Non-Pharmacological Interventions to Improve Chronic Disease Risk Factors and Sleep in Shift Workers: A Systematic Review and Meta-Analysis


Abstract
:1. Introduction
- (1)
- Which non-pharmacological interventions have been used to improve chronic disease risk factors and sleep in shift workers?
- (2)
- Which non-pharmacological interventions are most effective for improving chronic disease risk factors and sleep in shift workers?
2. Methods
2.1. Eligibility Citeria
2.2. Information Sources and Search Strategy
2.3. Study Selection
2.4. Data Collection Process
2.5. Risk of Bias in Individual Studies
2.6. Summary Measures
2.7. Synthesis of Results
2.8. Additional Analyses
3. Results
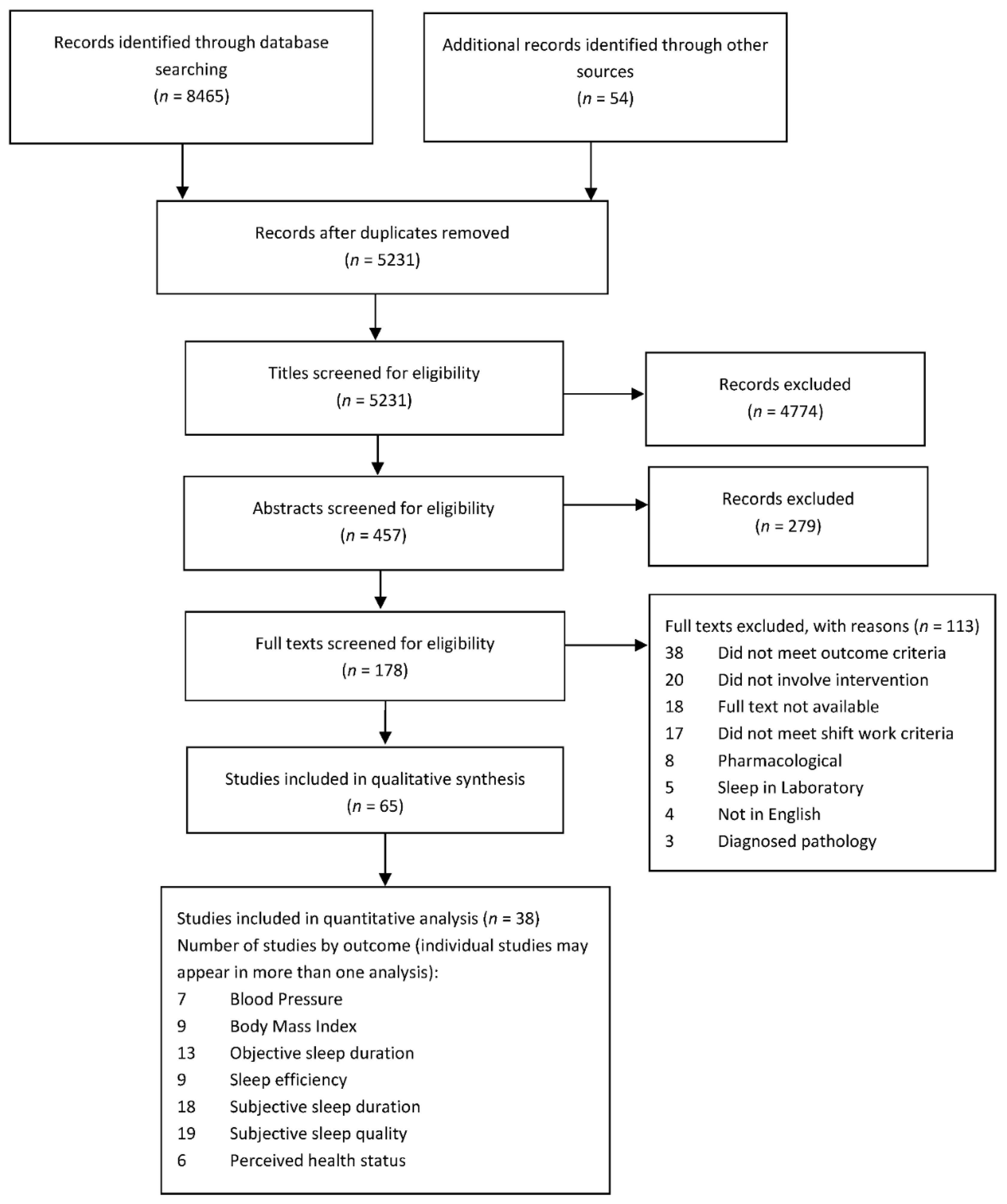
3.1. Study Selection
3.2. Study Characteristics
3.3. Risk of Bias within Studies
3.4. Participant Characteristics
3.5. Results of Individual Studies
3.5.1. Schedule Change
3.5.2. Behavioural Interventions
3.5.3. Controlled Light Exposure
3.5.4. Complementary Interventions
3.6. Synthesis of Quantitative Results
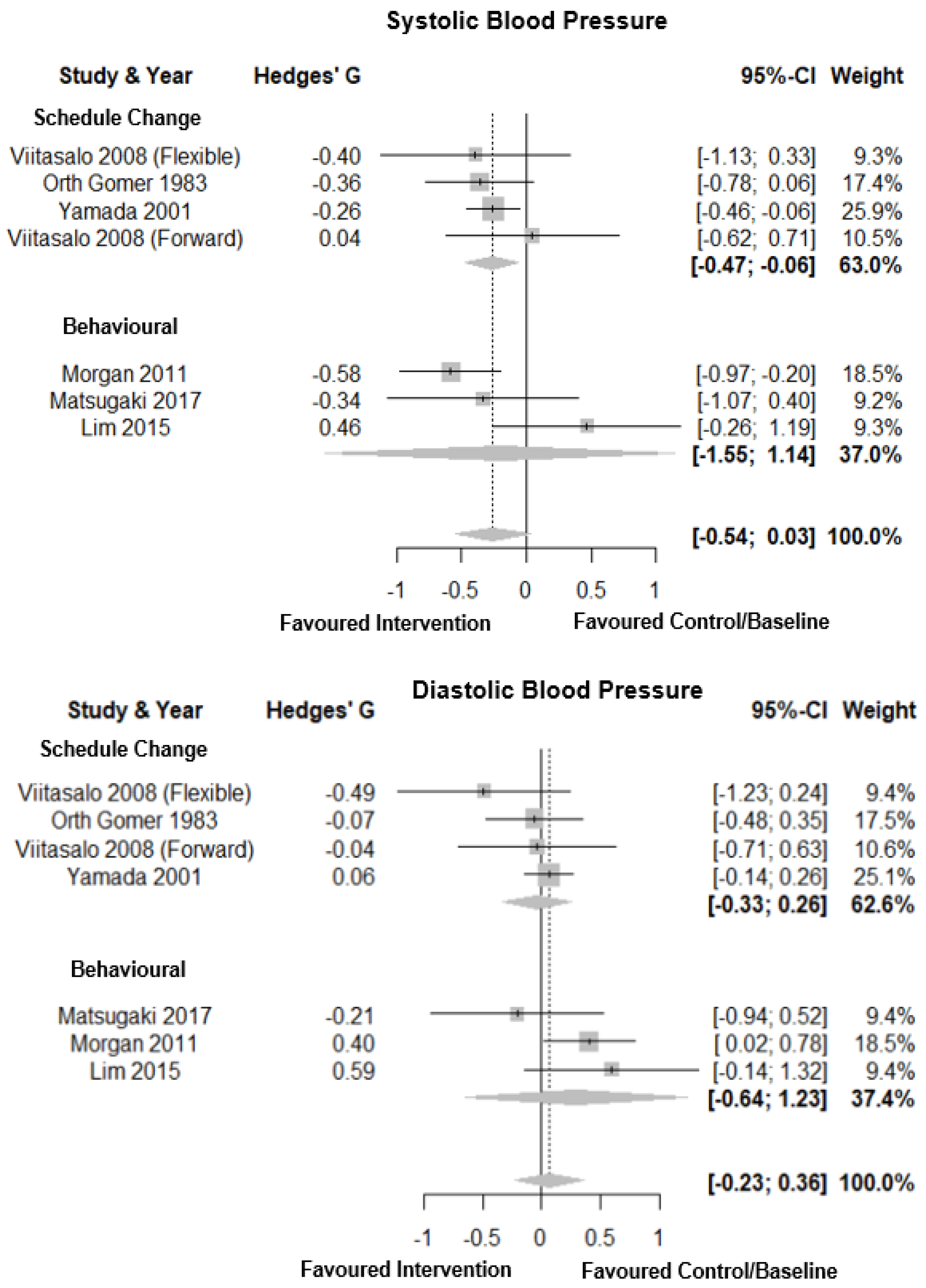
3.6.1. Blood Pressure
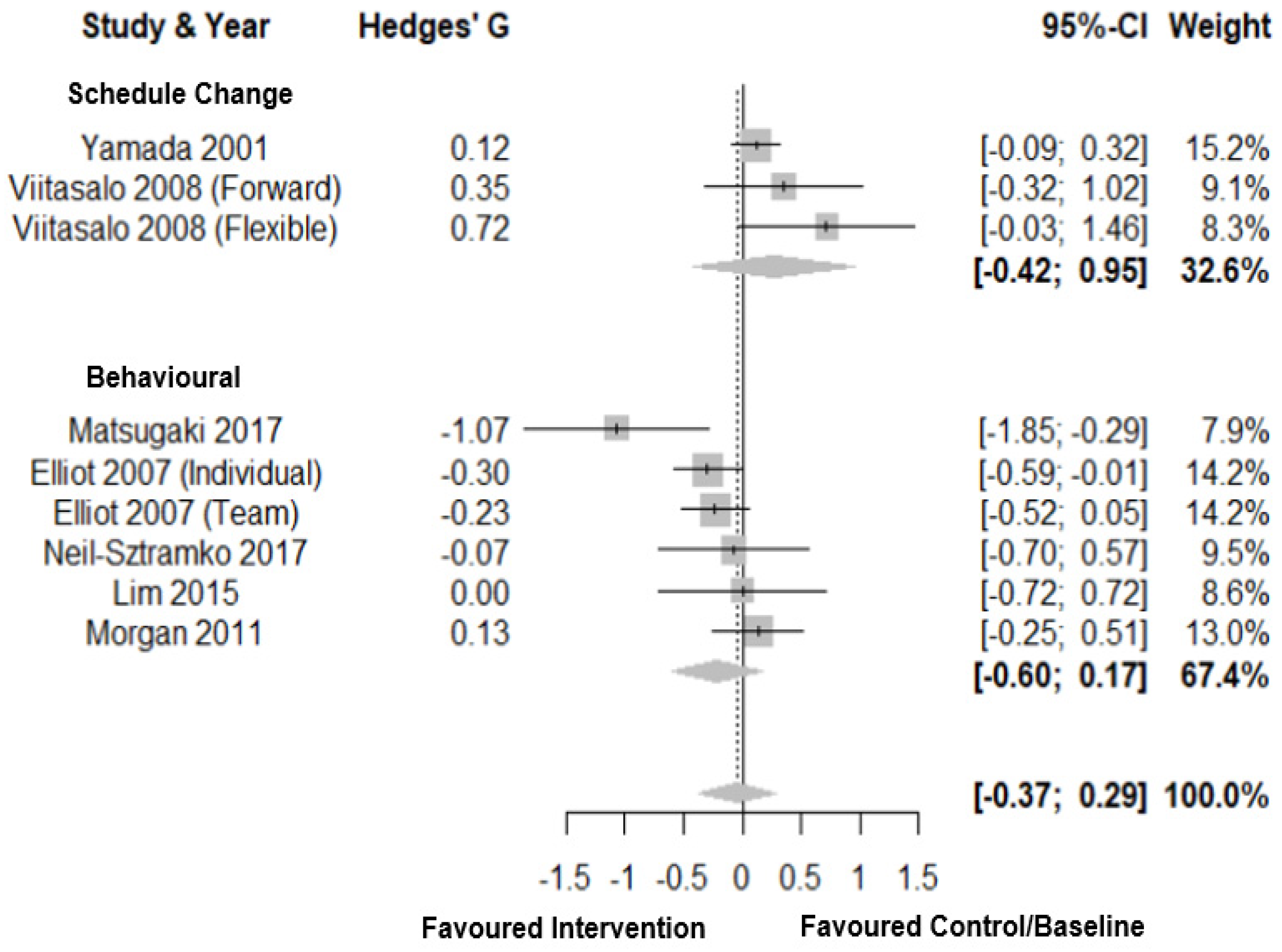
3.6.2. Body Mass Index
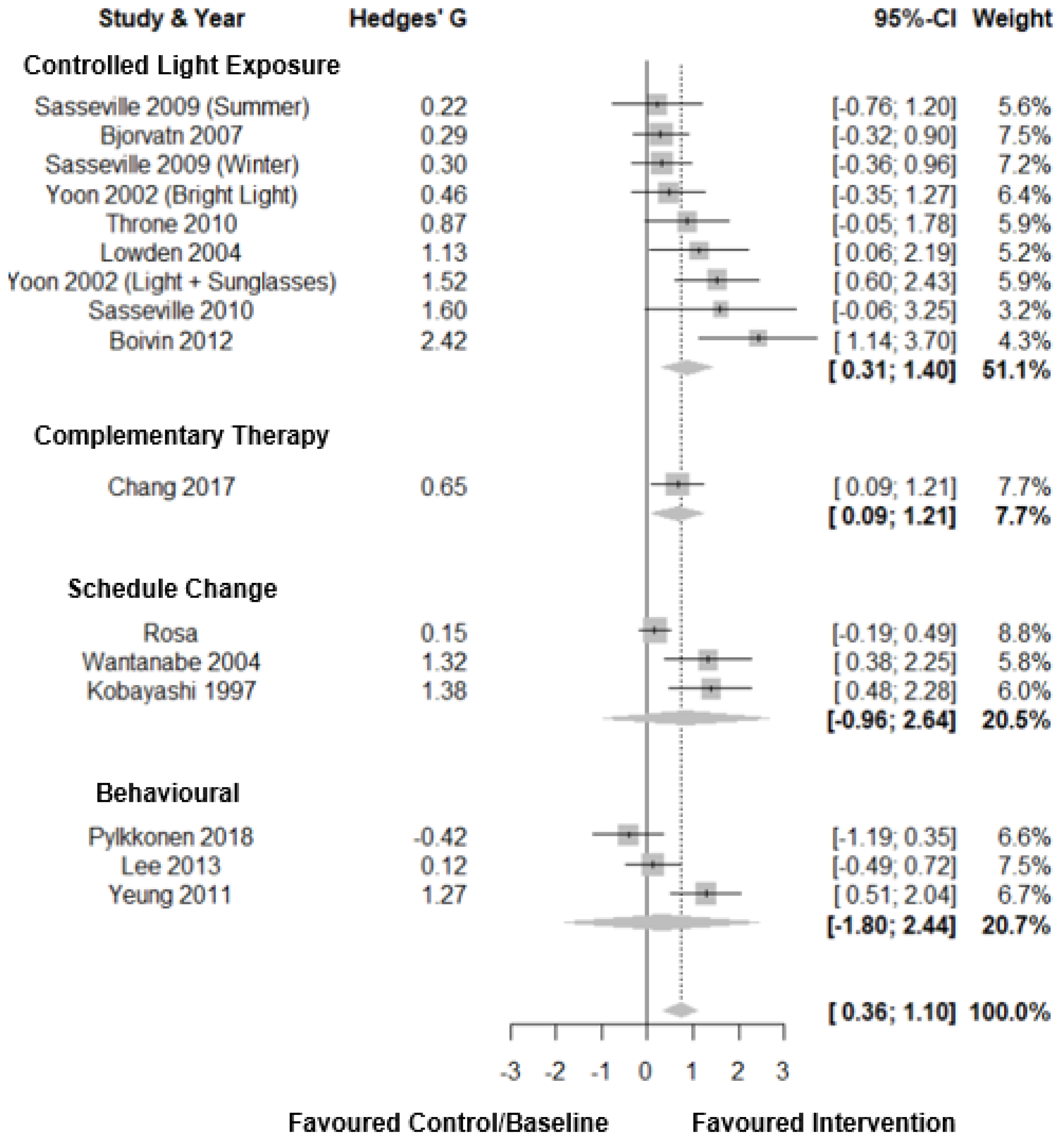
3.6.3. Objective Sleep Duration
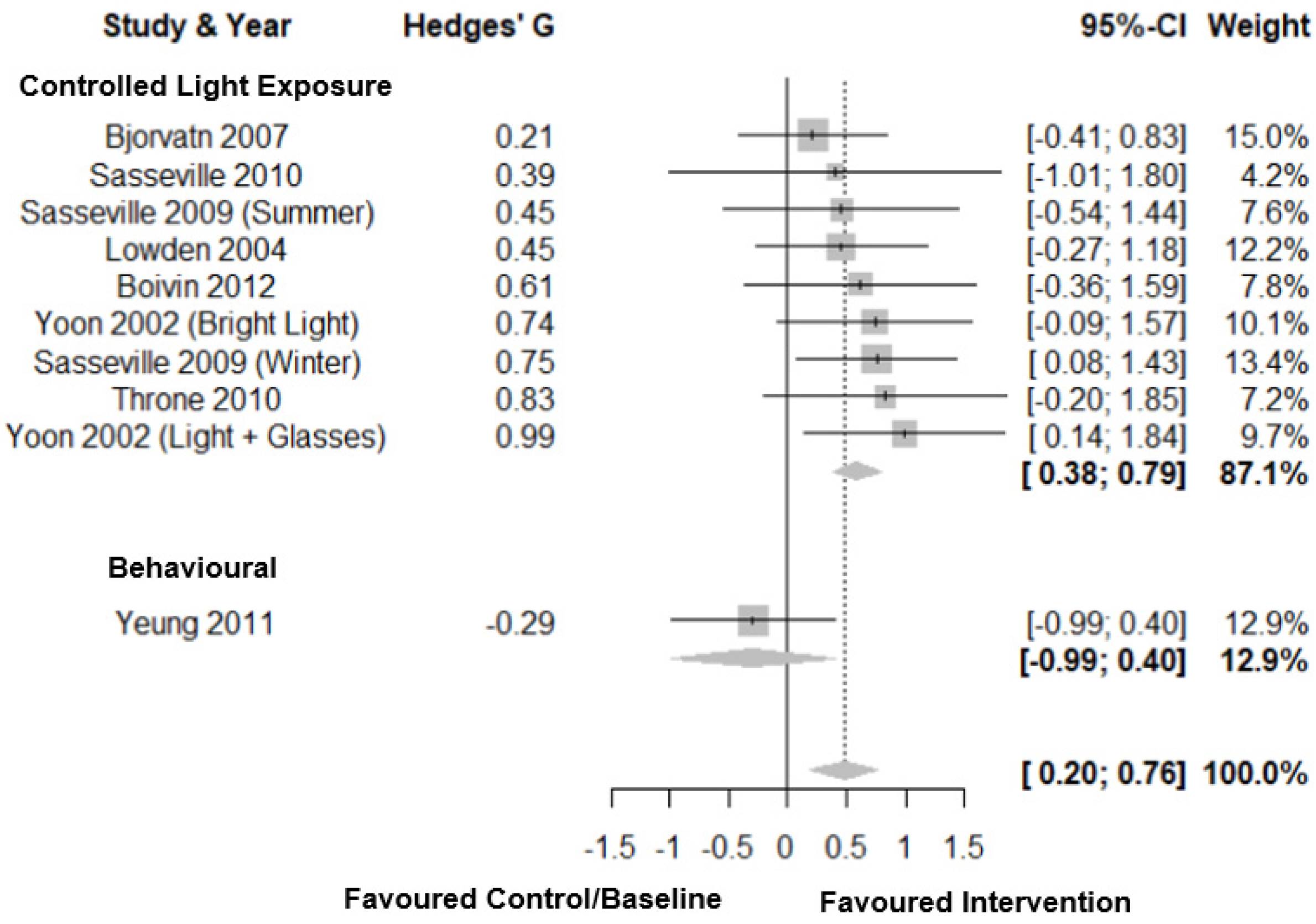
3.6.4. Sleep Efficiency
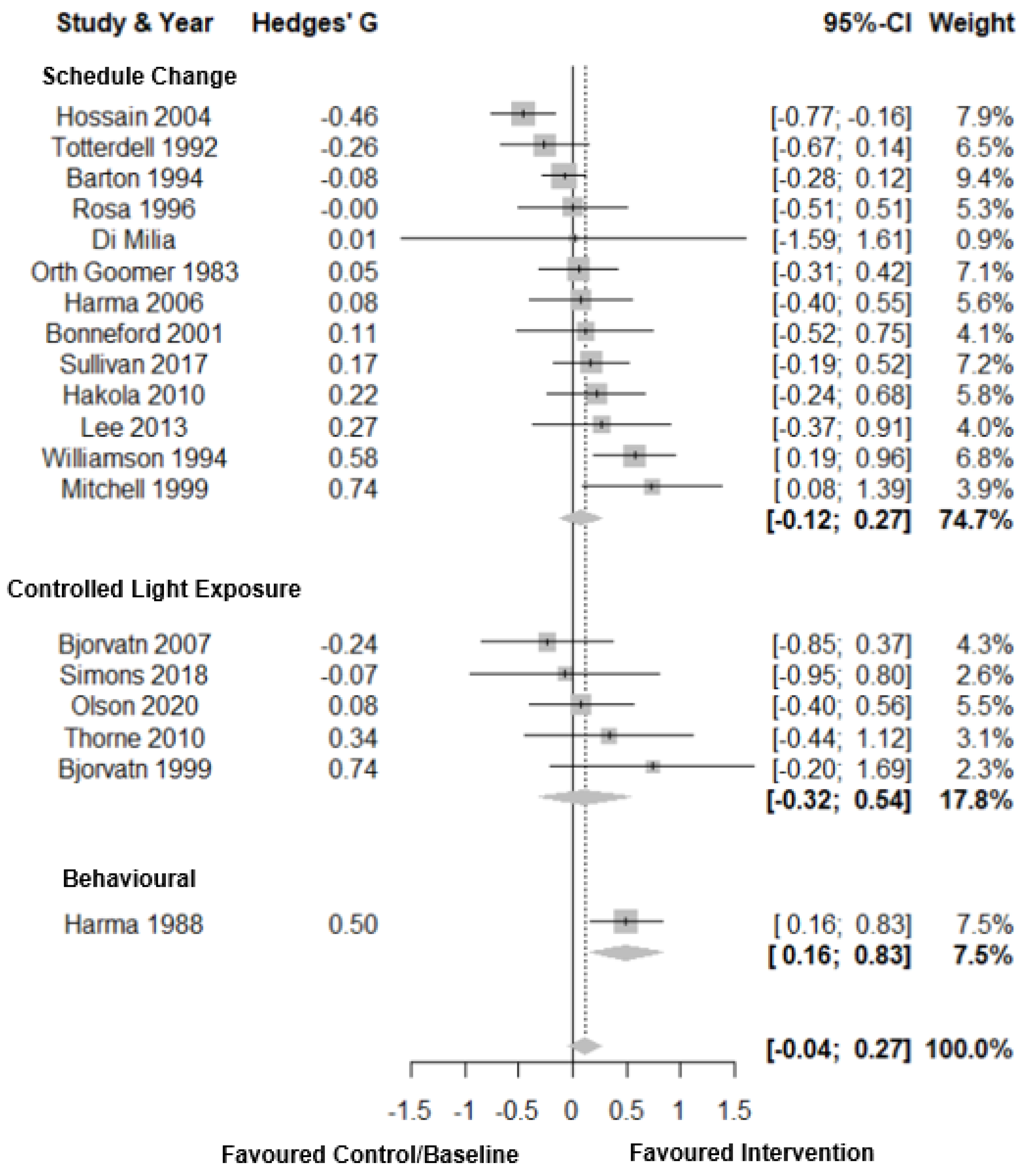
3.6.5. Subjective Sleep Duration
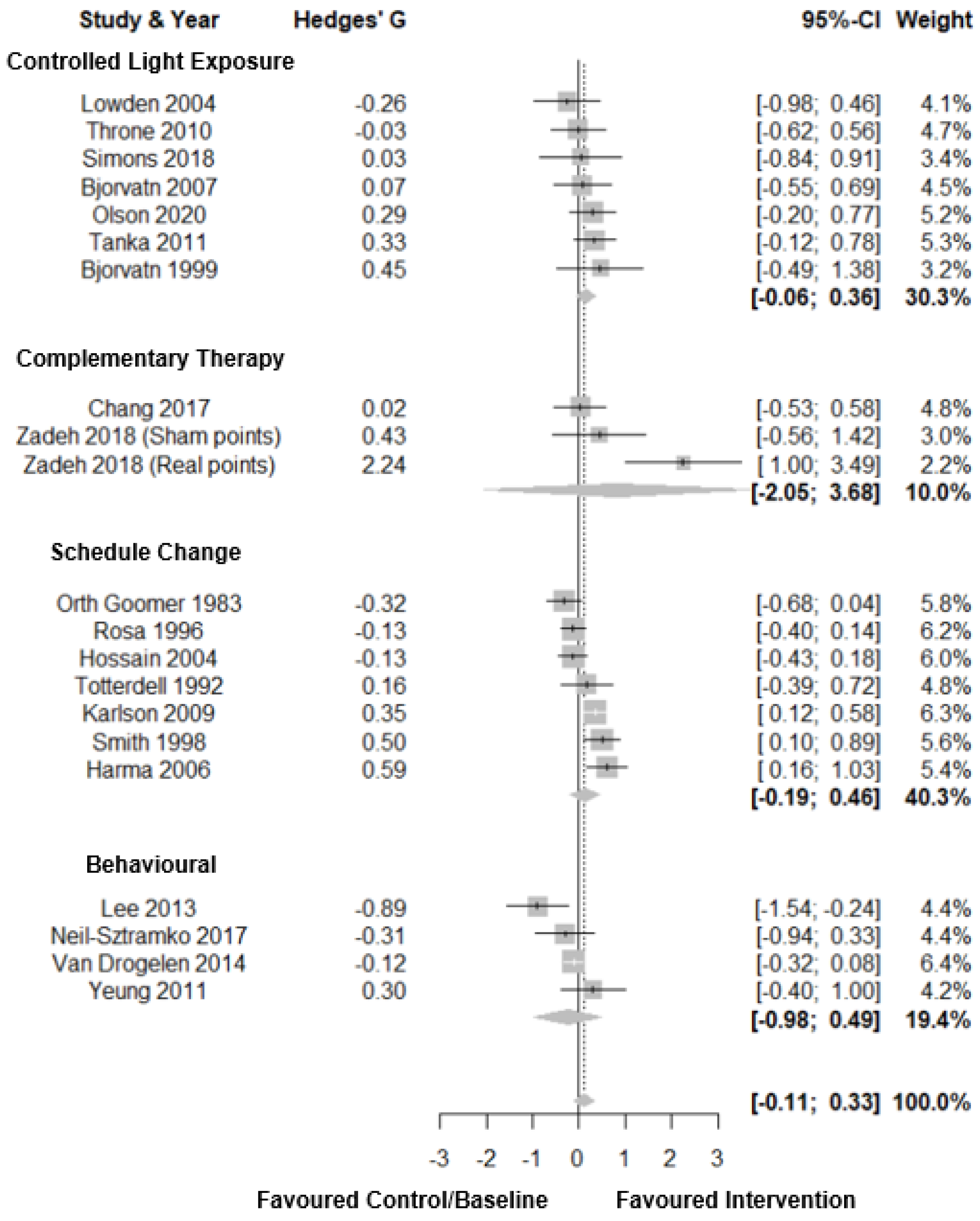
3.6.6. Subjective Sleep Quality
3.6.7. Perceived Health Status
4. Discussion
4.1. Summary of Evidence
4.2. Meta-Analytic Findings
4.3. Qualitative Findings
4.4. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kecklund, G.; Axelsson, J. Health consequences of shift work and insufficient sleep. BMJ 2016, 355, i5210. [Google Scholar] [CrossRef] [PubMed]
- Reynolds, A.C.; Paterson, J.L.; Ferguson, S.A.; Stanley, D.; Wright, K.P.; Dawson, D. The shift work and health research agenda: Considering changes in gut microbiota as a pathway linking shift work, sleep loss and circadian misalignment, and metabolic disease. Sleep Med. Rev. 2017, 34, 3–9. [Google Scholar] [CrossRef] [PubMed]
- Reynolds, A.C.; Broussard, J.; Paterson, J.L.; Wright, K.P., Jr.; Ferguson, S.A. Sleepy, circadian disrupted and sick: Could intestinal microbiota play an important role in shift worker health? Mol. Metab. 2017, 6, 12–13. [Google Scholar] [CrossRef] [PubMed]
- Australian Institute of Health and Welfare. Chronic Disease. Available online: https://www.aihw.gov.au/reports-data/health-conditions-disability-deaths/chronic-disease/overview (accessed on 10 September 2020).
- Torquati, L.; Mielke, G.I.; Brown, W.J.; Kolbe-Alexander, T. Shift work and the risk of cardiovascular disease. A systematic review and meta-analysis including dose–response relationship. Scand. J. Work Environ. Health 2017, 44, 229–238. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bøggild, H.; Knutsson, A. Shift work, risk factors and cardiovascular disease. Scand. J. Work Environ. Health 1999, 25, 85–99. [Google Scholar] [CrossRef]
- Wang, X.-S.; Armstrong, M.E.G.; Cairns, B.J.; Key, T.J.; Travis, R.C. Shift work and chronic disease: The epidemiological evidence. Occup. Med. 2011, 61, 78–89. [Google Scholar] [CrossRef] [Green Version]
- Vyas, M.V.; Garg, A.X.; Iansavichus, A.V.; Costella, J.; Donner, A.; Laugsand, L.E.; Janszky, I.; Mrkobrada, M.; Parraga, G.; Hackam, D.G. Shift work and vascular events: Systematic review and meta-analysis. BMJ 2012, 345, e4800. [Google Scholar] [CrossRef] [Green Version]
- Vetter, C.; Devore, E.E.; Wegrzyn, L.R.; Massa, J.; Speizer, F.E.; Kawachi, I.; Rosner, B.; Stampfer, M.J.; Schernhammer, E.S. Association Between Rotating Night Shift Work and Risk of Coronary Heart Disease Among Women. JAMA 2016, 315, 1726–1734. [Google Scholar] [CrossRef]
- Ellingsen, T.; Bener, A.; Gehani, A. Study of shift work and risk of coronary events. J. R. Soc. Promot. Health 2007, 127, 265–267. [Google Scholar] [CrossRef]
- Fujino, Y.; Iso, H.; Tamakoshi, A.; Inaba, Y.; Koizumi, A.; Kubo, T.; Yoshimura, T. A Prospective Cohort Study of Shift Work and Risk of Ischemic Heart Disease in Japanese Male Workers. Am. J. Epidemiol. 2006, 164, 128–135. [Google Scholar] [CrossRef] [Green Version]
- Mancio, J.; Leal, C.; Ferreira, M.; Norton, P.; Lunet, N. Does the association of prostate cancer with night-shift work differ according to rotating vs. fixed schedule? A systematic review and meta-analysis. Prostate Cancer Prostatic Dis. 2018, 21, 337–344. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xie, L.; Rao, D.; Yu, H.; Bai, Y.; Zheng, X. Does night-shift work increase the risk of prostate cancer? A systematic review and meta-analysis. OncoTargets Ther. 2015, 8, 2817–2826. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Behrens, T.; Rabstein, S.; Wichert, K.; Erbel, R.; Eisele, L.; Arendt, M.; Dragano, N.; Brüning, T.; Jöckel, K.-H. Shift work and the incidence of prostate cancer: A 10-year follow-up of a German population-based cohort study. Scand. J. Work Environ. Health 2017, 43, 560–568. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gan, Y.; Li, L.; Zhang, L.; Yan, S.; Gao, C.; Hu, S.; Qiao, Y.; Tang, S.; Wang, C.; Lu, Z. Association between shift work and risk of prostate cancer: A systematic review and meta-analysis of observational studies. Carcinogenesis 2017, 39, 87–97. [Google Scholar] [CrossRef] [PubMed]
- Wang, F.; Zhang, L.; Zhang, Y.; Zhang, B.; He, Y.; Xie, S.; Li, M.; Miao, X.; Chan, E.Y.Y.; Tang, J.L.; et al. Meta-analysis on night shift work and risk of metabolic syndrome. Obes. Rev. 2014, 15, 709–720. [Google Scholar] [CrossRef]
- De Bacquer, D.; Van Risseghem, M.; Clays, E.; Kittel, F.; De Backer, G.; Braeckman, L. Rotating shift work and the metabolic syndrome: A prospective study. Int. J. Epidemiol. 2009, 38, 848–854. [Google Scholar] [CrossRef] [Green Version]
- Sookoian, S.; Gemma, C.; Gianotti, T.F.; Burgueño, A.; Alvarez, A.; González, C.D.; Pirola, C.J. Effects of rotating shift work on biomarkers of metabolic syndrome and inflammation. J. Intern. Med. 2007, 261, 285–292. [Google Scholar] [CrossRef]
- Magrini, A.; Neri, A.; Somma, G.; Coppeta, L.; Iavicoli, I.; Bergamaschi, A.; Magrini, A. Incidence of metabolic syndrome among night-shift healthcare workers. Occup. Environ. Med. 2009, 67, 54–57. [Google Scholar] [CrossRef] [Green Version]
- Ye, H.H.; Jeong, J.U.; Jeon, M.-J.; Sakong, J. The Association between Shift Work and the Metabolic Syndrome in Female Workers. Ann. Occup. Environ. Med. 2013, 25, 33. [Google Scholar] [CrossRef] [Green Version]
- Lim, Y.C.; Hoe, V.C.W.; Darus, A.; Bhoo-Pathy, N. Association between night-shift work, sleep quality and metabolic syndrome. Occup. Environ. Med. 2018, 75, 716–723. [Google Scholar] [CrossRef]
- Schernhammer, E.S.; Kroenke, C.H.; Laden, F.; Hankinson, S.E. Night work and risk of breast cancer. Epidemiology 2006, 17, 108–111. [Google Scholar] [CrossRef] [PubMed]
- Hansen, J.; Lassen, C.F. Nested case–control study of night shift work and breast cancer risk among women in the Danish military. Occup. Environ. Med. 2012, 69, 551–556. [Google Scholar] [CrossRef] [PubMed]
- Lin, X.; Chen, W.; Wei, F.; Ying, M.; Wei, W.; Xie, X. Night-shift work increases morbidity of breast cancer and all-cause mortality: A meta-analysis of 16 prospective cohort studies. Sleep Med. 2015, 16, 1381–1387. [Google Scholar] [CrossRef]
- Rivera, A.S.; Akanbi, M.; O’Dwyer, L.C.; McHugh, M. Shift work and long work hours and their association with chronic health conditions: A systematic review of systematic reviews with meta-analyses. PLoS ONE 2020, 15, e0231037. [Google Scholar] [CrossRef]
- Brown, D.L.; Feskanich, D.; Sánchez, B.N.; Rexrode, K.M.; Schernhammer, E.S.; Lisabeth, L.D. Rotating Night Shift Work and the Risk of Ischemic Stroke. Am. J. Epidemiol. 2009, 169, 1370–1377. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, M.; Huang, J.-T.; Tan, Y.; Yang, B.-P.; Tang, Z.-Y. Shift work and risk of stroke: A meta-analysis. Int. J. Cardiol. 2016, 214, 370–373. [Google Scholar] [CrossRef]
- Costa, G. Shift Work and Health: Current Problems and Preventive Actions. Saf. Health Work 2010, 1, 112–123. [Google Scholar] [CrossRef] [Green Version]
- Dorrian, J.; Skinner, N. Alcohol Consumption Patterns of Shiftworkers Compared with Dayworkers. Chronobiol. Int. 2012, 29, 610–618. [Google Scholar] [CrossRef]
- Knauth, P.; Hornberger, S. Preventive and compensatory measures for shift workers. Occup. Med. 2003, 53, 109–116. [Google Scholar] [CrossRef] [Green Version]
- Australian Institute of Health and Welfare. Behavioural and Biomedical Risk Factors. Available online: https://www.aihw.gov.au/reports/chronic-disease/evidence-for-chronic-disease-risk-factors/contents/behavioural-and-biomedical-risk-factors (accessed on 12 December 2020).
- Medic, G.; Wille, M.; Hemels, M.E. Short- and long-term health consequences of sleep disruption. Nat. Sci. Sleep 2017, 9, 151–161. [Google Scholar] [CrossRef] [Green Version]
- Spiegel, K.; Knutson, K.; Leproult, R.; Tasali, E.; Van Cauter, E. Sleep loss: A novel risk factor for insulin resistance and Type 2 diabetes. J. Appl. Physiol. 2005, 99, 2008–2019. [Google Scholar] [CrossRef]
- Knutson, K.L.; Van Cauter, E. Associations between Sleep Loss and Increased Risk of Obesity and Diabetes. Ann. N. Y. Acad. Sci. 2008, 1129, 287–304. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoevenaar-Blom, M.P.; Spijkerman, A.M.; Kromhout, D.; Berg, J.F.V.D.; Verschuren, W.M. Sleep Duration and Sleep Quality in Relation to 12-Year Cardiovascular Disease Incidence: The MORGEN Study. Sleep 2011, 34, 1487–1492. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sabanayagam, C.; Shankar, A. Sleep Duration and Cardiovascular Disease: Results from the National Health Interview Survey. Sleep 2010, 33, 1037–1042. [Google Scholar] [CrossRef] [PubMed]
- Li, W.; Wang, D.; Cao, S.; Yin, X.; Gong, Y.; Gan, Y.; Zhou, Y.; Lu, Z. Sleep duration and risk of stroke events and stroke mortality: A systematic review and meta-analysis of prospective cohort studies. Int. J. Cardiol. 2016, 223, 870–876. [Google Scholar] [CrossRef]
- Bo, M.Y.; Yeoh, M.E.-K.; Guo, M.C.; Zhang, Z.; Tam, T.; Chan, T.-C.; Chang, L.-Y.; Lao, X. Sleep and the Risk of Chronic Kidney Disease: A Cohort Study. J. Clin. Sleep Med. 2019, 15, 393–400. [Google Scholar] [CrossRef] [Green Version]
- Cunningham, T.D.; Di Pace, B.S. Is Self-Reported Sleep Duration Associated with Osteoporosis? Data from a 4-Year Aggregated Analysis from the National Health and Nutrition Examination Survey. J. Am. Geriatr. Soc. 2015, 63, 1401–1406. [Google Scholar] [CrossRef]
- Idler, E.L.; Angel, R.J. Self-rated health and mortality in the NHANES-I Epidemiologic Follow-up Study. Am. J. Public Health 1990, 80, 446–452. [Google Scholar] [CrossRef] [Green Version]
- Mavaddat, N.; Valderas, J.M.; Van Der Linde, R.M.; Khaw, K.-T.; Kinmonth, A.-L. Association of self-rated health with multimorbidity, chronic disease and psychosocial factors in a large middle-aged and older cohort from general practice: A cross-sectional study. BMC Fam. Practt. 2014, 15, 185. [Google Scholar] [CrossRef] [Green Version]
- Burström, B.; Fredlund, P. Self rated health: Is it as good a predictor of subsequent mortality among adults in lower as well as in higher social classes? J. Epidemiol. Community Health 2001, 55, 836–840. [Google Scholar] [CrossRef] [Green Version]
- Neil-Sztramko, S.E.; Pahwa, M.; Demers, P.A.; Gotay, C.C. Health-related interventions among night shift workers: A critical review of the literature. Scand. J. Work Environ. Health 2014, 40, 543–556. [Google Scholar] [CrossRef] [PubMed]
- Weiss, P.; Kryger, M.; Knauert, M. Impact of extended duty hours on medical trainees. Sleep Health 2016, 2, 309–315. [Google Scholar] [CrossRef] [PubMed]
- Wagstaff, A.S.; Lie, J.-A.S. Shift and night work and long working hours—A systematic review of safety implications. Scand. J. Work Environ. Health 2011, 37, 173–185. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lauderdale, D.S.; Knutson, K.L.; Yan, L.L.; Liu, K.; Rathouz, P.J. Self-Reported and Measured Sleep Duration. Epidemiology 2008, 19, 838–845. [Google Scholar] [CrossRef] [Green Version]
- Jackson, C.L.; Patel, S.R.; Jackson, I.W.B.; Lutsey, P.L.; Redline, S. Agreement between self-reported and objectively measured sleep duration among white, black, Hispanic, and Chinese adults in the United States: Multi-Ethnic Study of Atherosclerosis. Sleep 2018, 41. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Prisma Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Bramer, W.M.; Rethlefsen, M.L.; Kleijnen, J.; Franco, O.H. Optimal database combinations for literature searches in systematic reviews: A prospective exploratory study. Syst. Rev. 2017, 6, 245. [Google Scholar] [CrossRef]
- The Cochrane Collaboration; Data Extraction Form. 2020. Available online: https://dplp.cochrane.org/data-extraction-forms (accessed on 11 January 2019).
- Downs, S.H.; Black, N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J. Epidemiol. Community Health 1998, 52, 377–384. [Google Scholar] [CrossRef] [Green Version]
- Signer, R.; Gafner, V.; Ernst, M.J. Adhäsive Kapsulitis der Schulter. Man. Med. 2016, 54, 95–100. [Google Scholar] [CrossRef]
- Shechter, A.; Quispe, K.A.; Barbecho, J.S.M.; Slater, C.; Falzon, L. Interventions to reduce short-wavelength (“blue”) light exposure at night and their effects on sleep: A systematic review and meta-analysis. SLEEP Adv. 2020, 1. [Google Scholar] [CrossRef]
- Higgins, J.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.; Welch, V.A. Cochrane Handbook for Systematic Reviews of Interventions. Version 6.1 (Updated September 2020). 2020. Available online: https://training.cochrane.org/handbook/current (accessed on 20 January 2021).
- Paul, G.; Huwaldt, J.A.; Steinhorst, S. Plot Digitizer 2.0; Free Software Foundation: Boston, MA, USA, 2015. [Google Scholar]
- Mavridis, D.; White, I.R. Dealing with missing outcome data in meta-analysis. Res. Synth. Methods 2020, 11, 2–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rothstein, H.R.; Borenstein, M.; Hedges, L.V.; Higgins, J.P.T. Multiple Outcomes or Time-Points within a Study. Introd. Meta-Anal. 2009, 225–238. [Google Scholar] [CrossRef]
- del Re, A.C.; Hoyt, W.T. MAd: Meta-Analysis with Mean Differences. R Package, Version 0.8-2. 2014. Available online: https://cran.r-project.org/package=MAd (accessed on 20 January 2021).
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2018; Available online: https://www.R-project.org/ (accessed on 10 November 2020).
- Harrer, M.; Cuijpers, P.; Furukawa, T.; Ebert, D.D. dmetar: Companion R Package for the Guide ‘Doing Meta-Analysis in R’. R Package Version 0.0.9000. 2019. Available online: http://dmetar.protectlab.org/ (accessed on 20 January 2021).
- Viechtbauer, W. Conducting meta-analyses in R with the metafor package. J. Stat. Softw. 2010, 36, 1–48. Available online: https://www.jstatsoft.org/v36/i03/ (accessed on 20 January 2021). [CrossRef] [Green Version]
- Lüdecke, D. esc: Effect Size Computation for Meta Analysis (Version 0.5.1). 2019. Available online: https://CRAN.R-project.org/package=esc (accessed on 20 January 2021).
- Borenstein, M.; Hedges, L.V.; Higgins, J.P.T.; Rothstein, H.R. Effect Sizes Based on Means. Introd. Meta Anal. 2009, 21–32. [Google Scholar] [CrossRef]
- Inthout, J.; Ioannidis, J.P.; Borm, G.F. The Hartung-Knapp-Sidik-Jonkman method for random effects meta-analysis is straightforward and considerably outperforms the standard DerSimonian-Laird method. BMC Med. Res. Methodol. 2014, 14, 25. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.T.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [Green Version]
- IntHout, J.; Ioannidis, J.P.A.; Rovers, M.M.; Goeman, J.J. Plea for routinely presenting prediction intervals in meta-analysis. BMJ Open 2016, 6, e010247. [Google Scholar] [CrossRef] [Green Version]
- Egger, M.; Smith, G.D.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [Green Version]
- Price, D.; Nelson, C.E.; Pollack, D. Communications among Scientists and Engineers; Heath Lexington Books; University of California: Madison, WI, USA, 1970. [Google Scholar]
- Sun, J.; Min, C.; Li, J. A vector for measuring obsolescence of scientific articles. Science 2016, 107, 745–757. [Google Scholar] [CrossRef]
- Akerstedt, T.; Torsvall, L. Experimental Changes in Shift Schedules—Their Effects on Well-Being. Ergonomics 1978, 21, 849–856. [Google Scholar] [CrossRef]
- Amendola, K.L.; Weisburd, D.; Hamilton, E.E.; Jones, G.; Slipka, M. An experimental study of compressed work schedules in policing: Advantages and disadvantages of various shift lengths. J. Exp. Criminol. 2011, 7, 407–442. [Google Scholar] [CrossRef]
- Barton, J.; Folkard, S.; Smith, L.; Poole, C.J. Effects on health of a change from a delaying to an advancing shift system. Occup. Environ. Med. 1994, 51, 749–755. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Basner, M.; Asch, D.A.; Shea, J.A.; Bellini, L.M.; Carlin, M.; Ecker, A.J.; Malone, S.K.; Desai, S.V.; Sternberg, A.L.; Tonascia, J.; et al. Sleep and Alertness in a Duty-Hour Flexibility Trial in Internal Medicine. N. Engl. J. Med. 2019, 380, 915–923. [Google Scholar] [CrossRef] [PubMed]
- Bøggild, H.; Jeppesen, H.J. Intervention in shift scheduling and changes in biomarkers of heart disease in hospital wards. Scand. J. Work Environ. Health 2001, 27, 87–96. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bonnefond, A.; Muzet, A.; Winter-Dill, A.-S.; Bailloeuil, C.; Bitouze, F.; Bonneau, A. Innovative working schedule: Introducing one short nap during the night shift. Ergonomics 2001, 44, 937–945. [Google Scholar] [CrossRef]
- Czeisler, C.A.; Moore-Ede, M.C.; Coleman, R.H. Rotating shift work schedules that disrupt sleep are improved by applying circadian principles. Science 1982, 217, 460–463. [Google Scholar] [CrossRef] [PubMed]
- Di Milia, L. A longitudinal study of the compressed workweek: Comparing sleep on a weekly rotating 8 h system to a faster rotating 12 h system. Int. J. Ind. Ergon. 1998, 21, 199–207. [Google Scholar] [CrossRef]
- Hakola, T.; Härmä, M. Evaluation of a fast forward rotating shift schedule in the steel industry with a special focus on ageing and sleep. J. Hum. Ergol. 2001, 30, 315–319. [Google Scholar]
- Hakola, T.; Paukkonen, M.; Pohjonen, T. Less quick returns--greater well-being. Ind. Health 2010, 48, 390–394. [Google Scholar] [CrossRef] [Green Version]
- Härmä, M.; Tarja, H.; Irja, K.; Mikael, S.; Jussi, V.; Anne, B.; Pertti, M. A controlled intervention study on the effects of a very rapidly forward rotating shift system on sleep–wakefulness and well-being among young and elderly shift workers. Int. J. Psychophysiol. 2006, 59, 70–79. [Google Scholar] [CrossRef]
- Hornberger, S.; Knauth, P. Effects of various types of change in shift schedules: A controlled longitudinal study. Work Stress 1995, 9, 124–133. [Google Scholar] [CrossRef]
- Hornberger, S.; Knauth, P. Follow-up intervention study on effects of a change in shift schedule on shiftworkers in the chemical industry. Int. J. Ind. Ergon. 1998, 21, 249–257. [Google Scholar] [CrossRef]
- Hossain, L.J.; Reinish, W.L.; Heslegrave, J.R.; Hall, W.G.; Kayumov, A.L.; Chung, M.S.; Bhuiya, P.; Jovanovic, D.; Huterer, N.; Volkov, J.; et al. Subjective and Objective Evaluation of Sleep and Performance in Daytime Versus Nighttime Sleep in Extended-Hours Shift-Workers at an Underground Mine. J. Occup. Environ. Med. 2004, 46, 212–226. [Google Scholar] [CrossRef] [Green Version]
- Karhula, K.; Hakola, T.; Koskinen, A.; Lallukka, T.; Ojajärvi, A.; Puttonen, S.; Oksanen, T.; Rahkonen, O.; Ropponen, A.; Härmä, M. Ageing shift workers’ sleep and working-hour characteristics after implementing ergonomic shift-scheduling rules. J. Sleep Res. 2020. [Google Scholar] [CrossRef] [PubMed]
- Karlson, B.; Eek, F.; Örbaek, P.; Österberg, K. Effects on sleep-related problems and self-reported health after a change of shift schedule. J. Occup. Health Psychol. 2009, 14, 97–109. [Google Scholar] [CrossRef]
- Knauth, P.; Hornberger, S. Changes from weekly backward to quicker forward rotating shift systems in the steel industry. Int. J. Ind. Ergon. 1998, 21, 267–273. [Google Scholar] [CrossRef]
- Kobayashi, F.; Furui, H.; Akamatsu, Y.; Watanabe, T.; Horibe, H. Changes in psychophysiological functions during night shift in nurses. Infuence of changing from a full-day to a half day work shift before night duty. Int. Arch. Occup. Environ. Health 1997, 69, 83–90. [Google Scholar] [CrossRef]
- Lowden, A.; Kecklund, G.; Axelsson, J.; Akerstedt, T. Change from an 8-hour shift to a 12-hour shift, attitudes, sleep, sleepiness and performance. Scand. J. Work Environ. Health 1998, 24, 69–75. [Google Scholar]
- Mitchell, R.; Williamson, A.M. Evaluation of an 8 hour versus a 12 hour shift roster on employees at a power station. Appl. Ergon. 2000, 31, 83–93. [Google Scholar] [CrossRef]
- Orth-Gomer, K. Intervention on Coronary Risk Factors by Adapting a Shift Work Schedule to Biologic Rhythmicity. Psychosom. Med. 1983, 45, 407–415. [Google Scholar] [CrossRef]
- Peacock, B.; Glube, R.; Miller, M.; Clune, P. Police officers’ responses to 8 and 12 hour shift schedules. Ergonomics 1983, 26, 479–493. [Google Scholar] [CrossRef] [PubMed]
- Rosa, R.R.; Harma, M.; Pulli, K.; Mulder, M.; Nasman, O. Rescheduling a three shift system at a steel rolling mill: Effects of a one hour delay of shift starting times on sleep and alertness in younger and older workers. Occup. Environ. Med. 1996, 53, 677–685. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, P.A.; Wright, B.M.; Mackey, R.W.; Milsop, H.W.; Yates, S.C. Change from slowly rotating 8-hour shifts to rapidly rotating 8-hour and 12-hour shifts using participative shift roster design. Scand. J. Work Environ. Health 1998, 24, 55–61. [Google Scholar] [PubMed]
- Totterdell, P.; Smith, L. Ten-hour days and eight-hour nights: Can the Ottawa Shift System reduce the problems of shiftwork? Work Stress 1992, 6, 139–152. [Google Scholar] [CrossRef]
- Viitasalo, K.; Kuosma, E.; Laitinen, J.; Härmä, M. Effects of shift rotation and the flexibility of a shift system on daytime alertness and cardiovascular risk factors. Scand. J. Work Environ. Health 2008, 34, 198–205. [Google Scholar] [CrossRef] [Green Version]
- Watanabe, M.; Akamatsu, Y.; Furui, H.; Tomita, T.; Watanabe, T.; Kobayashi, F. Effects of changing shift schedules from a full-day to a half-day shift before a night shift on physical activities and sleep patterns of single nurses and married nurses with children. Ind. Health 2004, 42, 34–40. [Google Scholar] [CrossRef] [Green Version]
- Williamson, A.M.; Gower, C.G.; Clarke, B.C. Changing the hours of shiftwork: A comparison of 8- and 12-hour shift rosters in a group of computer operators. Ergonomics 1994, 37, 287–298. [Google Scholar] [CrossRef]
- Williamson, A.M.; Sanderson, J.W. Changing the speed of shift rotation: A field study. Ergonomics 1986, 29, 1085–1096. [Google Scholar] [CrossRef]
- Yamada, Y.; Kameda, M.; Noborisaka, Y.; Suzuki, H.; Honda, M.; Yamada, S. Excessive fatigue and weight gain among cleanroom workers after changing from an 8-hour to a 12-hour shift. Scand. J. Work Environ. Health 2001, 27, 318–326. [Google Scholar] [CrossRef] [Green Version]
- Arora, V.M.; Georgitis, E.; Woodruff, J.N.; Humphrey, H.J.; Meltzer, D. Improving Sleep Hygiene of Medical InternsCan the Sleep, Alertness, and Fatigue Education in Residency Program Help? Arch. Intern. Med. 2007, 167, 1738. [Google Scholar] [CrossRef] [Green Version]
- Elliot, D.L.; Goldberg, L.; Kuehl, K.S.; Moe, E.L.; Breger, R.K.R.; Pickering, M.A. The PHLAME (Promoting Healthy Lifestyles: Alternative Models Effects) Firefighter Study: Outcomes of Two Models of Behavior Change. J. Occup. Environ. Med. 2007, 49, 204–213. [Google Scholar] [CrossRef] [PubMed]
- MacKinnon, D.P.; Elliot, D.L.; Thoemmes, F.; Kuehl, K.S.; Moe, E.L.; Goldberg, L.; Burell, G.L.; Ranby, K.W. Long-term effects of a worksite health promotion program for firefighters. Am. J. Health Behav. 2010, 34, 695–706. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Härmä, M.I.; Ilmarinen, J.; Knauth, P.; Rutenfranz, J.; Hanninen, O. Physical training intervention in female shift workers: I. The effects of intervention on fitness, fatigue, sleep, and psychosomatic symptoms. Ergonomics 1988, 31, 39–50. [Google Scholar] [CrossRef] [PubMed]
- Holbrook, M.I.; White, M.H.; Hutt, M.J. Increasing Awareness of Sleep Hygiene in Rotating Shift Workers: Arming Law-Enforcement Officers against Impaired Performance. Percept. Mot. Ski. 1994, 79, 520–522. [Google Scholar] [CrossRef] [PubMed]
- Kerin, A.; Aguirre, A. Improving Health, Safety, and Profits in Extended Hours Operations (Shiftwork). Ind. Health 2005, 43, 201–208. [Google Scholar] [CrossRef] [Green Version]
- Lee, K.A.; Gay, C.L.; Alsten, C.R. Home-Based Behavioral Sleep Training for Shift Workers: A Pilot Study. Behav. Sleep Med. 2013, 12, 455–468. [Google Scholar] [CrossRef]
- Leedo, E.; Beck, A.M.; Astrup, A.; Lassen, A.D. The effectiveness of healthy meals at work on reaction time, mood and dietary intake: A randomised cross-over study in daytime and shift workers at an university hospital. Br. J. Nutr. 2017, 118, 121–129. [Google Scholar] [CrossRef] [Green Version]
- Lim, S.-T.; Min, S.-K.; Kwon, Y.-C.; Park, S.-K.; Park, H. Effects of intermittent exercise on biomarkers of cardiovascular risk in night shift workers. Atherosclerosis 2015, 242, 186–190. [Google Scholar] [CrossRef]
- Matsugaki, R.; Kuhara, S.; Saeki, S.; Jiang, Y.; Michishita, R.; Ohta, M.; Yamato, H. Effectiveness of workplace exercise supervised by a physical therapist among nurses conducting shift work: A randomized controlled trial. J. Occup. Health 2017, 59, 327–335. [Google Scholar] [CrossRef] [Green Version]
- Morgan, P.; Collins, C.E.; Plotnikoff, R.C.; Cook, A.T.; Berthon, B.; Mitchell, S.; Callister, R. Efficacy of a workplace-based weight loss program for overweight male shift workers: The Workplace POWER (Preventing Obesity Without Eating like a Rabbit) randomized controlled trial. Prev. Med. 2011, 52, 317–325. [Google Scholar] [CrossRef]
- Neil-Sztramko, S.E.; Gotay, C.C.; Sabiston, C.M.; Demers, P.A.; Campbell, K.C. Feasibility of a telephone and web-based physical activity intervention for women shift workers. Trans. Behav. Med. 2017, 7, 268–276. [Google Scholar] [CrossRef] [PubMed]
- Pylkkönen, M.; Tolvanen, A.; Hublin, C.; Kaartinen, J.; Karhula, K.; Puttonen, S.; Sihvola, M.; Sallinen, M. Effects of alertness management training on sleepiness among long-haul truck drivers: A randomized controlled trial. Accid. Anal. Prev. 2018, 121, 301–313. [Google Scholar] [CrossRef] [PubMed]
- Smith-Coggins, R.; Rosekind, M.R.; Buccino, K.R.; Dinges, D.F.; Moser, R.P. Rotating Shiftwork Schedules: Can We Enhance Physician Adaptation to Night Shifts? Acad. Emerg. Med. 1997, 4, 951–961. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, J.P.; O’Brien, C.S.; Barger, L.K.; Rajaratnam, S.M.W.; Czeisler, C.A.; Lockley, S.W. Randomized, Prospective Study of the Impact of a Sleep Health Program on Firefighter Injury and Disability. Sleep 2017, 40. [Google Scholar] [CrossRef] [Green Version]
- Van Drongelen, A.; Boot, C.R.; Hlobil, H.; Twisk, J.W.; Smid, T.; Van Der Beek, A.J. Evaluation of an mHealth intervention aiming to improve health-related behavior and sleep and reduce fatigue among airline pilots. Scand. J. Work Environ. Health 2014, 40, 557–568. [Google Scholar] [CrossRef] [Green Version]
- Yeung, J.; Sletten, T.L.; Rajaratnam, S.M. A phase-advanced, extended sleep paradigm to increase sleep duration among early-morning shift workers: A preliminary investigation. Scand. J. Work Environ. Health 2010, 37, 62–69. [Google Scholar] [CrossRef] [Green Version]
- Bjorvatn, B.; Kecklund, G.; Åkerstedt, T. Bright light treatment used for adaptation to night work and re-adaptation back to day life. A field study at an oil platform in the North Sea. J. Sleep Res. 1999, 8, 105–112. [Google Scholar] [CrossRef] [Green Version]
- Bjorvatn, B.; Stangenes, K.; Oyane, N.; Forberg, K.; Lowden, A.; Holsten, F.; Akerstedt, T. Randomized placebo-controlled field study of the effects of bright light and melatonin in adaptation to night work. Scand. J. Work Environ. Health 2007, 33, 204–214. [Google Scholar] [CrossRef] [Green Version]
- Boivin, D.B.; Boudreau, P.; James, F.O.; Kin, N.M.K.N.Y. Photic Resetting in Night-Shift Work: Impact on Nurses’ Sleep. Chronobiol. Int. 2012, 29, 619–628. [Google Scholar] [CrossRef]
- Budnick, L.D.; Lerman, S.E.; Nicolich, M.J. An evaluation of scheduled bright light and darkness on rotating shiftworkers: Trial and limitations. Am. J. Ind. Med. 1995, 27, 771–782. [Google Scholar] [CrossRef]
- Costa, G.; Ghirlanda, G.; Minors, D.S.; Waterhouse, J.M. Effect of bright light on tolerance to night work. Scand. J. Work Environ. Health 1993, 19, 414–420. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jensen, H.I.; Markvart, J.; Holst, R.; Thomsen, T.D.; Larsen, J.W.; Eg, D.M.; Nielsen, L.S. Shift work and quality of sleep: Effect of working in designed dynamic light. Int. Arch. Occup. Environ. Health 2016, 89, 49–61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lowden, A.; Akerstedt, T.; Wibom, R. Suppression of sleepiness and melatonin by bright light exposure during breaks in night work. J. Sleep Res. 2004, 13, 37–43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Olson, J.A.; Artenie, D.Z.; Cyr, M.; Raz, A.; Lee, V. Developing a light-based intervention to reduce fatigue and improve sleep in rapidly rotating shift workers. Chronobiol. Int. 2019, 37, 573–591. [Google Scholar] [CrossRef]
- Sasseville, A.; Benhaberou-Brun, D.; Fontaine, C.; Charon, M.-C.; Hébert, M. Wearing Blue-Blockers in the Morning Could Improve Sleep of Workers on a Permanent Night Schedule: A Pilot Study. Chronobiol. Int. 2009, 26, 913–925. [Google Scholar] [CrossRef]
- Sasseville, A.; Hébert, M. Using blue-green light at night and blue-blockers during the day to improves adaptation to night work: A pilot study. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2010, 34, 1236–1242. [Google Scholar] [CrossRef]
- Simons, K.S.; Boeijen, E.R.K.; Mertens, M.C.; Rood, P.; de Jager, C.P.C.; den Boogaard, M.V. Effect of dynamic light application on cognitive performance and well-being of intensive care nuses. Am. J. Crit. Care. 2018, 27, 245–248. [Google Scholar] [CrossRef]
- Tanaka, K.; Takahashi, M.; Tanaka, M.; Takanao, T.; Nishinoue, N.; Kaku, A.; Kato, N.; Tagaya, H.; Miyaoka, H. Brief Morning Exposure to Bright Light Improves Subjective Symptoms and Performance in Nurses with Rapidly Rotating Shifts. J. Occup. Health 2011, 53, 258–266. [Google Scholar] [CrossRef] [Green Version]
- Thorne, H.C.; Hampton, S.M.; Morgan, L.M.; Skene, D.J.; Arendt, J. Returning from night shift to day life: Beneficial effects of light on sleep. Sleep Biol. Rhythm. 2010, 8, 212–221. [Google Scholar] [CrossRef] [Green Version]
- Yoon, I.-Y.; Jeong, D.-U.; Kwon, K.-B.; Kang, S.-B.; Song, B.-G. Bright Light Exposure at Night and Light Attenuation in the Morning Improve Adaptation of Night Shift Workers. Sleep 2002, 25, 351–356. [Google Scholar] [CrossRef]
- Chang, Y.-Y.; Lin, C.-L.; Chang, L.-Y. The Effects of Aromatherapy Massage on Sleep Quality of Nurses on Monthly Rotating Night Shifts. Evid. Based Complement. Altern. Med. 2017, 2017, 3861273. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fazeli, M.S.; Pourrahmat, M.-M.; Massah, G.; Lee, K.; Lavoie, P.M.; Fazeli, M.; Esser, A.; Collet, J.-P. The Effect of Massage on the Cardiac Autonomic Nervous System and Markers of Inflammation in Night Shift Workers: A Pilot Randomized Crossover Trial. Int. J. Ther. Massage Bodyw. 2020, 13, 6–17. [Google Scholar]
- McElligott, D.; Holz, M.B.; Carollo, L.; Somerville, S.; Baggett, M.; Kuzniewski, S.; Shi, Q. A pilot feasibility study of the effects of touch therapy on nurses. J. N. Y. State Nurses’ Assoc. 2003, 34, 16–24. [Google Scholar]
- Zadeh, B.Q.; Hadadian, F.; Salari, N.; Maazinezhad, S.; Paveh, B.K. The Effect of Transcotaneus Electrical Acupoint Stimulation on Sleep Quality in Nurses. J. Kermanshah Univ. Med. Sci. 2018, 22. [Google Scholar] [CrossRef] [Green Version]
- Härmä, M.; Karhula, K.; Ropponen, A.; Puttonen, S.; Koskinen, A.; Ojajärvi, A.; Hakola, T.; Pentti, J.; La Oksanen, T.; Vahtera, J.; et al. Association of changes in work shifts and shift intensity with change in fatigue and disturbed sleep: A within-subject study. Scand. J. Work Environ. Health 2018, 44, 394–402. [Google Scholar] [CrossRef]
- Garde, A.H.; Nabe-Nielsen, K.; Jensen, M.A.; Kristiansen, J.; Sørensen, J.K.; Hansen, Å.M. The effects of the number of consecutive night shifts on sleep duration and quality. Scand. J. Work Environ. Health 2020, 46, 446–453. [Google Scholar] [CrossRef]
- Harrington, J.M. Health effects of shift work and extended hours of work. Occup. Environ. Med. 2001, 58, 68–72. [Google Scholar] [CrossRef] [Green Version]
- Nielsen, H.B.; Larsen, A.D.; Dyreborg, J.; Hansen, Å.M.; Pompeii, L.A.; Conway, S.H.; Hansen, J.; Kolstad, H.A.; Nabe-Nielsen, K.; Garde, A.H. Risk of injury after evening and night work—findings from the Danish Working Hour Database. Scand. J. Work Environ. Health 2018, 44, 385–393. [Google Scholar] [CrossRef] [Green Version]
- Vedaa, Ø.; Harris, A.; Waage, S.; Bjorvatn, B.; Thun, E.; Buchvold, H.V.; Djupedal, I.L.R.; Pallesen, S. A longitudinal study on the association between quick returns and occupational accidents. Scand. J. Work Environ. Health 2020, 46, 645–649. [Google Scholar] [CrossRef]
- Bonde, J.P.; Hansen, J.; Kolstad, H.A.; Mikkelsen, S.; Olsen, J.H.; Blask, D.E.; Härmä, M.; Kjuus, H.; De Koning, H.J.; Olsen, J.; et al. Work at night and breast cancer—report on evidence-based options for preventive actions. Scand. J. Work Environ. Health 2012, 38, 380–390. [Google Scholar] [CrossRef] [Green Version]
- Finlay, A.; Evans, H.; Vincent, A.; Wittert, G.; Vandelanotte, C.; Short, C.E. Optimising Web-Based Computer-Tailored Physical Activity Interventions for Prostate Cancer Survivors: A Randomised Controlled Trial Examining the Impact of Website Architecture on User Engagement. Int. J. Environ. Res. Public Health 2020, 17, 7920. [Google Scholar] [CrossRef] [PubMed]
- De Cocker, K.; De Bourdeaudhuij, I.; Cardon, G.; Vandelanotte, C. The Effectiveness of a Web-Based Computer-Tailored Intervention on Workplace Sitting: A Randomized Controlled Trial. J. Med. Internet Res. 2016, 18, e96. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lowden, A.; Öztürk, G.; Reynolds, A.C.; Bjorvatn, B. Working Time Society consensus statements: Evidence based interventions using light to improve circadian adaptation to working hours. Ind. Health 2019, 57, 213–227. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wong, I.S.; McLeod, C.B.; Demers, P.A. Shift work trends and risk of work injury among Canadian workers. Scand. J. Work Environ. Health 2011, 37, 54–61. [Google Scholar] [CrossRef] [Green Version]
- Zhao, I.; Bogossian, F.; Turner, C. Shift work and work related injuries among health care workers: A systematic review. Aust. J. Adv. Nurs. 2010, 27, 1–89. [Google Scholar]
- Fischer, D.; Lombardi, D.A.; Folkard, S.; Willetts, J.; Christiani, D.C. Updating the “Risk Index”: A systematic review and meta-analysis of occupational injuries and work schedule characteristics. Chronobiol. Int. 2017, 34, 1423–1438. [Google Scholar] [CrossRef]
- Lombardi, D.A.; Folkard, S.; Willetts, J.L.; Smith, G.S. Daily sleep, weekly working hours, and risk of work-related injury: Us national health interview survey (2004–2008). Chronobiol. Int. 2010, 27, 1013–1030. [Google Scholar] [CrossRef]
- Ferri, P.; Guadi, M.; Marcheselli, L.; Balduzzi, S.; Magnani, D.; Di Lorenzo, R. The impact of shift work on the psychological and physical health of nurses in a general hospital: A comparison between rotating night shifts and day shifts. Health Policy 2016, 9, 203–211. [Google Scholar] [CrossRef] [Green Version]
- Angerer, P.; Schmook, R.; Elfantel, I.; Li, J. Night Work and the Risk of Depression: A Systematic Review. Dtsch. Aerzteblatt Online 2017, 114, 404–411. [Google Scholar] [CrossRef] [Green Version]
- Lee, A.; Myung, S.K.; Cho, J.J.; Jung, Y.-J.; Yoon, J.L.; Kim, M.Y. Night Shift Work and Risk of Depression: Meta-analysis of Observational Studies. J. Korean Med. Sci. 2017, 32, 1091–1096. [Google Scholar] [CrossRef]
- Jiang, Y.; Wu, C.; Hu, T.; Chen, M.; Liu, W.; Zhou, Y.; Chen, Z.; Xu, X. Association for combined exposure to job strain, shift work on mental health among Chinese railway workers: A cross-sectional study. BMJ Open 2020, 10, e037544. [Google Scholar] [CrossRef] [PubMed]
- Stocker, L.J.; Macklon, N.S.; Cheong, Y.C.; Bewley, S.J. Influence of shift work on early reproductive outcomes: A systematic review and meta-analysis. Obstet. Gynecol. 2014, 124, 99–110. [Google Scholar] [CrossRef] [PubMed]
- Kloss, J.D.; Perlis, M.L.; Zamzow, J.A.; Culnan, E.J.; Gracia, C.R. Sleep, sleep disturbance, and fertility in women. Sleep Med. Rev. 2015, 22, 78–87. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marino, J.L.; Varcoe, T.J.; Davis, S.; Moran, L.J.; Rumbold, A.R.; Brown, H.M.; Whitrow, M.J.; Davies, M.J.; Moore, V.M.; Fernandez, R.C. Fixed or Rotating Night Shift Work Undertaken by Women: Implications for Fertility and Miscarriage. Semin. Reprod. Med. 2016, 34, 74–82. [Google Scholar] [CrossRef] [PubMed]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Biomedical Risk Factors | Behavioural Risk Factors | |||||||
|---|---|---|---|---|---|---|---|---|
| Common Chronic Disease | High Blood Pressure | Obesity | Dyslipidaemia | Abnormal Glucose | Tobacco Smoking | Insufficient Physical Activity | Excessive Alcohol Consumption | Poor Nutritional Intake |
| Cardiovascular disease |
| |||||||
| Stroke | - |
| ||||||
| Type 2 diabetes |
| - |
| |||||
| Colorectal cancer |
| - | - |
| ||||
| Osteoporosis |
|
| - |
| ||||
| Breast cancer (in females) |
| - | - | - |
|
| ||
| Chronic kidney disease | - | - |
|
|
| |||
| Biomedical Risk Factors | Behavioural Risk Factors | Sleep | Global Health | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Study, Year | Intervention Type | Blood Pressure | Body Mass Index | Dyslipidemia (d) | Glucose (d) | Tobacco Smoking (d) | Physical Activity (d) | Alcohol Intake (d) | Nutritional Intake (d) | Objective Sleep Duration | Objective Sleep Efficiency | Subjective Sleep Length | Subjective Sleep Quality | Perceived Health Status |
| Akerstedt, 1978 | schedule |
| ||||||||||||
| Amendola, 2011 | schedule |
|
| |||||||||||
| Arora, 2007 | behaviour |
| ||||||||||||
| Barton, 1994 | schedule | |||||||||||||
| Basner 2019 | schedule |
|
| |||||||||||
| Bjorvatn, 1999 | light |
|
| |||||||||||
| Bjorvatn, 2007 | light | |||||||||||||
| Bøggild, 2001 | schedule |
|
|
|
| |||||||||
| Boivin, 2012 | light | |||||||||||||
| Bonneford, 2001 | schedule |
| ||||||||||||
| Budnick, 1995 | light |
|
| |||||||||||
| Chang, 2015 | complementary | |||||||||||||
| Costa 1993 | light |
| ||||||||||||
| Czeisler, 1982 | schedule |
|
| |||||||||||
| Di Milia, 1998 | schedule |
| ||||||||||||
| Elliot, 2007 | behaviour |
| ||||||||||||
| Fazeli, 2020 | complementary |
| ||||||||||||
| Hakola, 2002 | schedule |
|
|
|
| |||||||||
| Hakola, 2010 | schedule | |||||||||||||
| Harma, 2006 | schedule |
|
| |||||||||||
| Härmä, 1988 | behaviour |
| ||||||||||||
| Holbrook, 1994 | behaviour |
| ||||||||||||
| Hornberger, 1995 | schedule |
| ||||||||||||
| Hornberger, 1998 | schedule |
| ||||||||||||
| Hossain, 2004 | schedule |
|
|
| ||||||||||
| Jensen, 2016 | light |
|
|
|
| |||||||||
| Karhula, 2020 | schedule |
|
|
|
|
|
| |||||||
| Karlson, 2009 | schedule | |||||||||||||
| Kerin, 2005 | behaviour |
| ||||||||||||
| Knauth, 1998 | schedule |
|
| |||||||||||
| Kobayashi, 1997 | schedule | |||||||||||||
| Lee, 2014 | behaviour | |||||||||||||
| Leedo, 2017 | behaviour |
| ||||||||||||
| Lim, 2015 | behaviour | |||||||||||||
| Lowden, 2004 | light |
| ||||||||||||
| Lowden, 1998 | schedule |
|
|
|
|
| ||||||||
| MacKinnon, 2010 | behaviour |
|
|
|
| |||||||||
| Matsugaki, 2017 | behaviour | |||||||||||||
| McElligott, 2003 | complementary |
| ||||||||||||
| Mitchell, 2000 | schedule |
| ||||||||||||
| Morgan, 2011 | behaviour |
| ||||||||||||
| Neil-Sztramko, 2017 | behaviour | |||||||||||||
| Olson, 2020 | light |
| ||||||||||||
| Orth Gomer, 1983 | schedule |
|
| |||||||||||
| Peacock, 1983 | schedule |
|
| |||||||||||
| Pylkkönen, 2018 | behaviour |
|
| |||||||||||
| Rosa, 1996 | schedule | |||||||||||||
| Sasseville, 2009 | light | |||||||||||||
| Sasseville, 2010 | light | |||||||||||||
| Simons, 2018 | light | |||||||||||||
| Smith, 1998 | schedule |
|
| |||||||||||
| Smith-Coggins, 1997 | behaviour |
|
|
| ||||||||||
| Sullivan, 2017 | behaviour | |||||||||||||
| Tanaka, 2011 | light | |||||||||||||
| Thorne, 2010 | light |
| ||||||||||||
| Totterdell, 1992 | schedule | |||||||||||||
| van Drongelen, 2014 | behaviour |
|
| |||||||||||
| Viitasalon, 2008 | schedule |
|
|
|
| |||||||||
| Watanabe, 2004 | schedule | |||||||||||||
| Williamson, 1994 | schedule |
| ||||||||||||
| Williamson, 1986 | schedule |
|
|
|
| |||||||||
| Yamada, 2001 | schedule | |||||||||||||
| Yeung, 2011 | behaviour |
| ||||||||||||
| Yoon, 2002 | light |
| ||||||||||||
| Zadeh, 2018 | complementary | |||||||||||||
| Author Year | Sample Size | Sample Characteristics (Sex, Mean Age) | Occupation | Type of Shift Work at Baseline | Intervention Detail | Intervention Duration | Outcome Measure (Measurement Used) | Results |
|---|---|---|---|---|---|---|---|---|
| Akerstedt et al., 1978 [70] | 361 | Not reported | Steel manufacturing employees | Rotating shift work | (I1) change from 3/4 shift to 2 shift (n = 69) (I2) change from 4 to 3 shift (n = 41) (C1) 2 shift no change (n = 16) (C2) 3 shift no change (n = 73) (C3) 4 shift no change (n = 77) | 12 months | Subjective sleep duration (questionnaire) | (I1) Increased subjective sleep duration (I2) Decrease in subjective sleep duration |
| Amendola et al., 2011 [71] | 226 | M = 174 F = 52 Age not reported | Police officers | Not reported | Randomly assigned to 8, 10 or 12 h shifts | 6 months | Subjective sleep duration (aleep diary) Subjective sleep quality (sleep diary) | Officers in the 10 h condition averaged more hours of sleep than officers in the 8 and 12 h shifts |
| Barton et al., 1994 [72] | 293 | M = 271 F = 22 30.2 years | Car manufacturing employees | Rotating shift work | Change from an 8 h forward rotation to an 8 h backward system | 6 months | Cigarette consumption (questionnaire) Alcohol consumption (questionnaire) Subjective sleep duration (sleep diary) Subjective sleep quality (sleep diary) | Increased sleep difficulties between afternoon shifts |
| Basner et al., 2019 [73] | 398 | M = 203 F = 195 27.9 years | Medical interns | Rotating shift work | (i) Standard 2011 duty hour policies (ii) Flexible policies—80 h work week without limits on shift duration or mandatory time off between shifts | 14 days | Objective sleep duration (actigraphy) | No significant difference in objective sleep duration |
| Bøggild et al., 2001 [74] | 101 | Sex not reported Median age: Intervention = 34.5 Control = 42.0 | Nurses and nurses′ aids | Rotating and permanent evening or night shifts | Ergonomic shift design—more regular, more weekends off and maximum of 3 to 4 consecutive night shifts followed by extra day off | 6 months | Cholesterol (HDL-C, LDL-C) Cigarette consumption (Standard Shiftwork Index) Physical activity (Standard Shiftwork Index) Alcohol consumption (Standard Shiftwork Index) | HDL-C level increased LDL-C and the total HDL-C cholesterol ratio decreased |
| Bonnefond et al., 2001 [75] | 12 | M = 12 F = 0 37.0 years | Electric power plant employees | Rotating shift work | One short rest period approx. 1 h, during nightshift whenever possible | 1 year | Subjective sleep duration (sleep diary) Subjective sleep quality (sleep diary) | Improved subjective sleep quality |
| Czeisler et al., 1982 [76] | 85 | M = 85 F = 0 31.4 years | Minerals and chemical corporation plant employees | Rotating shift work | Intervention: 52 others rotated shifts by phase delay once every 21 days Control: 33 workers continued to change shifts each week | 9 months | Subjective sleep quality (sleep–wake questionnaire) Perceived health status (questionnaire) | Improved perceived health status |
| Di Milia et al., 1998 [77] | 3 | M = 3 F = 0 Ages 34, 27, 30 years | Electricians in coal mine | Rotating shift work | Change from 8 to 12 h system | 11 months | Subjective sleep duration (sleep diary) | Decrease in subjective sleep duration on night shift |
| Hakola and Harma, 2002 [78] | 16 | M = 16 F = 0 42.0 years | Steel industry employees | Rotating shift work | A continuous three-shift schedule was changed from a slow backward-rotating to a fast forward-rotating system | 1 year | Objective sleep duration (actigraphy) Objective sleep efficiency (actigraphy) Subjective sleep duration (sleep log) Subjective sleep quality (sleep log) | Improved objective sleep efficiency Improved subjective sleep quality after morning shift |
| Hakola et al., 2010 [79] | 75 | M = 3 F = 72 46.0 years | Nurses | Rotating shift work | Increased recovery time between evening and morning shifts | 1 year | Subjective sleep duration (Modified Standard Shiftwork Index) | Increased subjective sleep duration |
| Harma et al., 2006 [80] | 140 | M = 140 F = 0 45- Control = 36.0 45- Intervention = 36.0 45+ Control = 50.0 45+ Intervention = 52.0 | Maintenance employees | Rotating shift work | Change from backward-rotating three-shift system to very quickly forward-rotating shift system was developed | 6 months | Objective sleep (actigraphy) Subjective sleep duration (sleep diary) Subjective sleep quality (sleep diary) | Increased subjective sleep duration following night shift |
| Hornberger et al., 1995 [81] | 260 | M = 260 F = 0 Group B = 38.2 years Group E = 38.9 years | Chemical industry employees | Rotating shift work | Change from discontinuous to continuous shift system. Change to faster rotation with shorter working days | 7–9 months | Subjective sleep quality (questionnaire) | 2 groups showed improved subjective sleep quality 1 group showed decreased subjective sleep quality |
| Hornberger et al., 1998 [82] Follow up of study Hornberger et al., 1995 | 50 | M = 50 F = 0 32.8 years | Chemical industry employees | Rotating shift work | Change from discontinuous to continuous shift system. Change to faster rotation with shorter working days | 4.5 year follow up | Subjective sleep quality (questionnaire) | No change |
| Hossain et al., 2004 [83] | 58 | M = 58 F = 0 40.3 years | Mine workers | Rotating shift work | Change from a backward-rotating 8 h to a forward-rotating 10 h shift schedule | 1 month | Subjective sleep quality (shift work and you) Subjective sleep duration (shift work and you) Perceived health status (shift work and you) | Increased subjective sleep duration on day shift schedule Improved subjective sleep quality on night shift and days off |
| Karhula et al., 2020 [84] | 1487 | M = 70 F = 1417 Control = 52.3 years Intervention = 52.5 years | Social and healthcare employees (nurses, nurse assistants, social workers) | Rotating shift work | Ergonomic roster: Change from backward to forward rotation. Max of 50 h worked per week. Night shifts followed by at least two days off. Maximum shift shift 10 h. Increased recovery time between shifts. | 5–6 years | Subjective sleep duration (self-report average 24 h sleep duration) Subjective sleep quality (survey for past 4 weeks) Smoking (Yes/No) Physical activity (self-report hours per week) Alcohol intake (questionnaire) Perceived health status (“How is your health compared to someone else your age?”) | Improved subjective sleep quality Increases in intervention workers reporting long sleep (>9 h) Improved perceived health status |
| Karlson and Eek, 2009 [85] | 118 | M = 98 F = 20 44.6 years | Manufacturing plant employees | Rotating shift work | Change from fast forward rotation to a slower backward rotation with 3 days on a given shift followed by 3 days off | 15 months | Subjective sleep quality (Karolinska Sleep Questionnaire) Perceived health status (self-rated health question) | Improved sleep quality Improved perceived health status |
| Knauth and Hornberger, 1998 [86] | 90 | Sex not reported E1—35.6 years C1—39.8 years E2—34.1 years C2—35.8 years | Steel industry employees | Rotating shift work | (El) changed from a discontinuous weekly backward-rotating to a quicker forward-rotating shift system (E2) first worked in a weekly backward-rotating and then in a quicker forward-rotating shift system | 10 months | Subjective sleep duration (questionnaire) Subjective sleep quality (questionnaire) | No significant differences |
| Kobayashi et al., 1997 [87] | 12 | M = 0 F = 12 24.8 years | Nurses | Rotating shift work | Change from full-day shift to half-day shift before night shift | 3 days | Objective sleep duration activity (actigraphy) | Increased objective sleep duration |
| Lowden et al., 1998 [88] | 34 | M = 30 F = 4 34.0 years | Chemical plant employees | Rotating shift workers | Change from rotating 3 shift (8 h) to a 2 shift (12 h) schedule | 10 months | Objective sleep duration (actigraphy) Objective sleep efficiency (actigraphy) Subjective sleep duration (Karolinska sleep diary) Subjective sleep quality (Karolinska sleep diary) Perceived health status (questionnaire) | Improved subjective sleep quality |
| Mitchell et al., 1999 [89] | 27 | M = 27 F = 0 8 h = 43.8 years 12 h = 44.3 years | Power station employees | Rotating shift work | Change from 8 to 12 h shifts | 10 months | Subjective sleep duration (sleep dairy) Subjective sleep quality (sleep diary) | Increased subjective sleep duration Improved subjective sleep quality |
| Orth Goomer, 1983 [90] | 45 | M = 45 F = 0 Group 1 = 30.4 years Group 2 = 30.8 years | Police officers | Rotating shift work | Change from backward rotation to forward rotation | 8 week crossover | Blood pressure Cholesterol (not reported) Serum glucose Subjective sleep duration (post-sleep assessment) Subjective sleep quality (post-sleep assessment) Tobacco smoking (questionnaire) Perceived health status (questionnaire) | Systolic blood pressure decreased Lowered serum glucose Increased subjective sleep duration for night sleeps Improved subjective sleep quality for night sleeps Improved perceived health status |
| Peacock et al., 1983 [91] | 75 | Sex not reported 32.8 years | Police officers | Rotating shift work | Change from 8 h 12 day shift cycle to a 12 h 8 day system | 6 months | Blood pressure Subjective sleep duration (questionnaire) Subjective sleep quality (questionnaire) | Blood pressure decreased Increased subjective sleep duration Improved subjective sleep quality |
| Rosa et al., 1996 [92] | 208 | M = 190 F = 28 Young = 31.5 years Older = 50.0 years | Steel mill employees | Rotating shift work | Delaying shift start times by one hour | 4 months | Objective sleep duration (actigraphy) Objective sleep quality (actigraphy) Subjective sleep duration (sleep diary) Subjective sleep quality (sleep diary) | Increased objective sleep duration on morning shift Increased subjective sleep duration on morning and night shift Deteriorated subjective sleep quality for evening and night shifts |
| Smith et al., 1998 [93] | 72 | M = 72 F = 0 39.1 years | Sewerage treatment plant employees | Rotating shift work | Change from slowly forward-rotating three shift (8 h) to continuous two shift (12 h) | Subjective sleep duration (sleep diary) Subjective sleep quality (sleep diary) | Improved subjective sleep quality for day sleep | |
| Totterdell et al., 1992 [94] | 71 | Sex not reported Control = 29.5 years Intervention = 34.2 years | Police officers | Rotating shift work | Change from 8 h shifts with seven consecutive shifts to 8 h night shift and 10 h day | 6 months | Subjective sleep duration (sleep diary) Subjective sleep quality (sleep diary) | Increased subjective sleep duration |
| Viitasalo et al., 2008 [95] | 84 | M = 84 F = 0 Rapidly forward-rotating = 47.0 years Flexible shift system = 37.0 years Control = 44.0 years | Maintenance employees | Rotating shift work | (I1) Change from backward-rotating to rapidly forward-rotating shift system (I2) Change from backward-rotating to more flexible system | 7–8 months | Blood pressure BMI Blood lipids (TC, HDL-C, LDL-C) Blood glucose (fasting glucose) Self-report physical activity (International Physical Activity Questionnaire) Alcohol consumption (questionnaire) Nutritional intake (questionnaire) Subjective sleep quality (Basic Nordic Sleep Questionnaire) | (I1) Systolic blood pressure increased (12) Systolic blood pressure decreased |
| Watanabe et al., 2004 [96] | 30 | Sex not reported Single = 24.8 years Married = 32.5 years | Nurses | Rotating shift work | Change to a half day before night shift | 4 day crossover | Objective sleep duration (actigraphy) Subjective sleep duration (sleep diary) | Increased objective sleep duration |
| Williamson et al., 1994 [97] | 18 | Sex not reported 23.8 years | Computer operators | Rotating shift work | Change from 8 h irregular roster to 12 h regular roster | 12 months | Subjective sleep duration (sleep diary) Subjective sleep quality (sleep diary) | Increased subjective sleep duration after day shift and rest days Decreased subjective sleep duration following night shift |
| Williamson and Sanderson, 1986 [98] | 16 | Sex and age not reported | Controllers of emergency service | Rotating shift work | Change from weekly rotation 3 shift (7 days of same shift) to rapidly rotating roster of shifts with no more than three consecutive night shifts | 5 months | Tobacco use (interview) Nutritional intake (food diary) Subjective sleep duration (sleep diary) Subjective sleep quality (sleep diary) | Improved subjective sleep quality |
| Yamada et al., 2001 [99] | 205 | M = 205 F = 0 Intervention group = 31.1 years Control group = 32.8 | Clean room employees | Rotating shift work | Change from 8 h shift to 12 h shift | 12 months | Blood pressure BMI | Significantly increased BMI |
| Author Year | Sample Size | Sample Characteristics (Sex, Mean Age) | Occupation | Type of Shift Work at Baseline | Intervention Detail | Intervention Duration | Outcome (Measurement Used) | Results |
|---|---|---|---|---|---|---|---|---|
| Arora et al., 2007 [100] | 58 | Not reported | Medical interns | On-call rotating shift work | SAFER program 1 h lecture on Sleep, Alertness, and Fatigue Education in Residency | SAFER lecture = 60–90 min Intervention measurement = 1 month | Objective sleep (actigraphy) | No significant changes |
| Elliot et al., 2007 [101] | 599 | M = 579 F = 20 41.0 years | Firefighters | Rotating shifts | (I1) team-centred curriculum; leader ran 112 45 min team sessions using workbooks (I2) individual-centred motivational interviewing; | (I1) 11 × 45 min sessions (I2) 4 sessions Total study period = 12 months | BMI Physical activity (questionnaire) Nutritional Intake (questionnaire) Perceived health status (Modified RAND 36-Item Short-Form Health Survey) | (I1) Increased fruit and vegetable consumption Improved perceived health status (I2) Increased fruit and vegetable consumption Improved perceived health status |
| MacKinnon et al., [102] Follow up of Elliot et al., 2007 | 127 | Not reported | Firefighters | Rotating shifts | Four-year follow up: (I1) team-centred curriculum; leader ran 112 45 min team sessions using workbooks (i2) individual-centred motivational interviewing | Four-year follow up | BMI Physical activity (questionnaire) Nutritional Intake (questionnaire) Perceived health status (Modified RAND 36-Item Short-Form Health Survey) | Improvements were not sustained at follow up |
| Harma et al., 1988 [103] | 75 | M = 0 F = 75 Training = 34.6 Control = 35.7 | Nurses and nurses′ aids | Rotating shift work | Controlled physical activity training. Weekly training sessions (2–6 per week) were provided = | 4 months | Subjective sleep quality (questionnaire) Subjective sleep duration (questionnaire) | Increased subjective sleep duration following evening shifts |
| Holbrook et al., 1994 [104] | 38 | M = 31 F = 7 M = 37.0 years F = 35.0 years | Police officers | Rotating shift work | Education of sleep hygiene practices | Education session = 1 h Total study period = 1 month | Subjective sleep quality (post-sleep inventory) | No significant changes |
| Kerin and Aguirre, 2005 [105] | Not reported | Not reported | Mine workers | Not reported | Workers and their spouses/partners attended the “Managing A Shiftwork Lifestyle” training workshop. Provided information on the solutions to the special challenges of shift work | 6 weeks | Subjective sleep duration (sleep/wake logs) | Increased subjective sleep duration |
| Lee et al., 2013 [106] | 21 | M = 1 F = 20 45.5 years | Nurses | Night shift | Home-based cognitive-behavioural intervention—the Sleep Enhancement Training System for Shift Workers (SETS-SW) | 8 week crossover | Objective sleep duration (actigraphy) Sleep efficiency (actigraphy) Subjective sleep quality (Pittsburgh Sleep Quality Index and General Sleep Disturbance) | Improved subjective sleep quality |
| Leedo et al., 2017 [107] | 16 | Sex not reported 40.9 years | Healthcare | Evening, night or weekend | Healthy meals and water provided at work | 8 week crossover | BMI Self-report nutritional intake (dietary record) | Increased water intake |
| Lim et al., 2005 [108] | 30 | M = 30 F = 0 Control = 58.3 Intervention = 56.8 | Not reported | Night shift | The experimental group performed an intermittent exercise at 10 min bouts (30 min per day), three days a week during 10 weeks | 10 weeks | Blood Pressure BMI | No significant changes |
| Matsugaki et al., 2017 [109] | 29 | M = 0 F = 29 Supervised = 25.3 years Voluntary = 24.7 years | Nurses | Not reported | The supervised exercise group (SG; participants exercised under the supervision of a physical therapist (PT)) and the voluntary exercise group (VG; participants exercised without supervision). The study participants were asked to exercise twice/week for 12 weeks for 24 sessions | 12 weeks | Blood pressure BMI Cholesterol (TC, LDL-C, HDL-C) | HDL-C increased |
| Morgan et al., 2011 [110] | 110 | M = 110 F = 0 44.4 years | Aluminium plant workers | Rotating shift work | The 3 month program involved one information session, program booklets, group-based financial incentives and an online component weight loss | 14 weeks | Blood Pressure BMI Physical activity (Godin Leisure-Time Exercise Questionnaire) Dietary variables (questionnaire) | Blood pressure decreased Decreased BMI Increased physical activity Decreased sugary drink intake |
| Neil-Sztramko et al., 2017 [111] | 20 | M = 0 F = 20 42.2 years | 17 = nurse/care aid 1 = service industry 1 = airline industry 1 = communications | 19 = rotating, 1 = permanent night | Physical activity education 12 weekly sessions with physical activity coach (via phone) | 12 weeks | BMI Physical Activity (actigraphy) Subjective sleep duration (Pittsburgh Sleep Quality Index) Subjective sleep quality (Pittsburgh Sleep Quality Index) Perceived health status (RAND 36-Item Short-Form Health Survey) | Decreased BMI Increased physical activity |
| Pylkkönen et al., 2018 [112] | 49 | Sex not reported Intervention = 37.9 years Control = 37.8 years | Truck drivers | Rotating shift work | The intervention group received a 3.5 h alertness management training followed by a two-month consultation period and motivational self-evaluation tasks two and 4–5 months after the training | 4–5 months | Objective sleep duration (actigraphy) Subjective sleep duration (sleep log) | No significant changes |
| Smith-Coggins et al., 1997 [113] | 6 | M = 6 F = 0 34.0 years | Physicians in Emergency Department | Rotating shift work | Education session on sleep and sleep hygiene | 1 month | Objective sleep duration (PSG) Subjective sleep duration (sleep diary) Subjective sleep quality (sleep diary) | No significant changes |
| Sullivan et al., 2017 [114] | 1189 | M = 1173 F = 16 43.6 years | US firefighters | Rotating shift work (including extended shifts) | Sleep hygiene education | 1 year | Subjective sleep duration (questionnaire) Perceived health status (questionnaire) | No significant changes |
| Van Drongelen et al., 2014 [115] | 502 | M = 468 F = 34 40.9 years | Airline pilots | Not reported | The intervention group was given access to both the MORE Energy mobile application (app) with tailored advice and a website with background information. The control group was directed to a website with standard information about fatigue | 3 months | Tobacco smoking (questionnaire) Physical activity (questionnaire) Alcohol consumption (questionnaire) Nutritional intake (questionnaire) Subjective sleep quality (Jenkins Sleep Scale) Subjective sleep duration (Pittsburgh Sleep Quality Index) Nutritional intake (questionnaire) Perceived health status (RAND 36-Item Short-Form Health Survey) | Increased physical activity Improved subjective sleep quality |
| Yeung et al., 2011 [116] | 16 | M = 7 F = 9 35.44 years | Manufacturing = 6 Customer service/management = 4 Nursing = 3 Public service = 1 | Early morning shift | Participants advanced sleep time to 10 h before start of shift | 2 week crossover | Objective sleep duration (actigraphy) Objective sleep efficiency (actigraphy) Subjective sleep duration (sleep diary) Subjective sleep quality (sleep diary) | Increased objective sleep duration Increased subjective sleep duration Improved subjective sleep quality |
| Author Year | Sample Size | Sample Characteristics (Sex, Mean Age) | Occupation | Type of Shift Work at Baseline | Intervention Detail | Intervention Duration | Outcome Measure (Measurement Used) | Results |
|---|---|---|---|---|---|---|---|---|
| Bjorvatn et al., 1999 [117] | 7 | M = 7 F = 0 38.9 years | Oil platform workers | Rotating shift work | Light box 10,000 lux for 30 min per day | 4 nights offshore bright light 4 nights onshore bright light Total study period = 3 weeks | Subjective sleep duration (Karolinska sleep diary) Subjective sleep quality (Karolinska sleep/wake diary) | No significant changes |
| Bjorvatn et al., 2007 [118] | 17 | M = 16 F = 1 42.0 years | Oil platform workers | Rotating shift work | (i) Light box 10,000 lux for 30 min 4 night shifts and 4 day shifts (ii) Placebo capsule | Light period = 4 days on night shift 4 days of day shift Total study period = 6 weeks | Objective sleep duration (actigraphy) Objective sleep efficiency (actigraphy) Subjective sleep duration (sleep diary) Subjective sleep quality (sleep diary) | Reduction in objective sleep onset latency for night shift |
| Boivin et al., 2012 [119] | 15 | M = 6 F = 9 41.8 years | Nurses | Night shift | Intermittent bright light 3243 lux during first 6 h of each night shift Wore shaded goggles for 2 h following night shift | 10 days | Objective sleep duration (nightcap or PSG) Objective sleep efficiency (nightcap or PSG) | Increased objective sleep duration |
| Budnick et al., 1995 [120] | 13 | M = 11 F = 2 Median age = 35.0 years | Industrial workers | Rotating shift work | Scheduled bright light (6000–12,000 lux) | 3 months | Subjective sleep duration (sleep diary) Subjective sleep quality (sleep diary) | No significant changes |
| Costa et al., 1993 [121] | 15 | M = 0, F = 15 23.4 years | Nurses | Rotating shift work | Two consecutive night shifts exposed to short periods (4 × 20 min) of bright light (2350 Iux) | 2 days control 2 days bright light | Subjective sleep duration (sleep diary) | Decreased subjective sleep duration between night shifts |
| Jensen et al., 2016 [122] | 113 | Sex not reported Intervention group = median age 43.0 years Control group = median age 42.0 years | Nurses | Rotating shift work | Intervention group worked in dynamic lighting designed to mimic natural daylight changes | 10 days | Objective sleep duration (actigraphy) Sleep efficiency (actigraphy) Subjective sleep duration (sleep diary) Subjective sleep quality (sleep diary) | No significant changes |
| Lowden et al., 2004 [123] | 18 | M = 17 F = 1 36.2 years | Industrial truck production | Rotating shift work | 20 min bright light (2500 lux) during breaks | 4 week control 4 week bright light | Objective sleep duration (actigraphy) Sleep efficiency (actigraphy) Subjective sleep duration (sleep diary) Subjective sleep quality (sleep diary) | Increased objective sleep duration |
| Olson et al., 2020 [124] | 33 | M = 7 F = 26 32.7 years | Nurses | Rotating shift work | Light box (5500 lux) 40 min of light prior to night shift Sunglasses after night shift Sleep mask for sleeping after night shift | 2 week control 2 week intervention | Subjective sleep duration (12 h sleep diary) Subjective sleep quality (Sleep Quality Scale) Objective physical activity (pedometer) Alcohol consumption (logbook) | Increased subjective sleep duration Improved subjective sleep quality |
| Sasseville et al., 2009 [125] | 28 | M = 13 F = 15 Summer = 42.4 years Winter = 37.2 years | Canada Post′s distribution centre | Fixed night workers | Blue-blockers glasses; (a) Summer group: just before leaving the workplace (b) Winter group: 2 h before the end of night shift | 2 week control 2 week intervention | Objective sleep duration (actigraphy) Sleep efficiency (actigraphy) | Increased objective sleep duration Improved sleep efficiency |
| Sasseville et al., 2010 [126] | 4 | M = 4, F = 0 44.8 years | Sawmill workers | Rotating shift work | Blue-green light (200 lux) in workplace during shift Blue-blockers had to be worn outside from the end of the night shift until 16:00 h | 1 week control 1 week light night shift 1 week light day shift | Objective sleep duration (actigraphy) Sleep efficiency (actigraphy) | Increased objective sleep duration |
| Simons et al., 2018 [127] | 10 | M = 3 F = 7 34.0 years | Intensive Care Unit nurses | Rotating shift workers (only on day shift for experiment) | Ceiling mounted dynamic light (1700 lux) in patients’ room | 4 day control 4 day dynamic light | Subjective sleep quality (daily questionnaire) Subjective sleep duration (daily questionnaire) Perceived health status (World Health Organisation Quality of Life Short Form) | Deterioration in perceived health status |
| Tanaka et al., 2011 [128] | 61 | M = 0 F = 61 29.7 years | Nurses | Rotating shift work | Bright light (6666 lux) for 10 min prior to work in workplace | 4 week control 4 week bright light | Alcohol consumption (self-report times per week) Subjective sleep quality (post-sleep visual analogue scale) | Improved subjective sleep quality |
| Thorne et al., 2010 [129] | 10 | M = 10 F = 0 Summer = 46.0 years Winter = 49.0 years | Offshore | Fixed night workers | Light box (3000 lux) and light-blocking glasses from waking until light treatment | 21 days | Objective sleep duration (actigraphy) Objective sleep efficiency (actigraphy) Subjective sleep duration (sleep diary) Subjective sleep quality (sleep diary) | Increased objective sleep duration Improved sleep efficiency Decreased subjective sleep quality |
| Yoon et al., 2002 [130] | 12 | M = 0 F = 12 Age range = 21–24 years | Nurses | Night shift | (i) Room light (ii) Light box (4000–6000 lux) intermittent for four hours (iii) Light box with sunglasses worn next morning | 4 days room light 4 days bright light 4 days light box with sunglasses | Objective sleep duration (actigraphy) Sleep efficiency (actigraphy) Subjective sleep duration (sleep diary) Subjective sleep quality (sleep diary) | (ii) Increased objective sleep duration Improved sleep efficiency (iii) Increased objective sleep duration Improved sleep efficiency |
| Author Year | Sample Size | Sample Characteristics (Sex, Mean Age) | Occupation | Type of Shift Work at Baseline | Intervention Detail | Intervention Duration | Outcome Measure (Measurement Used) | Results |
|---|---|---|---|---|---|---|---|---|
| Chang et al., 2017 [131] | 50 | M = 0 F = 50 Intervention = 28.36 years Control = 30.55 years | Nurses | Rotating shift work | Intervention = 1 h lay down + 25 min aromatherapy massage once a week Control = once a week/4 times total 1 h lay down + music (no massage) | 4 weeks | Sleep quality (Pittsburgh Sleep Quality Index) Objective sleep duration (Ezsleep—Electro-cardiogram signal collector) | Increased subjective sleep quality |
| Fazeli et al., 2020 [132] | 12 | M = 3 F = 9 Median age = 28.0 | Medical residents | Rotating shift work | Intervention = 30 min massage Control = 30 min reading in chair | At least 18 days | Blood pressure | No significant change in intervention Blood pressure decreased in control group |
| McElligott et al., 2003 [133] | 24 | M = 3 F = 19 Control = 38.0 years Intervention = 34.0 years | Nurse | Rotating shift work | Touch therapy | 4 weeks | Blood pressure | No significant result |
| Zadeh et al., 2018 [134] | 36 | M = 14, F = 22 Age 34.2 years | Nurse | Not reported | Transcutaneous Electrical Acupoint Stimulation (TEAS) (I1) Real TEAS points (I2) Sham points (I3) No intervention | 4 weeks | Subjective sleep quality (Pittsburgh Sleep Quality Index) | (I1) Significantly improved subjective sleep quality (I2) Improved subjective sleep quality |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Crowther, M.E.; Ferguson, S.A.; Vincent, G.E.; Reynolds, A.C. Non-Pharmacological Interventions to Improve Chronic Disease Risk Factors and Sleep in Shift Workers: A Systematic Review and Meta-Analysis. Clocks & Sleep 2021, 3, 132-178. https://0-doi-org.brum.beds.ac.uk/10.3390/clockssleep3010009
Crowther ME, Ferguson SA, Vincent GE, Reynolds AC. Non-Pharmacological Interventions to Improve Chronic Disease Risk Factors and Sleep in Shift Workers: A Systematic Review and Meta-Analysis. Clocks & Sleep. 2021; 3(1):132-178. https://0-doi-org.brum.beds.ac.uk/10.3390/clockssleep3010009
Chicago/Turabian StyleCrowther, Meagan E, Sally A Ferguson, Grace E Vincent, and Amy C Reynolds. 2021. "Non-Pharmacological Interventions to Improve Chronic Disease Risk Factors and Sleep in Shift Workers: A Systematic Review and Meta-Analysis" Clocks & Sleep 3, no. 1: 132-178. https://0-doi-org.brum.beds.ac.uk/10.3390/clockssleep3010009