Efficacy and Safety of Dor Fundoplication in Patients with Severe Gastroparesis and Refractory Gastroesophageal Reflux Disease



Abstract
:1. Introduction
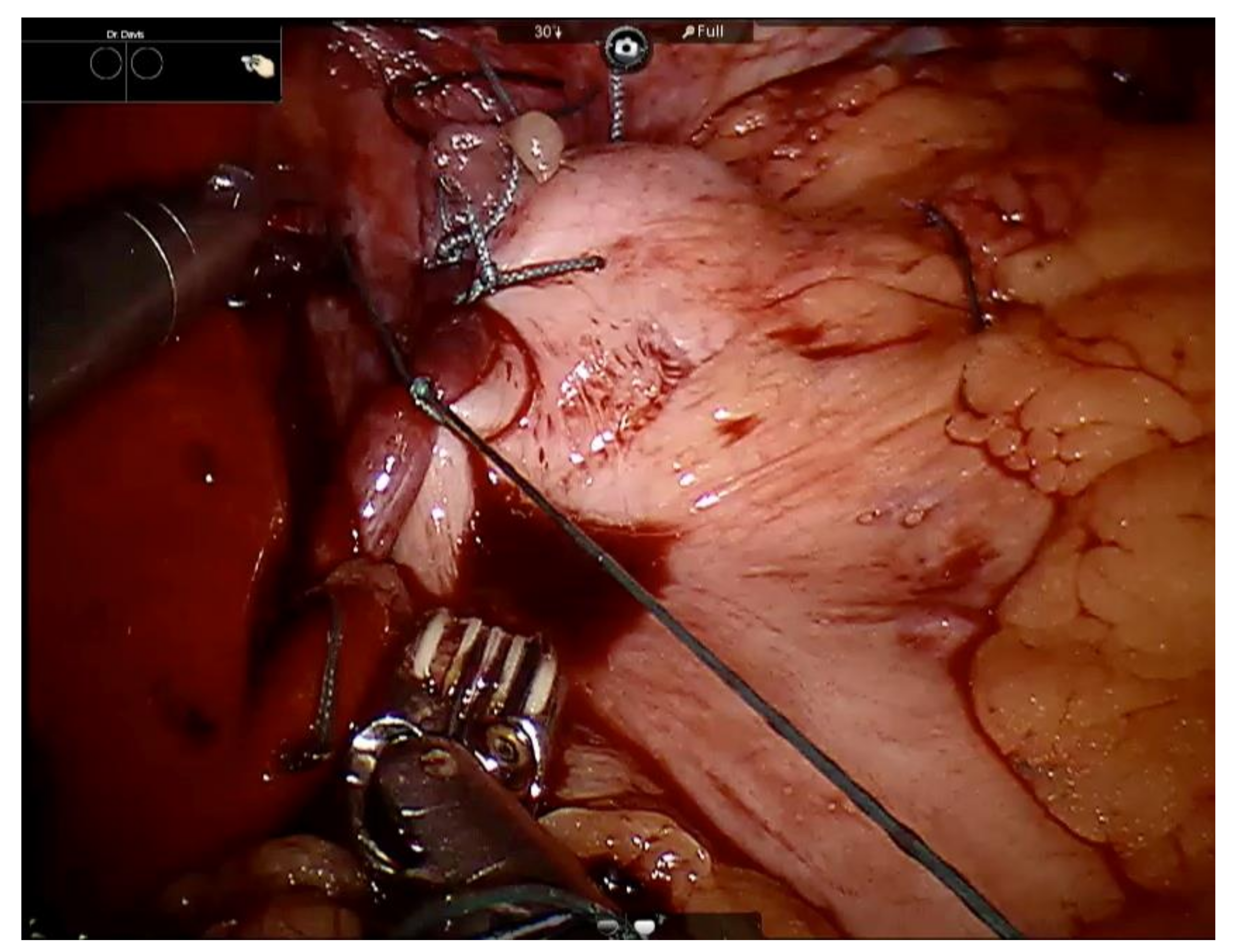
The Surgical Technique
2. Results
3. Discussion
Limitations
4. Materials and Methods
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Katz, P.O.; Gerson, L.B.; Vela, M.F. Guidelines for the diagnosis and management of gastroesophageal reflux disease. Am. J. Gastroenterol. 2013, 108, 308–328. [Google Scholar] [CrossRef] [PubMed]
- Parkman, H.P.; Hasler, W.L.; Fisher, R.S. American Gastroenterological Association technical review on the diagnosis and treatment of gastroparesis. Gastroenterology 2004, 127, 1592–1622. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Loganathan, P.; Gajendran, M.; McCallum, R.W. Clinical Manifestation and Natural History of Gastroparesis. Gastrointest. Endosc. Clin. 2019, 29, 27–38. [Google Scholar] [CrossRef] [PubMed]
- Du, X.; Wu, J.M.; Hu, Z.W.; Wang, F.; Wang, Z.G.; Zhang, C.; Yan, C.; Chen, M.P. Laparoscopic Nissen (total) versus anterior 180° fundoplication for gastro-esophageal reflux disease. Medicine 2017, 96, e8085. [Google Scholar] [CrossRef] [PubMed]
- Shada, A.L.; Dunst, C.M.; Pescarus, R.; Speer, E.A.; Cassera, M.; Reavis, K.M.; Swanstrom, L.L. Laparoscopic pyloroplasty is a safe and effective first-line surgical therapy for refractory gastroparesis. Surg. Endosc. 2016, 30, 1326–1332. [Google Scholar] [CrossRef] [PubMed]
- Sarosiek, I.; Davis, B.; Eichler, E.; McCallum, R.W. Surgical approaches to treatment of gastroparesis: Gastric electrical stimulation, pyloroplasty, total gastrectomy and enteral feeding tubes. Gastroenterol. Clin. 2015, 44, 151–167. [Google Scholar] [CrossRef] [PubMed]
- Thompson, S.K.; Watson, D.I. What is the best anti-reflux operation? All fundoplications are not created equal. World J. Surg. 2015, 39, 997–999. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Watson, D.I.; Liu, J.F.; Devitt, P.G.; Game, P.A.; Jamieson, G.G. Outcome of laparoscopic anterior 180-degree partial fundoplication for gastroesophageal reflux disease. J. Gastrointest. Surg. 2000, 4, 486–492. [Google Scholar] [CrossRef]
- Khajanchee, Y.S.; Dunst, C.M.; Swanstrom, L.L. Outcomes of Nissen fundoplication in patients with gastroesophageal reflux disease and delayed gastric emptying. Arch. Surg. 2009, 144, 823–828. [Google Scholar] [CrossRef] [PubMed]
- Revicki, D.A.; Rentz, A.M.; Tack, J.; Stanghellini, V.; Talley, N.J.; Kahrilas, P.; De La Loge, C.; Trudeau, E.; Dubois, D. Responsiveness and interpretation of a symptom severity index specific to upper gastrointestinal disorders. Clin. Gastroenterol. Hepatol. 2004, 2, 769–777. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Pre-op | Post-op | |||||||
|---|---|---|---|---|---|---|---|---|
| Patient/Symptoms | DHB | NHB | DR | NR | DHB | NHB | DR | NR |
| Patient 1 | 1 | 4 | 4 | 4 | 1 | 1 | 0 | 0 |
| Patient 2 | 1 | 2 | 2 | 3 | 2 | 2 | 2 | 2 |
| Patient 3 | 4 | 4 | 5 | 5 | 4 | 4 | 3 | 4 |
| Patient 4 | 5 | 5 | 5 | 5 | 4 | 4 | 1 | 1 |
| Patient 5 | 2 | 2 | 2 | 2 | 1 | 1 | 2 | 2 |
| Patient 6 | 3 | 3 | 4 | 4 | 3 | 3 | 4 | 4 |
| Mean Score | 2.6 | 3.4 | 3.6 | 3.8 | 2.5 | 2.5 | 2 | 2.2 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ishak, A.; Al-Bayati, I.; Davis, B.; Sarosiek, I.; McCallum, R.W. Efficacy and Safety of Dor Fundoplication in Patients with Severe Gastroparesis and Refractory Gastroesophageal Reflux Disease. Gastrointest. Disord. 2020, 2, 134-139. https://0-doi-org.brum.beds.ac.uk/10.3390/gidisord2020013
Ishak A, Al-Bayati I, Davis B, Sarosiek I, McCallum RW. Efficacy and Safety of Dor Fundoplication in Patients with Severe Gastroparesis and Refractory Gastroesophageal Reflux Disease. Gastrointestinal Disorders. 2020; 2(2):134-139. https://0-doi-org.brum.beds.ac.uk/10.3390/gidisord2020013
Chicago/Turabian StyleIshak, Asaad, Ihsan Al-Bayati, Brian Davis, Irene Sarosiek, and Richard W. McCallum. 2020. "Efficacy and Safety of Dor Fundoplication in Patients with Severe Gastroparesis and Refractory Gastroesophageal Reflux Disease" Gastrointestinal Disorders 2, no. 2: 134-139. https://0-doi-org.brum.beds.ac.uk/10.3390/gidisord2020013