
Concurrent Exercise Training: Long-Term Changes in Body Composition and Motives for Continued Participation in Women with Obesity
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
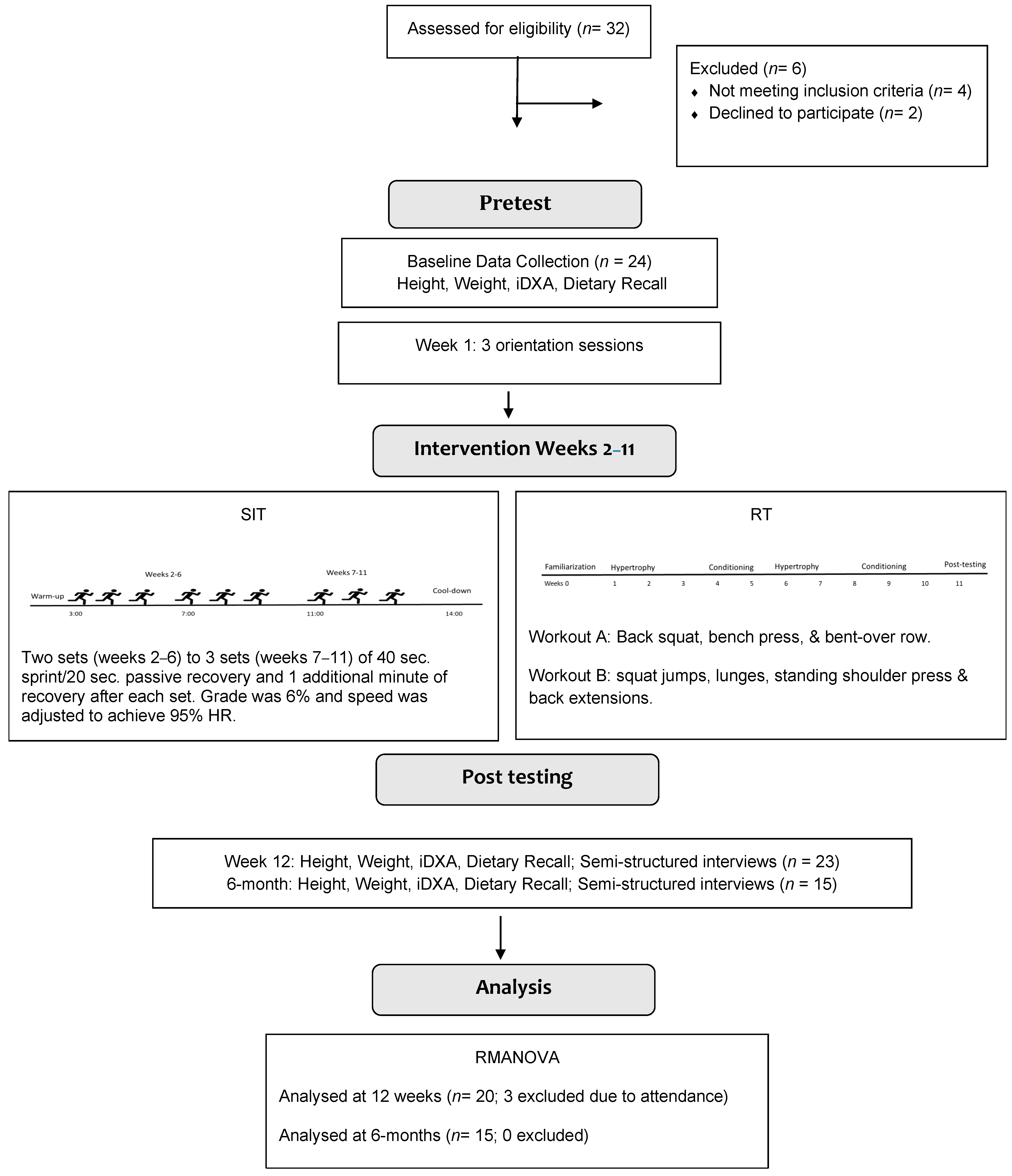
2.2. Study Design
2.3. Concurrent Exercise Program
2.3.1. SIT Protocol
2.3.2. Resistance Training Protocol
2.4. Measures
2.4.1. Anthropometrics
2.4.2. Body Composition
2.4.3. Dietary Recall
2.4.4. Semi-Structured Interviews
2.5. Statistical Analysis
3. Results
3.1. Body Composition
3.1.1. Fat Mass
3.1.2. Visceral Fat Mass
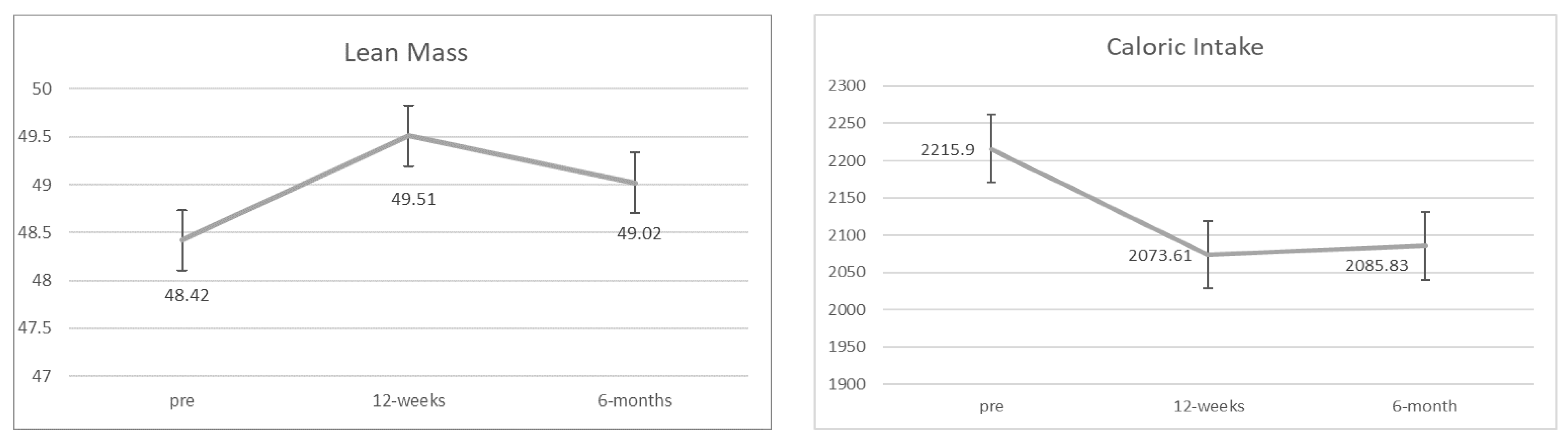
3.1.3. Lean Body Mass
3.2. Semi-Structured Interviews
3.2.1. 12 Weeks
3.2.2. 6 Months
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Puska, P.; Nishida, C.; Porter, D. Obesity and Overweight; World Health Organization: Geneva, Switzerland, 2003; pp. 1–2. [Google Scholar]
- Hales, C.M.; Fryar, C.D.; Carroll, M.D.; Freedman, D.S.; Aoki, Y.; Ogden, C.L. Differences in obesity prevalence by demographic characteristics and urbanization level among adults in the United States, 2013–2016. JAMA 2018, 319, 2419–2429. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Y.; Beydoun, M.A.; Min, J.; Xue, H.; Kaminsky, L.A.; Cheskin, L.J. Has the prevalence of overweight, obesity and central obesity levelled off in the United States? Trends, patterns, disparities, and future projections for the obesity epidemic. Int. J. Epidemiol. 2020, 49, 810–823. [Google Scholar] [CrossRef]
- Chu, D.T.; Nguyet, M.; Dinh, T.C.; Lien, T.; Nguyen, K.H.; Ngoc, V.N.; Tao, Y.; Le, D.H.; Nga, V.B.; Jurgoński, A.; et al. An update on physical health and economic consequences of overweight and obesity. Diabetol. Metab. Syndr. 2018, 12, 1095–1100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zheng, Y.; Manson, J.E.; Yuan, C.; Liang, M.H.; Grodstein, F.; Stampfer, M.J.; Willett, W.C.; Hu, F.B. Associations of weight gain from early to middle adulthood with major health outcomes later in life. JAMA 2017, 318, 255–269. [Google Scholar] [CrossRef] [PubMed]
- King, A.C.; Whitt-Glover, M.C.; Marquez, D.X.; Buman, M.P.; Napolitano, M.A.; Jakicic, J.; Fulton, J.E.; Tennant, B.L. Physical Activity Promotion: Highlights from the 2018 Physical Activity Guidelines Advisory Committee Systematic Review. MSSE 2019, 51, 1340–1353. [Google Scholar] [CrossRef] [PubMed]
- Verheggen, R.; Maessen, M.; Green, D.J.; Hermus, A.; Hopman, M.; Thijssen, D. A systematic review and meta-analysis on the effects of exercise training versus hypocaloric diet: Distinct effects on body weight and visceral adipose tissue. Obes. Rev. 2016, 17, 664–690. [Google Scholar] [CrossRef]
- Després, J.P. Is visceral obesity the cause of the metabolic syndrome? Ann. Behav. Med. 2006, 38, 52–63. [Google Scholar] [CrossRef]
- Eckel, R.H.; Grundy, S.M.; Zimmet, P.Z. The metabolic syndrome. Lancet 2005, 365, 1415–1428. [Google Scholar] [CrossRef]
- Center for Disease Control and Prevention. Table A-14a. Age-Adjusted Percent Distributions (with Standard Errors) of Participation in Leisure-Time Aerobic and Muscle-Strengthening Activities that Meet the 2008 Federal Physical Activity Guidelines among Adults Aged 18 and over, by Selected Characteristics; Center for Disease Control and Prevention: Atlanta, GA, USA, 2018.
- Edwards, E.S.; Sackett, S.C. Psychosocial Variables Related to Why Women are Less Active than Men and Related Health Implications. Clin. Med. Insights Women’s Health 2016, 9, 47–56. [Google Scholar] [CrossRef] [Green Version]
- Towne, S.D.; Xu, M.; Zhu, X.; Ory, M.G.; Lee, S.; Lee, C. Differential Effects of a Global Public Health Crisis on Physical Activity: Evidence From a Statewide Survey From the United States. HERD Health Environ. Res. Des. J. 2022, 15, 63–80. [Google Scholar] [CrossRef]
- Atakan, M.M.; Li, Y.; Koşar, Ş.N.; Turnagöl, H.H.; Yan, X. Evidence-based effects of high-intensity interval training on exercise capacity and health: A review with historical perspective. Int. J. Environ. Res. Public Health 2021, 18, 7201. [Google Scholar] [CrossRef] [PubMed]
- Gibala, M.J.; McGee, S.L. Metabolic adaptations to short-term high-intensity interval training: A little pain for a lot of gain? Exerc. Sport Sci. Rev. 2008, 36, 58–63. [Google Scholar] [CrossRef] [PubMed]
- Babraj, J.A.; Vollaard, N.B.; Keast, C.; Guppy, F.M.; Cottrell, G.; Timmons, J.A. Extremely short duration high intensity interval training substantially improves insulin action in young healthy males. BMC Endocr. Disord. 2009, 9, 3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cocks, M.; Shaw, C.S.; Shepherd, S.O.; Fisher, J.P.; Ranasinghe, A.M.; Barker, T.A.; Tipton, K.D.; Wagenmakers, A.J. Sprint interval and endurance training are equally effective in increasing muscle microvascular density and eNOS content in sedentary males. J. Physiol. 2013, 591, 641–656. [Google Scholar] [CrossRef] [PubMed]
- Wewege, M.; Van Den Berg, R.; Ward, R.; Keech, A. The effects of high-intensity interval training vs. moderate-intensity continuous training on body composition in overweight and obese adults: A systematic review and meta-analysis. Obes. Rev. 2017, 18, 635–646. [Google Scholar] [CrossRef] [PubMed]
- Boutcher, S.H. High-intensity intermittent exercise and fat loss. J. Obes. 2011, 2011, 868305. [Google Scholar] [CrossRef] [Green Version]
- Zhang, H.; Tong, T.K.; Kong, Z.; Shi, Q.; Liu, Y.; Nie, J. Exercise training-induced visceral fat loss in obese women: The role of training intensity and modality. Scand. J. Med. Sci. Sport. 2021, 31, 30–43. [Google Scholar] [CrossRef]
- Piercy, K.L.; Troiano, R.P.; Ballard, R.M.; Carlson, S.A.; Fulton, J.E.; Galuska, D.A.; George, S.M.; Olson, R.D. The physical activity guidelines for Americans. JAMA 2018, 320, 2020–2028. [Google Scholar] [CrossRef]
- Sarsan, A.; Ardiç, F.; Özgen, M.; Topuz, O.; Sermez, Y. The effects of aerobic and resistance exercises in obese women. Clin. Rehabil. 2006, 20, 773–782. [Google Scholar] [CrossRef]
- Petridou, A.; Siopi, A.; Mougios, V. Exercise in the management of obesity. Metabolism 2019, 92, 163–169. [Google Scholar] [CrossRef]
- Momma, H.; Kawakami, R.; Honda, T.; Sawada, S.S. Muscle-strengthening activities are associated with lower risk and mortality in major non-communicable diseases: A systematic review and meta-analysis of cohort studies. BJSM 2022, 56, 755–763. [Google Scholar] [CrossRef] [PubMed]
- Wilson, J.M.; Marin, P.J.; Rhea, M.R.; Wilson, S.M.; Loenneke, J.P.; Anderson, J.C. Concurrent training: A meta-analysis examining interference of aerobic and resistance exercises. J. Strength Cond. Res. 2012, 26, 2293–2307. [Google Scholar] [CrossRef] [PubMed]
- Davis, W.J.; Wood, D.T.; Andrews, R.G.; Elkind, L.M.; Davis, W.B. Concurrent training enhances athletes’ strength, muscle endurance, and other measures. J. Strength Cond. Res. 2008, 22, 1487–1502. [Google Scholar] [CrossRef]
- Hardcastle, S.J.; Ray, H.; Beale, L.; Hagger, M.S. Why sprint interval training is inappropriate for a largely sedentary population. Front. Psychol. 2014, 5, 1505. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bartlett, J.D.; Close, G.L.; MacLaren, D.P.; Gregson, W.; Drust, B.; Morton, J.P. High-intensity interval running is perceived to be more enjoyable than moderate-intensity continuous exercise: Implications for exercise adherence. J. Sport. Sci. 2011, 29, 547–553. [Google Scholar] [CrossRef] [PubMed]
- Thum, J.S.; Parsons, G.; Whittle, T.; Astorino, T.A. High-intensity interval training elicits higher enjoyment than moderate intensity continuous exercise. PLoS ONE 2017, 12, e0166299. [Google Scholar] [CrossRef] [Green Version]
- Kong, Z.; Fan, X.; Sun, S.; Song, L.; Shi, Q.; Nie, J. Comparison of high-intensity interval training and moderate-to-vigorous continuous training for cardiometabolic health and exercise enjoyment in obese young women: A randomized controlled trial. PLoS ONE 2016, 11, e0158589. [Google Scholar] [CrossRef] [Green Version]
- Jamnik, V.K.; Warburton, D.E.; Makarski, J.; McKenzie, D.C.; Shephard, R.J.; Stone, J.A.; Charlesworth, S.; Gledhill, N. Enhancing the effectiveness of clearance for physical activity participation: Background and overall process. Appl. Physiol. Nutr. Metab. 2011, 36, S3–S13. [Google Scholar] [CrossRef] [Green Version]
- American College of Sports Medicine. ACSM Health-Related Physical Fitness Assessment Manual; Wolters Kluwer Health: Philadelphia, PA, USA; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2013. [Google Scholar]
- McNair, P.J.; Colvin, M.; Reid, D. Predicting maximal strength of quadriceps from submaximal performance in individuals with knee joint osteoarthritis. Arthritis Care Res. 2011, 63, 216–222. [Google Scholar] [CrossRef]
- Toombs, R.J.; Ducher, G.; Shepherd, J.A.; De Souza, M.J. The impact of recent technological advances on the trueness and precision of DXA to assess body composition. Obesity 2012, 20, 30–39. [Google Scholar] [CrossRef]
- Rothney, M.P.; Martin, F.P.; Xia, Y.; Beaumont, M.; Davis, C.; Ergun, D.; Fay, L.; Ginty, F.; Kochhar, S.; Wacker, W. Precision of GE Lunar iDXA for the measurement of total and regional body composition in nonobese adults. J. Clin. Densitom. 2012, 15, 399–404. [Google Scholar] [CrossRef] [PubMed]
- Rezzi, S.; Ginty, F.; Beaumont, M.; Blondel-Lubrano, A.; Oguey-Araymon, S.; Wacker, W.; Barden, H.; Kochhar, S.; Fay, L.; Ergun, D. Body composition precision with the Lunar iDXA. J. Clin. Densitom. 2009, 3, 402. [Google Scholar] [CrossRef]
- Kaul, S.; Rothney, M.P.; Peters, D.M.; Wacker, W.K.; Davis, C.E.; Shapiro, M.D.; Ergun, D.L. Dual-energy X-ray absorptiometry for quantification of visceral fat. Obesity 2012, 20, 1313–1318. [Google Scholar] [CrossRef] [Green Version]
- Carter, C.; Bryant-Lukosius, D.; DiCenso, A.; Blythe, J.; Neville, A. The use of triangulation in qualitative research. Oncol. Nurs. Forum 2014, 41, 545–547. [Google Scholar] [CrossRef]
- Xiao, T.; Fu, Y.F. Resistane training vs. aerobic training and role of other factors on the exercise effects on visceral fat. Eur. Rev. Med. Pharmacol. Sci. 2015, 19, 1779–1784. [Google Scholar]
- Thomas, E.; Gentile, A.; Lakicevic, N.; Moro, T.; Bellafiore, M.; Paoli, A.; Drid, P.; Palma, A.; Bianco, A. The effect of resistance training programs on lean body mass in postmenopausal and elderly women: A meta-analysis of observational studies. Aging Clin. Exp. Res. 2021, 33, 2941–2952. [Google Scholar] [CrossRef] [PubMed]
- Rashti, B.A.; Mehrabani, J.; Damirchi, A.; Babaei, P. The influence of concurrent training intensity on serum irisin and abdominal fat in postmenopausal women. Menopause Rev. 2019, 18, 166–173. [Google Scholar] [CrossRef]
- Deci, E.L.; Ryan, R.M. Handbook of Self-Determination Research; University Rochester Press: Rochester, NY, USA, 2004. [Google Scholar]
- Lakicevic, N.; Gentile, A.; Mehrabi, S.; Cassar, S.; Parker, K.; Roklicer, R.; Bianco, A.; Drid, P. Make fitness fun: Could novelty be the key determinant for physical activity adherence? Front. Psychol. 2020, 11, 577522. [Google Scholar] [CrossRef]
- Wadsworth, D.D.; Hallam, J.S. Effect of a web site intervention on physical activity of college females. Am. J. Health Promot. 2010, 34, 60–69. [Google Scholar] [CrossRef]
- Gell, N.M.; Wadsworth, D.D. How dothey do it: Working women meeting physical activity recommendations. Am. J. Health Behav. 2014, 38, 208–217. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Pre (n = 24) M ± SD (95% CI) | 12 Weeks (n = 20) M ± SD (95% CI) | % Change from Pre | 6 Months (n = 15) M ± SD (95% CI) | % Change from Pre | ||||
|---|---|---|---|---|---|---|---|---|
| Age (yrs) | 37.10 ± 7.40 | |||||||
| Height (m) | 1.63 ± 0.09 | |||||||
| Weight (kg) | 97.91 ± 21.89 | 96.74 ± 22.55 | 1.19 | 94.54 ± 22.65 | 3.44 | |||
| BMI (kg/m2) | 36.90 ± 2.50 | 36.40 ± 2.98 | 1.35 | 35.40 ± 3.02 | 4.07 | |||
| F | p | η2 | ||||||
| Total Fat (kg) | 46.33 ± 16.78 (37.28, 55.87) | 43.97 ± 16.28 (34.12, 52.16) | −5.09 | 43.32 ± 17.59 (33.58, 53.06) | −6.50 | 8.82 | 0.001 | 0.390 |
| Gynoid Fat (kg) | 7.77 ± 2.53 (6.40, 2.91) | 7.22 ± 2.00 (5.88, 2.67) | −7.07 | 6.94 ± 2.04 (5.79, 2.63) | −10.68 | 6.13 | 0.006 | 0.305 |
| Android Fat (kg) | 4.48 ± 2.07 (3.36, 5.65) | 4.10 ± 1.76 (3.00, 4.95) | −8.48 | 4.09 ± 2.04 (2.95, 5.21) | −8.70 | 5.37 | 0.011 | 0.277 |
| Visceral Fat (kg) | 1.39 ± 0.84 (0.85, 1.88) | 1.11 ± 0.72 (0.70, 1.55) | −20.14 | 1.10 ± 0.95 (0.52, 1.6) | −20.86 | 4.13 | 0.029 | 0.256 |
| Lean Mass (kg) | 48.42 ± 7.75 (44.12, 52.72) | 49.51 ± 8.81 (44.63, 54.39) | 2.25 | 49.02 ± 8.88 (44.10, 53.95) | 1.23 | 2.52 | 0.099 | 0.152 |
| Caloric Intake (kcals) | 2224.00 ± 432.23 (1996.78, 2389.22) | 2093.00 ± 390.80 (1906.65, 2244.81) | −5.84 | 2085.00 ± 391.74 (1900.47, 2239.15) | −6.25 | 3.26 | 0.053 | 0.189 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wadsworth, D.D.; Suire, K.B.; Peart, A.; Foote, S.; Jones, C.; Rodriguez-Hernandez, M.; McDonald, J.R.; Pascoe, D.D. Concurrent Exercise Training: Long-Term Changes in Body Composition and Motives for Continued Participation in Women with Obesity. J. Funct. Morphol. Kinesiol. 2022, 7, 110. https://0-doi-org.brum.beds.ac.uk/10.3390/jfmk7040110
Wadsworth DD, Suire KB, Peart A, Foote S, Jones C, Rodriguez-Hernandez M, McDonald JR, Pascoe DD. Concurrent Exercise Training: Long-Term Changes in Body Composition and Motives for Continued Participation in Women with Obesity. Journal of Functional Morphology and Kinesiology. 2022; 7(4):110. https://0-doi-org.brum.beds.ac.uk/10.3390/jfmk7040110
Chicago/Turabian StyleWadsworth, Danielle D., Kameron B. Suire, Ashley Peart, Shelby Foote, Chloe Jones, Mynor Rodriguez-Hernandez, James R. McDonald, and David D. Pascoe. 2022. "Concurrent Exercise Training: Long-Term Changes in Body Composition and Motives for Continued Participation in Women with Obesity" Journal of Functional Morphology and Kinesiology 7, no. 4: 110. https://0-doi-org.brum.beds.ac.uk/10.3390/jfmk7040110