
Musculoskeletal Morphology and Joint Flexibility-Associated Functional Characteristics across Three Time Points during the Menstrual Cycle in Female Contemporary Dancers

 and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Timing and Order of Procedures
2.3. A priori Identification of Menstrual Cycle Phases, Length, and Regularity
2.4. Biochemical Analyses
2.5. Anthropometry and In Vivo Body Composition
2.6. Muscle Architecture
2.7. Jump Performance Assessment
2.8. Semitendinosus Flexibility
2.9. Muscle Electromyographical Activity
2.10. Pain Mixed-Method Assessment
2.11. Data Reduction
2.12. Outcome Variables
2.13. Statistical Analyses
3. Results
3.1. Descriptive Analysis
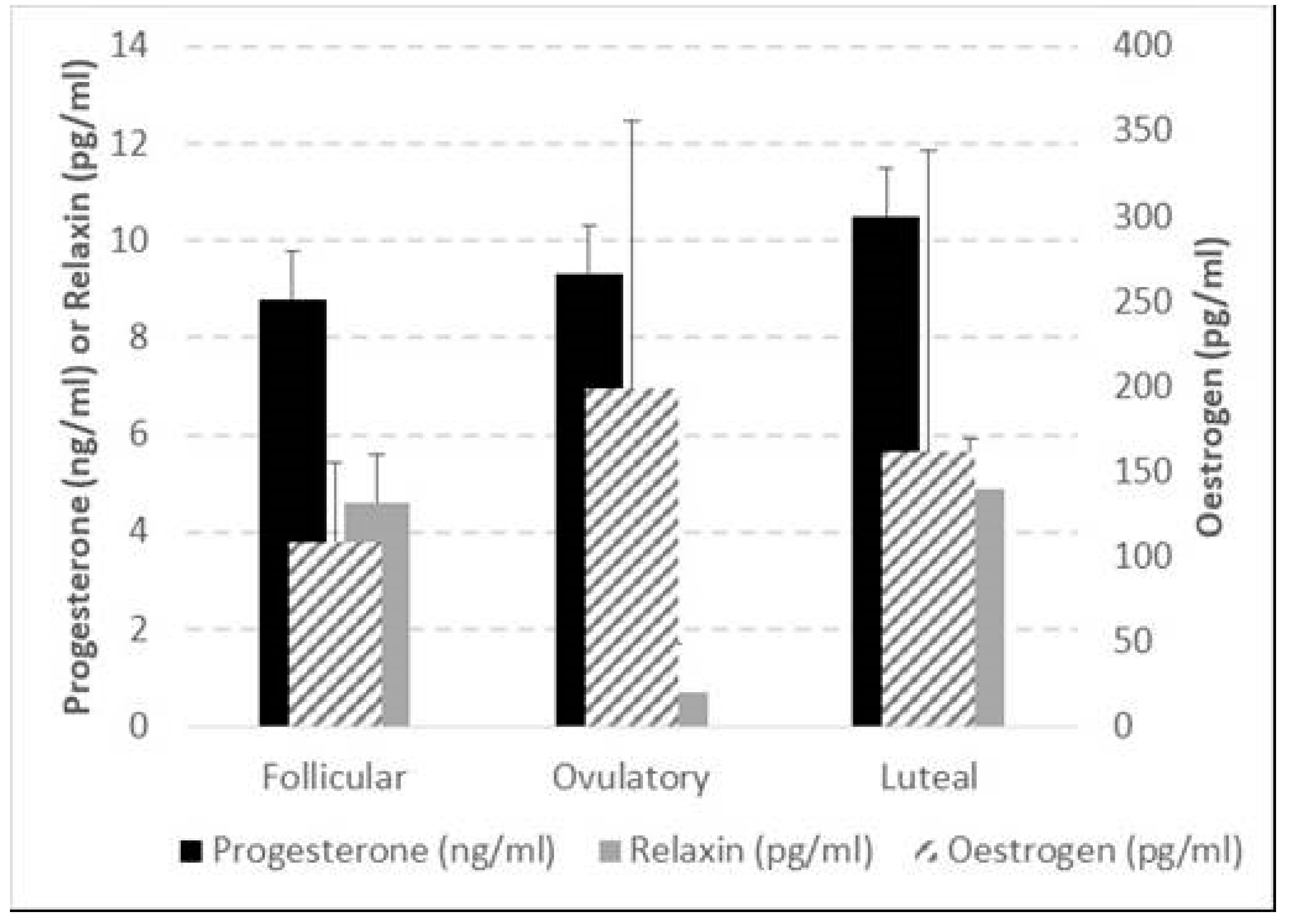
3.2. Hormonal Variation between Three Menstrual Cycle Phases
3.3. Structural, Functional, and Pain Sensation Characteristics across Three Menstrual Cycle Phases and Limb Comparisons
3.4. Relative Changes and Correlations between Change in Outcome Variables and Change in Hormone Levels
4. Discussion
4.1. Accuracy of Targeting of Hormonal Peaks within the MCP
4.2. Inferences from Grouped Raw Data
4.3. Inferences from Individually Normalised Data
4.4. Study Limitations and Recommendations for Future Work
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Strauss, J.F.; Barbieri, R.L. Yen & Jaffe’s Reproductive Endocrinology E-Book: Physiology, Pathophysiology, and Clinical Management; Elsevier Health Sciences: Amsterdam, The Netherlands, 2013. [Google Scholar]
- Becker, J.B.; Hu, M. Sex differences in drug abuse. Front. Neuroendocrinol. 2008, 29, 36–47. [Google Scholar] [CrossRef] [PubMed]
- Hackney, A.C.; Kallman, A.L.; Ağgön, E. Female sex hormones and the recovery from exercise: Menstrual cycle phase affects responses. Biomed. Hum. Kinet. 2019, 11, 87–89. [Google Scholar] [CrossRef] [PubMed]
- Xanne, A.K.; De Jonge, J. Effects of the Menstrual Cycle on Exercise Performance. Sports Med. 2003, 33, 833–851. [Google Scholar]
- Carmichael, M.A.; Thomson, R.L.; Moran, L.J.; Wycherley, T.P. The impact of menstrual cycle phase on athletes’ performance: A narrative review. Int. J. Environ. Res. Public Health 2021, 18, 1667. [Google Scholar] [CrossRef] [PubMed]
- Meignié, A.; Duclos, M.; Carling, C.; Orhant, E.; Provost, P.; Toussaint, J.-F.; Antero, J. The effects of menstrual cycle phase on elite athlete performance: A critical and systematic review. Front. Physiol. 2021, 12, 654585. [Google Scholar] [CrossRef] [PubMed]
- Pearson, S.J.; Burgess, K.E.; Onambélé, G.L. Serum relaxin levels affect the properties of some but not all tendons in normally menstruating young women. Exp. Physiol. 2011, 96, 681–688. [Google Scholar] [CrossRef] [PubMed]
- Sciore, P.; Frank, C.B.; Hart, D.A. Identification of sex hormone receptors in human and rabbit ligaments of the knee by reverse transcription-polymerase chain reaction: Evidence that receptors are present in tissue from both male and female subjects. J. Orthop. Res. 1998, 16, 604–610. [Google Scholar] [CrossRef] [PubMed]
- Park, S.-K.; Stefanyshyn, D.J.; Loitz-Ramage, B.; Hart, D.A.; Ronsky, J.L. Changing hormone levels during the menstrual cycle affect knee laxity and stiffness in healthy female subjects. Am. J. Sports Med. 2009, 37, 588–598. [Google Scholar] [CrossRef]
- Deie, M.; Sakamaki, Y.; Sumen, Y.; Urabe, Y.; Ikuta, Y. Anterior knee laxity in young women varies with their menstrual cycle. Int. Orthop. 2002, 26, 154–156. [Google Scholar] [CrossRef]
- Heitz, N.A.; Eisenman, P.A.; Beck, C.L.; Walker, J.A. Hormonal changes throughout the menstrual cycle and increased anterior cruciate ligament laxity in females. J. Athl. Train. 1999, 34, 144–149. [Google Scholar]
- Yamazaki, T.; Maruyama, S., Sato; Suzuki, Y.; Shimizu, S.; Kaneko, F.; Ikezu, M.; Matsuzawa, K.; Edama, M. A preliminary study exploring the change in ankle joint laxity and general joint laxity during the menstrual cycle in cis women. J. Foot Ankle Res. 2021, 14, 21. [Google Scholar] [CrossRef] [PubMed]
- Belanger, M.J.; Moore, D.C.; Crisco, J.J.; Fadale, P.D.; Hulstyn, M.J.; Ehrlich, M.G. Knee laxity does not vary with the menstrual cycle, before or after exercise. Am. J. Sports Med. 2004, 32, 1150–1157. [Google Scholar] [CrossRef]
- Eiling, E.; Bryant, A.L.; Petersen, W.; Murphy, A.; Hohmann, E. Effects of menstrual-cycle hormone fluctuations on musculotendinous stiffness and knee joint laxity. Knee Surg. Sports Traumatol. Arthrosc. 2007, 15, 126–132. [Google Scholar] [CrossRef]
- Parker, E.A.; Meyer, A.M.; Goetz, J.E.; Willey, M.C.; Westermann, R.W. Do Relaxin Levels Impact Hip Injury Incidence in Women? A Scoping Review. Front. Endocrinol. 2022, 13, 827512. [Google Scholar] [CrossRef] [PubMed]
- Tommaso, M. Pain Perception during Menstrual Cycle. Curr. Pain Headache Rep. 2011, 15, 400–406. [Google Scholar] [CrossRef] [PubMed]
- Piroli, A.; Mattei, A.; Carta, G.; D’Alfonso, A.; Palermo, P.; Marinangeli, F.; Alfonsi, B.; Testa, A.; Pasquale, C.; Varrassi, G.; et al. Influence of the menstrual cycle phase on pain perception and analgesic requirements in young women undergoing gynecological laparoscopy. Pain Pract. 2018, 19, 140–148. [Google Scholar] [CrossRef]
- Chagas, M.H.; Menzel, H.-J.; Bhering, E.L.; Bergamini, J.C. Comparação de duas diferentes intensidades de alongamento na amplitude de movimento. Rev. Bras. de Med. do Esporte 2008, 14, 99–103. [Google Scholar] [CrossRef]
- Pessali-Marques, B.; Peixoto, G.H.; Cabido, C.E.; Andrade, A.G.P.; Rodrigues, S.A.; Tourino, F.D.; O’Dowd, D.; Chagas, M.H. Biomechanical Response to Acute Stretching in Dancers and Non-Dancers. J. Danc. Med. Sci. 2020, 24, 12–18. [Google Scholar] [CrossRef]
- Sumant, S.A.; Wakode, P. Game of laxity between female sex hormones in menstrual cycle & ligamentous structures: A mini literature review. Int. J. Recent Adv. Multidiscip. Res. 2021, 08, 7144–7147. [Google Scholar]
- Chagas, M.H.; Magalhães, F.A.; Peixoto, G.H.C.; Pereira, B.M.; Andrade, A.G.P.; Menzel, H.-J.K. Exploratory factor analysis for differentiating sensory and mechanical variables related to muscle-tendon unit elongation. Braz. J. Phys. Ther. 2016, 20, 240–247. [Google Scholar] [CrossRef]
- Association, W.M. World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA 2013, 310, 2191–2194. [Google Scholar]
- American College of Sports Medicine. ACSM’s Health/Fitness Facility Standards and Guidelines; Human Kinetics: Champaign, IL, USA, 2012. [Google Scholar]
- Miller, P.B.; Soules, M.R. The usefulness of a urinary LH kit for ovulation prediction during menstrual cycles of normal women. Obstet. Gynecol. 1996, 87, 13–17. [Google Scholar] [CrossRef] [PubMed]
- Coqueiro, R.d.S.; Santos, M.C.; Neto, J.d.S.L.; de Queiroz, B.M.; Brügger, N.A.J.; Barbosa, A.R. Validity of a Portable Glucose, Total Cholesterol, and Triglycerides Multi-Analyzer in Adults. Biol. Res. Nurs. 2014, 16, 288–294. [Google Scholar] [CrossRef]
- Miyatani, M.; Kanehisa, H.; Kuno, S.; Nishijima, T.; Fukunaga, T. Validity of ultrasonograph muscle thickness measurements for estimating muscle volume of knee extensors in humans. Eur. J. Appl. Physiol. 2001, 86, 203–208. [Google Scholar] [CrossRef] [PubMed]
- Kanehisa, H.; Ito, M.; Kawakami, Y.; Fukunaga, T.; Miyatani, M. The accuracy of volume estimates using ultrasound muscle thickness measurements in different muscle groups. Eur. J. Appl. Physiol. 2004, 91, 264–272. [Google Scholar] [CrossRef]
- Menzel, H.-J.; Chagas, M.H.; Szmuchrowski, L.A.; Araujo, S.R.; de Andrade, A.G.; de Jesus-Moraleida, F.R. Analysis of Lower Limb Asymmetries by Isokinetic and Vertical Jump Tests in Soccer Players. J. Strength Cond. Res. 2013, 27, 1370–1377. [Google Scholar] [CrossRef]
- Latash, M.L.; Zatsiorsky, V. Biomechanics and Motor Control: Defining Central Concepts; Academic Press: Cambridge, MA, USA, 2015. [Google Scholar]
- Cicchetti, D.V. Guidelines, criteria, and rules of thumb for evaluating normed and standardized assessment instruments in psychology. Psychol. Assess. 1994, 6, 284. [Google Scholar] [CrossRef]
- Mchugh, M.P.; Magnusson, S.P.; Gleim, G.W.; Nicholas, J.A. Viscoelastic stress relaxation in human skeletal muscle. Med. Sci. Sports Exerc. 1992, 24, 1375–1382. [Google Scholar] [CrossRef]
- Rodacki, A.L.; Fowler, N.E.; Bennett, S.J. Multi-segment coordination: Fatigue effects. Med. Sci. Sports Exerc. 2001, 33, 1157–1167. [Google Scholar] [CrossRef] [PubMed]
- Chauhan, B.; Hamzeh, M.A.; Cuesta-Vargas, A.I. Prediction of muscular architecture of the rectus femoris and vastus lateralis from EMG during isometric contractions in soccer players. SpringerPlus 2013, 2, 548. [Google Scholar] [CrossRef]
- Yurt, Y.; Yakut, Y.; Sener, G. AB1106 Validity and reliability of turkish version of self estimated functional inability because of pain (SEFIP) questionnaire and determination of pain profile in a turkish folk dancer group. Ann. Rheum. Dis. 2013, 71, 701. [Google Scholar] [CrossRef]
- Miletic, D.; Sekulic, D.; Ostojic, L. Body physique and prior training experience as determinants of SEFIP score for university dancers. Med. Probl. Perform. Artist. 2007, 22, 110–115. [Google Scholar] [CrossRef]
- McCracken, L.M.; Dhingra, L. A short version of the pain anxiety symptoms scale (PASS-20): Preliminary development and validity. Pain Res. Manag. 2002, 7, 45–50. [Google Scholar] [CrossRef] [PubMed]
- McCracken, L.M. Pain Anxiety Symptoms Scale (PASS) and short version PASS-20. In Encyclopedia of Behavioral Medicine; Springer: New York, NY, USA, 2013; pp. 1423–1424. [Google Scholar]
- Manning, J.T.; Gage, A.R.; Diver, M.J.; Scutt, D.; Fraser, W.D. Short-term changes in asymmetry and hormones in men. Evol. Hum. Behav. 2002, 23, 95–102. [Google Scholar] [CrossRef]
- Abt, J.P.; Sell, T.C.; Laudner, K.G.; McCrory, J.L.; Loucks, T.L.; Berga, S.L.; Lephart, S.M. Neuromuscular and biomechanical characteristics do not vary across the menstrual cycle. Knee Surg. Sports Traumatol. Arthrosc. 2007, 15, 901–907. [Google Scholar] [CrossRef] [PubMed]
- Frisch, R.E.; Wyshak, G.; Vincent, L. Delayed Menarche and Amenorrhea in Ballet Dancers. N. Engl. J. Med. 1980, 303, 17–19. [Google Scholar] [CrossRef] [PubMed]
- Warren, M.P.; Brooks-Gunn, J.; Fox, R.P.; Holderness, C.C.; Hyle, E.P.; Hamilton, W.G. Osteopenia in exercise-associated amenorrhea using ballet dancers as a model: A longitudinal study. J. Clin. Endocrinol. Metab. 2002, 87, 3162–3168. [Google Scholar] [CrossRef]
- Warren, M.P.; Brooks-Gunn, J.; Fox, R.P.; Holderness, C.C.; Hyle, E.P.; Hamilton, W.G.; Hamilton, L. Persistent osteopenia in ballet dancers with amenorrhea and delayed menarche despite hormone therapy: A longitudinal study. Fertil. Steril. 2003, 80, 398–404. [Google Scholar] [CrossRef] [PubMed]
- Brooks-Gunn, J.; Warren, M.P.; Hamilton, L.H. The relation of eating problems and amenorrhea in ballet dancers. Med. Sci. Sports Exerc. 1987, 19, 41–44. [Google Scholar] [CrossRef]
- Carson, T.L.; Hazzard, V.M.; Finn, E.; Lipson, S.K. Participation in varsity sports, dance, and Greek life associated with menstrual disturbance in a national sample of female college students. J. Am. Coll. Health 2022, 70, 2365–2372. [Google Scholar] [CrossRef]
- Witkoś, J.; Wróbel, P. Menstrual disorders in amateur dancers. BMC Women’s Health 2019, 19, 87. [Google Scholar] [CrossRef]
- Gupta, D.S.; Jadhav, N.A.; Kanase, S.B. Effect of Diet, Physical Activity, and Psychosocial Factors, on Menstrual Cycle Abnormalities in College Students of Karad, Maharashtra, India. J. Evol. Med. Dent. Sci. 2021, 10, 1048–1054. [Google Scholar] [CrossRef]
- Green, S.A.; Graham, B.M. Symptom fluctuation over the menstrual cycle in anxiety disorders, PTSD, and OCD: A systematic review. Arch. Women’s Ment. Health 2021, 25, 1–15. [Google Scholar]
- Schliep, K.C.; Mumford, S.L.; Vladutiu, C.J.; Ahrens, K.A.; Perkins, N.J.; Sjaarda, L.A.; Kissell, K.A.; Prasad, A.; Wactawski-Wende, J.; Schisterman, E.F. Perceived stress, reproductive hormones, and ovulatory function: A prospective cohort study. Epidemiology 2015, 26, 177. [Google Scholar] [CrossRef]
- Schmalenberger, K.M.; Tauseef, H.A.; Barone, J.C.; Owens, S.A.; Lieberman, L.; Jarczok, M.N.; Girdler, S.S.; Kiesner, J.; Ditzen, B.; Eisenlohr-Moul, T.A. How to study the menstrual cycle: Practical tools and recommendations. Psychoneuroendocrinology 2020, 123, 104895. [Google Scholar] [CrossRef]
- Sarwar, R.; Niclos, B.B.; Rutherford, O.M. Changes in muscle strength, relaxation rate and fatiguability during the human menstrual cycle. J. Physiol. 1996, 493, 267–272. [Google Scholar] [CrossRef]
- Sherman, B.M.; Korenman, S.G. Hormonal characteristics of the human menstrual cycle throughout reproductive life. J. Clin. Investig. 1975, 55, 699–706. [Google Scholar] [CrossRef]
- Sherman, B.M.; West, J.H.; Korenman, S.G. The menopausal transition: Analysis of LH, FSH, estradiol, and progesterone concentrations during menstrual cycles of older women. J. Clin. Endocrinol. Metab. 1976, 42, 629–636. [Google Scholar] [CrossRef]
- Van Goozen, S.H.; Wiegant, V.M.; Endert, E.; Helmond, F.A.; Van de Poll, N.E. Psychoendocrinological assessment of the menstrual cycle: The relationship between hormones, sexuality, and mood. Arch. Sex. Behav. 1997, 26, 359–382. [Google Scholar] [CrossRef]
- Wojtys, E.M.; Huston, L.J.; Boynton, M.D.; Spindler, K.P.; Lindenfeld, T.N. The effect of the menstrual cycle on anterior cruciate ligament injuries in women as determined by hormone levels. Am. J. Sports Med. 2002, 30, 182–188. [Google Scholar] [CrossRef]
- Falk, R.T.; Xu, X.; Keefer, L.; Veenstra, T.D.; Ziegler, R.G. A liquid chromatography-mass spectrometry method for the simultaneous measurement of 15 urinary estrogens and estrogen metabolites: Assay reproducibility and interindividual variability. Cancer Epidemiol. Biomark. Prev. 2008, 17, 3411–3418. [Google Scholar] [CrossRef]
- Marshall, J. Thermal Changes in the Normal Menstrual Cycle. BMJ 1963, 1, 102–104. [Google Scholar] [CrossRef]
- Horvath, S.M.; Drinkwater, B.L. Thermoregulation and the menstrual cycle. Aviat. Space Environ. Med. 1982, 53, 790–794. [Google Scholar]
- Bauman, J.E. Basal body temperature: Unreliable method of ovulation detection. Fertil. Steril. 1981, 36, 729–733. [Google Scholar] [CrossRef]
- Bull, J.R.; Rowland, S.P.; Scherwitzl, E.B.; Scherwitzl, R.; Danielsson, K.G.; Harper, J. Real-world menstrual cycle characteristics of more than 600,000 menstrual cycles. NPJ Digit. Med. 2019, 2, 83. [Google Scholar] [CrossRef]
- Treloar, A.E.; Boynton, R.E.; Behn, B.G.; Brown, B.W. Variation of the human menstrual cycle through reproductive life. Int. J. Fertil. 1967, 12 Pt 2, 77–126. [Google Scholar] [CrossRef]
- Shea, A.A.; Vitzthum, V.J. The extent and causes of natural variation in menstrual cycles: Integrating empirically-based models of ovarian cycling into research on women’s health. Drug Discov. Today Dis. Model. 2020, 32, 41–49. [Google Scholar] [CrossRef]
- Soria-Contreras, D.C.; Perng, W.; Rifas-Shiman, S.L.; Hivert, M.; Chavarro, J.E.; Oken, E. Menstrual cycle length and adverse pregnancy outcomes among women in Project Viva. Paediatr. Périnat. Epidemiol. 2022, 36, 347–355. [Google Scholar] [CrossRef]
- Li, H.; Gibson, E.A.; Jukic, A.M.Z.; Baird, D.D.; Wilcox, A.J.; Curry, C.L.; Fischer-Colbrie, T.; Onnela, J.-P.; Williams, M.A.; Hauser, R.; et al. Variation in menstrual cycle length by age, race/ethnicity, and body mass index in a large digital cohort of women in the US. medRxiv 2022. [Google Scholar] [CrossRef]
- Harlow, S.D.; Ephross, S.A. Epidemiology of menstruation and its relevance to women’s health. Epidemiol. Rev. 1995, 17, 265–286. [Google Scholar] [CrossRef]
- Sherman, B.M.; Korenman, S.G. Measurement of plasma LH, FSH, estradiol and progesterone in disorders of the human menstrual cycle: The short luteal phase. J. Clin. Endocrinol. Metab. 1974, 38, 89–93. [Google Scholar] [CrossRef]
- Nielsen, M.S.; Barton, S.D.; Hatasaka, H.H.; Stanford, J.B. Comparison of several one-step home urinary luteinizing hormone detection test kits to OvuQuick®. Fertil. Steril. 2001, 76, 384–387. [Google Scholar] [CrossRef]
- Su, H.W.; Yi, Y.C.; Wei, T.Y.; Chang, T.C.; Cheng, C.M. Detection of ovulation, a review of currently available methods. Bioeng. Transl. Med. 2017, 2, 238–246. [Google Scholar] [CrossRef]
- Quagliarello, J.; Arny, M. Inaccuracy of basal body temperature charts in predicting urinary luteinizing hormone surges. Fertil. Steril. 1986, 45, 334–337. [Google Scholar] [CrossRef]
- Lynch, K.E.; Mumford, S.L.; Schliep, K.C.; Whitcomb, B.W.; Zarek, S.M.; Pollack, A.Z.; Bertone-Johnson, E.R.; Danaher, M.; Wactawski-Wende, J.; Gaskins, A.J.; et al. Assessment of anovulation in eumenorrheic women: Comparison of ovulation detection algorithms. Fertil. Steril. 2014, 102, 511–518. [Google Scholar] [CrossRef]
- Juppi, H.-K.; Sipilä, S.; Cronin, N.J.; Karvinen, S.; Karppinen, J.E.; Tammelin, T.H.; Aukee, P.; Kovanen, V.; Kujala, U.M.; Laakkonen, E.K. Role of menopausal transition and physical activity in loss of lean and muscle mass: A follow-up study in middle-aged finnish women. J. Clin. Med. 2020, 9, 1588. [Google Scholar] [CrossRef]
- Phillips, S.K.; Sanderson, A.G.; Birch, K.; Bruce, S.A.; Woledge, R.C. Changes in maximal voluntary force of human adductor pollicis muscle during the menstrual cycle. J. Physiol. 1996, 496, 551–557. [Google Scholar] [CrossRef]
- Chidi-Ogbolu, N.; Baar, K. Effect of estrogen on musculoskeletal performance and injury risk. Front. Physiol. 2019, 9, 1834. [Google Scholar] [CrossRef]
- Lebrun, C.M.; McKENZIE, D.C.; Prior, J.C.; Taunton, J.E. Effects of menstrual cycle phase on athletic performance. Med. Sci. Sports Exerc. 1995, 27, 437–444. [Google Scholar] [CrossRef]
- de Souza, L.B.; Martins, K.A.; Cordeiro, M.M.; Rodrigues, Y.d.S.; Rafacho, B.P.M.; Bomfim, R.A. Do food intake and food cravings change during the menstrual cycle of young women? Rev. Bras. De Hematol. E Hemoter. 2018, 40, 686–692. [Google Scholar] [CrossRef]
- Watson, P.E.; Robinson, M.F. Variations in body-weight of young women during the menstrual cycle. Br. J. Nutr. 1965, 19, 237–248. [Google Scholar] [CrossRef] [PubMed]
- White, C.P.; Hitchcock, C.L.; Vigna, Y.M.; Prior, J.C. Fluid Retention over the Menstrual Cycle: 1-Year Data from the Prospective Ovulation Cohort. Obstet. Gynecol. Int. 2011, 2011, 138451. [Google Scholar] [CrossRef]
- Bell, D.R.; Myrick, M.P.; Blackburn, J.T.; Shultz, S.J.; Guskiewicz, K.M.; Padua, D.A. The effect of menstrual-cycle phase on hamstring extensibility and muscle stiffness. J. Sport Rehabil. 2009, 18, 553–563. [Google Scholar] [CrossRef]
- Burgess, K.; Pearson, S.; Breen, L.; Onambélé, G. Tendon structural and mechanical properties do not differ between genders in a healthy community-dwelling elderly population. J. Orthop. Res. 2009, 27, 820–825. [Google Scholar] [CrossRef] [PubMed]
- Burgess, K.E.; Pearson, S.J.; Onambélé, G.L. Patellar Tendon Properties with Fluctuating Menstrual Cycle Hormones. J. Strength Cond. Res. 2010, 24, 2088–2095. [Google Scholar] [CrossRef]
- Blagrove, R.C.; Bruinvels, G.; Pedlar, C.R. Variations in strength-related measures during the menstrual cycle in eumenorrheic women: A systematic review and meta-analysis. J. Sci. Med. Sport 2020, 23, 1220–1227. [Google Scholar] [CrossRef]
- Wojtys, E.M.; Huston, L.J.; Lindenfeld, T.N.; Hewett, T.E.; Greenfield, M.L.V.H. Association between the menstrual cycle and anterior cruciate ligament injuries in female athletes. Am. J. Sports Med. 1998, 26, 614–619. [Google Scholar] [CrossRef]
- Chaudhari, A.M.W.; Lindenfeld, T.N.; Andriacchi, T.P.; Hewett, T.E.; Riccobene, J.; Myer, G.D.; Noyes, F.R. Knee and Hip Loading Patterns at Different Phases in the Menstrual Cycle. Am. J. Sports Med. 2007, 35, 793–800. [Google Scholar] [CrossRef]
- Syrop, C.H.; Hammond, M.G. Diurnal variations in midluteal serum progesterone measurements. Fertil. Steril. 1987, 47, 67–70. [Google Scholar] [CrossRef] [PubMed]
- Keizer, H.A.; Rogol, A.D. Physical Exercise and Menstrual Cycle Alterations. Sports Med. 1990, 10, 218–235. [Google Scholar] [CrossRef]
- Jurkowski, J.E.; Jones, N.L.; Walker, C.; Younglai, E.V.; Sutton, J.R.; Horton, T.J.; Miller, E.K.; Bourret, K.; Glueck, D.; Tench, K.; et al. Ovarian hormonal responses to exercise. J. Appl. Physiol. 1978, 44, 109–114. [Google Scholar] [CrossRef] [PubMed]
- Zvolensky, M.J.; Goodie, J.L.; McNeil, D.W.; Sperry, J.A.; Sorrell, J.T. Anxiety sensitivity in the prediction of pain-related fear and anxiety in a heterogeneous chronic pain population. Behav. Res. Ther. 2001, 39, 683–696. [Google Scholar] [CrossRef] [PubMed]
- Morishita, K.; Karasuno, H.; Yokoi, Y.; Morozumi, K.; Ogihara, H.; Ito, T.; Hanaoka, M.; Fujiwara, T.; Fujimoto, T.; Abe, K. Effects of Therapeutic Ultrasound on Range of Motion and Stretch Pain. J. Phys. Ther. Sci. 2014, 26, 711–715. [Google Scholar] [CrossRef] [PubMed]
- Kowalczyk, W.J.; Evans, S.M.; Bisaga, A.M.; Sullivan, M.A.; Comer, S.D. Sex Differences and Hormonal Influences on Response to Cold Pressor Pain in Humans. J. Pain 2006, 7, 151–160. [Google Scholar] [CrossRef]
- Dragoo, J.L.; Castillo, T.N.; Braun, H.J.; Ridley, B.A.; Kennedy, A.C.; Golish, S.R. Prospective correlation between serum relaxin concentration and anterior cruciate ligament tears among elite collegiate female athletes. Am. J. Sports Med. 2011, 39, 2175–2180. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Flexibility | Vertical Jump | Pain Mix Method | EMG | Ultrasonography | Serum, Saliva, and Whole Blood |
|---|---|---|---|---|---|
| ROMMax TorqueMax FSSROM FSStorque SMTU | Jump height Impulse GRF Forcepeak vtake-off | SEFIP PASS VAS Ice Water Test | EMGST EMGRF during CMJ and SJ and flexibility tests | CSA Length Width Fat thickness Lean thickness Semitendinosus thickness | Oestrogen Progesterone Relaxin (serum) Glucose |
| Follicular | Ovulatory | Luteal | ||||
|---|---|---|---|---|---|---|
| Age (years) | 23.5 ± 2.94 | |||||
| Height (m) | 1.63 ± 0.05 | |||||
| Body mass (kg) | 67.5 ± 16.0 | 67.6 ± 15.6 | 67.8 ± 16.0 | |||
| Fat% | 25.35 ± 4.53 | 30.3 ± 6.8 | 30.81 ± 6.03 | |||
| Lean% | 69.50 ± 6.94 | 69.7 ± 6.8 | 69.18 ± 6.03 | |||
| Estimated basal metabolic rate (j) | 6487.20 ± 636.34 | 6460.7 ± 588.1 | 6449.00 ± 696.53 | |||
| Body mass index (Kg/m2) | 25.29 ± 4.62 | 25.4 ± 4.5 | 25.35 ± 4.53 | |||
| Fasted glucose (mmol/L) | 5.80 ± 2.97 | 6.06 ± 3.61 | 5.04 ± 1.16 | |||
| Oestrogen (pg/mL) | 108.7 ± 46.4 | 199.28 ± 157.4 | 161.4 ± 177.3 | |||
| Progesterone (ng/mL) | 8.8 ± 2.6 | 9.3 ± 3.0 | 10.5 ± 2.1 | |||
| Relaxin (pg/mL) | 4.6 ± 1.3 | 0.7 ± 0.4 | 4.9 ± 6.6 | |||
| Hips circumference (cm) | 98.2 ± 10.6 | 98.8 ± 10.1 | 100.9 ± 6.1 | |||
| Waist circumference (cm) | 79.7 ± 16.9 | 78.8 ± 16.6 | 77.5 ± 15.3 | |||
| Dominant | Non-dominant | Dominant | Non-dominant | Dominant | Non-dominant | |
| Calf limb circumference (cm) | 36.72 ± 4.06 | 36.86 ± 3.67 | 37.11 ± 6.40 | 37.11 ± 0.39 | 36.22 ± 7.84 | 36.05 ± 7.84 |
| Thigh circumference (cm) | 53.31 ± 3.30 | 53.37 ± 3.75 | 51.72 ± 6.40 | 51.54 ±6.61 | 51.31 ± 6.17 | 51.31± 5.96 |
| ROMMax (°) | 135.7 ± 11 98 | 128.6 ± 13.9 | 135.6 ± 14.4 | 130.5 ± 12.8 | 136.9 ± 14.2 | 132.5 ± 39.7 |
| TorqueMax (Nm) | 121.3 ± 37.3 | 134.3 ± 40.0 | 129.9 ± 40.5 | 141.7 ± 36.9 | 134.7 ± 39.9 | 136.5 ± 39.7 |
| FSSROM (°) | 102.2 ± 15.8 | 94.9 ± 13.9 | 99.0 ± 10.5 | 96.7 ± 9.8 | 98.9 ± 9.5 | 91.6 ± 11.1 |
| FSStorque (Nm) | 32.0 ± 13.3 | 49.2 ± 31.5 | 46.4 ± 21.6 | 55.3 ± 29.6 | 46.7 ± 29.4 | 34.5 ± 25.9 |
| SMTU (Nm/°) | 2.9 ± 1.0 | 3.3 ± 0.9 | 3.1 ± 1.3 | 3.4 ± 0.9 | 3.2 ± 0.8 | 3.3 ± 1.3 |
| Elastic potential energy (Nm°) | 307.3 ± 105.3 | 302.2 ± 90.6 | 334.1 ± 122.6 | 342.6 ± 111.0 | 325.9 ± 93.7 | 341.9 ± 154.4 |
| ST muscle length (cm) | 39.2 ± 2.6 | 39.3 ± 2.5 | 39.3 ± 1.9 | 39.5 ± 2.0 | 39.6 ± 1.9 | 39.3 ± 1.7 |
| ST muscle width (cm) | 3.8 ± 0.5 | 3.7 ± 0.6 | 3.8 ± 0.8 | 3.82 ± 0.6 | 3.9 ± 0.9 | 4.1 ± 1.1 |
| ST CSA (mm2) | 5.2 ± 1.4 | 5.3 ± 1.2 | 5.6 ± 1.8 | 5.4 ± 2.0 | 5.4 ± 1.8 | 5.2 ± 1.8 |
| ST fat thickness (mm) | 1.3 ± 0.6 | 1.4 ± 0.6 | 1.4 ± 0.5 | 1.4 ± 0.5 | 1.13 ± 0.4 | 1.2 ± 0.5 |
| ST muscle lean (mm) | 5.2 ± 0.6 | 5.3 ± 0.8 | 5.4 ± 0.4 | 5.4 ± 0.3 | 5.3 ± 0.6 | 5.2 ± 0.8 |
| CMJ impulse (Ns) | 85.7 ± 32.9 | 64.0 ± 26.3 | 70.9 ± 23.8 | 76.9 ± 15.5 | 73.0 ± 15.4 | 74.5 ± 22.9 |
| CMJ ground reaction force (N) | 349.0 ± 97.3 | 356.1 ± 71.3 | 360.3 ± 95.6 | 350.4 ± 73.8 | 376.9 ± 95.7 | 332.5 ± 64.6 |
| CMJ peakforce (N) | 412.7 ± 107.7 | 364.0 ± 83.3 | 404.6 ± 73.3 | 385.8 ± 72.3 | 388.5 ± 64.1 | 402.4 ± 72.0 |
| CMJ vtake-off (m/s) | 2.1 ± 0.3 | 2.1 ± 0.2 | 2.0 ± 0.2 | |||
| CMJ height (m) | 0.22 ± 0.1 | 0.22 ± 0.1 | 0.21 ± 0.1 | |||
| SJ impulse (Ns) | 122.3 ± 52.3 | 106.3 ± 36.7 | 114.8 ± 40.16 | |||
| SJ ground reaction force (N) | 363.1 ± 102.5 | 343.7 ± 62.5 | 357.8 ± 94.1 | 122.6 ± 31.9 | 123.6 ± 68.0 | 121.1 ± 36.9 |
| SJ peakforce (N) | 426.9 ± 123.8 | 386.6 ± 105.1 | 429.4 ± 127.6 | 354.0 ± 74.6 | 372.2 ± 94.8 | 336.2 ± 65.1 |
| SJ vtake-off (m/s) | 2.0 ± 0.2 | 1.9 ± 0.2 | 2.0 ± 0.2 | 402.5 ± 96.9 | 403.5 ± 76.8 | 393.3 ± 90.8 |
| SJ height (m) | 0.20 ± 0.1 | 0.20 ± 0.1 | 0.22 ± 0.1 | |||
| Oestrogen | Progesterone | Relaxin | ||
|---|---|---|---|---|
| Significant correlations Luteal/Follicular | Muscle length | p = 0.008 r = −0.560 ** | p = 0.022 r = 0.587 * | n.s. |
| Muscle CSA | p = 0.044 r = −0.413 * | n.s. | n.s. | |
| Fat thickness | p = 0.022 r = −0.480 * | p = 0.044 r = 0.513 * | p = 0.007 r = 0.683 ** | |
| Lean | n.s. | n.s. | p = 0.015 r = 0.626 * | |
| CMJ EMGRF | p = 0.010 r = −0.611 * | n.s. | n.s. | |
| CMJ EMGST | p = 0.001 r = −0.926 ** | p = 0.006 r = 0.822 ** | n.s. | |
| SJ EMGRF | n.s. | n.s. | p = 0.017 r = 0.790 * | |
| SJ EMGST | n.s. | n.s. | p = 0.002 r = 0.911 ** | |
| Significant correlations Ovulatory/Follicular | Muscle length | p = 0.004 r = 0.599 ** | n.s. | p = 0.049 r = 0.460 * |
| Muscle CSA | n.s. | n.s. | p = 0.006 r = −0.646 ** | |
| Fat thickness | n.s. | n.s. | p = 0.006 r = −0.647 ** | |
| ST thickness | p = 0.001 r = 0.676 ** | p = 0.010 r = −0.612 * | p = 0.001 r = −0.872 ** | |
| Lean Muscle | n.s. | p = 0.045 r = −0.470 * | p = 0.001 r = −0.881 ** | |
| FSStorque | p = 0.020 r = 0.463 * | n.s. | p = 0.028 r = −0.485 * | |
| SMTU | n.s. | n.s. | p = 0.001 r = −0.781 ** | |
| Elastic potential Energy | n.s. | p = 0.034 r = −0.467 * | p = 0.021 r = −0.512 * | |
| CMJ ForcePeak | n.s. | n.s. | p = 0.022 r = −0.509 * | |
| CMJ Total Forcepeak | p = 0.040 r = −0.578 * | n.s. | n.s. | |
| SJ ForcePeak | p = 0.021 r = −0.459 * | n.s. | n.s. | |
| CMJ EMGRF | p = 0.021 r = 0.549 * | n.s. | n.s. | |
| SJ EMGRF | n.s. | n.s. | p = 0.007 r = 0.812 ** |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pessali-Marques, B.; Burden, A.M.; Morse, C.I.; Onambélé-Pearson, G.L. Musculoskeletal Morphology and Joint Flexibility-Associated Functional Characteristics across Three Time Points during the Menstrual Cycle in Female Contemporary Dancers. J. Funct. Morphol. Kinesiol. 2024, 9, 38. https://0-doi-org.brum.beds.ac.uk/10.3390/jfmk9010038
Pessali-Marques B, Burden AM, Morse CI, Onambélé-Pearson GL. Musculoskeletal Morphology and Joint Flexibility-Associated Functional Characteristics across Three Time Points during the Menstrual Cycle in Female Contemporary Dancers. Journal of Functional Morphology and Kinesiology. 2024; 9(1):38. https://0-doi-org.brum.beds.ac.uk/10.3390/jfmk9010038
Chicago/Turabian StylePessali-Marques, Bárbara, Adrian M. Burden, Christopher I. Morse, and Gladys L. Onambélé-Pearson. 2024. "Musculoskeletal Morphology and Joint Flexibility-Associated Functional Characteristics across Three Time Points during the Menstrual Cycle in Female Contemporary Dancers" Journal of Functional Morphology and Kinesiology 9, no. 1: 38. https://0-doi-org.brum.beds.ac.uk/10.3390/jfmk9010038