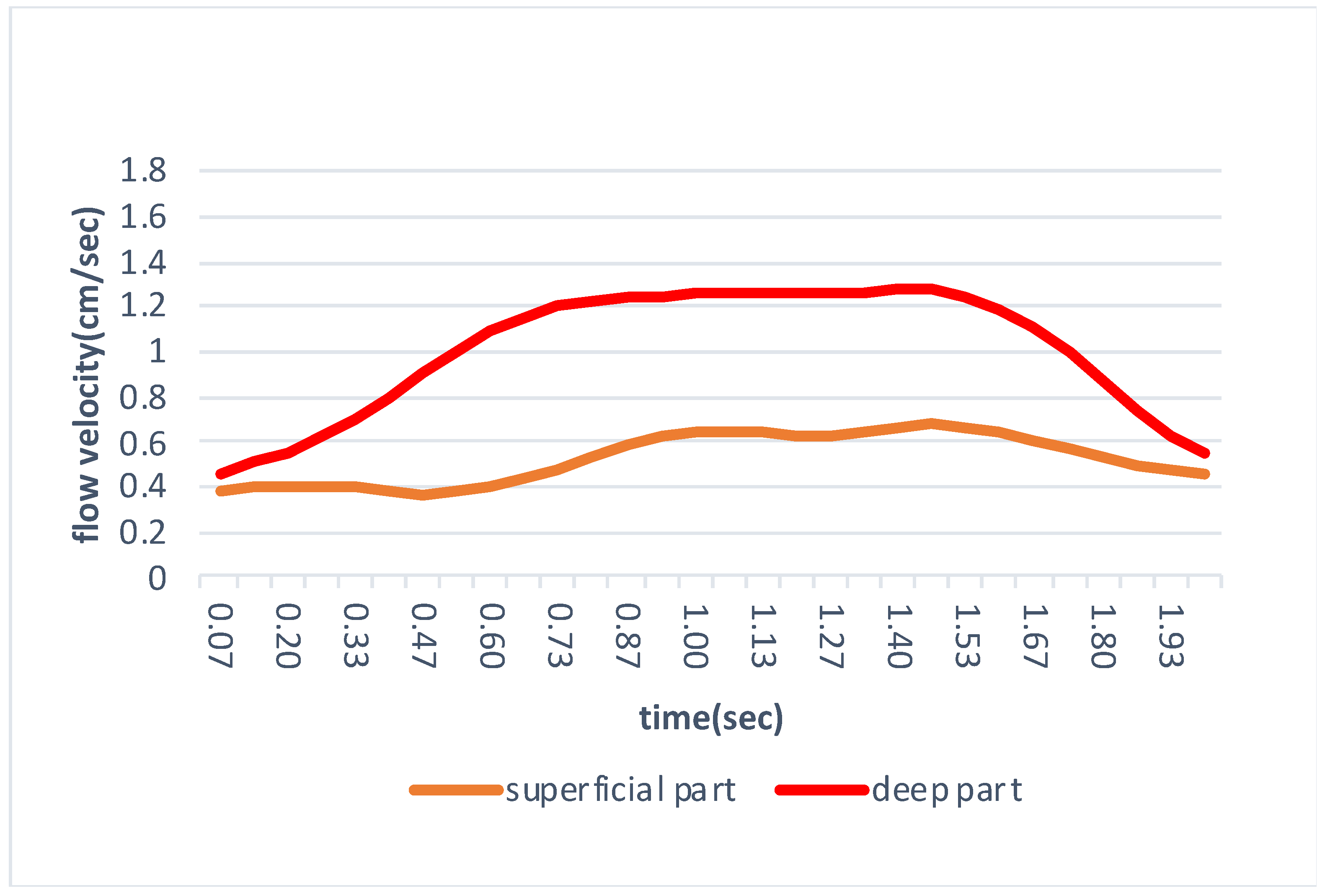
3. Results
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Carter, H.G. Gray’s Anatomy, 40th ed.; Elsevier: London, UK, 2016; p. 1576. [Google Scholar]
- Mace, J.; Bhatti, W.; Anand, S. Infrapatellar Fat Pad Syndrome: A Review of Anatomy, Function, Treatment and Dynamics. Acta Orthop. Belg. 2016, 82, 94–101. [Google Scholar] [PubMed]
- Dragoo, J.L.; Johnson, C.; McConnell, J. Evaluation and Treatment of Disorders of the Infrapatellar Fat Pad. Sports Med. 2012, 42, 51–67. [Google Scholar] [CrossRef] [PubMed]
- Eymard, F.; Chevalier, X. Inflammation of the Infrapatellar Fat Pad. Jt. Bone Spine 2016, 83, 389–393. [Google Scholar] [CrossRef] [PubMed]
- Murakami, S.; Muneta, T.; Ezura, Y.; Furuya, K.; Yamamoto, H. Quantitative Analysis of Synovial Fibrosis in the Infrapatellar Fat Pad before and after Anterior Cruciate Ligament Reconstruction. Am. J. Sports Med. 1997, 25, 29–34. [Google Scholar] [CrossRef] [PubMed]
- Paulos, L.E.; Wnorowski, D.C.; Greenwald, A.E. Infrapatellar Contracture Syndrome Diagnosis, Treatment, and Long-Term Followup. Am. J. Sports Med. 1994, 22, 440–449. [Google Scholar] [CrossRef] [PubMed]
- Macchi, V.; Picardi, E.E.E.; Fontanella, C.G.; Porzionato, A.; Stecco, C.; Tortorella, C.; Favero, M.; Natali, A.; de Caro, R. The Characteristics of the Lobular Arrangement Indicate the Dynamic Role Played by the Infrapatellar Fat Pad in Knee Kinematics. J. Anat. 2019, 235, 80–87. [Google Scholar] [CrossRef] [PubMed]
- Kitagawa, T.; Nakase, J.; Takata, Y.; Shimozaki, K.; Asai, K.; Tsuchiya, H. Use of Ultrasonography to Evaluate the Dynamics of the Infrapatellar Fat Pad after Anterior Cruciate Ligament Reconstruction: A Feasibility Study. J. Med. Ultrason. 2019, 46, 147–151. [Google Scholar] [CrossRef] [PubMed]
- Fontanella, C.G.; Macchi, V.; Porzionato, A.; Arduino, A.; Fotso Fogang, J.V.; de Caro, R.; Natali, A.N.; Carniel, E.L. A Numerical Investigation of the Infrapatellar Fat Pad. Proc. Inst. Mech. Eng. Part H J. Eng. Med. 2020, 234, 1113–1121. [Google Scholar] [CrossRef] [PubMed]
- Dragoo, J.L.; Phillips, C.; Schmidt, J.D.; Scanlan, S.F.; Blazek, K.; Steadman, J.R.; Williams, A. Mechanics of the Anterior Interval of the Knee Using Open Dynamic MRI. Clin. Biomech. 2010, 25, 433–437. [Google Scholar] [CrossRef] [PubMed]
- Okita, Y.; Oba, H.; Miura, R.; Morimoto, M.; Gamada, K. Movement and Volume of Infrapatellar Fat Pad and Knee Kinematics during Quasi-Static Knee Extension at 30 and 0° Flexion in Young Healthy Individuals. Knee 2020, 27, 71–80. [Google Scholar] [CrossRef] [PubMed]
- Kitagawa, T.; Nakase, J.; Takata, Y.; Shimozaki, K.; Asai, K.; Toyooka, K.; Tsuchiya, H. Relationship between the Deep Flexion of the Knee Joint and the Dynamics of the Infrapatellar Fat Pad after Anterior Cruciate Ligament Reconstruction via Ultrasonography. J. Phys. Ther. Sci. 2019, 31, 569–572. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mikkilineni, H.; Delzell, P.B.; Andrish, J.; Bullen, J.; Obuchowski, N.A.; Subhas, N.; Polster, J.M.; Schils, J.P. Ultrasound Evaluation of Infrapatellar Fat Pad Impingement: An Exploratory Prospective Study. Knee 2018, 25, 279–285. [Google Scholar] [CrossRef] [PubMed]
- Chang, P.H.; Chen, Y.J.; Chang, K.V.; Wu, W.T.; Özçakar, L. Ultrasound Measurements of Superficial and Deep Masticatory Muscles in Various Postures: Reliability and Influencers. Sci. Rep. 2020, 10, 14357. [Google Scholar] [CrossRef] [PubMed]
- Dilley, A.; Greening, J.; Lynn, B.; Leary, R.; Morris, V. The Use of Cross-Correlation Analysis between High-Frequency Ultrasound Images to Measure Longitudinal Median Nerve Movement. Ultrasound Med. Biol. 2001, 27, 1211–1218. [Google Scholar] [CrossRef]
- Kawanishi, K.; Kudo, S.; Yokoi, K. Relationship between Gliding and Lateral Femoral Pain in Patients with Trochanteric Fracture. Arch. Phys. Med. Rehabil. 2019, 101, 457–463. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variable | |
|---|---|
| Sex (male:female) | 8:7 |
| Age (years) | 20.6 ± 0.5 |
| Height (cm) | 164.5 ± 10.4 |
| Weight (kg) | 60.4 ± 14.0 |
| Body mass index (kg/m²) | 22.1 ± 3.5 |
| Intra-Rater Correlation Coefficient | ICC(1.2) | 95%CI | df | SEM(m/s) | MDC95(m/s) |
| flow velocity of superficial part | 0.92 | 0.78–0.97 | 14.00 | 0.06 | 0.16 |
| flow velocity of deep part | 0.82 | 0.56–0.94 | 14.00 | 0.08 | 0.21 |
| Inter-Rater Correlation Coefficient | ICC(2.2) | 95%CI | df | SEM(m/s) | MDC95(m/s) |
| flow velocity of superficial part | 0.96 | 0.89–0.98 | 14.00 | 0.06 | 0.16 |
| flow velocity of deep part | 0.89 | 0.66–0.96 | 14.00 | 0.05 | 0.15 |
| Superficial Part | Deep Part | p-Value | |
|---|---|---|---|
| flow velocity(cm/s) | 0.80 ± 0.21 | 1.33 ± 0.10 | <0.05 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nakanishi, S.; Morimoto, R.; Kitano, M.; Kawanishi, K.; Tanaka, A.; Kudo, S. Difference in Movement between Superficial and Deep Parts of the Infrapatellar Fat Pad during Knee Extension. J. Funct. Morphol. Kinesiol. 2021, 6, 68. https://0-doi-org.brum.beds.ac.uk/10.3390/jfmk6030068
Nakanishi S, Morimoto R, Kitano M, Kawanishi K, Tanaka A, Kudo S. Difference in Movement between Superficial and Deep Parts of the Infrapatellar Fat Pad during Knee Extension. Journal of Functional Morphology and Kinesiology. 2021; 6(3):68. https://0-doi-org.brum.beds.ac.uk/10.3390/jfmk6030068
Chicago/Turabian StyleNakanishi, Syoya, Ryosuke Morimoto, Masashi Kitano, Kengo Kawanishi, Arisa Tanaka, and Shintarou Kudo. 2021. "Difference in Movement between Superficial and Deep Parts of the Infrapatellar Fat Pad during Knee Extension" Journal of Functional Morphology and Kinesiology 6, no. 3: 68. https://0-doi-org.brum.beds.ac.uk/10.3390/jfmk6030068