
Molecular Epidemiology of Human Papillomaviruses, Neisseria gonorrhoeae, Chlamydia trachomatis and Mycoplasma genitalium among Female Sex Workers in Burkina Faso: Prevalence, Coinfections and Drug Resistance Genes

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Setting of the Survey
2.2. Study Variables
2.3. Sampling
2.4. Molecular Characterization
2.4.1. DNA Extraction
2.4.2. Real-Time PCR Amplification for the Urogenital STI Pathogens
2.4.3. Identification of Resistance Genes by Classical PCR
2.4.4. Data Analyses
3. Results
HIV Status of Patients
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Burns, K.; Keating, P.; Free, C. A systematic review of randomised control trials of sexual health interventions delivered by mobile technologies. BMC Public Health 2016, 16, 778. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Report on Global Sexually Transmitted Infection Surveillance; WHO/OMS: Geneva, Switzerland, 2018. [Google Scholar]
- World Health Organization. Stratégie Mondiale du Secteur de la Santé Contre Les Infections Sexuellement Transmissibles 2016–2021; WHO/OMS: Geneva, Switzerland, 2016. [Google Scholar]
- Rowley, J.; Vander, H.S.; Korenromp, E.; Low, N.; Unemo, M.; Abu-Raddad, L.J.; Chico, R.M.; Smolak, A.; Newman, L.; Gottlieb, S.; et al. Chlamydia, gonorrhoea, trichomoniasis and syphilis: Global prevalence and incidence estimates, 2016. Bull. World Health Organ. 2019, 97, 548. [Google Scholar] [CrossRef] [PubMed]
- Woodhall, S.C.; Wills, G.S.; Horner, P.J.; Craig, R.; Mindell, J.S.; Murphy, G.; McClure, M.O.; Soldan, K.; Nardone, A.; Johnson, A.M. Chlamydia trachomatis Pgp3 Antibody Population Seroprevalence before and during an Era of Widespread Opportunistic Chlamydia Screening in England (1994–2012). PLoS ONE 2017, 12, e0152810. [Google Scholar] [CrossRef] [PubMed]
- Essome, M.C.; Nsawir, B.J.; Nana, R.D.; Molu, P.; Mohamadou, M. Sero-epidemiological study of three sexually transmitted infections: Chlamydia trachomatis, Hepatitis, B.; Syphilis. A case study conducted at the Nkoldongo District Hospital in Yaoundé. Pan Afr. Med. J. 2016, 25, 244. [Google Scholar] [PubMed]
- Traore, I.M.A.; Zohoncon, T.M.; Ndo, O.; Djigma, F.W.; Obiri Yeboah, D.; Compaore, T.R.; Guigma, S.P.; Yonli, A.T.; Traore, G.; Ouedraogo, P.; et al. Oncogenic Human Papillomavirus Infection and Genotype Characterization among Women in Orodara, Western Burkina Faso. Pak. J. Biol. Sci. 2016, 19, 306–311. [Google Scholar] [CrossRef] [PubMed]
- Nadembega, C.W.; Djigma, F.; Ouermi, D.; Karou, S.D.; Simpore, J. Prevalence of vaginal infection in 15 to 24 years women in Ouagadougou, Burkina Faso. J. Appl. Pharm. Sci. 2017, 7, 209–213. [Google Scholar] [CrossRef] [Green Version]
- Krings, A.; Dunyo, P.; Pesic, A.; Tetteh, S.; Hansen, B.; Gedzah, I. Characterization of Human Papillomavirus prevalence and risk factors to guide cervical cancer screening in the North Tongu District, Ghana. PLoS ONE 2019, 14, e0218762. [Google Scholar] [CrossRef] [PubMed]
- Okunade, K.S.; Nwogu, C.M.; Oluwole, A.A.; Anorlu, R.I. Prevalence and risk factors for genital high-risk human papillomavirus infection among women attending the out-patient clinics of a university teaching hospital in Lagos, Nigeria. Pan Afr. Med. J. 2017, 28, 227. [Google Scholar] [CrossRef] [PubMed]
- Longo, J.D.D.; Simaleko, M.M.; Diemer, H.S.C.; Grésenguet, G.; Brücker, G.; Belec, L. Risk factors for HIV infection among female sex workers in Bangui, Central African Republic. PLoS ONE 2017, 12, e0187654. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mayer, K.; De Vries, H. HIV and sexually transmitted infections: Reconciling estranged bedfellows in the U = U and Pr EP era. J. Int. AIDS Soc. 2019, 22, e25357. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Longo, J.D.; Simaléko, M.M.; Ngbale, R.; Grésenguet, G.; Brücker, G.; Bélec, L. Spectrum of female commercial sex work in Bangui, Central African Republic. SAHARA-J J. Soc. Asp. HIV/AIDS Res. Alliance 2017, 14, 84–171. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coudray, M.S.; Madhivanan, P. Bacterial vaginosis-A brief synopsis of the literature. Eur. J. Obstet. Gynecol. Reprod. Biol. 2020, 245, 143–148. [Google Scholar] [CrossRef] [PubMed]
- Lv, P.; Zhao, F.; Xu, X.; Xu, J.; Wang, Q.; Zhao, Z. Correlation between Common Lower Genital Tract Microbes and High-Risk Human Papillomavirus Infection. Can. J. Infect. Dis. Med. Microbiol. 2019, 2019, 9678104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tovo, S.F.; Ouattara, A.K.; Zohoncon, M.T.; Obiri-Yeboah, D.; Yonli, A.T.; Djigma, W.F.; Sangaré, L.; Simporé, J. Prevalence of lower genial tract infections in women: Case of Saint Camille Hospital of Ouagadougou from 2015 to 2018. Int. J. Curr. Res. 2019, 11, 7721–7727. [Google Scholar]
- Zohoncon, T.M.; Djigma, W.F.; Ouattara, A.K.; Traore, I.M.; Ouedraogo, R.A.; Traore, E.M.; Bado, P.; Ouedraogo, T.C.; Diarra, B.; Ilboudo, M.; et al. Mapping of fourteen high-risk human papillomavirus genotypes by molecular detection in sexually active women in the West African sub-region. Int. J. Gen. Mol. Biol. 2020, 12, 11–21. [Google Scholar]
- Kubone, P.Z.; Mlisana, K.P.; Govinden, U.; Abia, A.L.K.; Essack, S.Y. Antibiotic Susceptibility and Molecular Characterization of Uropathogenic Escherichia coli Associated with Community-Acquired Urinary Tract Infections in Urban and Rural Settings in South Africa. Trop. Med. Infect. Dis. 2020, 5, 176. [Google Scholar] [CrossRef] [PubMed]
- Mètuor Dabiré, A.; Zongo, J.; Kaboré, B.; Zèba, B.; Baucher, M.; El Jaziri, M.; Simporé, J. Resistance to β-Lactamines by Gram Negative Bacteria, Producing Several Types of Enzymes, Isolated from Urines in Pediatric Center of Ouagadougou in Burkina Faso. Int. J. Microbiol. Biotech. 2018, 3, 95–98. [Google Scholar]
- Salah, F.D.; Soubeiga, S.T.; Ouattara, A.K.; Sadji, A.Y.; Metuor-Dabire, A.; Obiri-Yeboah, D.; Banla-Kere, A.; Karou, S.; Simpore, J. Distribution of quinolone resistance gene (qnr) in ESBL-producing Escherichia coli and Klebsiella spp. in Lomé, Togo. Antimicrob. Resist. Infect. Control. 2019, 8, 104. [Google Scholar] [CrossRef] [PubMed]
- Amana, M.D.; Wend-Kuni, T.; Yasmine, E.R.; Aminata, B.; Yasmine, E.; Zohoncon, T.M.; Sougué, S.; Zongo, J.K.; Simporé, J. Detection of multidrug-resistant enterobacteria simultaneously producing extended-spectrum-lactamases of the PER and GES types isolated at Saint Camille Hospital Center, Ouagadougou, Burkina Faso. Afr. J. Microbiol. Res. 2019, 13, 414–420. [Google Scholar]
- Tiemtoré, R.Y.; Mètuor-Dabiré, A.; Zohoncon, T.M.; Bangré, Y.A.; Sougue, S.; Zongo, J.; Simpore, J. First Detection of PE-Type Extended-Spectrum β-lactamases at Saint Camille Hospital Center of Ouagadougou, Burkina Faso. Int. J. Biochem. Biophys. Mol. Biol. 2019, 4, 7. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| TEM-F: 5′-ATAAAATTCTTGAAGACGAAA-3′ TEM-R: 5′-GACAGTTACCAATGCTTAATCA-3′ | bla TEM | 1000 Pb |
| CTX-MF: 5′-GTTACAATGTGTGAGAAGCAG-3′ CTX-M-R: 5′-CCGTTTCCGCTATTACAAAC-3′ | bla CTX-M | 1000 Pb |
| PER-F: 5′-ATGAATGTCATTATAAAAGC-3′ PER-R: 5′-AATTTGGGCTTAGGGCAGAA-3′ | bla PER | 925 Pb |
| QNR A-F: 5′-ATTTCTCACGCCAGGATTTG-3′ QNR A-R: 5′-GATCGGCAAAGGTTAGGTCA-3′ | bla QNR A | 846 Pb |
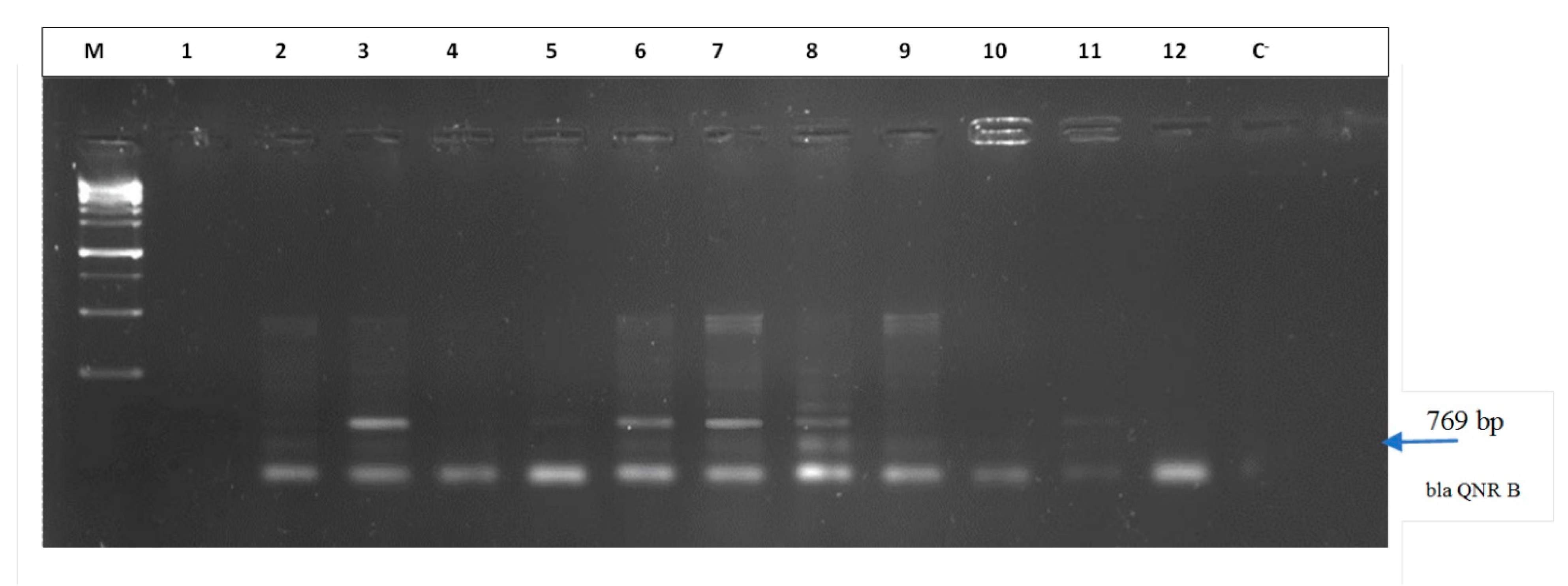
| QNR B-F: 5′-GATCGTGAAAGCCAGAAAGG-3′ QNR B-R: 5′-ACGATGCCTGGTAGTTGTCC-3′ | bla QNR B | 769 Pb |
| QNR S-F: 5′-ACGACATTCGTCAACTGCAA-3′ QNR S-R: 5′-TAAATTGGCACCCTGTAGGC-3′ | bla QNR S | 566 Pb |
| SHV-F: 5′-ATG-CGTTATATTCGCCTGTG-3′ SHV-R: 5′-TTAGCGTTGCCAGTGCTC-3′ | bla SHV | 875 Pb |
| GES-F: 5′-ATGCGCTTCATTCACGCAC-3′ GES-R: 5′-CTATTTGTCCGTGCTCAGG-3′ | bla GES | 863 Pb |
| Sociodemographic Characteristics | Positive | Negative | p Value | Positive | Negative | p Value |
|---|---|---|---|---|---|---|
| N = 56 (%) | N =126 (%) | N = 100 (%) | N = 82 (%) | |||
| Age Classes | ||||||
| ˂21 | 3 (1.65) | 16 (8.79) | 13 (7.14) | 6 (3.30) | ||
| 21–30 | 17 (9.34) | 101 (55.49) | 63 (34.62) | 55 (30.22) | ||
| >30 | 1 (0.55) | 44 (24.18) | 0.07 | 24 (13.18) | 21 (11.54) | 0.45 |
| Scholastic Level | ||||||
| Not attending school | 7 (3.85) | 29 (15.93) | 16 (8.79) | 20 (10.99) | ||
| Primary | 12 (6.60) | 29 (15.93) | 0.2 | 19 (10.44) | 22 (12.09) | 0.08 |
| Secondary & University | 37 (20.33) | 68 (37.36) | 65 (35.71) | 40 (21.98) | ||
| SEXUAL PARTNERS | ||||||
| ≤500 | 53 (29.12) | 116 (63.73) | 0.75 | 94 (51.65) | 75 (41.21) | 0.5 |
| >500 | 3 (1.65) | 10 (5.59) | 6 (3.30) | 7 (3.84) | ||
| MARITAL SITUATION | ||||||
| Unmarried | 50 (27.47) | 118 (64.83) | 0.47 | 95 (52.20) | 73 (40.11) | 0.13 |
| Married | 6 (3.30) | 8 (4.40) | 5 (2.75) | 9 (4.94) | ||
| NATIONALITIES | ||||||
| Burkinabè | 19 (10.44) | 60 (32.97) | 42 (23.08) | 37 (20.33) | ||
| Nigerian | 31 (17.03) | 49 (26.92) | 0.11 | 46 (25.28) | 34 (18.68) | 0.82 |
| Others | 6 (3.30) | 17 (9.34) | 12 (6.59) | 11 (6.04) | ||
| Totals | 56 (30.76) | 126 (69.23) | ˂0.0001 | 100 (54.94) | 82 (45.05) | NS |
| Pathogens Germs N = 182 | Positive (%) | Negative (%) | p-Value |
|---|---|---|---|
| Only one Infection | |||
| MG | 21 (11.54) | 161 (88.46) | |
| CT | 21 (11.54) | 161 (88.46) | 0.76 |
| NG | 25 (13.74) | 157 (86.26) | |
| TV | 0.00 | 182 (100) | |
| Total (at least one infection) | 56 (30.77) | 126 (69.23) | |
| Coinfections | |||
| MG/CT | 6 (3.30) | 176 (96.70) | |
| MG/NG | 2 (1.10) | 180 (98.90) | 0.20 |
| CT/NG | 4 (2.20) | 178 (97.80) | |
| MG/NG/CT | 1 (0.55) | 181 (99.45) |
| Coinfections | HPV+ N = 100 | HPV− N = 82 | p Value |
|---|---|---|---|
| NG+ | 15 (15.00%) | 10 (12.19%) | 0.74 |
| NG− | 85 (85.00%) | 72 (87.80%) | |
| CT+ | 8 (8.00%) | 13 (15.85%) | 0.16 |
| CT− | 92 (92.00%) | 69 (84.14%) | |
| MG+ | 12 (12.00%) | 9 (11.00%) | 0.83 |
| MG− | 88 (88.00%) | 73 (89.00%) | |
| NG+CT+ | 2 (2.00%) | 2 (2.43%) | 0.76 |
| NG−CT− | 98 (98.00%) | 80 (97.56%) | |
| NG+MG+ | 2 (2.00%) | 0 (0.00%) | - |
| NG−MG− | 98 (98.00%) | 82 (100.00%) | |
| CT+MG+ | 2 (2.00%) | 4 (4.87%) | 0.51 |
| CT−MG− | 98 (98.00%) | 78 (95.12%) | |
| Vaginal infections | 30 (30.00%) | 26 (31.71%) | 0.80 |
| No Vaginal infections | 70 (70.00%) | 56 (68.29%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tovo, S.F.; Zohoncon, T.M.; Dabiré, A.M.; Ilboudo, R.; Tiemtoré, R.Y.; Obiri-Yeboah, D.; Yonli, A.T.; Dovo, E.E.; Ouédraogo, R.A.; Ouattara, A.K.; et al. Molecular Epidemiology of Human Papillomaviruses, Neisseria gonorrhoeae, Chlamydia trachomatis and Mycoplasma genitalium among Female Sex Workers in Burkina Faso: Prevalence, Coinfections and Drug Resistance Genes. Trop. Med. Infect. Dis. 2021, 6, 90. https://0-doi-org.brum.beds.ac.uk/10.3390/tropicalmed6020090
Tovo SF, Zohoncon TM, Dabiré AM, Ilboudo R, Tiemtoré RY, Obiri-Yeboah D, Yonli AT, Dovo EE, Ouédraogo RA, Ouattara AK, et al. Molecular Epidemiology of Human Papillomaviruses, Neisseria gonorrhoeae, Chlamydia trachomatis and Mycoplasma genitalium among Female Sex Workers in Burkina Faso: Prevalence, Coinfections and Drug Resistance Genes. Tropical Medicine and Infectious Disease. 2021; 6(2):90. https://0-doi-org.brum.beds.ac.uk/10.3390/tropicalmed6020090
Chicago/Turabian StyleTovo, Sessi Frida, Théodora Mahoukèdè Zohoncon, Amana Metuor Dabiré, Régine Ilboudo, Rahimatou Yasmine Tiemtoré, Dorcas Obiri-Yeboah, Albert Théophane Yonli, Essi Etonam Dovo, Rogomenoma Alice Ouédraogo, Abdoul Karim Ouattara, and et al. 2021. "Molecular Epidemiology of Human Papillomaviruses, Neisseria gonorrhoeae, Chlamydia trachomatis and Mycoplasma genitalium among Female Sex Workers in Burkina Faso: Prevalence, Coinfections and Drug Resistance Genes" Tropical Medicine and Infectious Disease 6, no. 2: 90. https://0-doi-org.brum.beds.ac.uk/10.3390/tropicalmed6020090