
First Detection of Methanogens in Orthopedic Prosthesis Infection: A Four-Case Founding Series

Abstract
:1. Introduction
2. Results
2.1. Routine Bacteriological Investigations
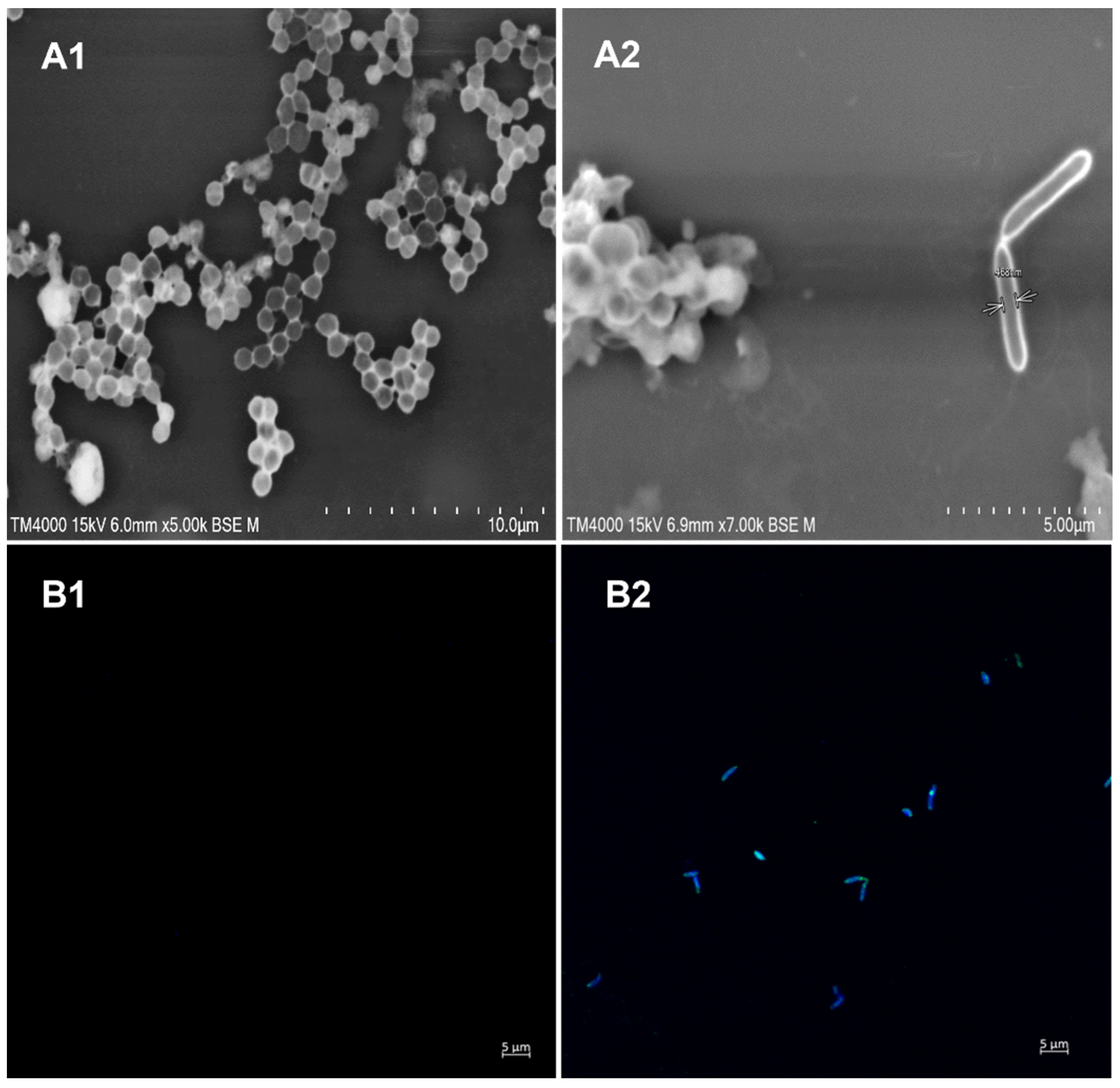
2.2. Methanogen Investigations
2.3. Medical History
2.3.1. Case 1
2.3.2. Case 2
2.3.3. Case 3
2.3.4. Case 4
3. Discussion
4. Materials and Methods
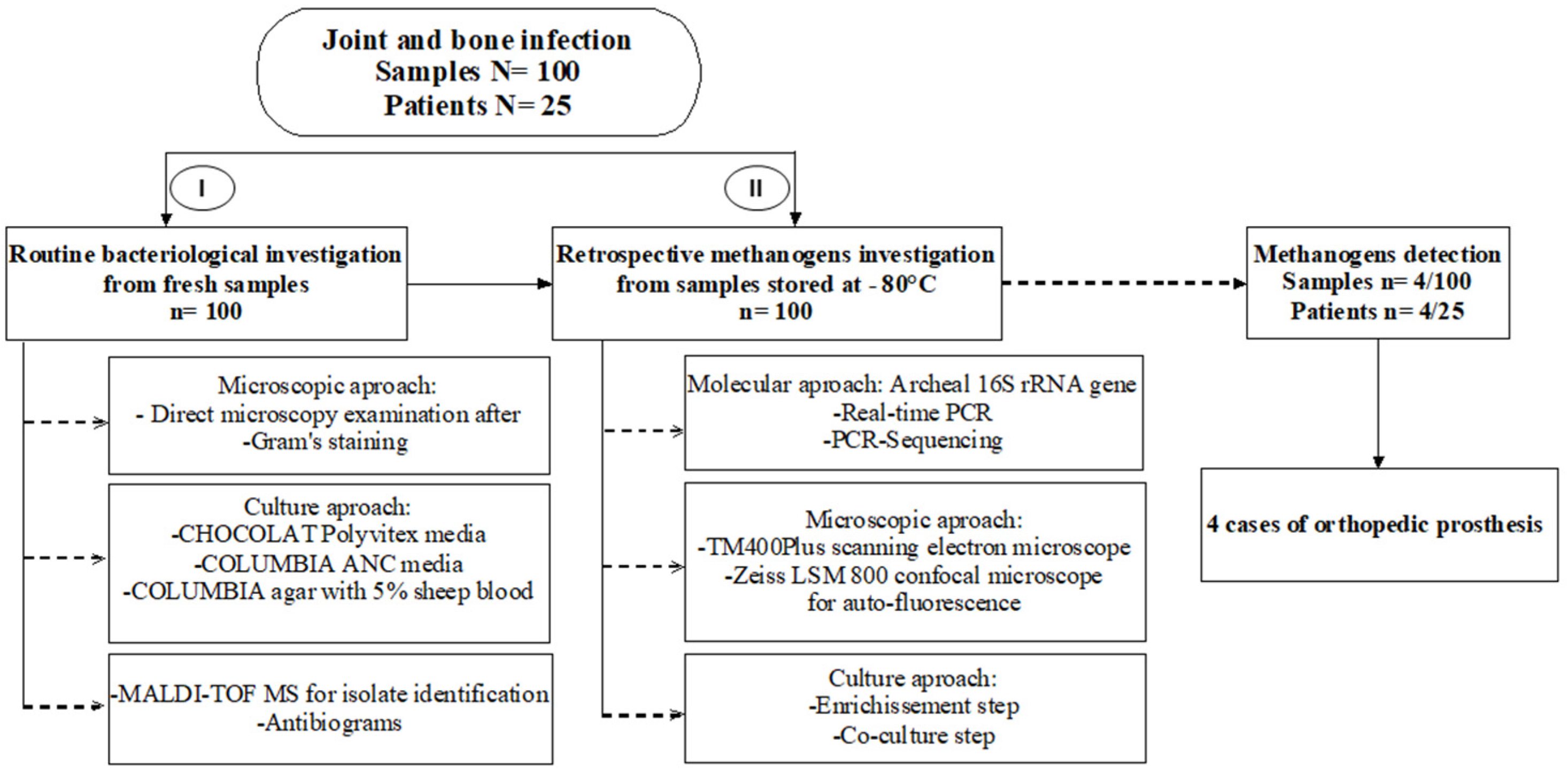
4.1. Patients and Study Design
4.2. Routine Bacteriological Investigations
4.3. Methanogen PCR-Based Identification
4.4. Microscopic Examinations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Pulido, L.; Ghanem, E.; Joshi, A.; Purtill, J.J.; Parvizi, J. Periprosthetic joint infection: The incidence, timing, and predisposing factors. Clin. Orthop. Relat. Res. 2008, 466, 1710–1715. [Google Scholar] [CrossRef] [Green Version]
- Pedersen, A.B.; Svendsson, J.E.; Johnsen, S.P.; Riis, A.; Overgaard, S. Risk factors for revision due to infection after primary total hip arthroplasty. A population-based study of 80,756 primary procedures in the Danish Hip Arthroplasty Registry. Acta Orthop. 2010, 81, 542–547. [Google Scholar] [CrossRef]
- Tibrewal, S.; Malagelada, F.; Jeyaseelan, L.; Posch, F.; Scott, G. Single-stage revision for the infected total knee replacement: Results from a single centre. Bone Jt. J. 2014, 96, 759–764. [Google Scholar] [CrossRef] [PubMed]
- Mahomed, N.N.; Barrett, J.A.; Katz, J.N.; Phillips, C.B.; Losina, E.; Lew, R.A.; Guadagnoli, E.; Harris, W.H.; Poss, R.; Baron, J.A. Rates and outcomes of primary and revision total hip replacement in the United States medicare population. J. Bone Jt. Surg. Am. 2003, 85, 27–32. [Google Scholar] [CrossRef] [PubMed]
- Spitzmüller, R.; Gümbel, D.; Güthoff, C.; Zaatreh, S.; Klinder, A.; Napp, M.; Bader, R.; Mittelmeier, W.; Ekkernkamp, A.; Kramer, A.; et al. Duration of antibiotic treatment and risk of recurrence after surgical management of orthopaedic device infections: A multicenter case-control study. BMC Musculoskelet. Disord. 2019, 20, 184. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parvizi, J.; Zmistowski, B.; Berbari, E.F.; Bauer, T.W.; Springer, B.D.; Della Valle, C.J.; Garvin, K.L.; Mont, M.A.; Wongworawat, M.D.; Zalavras, C.G. New definition for periprosthetic joint infection: From the Workgroup of the Musculoskeletal Infection Society. Clin. Orthop. Relat. Res. 2011, 469, 2992–2994. [Google Scholar] [CrossRef] [Green Version]
- Levy, P.Y.; Fournier, P.E.; Fenollar, F.; Raoult, D. Systematic PCR detection in culture-negative osteoarticular infections. Am. J. Med. 2013, 126, 1143.e25–1143.e33. [Google Scholar] [CrossRef]
- Osmon, D.R.; Berbari, E.F.; Berendt, A.R.; Lew, D.; Zimmerli, W.; Steckelberg, J.M.; Rao, N.; Hanssen, A.; Wilson, W.R.; Infectious Diseases Society of America. Infectious Diseases Society of America. Diagnosis and management of prosthetic joint infection: Clinical practice guidelines by the Infectious Diseases Society of America. Clin. Infect. Dis. 2013, 56, e1–e25. [Google Scholar] [CrossRef] [Green Version]
- Fink, B.; Schuster, P.; Braun, R.; Tagtalianidou, E.; Schlumberger, M. The diagnostic value of routine preliminary biopsy in diagnosing late prosthetic joint infection after hip and knee arthroplasty. Bone Jt. J. 2020, 102, 329–335. [Google Scholar] [CrossRef]
- Widmer, A.F. New developments in diagnosis and treatment of infection in orthopedic implants. Clin. Infect. Dis. 2001, 1, 33. [Google Scholar] [CrossRef]
- Trampuz, A.; Zimmerli, W. Prosthetic joint infections: Update in diagnosis and treatment. Swiss Med. Wkly. 2005, 135, 243–251. [Google Scholar] [PubMed]
- Toms, A.D.; Davidson, D.; Masri, B.A.; Duncan, C.P. The management of peri-prosthetic infection in total joint arthroplasty. J. Bone Jt. Surg. Br. 2006, 88, 149–155. [Google Scholar] [CrossRef] [PubMed]
- Tunney, M.M.; Patrick, S.; Curran, M.D.; Ramage, G.; Hanna, D.; Nixon, J.R.; Gorman, S.P.; Davis, R.I.; Anderson, N. Detection of prosthetic hip infection at revision arthroplasty by immunofluorescence microscopy and PCR amplification of the bacterial 16S rRNA gene. J. Clin. Microbiol. 1999, 37, 3281–3290. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brown, T.S.; Petis, S.M.; Osmon, D.R.; Mabry, T.M.; Berry, D.J.; Hanssen, A.D.; Abdel, M.P. Periprosthetic Joint Infection with Fungal Pathogens. J. Arthroplast. 2018, 33, 2605–2612. [Google Scholar] [CrossRef] [PubMed]
- Bapteste, E.; Brochier, C.; Boucher, Y. Higher-level classification of the Archaea: Evolution of methanogenesis and methanogens. Archaea 2005, 1, 353–363. [Google Scholar] [CrossRef] [Green Version]
- Liu, Y.; Whitman, W.B. Metabolic, phylogenetic, and ecological diversity of the methanogenic archaea. Ann. N. Y. Acad. Sci. 2008, 1125, 171–189. [Google Scholar] [CrossRef]
- Dridi, B.; Henry, M.; El Khéchine, A.; Raoult, D.; Drancourt, M. High prevalence of Methanobrevibacter smithii and Methanosphaera stadtmanae detected in the human gut using an improved DNA detection protocol. PLoS ONE 2009, 4, e7063. [Google Scholar] [CrossRef]
- Koskinen, K.; Pausan, M.R.; Perras, A.K.; Beck, M.; Bang, C.; Mora, M.; Schilhabel, A.; Schmitz, R.; Moissl-Eichinger, C. First Insights into the Diverse Human Archaeome: Specific Detection of Archaea in the Gastrointestinal Tract, Lung, and Nose and on Skin. mBio 2017, 8, e00824-17. [Google Scholar] [CrossRef] [Green Version]
- Sieber, J.R.; McInerney, M.J.; Gunsalus, R.P. Genomic insights into syntrophy: The paradigm for anaerobic metabolic cooperation. Annu. Rev. Microbiol. 2012, 66, 429–452. [Google Scholar] [CrossRef]
- Brugère, J.F.; Borrel, G.; Gaci, N.; Tottey, W.; O’Toole, P.W.; Malpuech-Brugère, C. Archaebiotics: Proposed therapeutic use of archaea to prevent trimethylaminuria and cardiovascular disease. Gut Microbes 2014, 5, 5–10. [Google Scholar] [CrossRef] [Green Version]
- Camara, A.; Konate, S.; Tidjani Alou, M.; Kodio, A.; Togo, A.H.; Cortaredona, S.; Henrissat, B.; Thera, M.A.; Doumbo, O.K.; Raoult, D.; et al. Clinical evidence of the role of Methanobrevibacter smithii in severe acute malnutrition. Sci. Rep. 2021, 11, 5426. [Google Scholar] [CrossRef] [PubMed]
- Million, M.; Tidjani Alou, M.; Khelaifia, S.; Bachar, D.; Lagier, J.C.; Dione, N.; Brah, S.; Hugon, P.; Lombard, V.; Armougom, F.; et al. Increased Gut Redox and Depletion of Anaerobic and Methanogenic Prokaryotes in Severe Acute Malnutrition. Sci. Rep. 2016, 6, 26051. [Google Scholar] [CrossRef] [PubMed]
- Blais Lecours, P.; Marsolais, D.; Cormier, Y.; Berberi, M.; Haché, C.; Bourdages, R.; Duchaine, C. Increased prevalence of Methanosphaera stadtmanae in inflammatory bowel diseases. PLoS ONE 2014, 9, e87734. [Google Scholar] [CrossRef] [PubMed]
- Ghavami, S.B.; Rostami, E.; Sephay, A.A.; Shahrokh, S.; Balaii, H.; Aghdaei, H.A.; Zali, M.R. Alterations of the human gut Methanobrevibacter smithii as a biomarker for inflammatory bowel diseases. Microb. Pathog. 2018, 117, 285–289. [Google Scholar] [CrossRef]
- Soares, A.C.; Lederman, H.M.; Fagundes-Neto, U.; de Morais, M.B. Breath methane associated with slow colonic transit time in children with chronic constipation. J. Clin. Gastroenterol. 2005, 39, 512–515. [Google Scholar] [CrossRef]
- Li, C.L.; Liu, D.L.; Jiang, Y.T.; Zhou, Y.B.; Zhang, M.Z.; Jiang, W.; Liu, B.; Liang, J.P. Prevalence and molecular diversity of Archaea in subgingival pockets of periodontitis patients. Oral Microbiol. Immunol. 2009, 24, 343–346. [Google Scholar] [CrossRef]
- Huynh, H.T.; Pignoly, M.; Nkamga, V.D.; Drancourt, M.; Aboudharam, G. The repertoire of archaea cultivated from severe periodontitis. PLoS ONE 2015, 10, e0121565. [Google Scholar] [CrossRef]
- Nkamga, V.D.; Lotte, R.; Roger, P.M.; Drancourt, M.; Ruimy, R. Methanobrevibacter smithii and Bacteroides thetaiotaomicron cultivated from a chronic paravertebral muscle abscess. Clin. Microbiol. Infect. 2016, 22, 1008–1009. [Google Scholar] [CrossRef]
- Drancourt, M.; Nkamga, V.D.; Lakhe, N.A.; Régis, J.M.; Dufour, H.; Fournier, P.E.; Bechah, Y.; Scheld, W.M.; Raoult, D. Evidence of Archaeal Methanogens in Brain Abscess. Clin. Infect. Dis. 2017, 65, 1–5. [Google Scholar] [CrossRef]
- Grine, G.; Lotte, R.; Chirio, D.; Chevalier, A.; Raoult, D.; Drancourt, M.; Ruimy, R. Co-culture of Methanobrevibacter smithii with enterobacteria during urinary infection. EBioMedicine 2019, 43, 333–337. [Google Scholar] [CrossRef] [Green Version]
- Argenson, J.N.; Arndt, M.; Babis, G.; Battenberg, A.; Budhiparama, N.; Catani, F.; Chen, F.; de Beaubien, B.; Ebied, A.; Esposito, S.; et al. Hip and Knee Section, Treatment, Debridement and Retention of Implant: Proceedings of International Consensus on Orthopedic Infections. J. Arthroplast. 2019, 34, S399–S419. [Google Scholar] [CrossRef] [PubMed]
- Chaudhary, P.P.; Conway, P.L.; Schlundt, J. Methanogens in humans: Potentially beneficial or harmful for health. Appl. Microbiol. Biotechnol. 2018, 102, 3095–3104. [Google Scholar] [CrossRef] [PubMed]
- Drancourt, M.; Djemai, K.; Gouriet, F.; Grine, G.; Loukil, A.; Bedotto, M.; Levasseur, A.; Lepidi, H.; Bou-Khalil, J.; Khelaifia, S.; et al. Methanobrevibacter smithii archaemia in febrile patients with bacteremia, including those with endocarditis. Clin. Infect. Dis. 2020, 15, ciaa998. [Google Scholar] [CrossRef] [PubMed]
- Sogodogo, E.; Fellag, M.; Loukil, A.; Nkamga, V.D.; Michel, J.; Dessi, P.; Fournier, P.-E.; Drancourt, M. Nine Cases of Methanogenic Archaea in Refractory Sinusitis, an Emerging Clinical Entity. Front. Public Health 2019, 7, 38. [Google Scholar] [CrossRef]
- Grine, G.; Drouet, H.; Fenollar, F.; Bretelle, F.; Raoult, D.; Drancourt, M. Detection of Methanobrevibacter smithii in vaginal samples collected from women diagnosed with bacterial vaginosis. Eur. J. Clin. Microbiol. Infect. Dis. 2019, 38, 1643–1649. [Google Scholar] [CrossRef]
- Miller, T.L.; Lin, C. Description of Methanobrevibacter gottschalkii sp. nov., Methanobrevibacter thaueri sp. nov., Methanobrevibacter woesei sp. nov. and Methanobrevibacter wolinii sp. nov. Int. J. Syst. Evol. Microbiol. 2002, 52, 819–822. [Google Scholar] [CrossRef] [Green Version]
- Matarazzo, F.; Ribeiro, A.C.; Feres, M.; Faveri, M.; Mayer, M.P. Diversity and quantitative analysis of Archaea in aggressive periodontitis and periodontally healthy subjects. J. Clin. Periodontol. 2011, 38, 621–627. [Google Scholar] [CrossRef]
- Efenberger, M.; Agier, J.; Pawłowska, E.; Brzezińska-Błaszczyk, E. Archaea prevalence in inflamed pulp tissues. Cent. Eur. J. Immunol. 2015, 40, 194–200. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wright, J.A.; Nair, S.P. Interaction of staphylococci with bone. Int. J. Med. Microbiol. 2010, 300, 193–204. [Google Scholar] [CrossRef] [Green Version]
- Tyner, H.; Patel, R. Propionibacterium acnes biofilm—A sanctuary for Staphylococcus aureus? Anaerobe 2016, 40, 63–67. [Google Scholar] [CrossRef]
- McDowell, A.; Patrick, S. Evaluation of nonculture methods for the detection of prosthetic hip biofilms. Clin. Orthop. Relat. Res. 2005, 437, 74–82. [Google Scholar] [CrossRef]
- Bang, C.; Schmitz, R.A. Archaea: Forgotten players in the microbiome. Emerg. Top. Life Sci. 2018, 2, 459–468. [Google Scholar] [CrossRef] [PubMed]
- Orell, A.; Fröls, S.; Albers, S.V. Archaeal biofilms: The great unexplored. Annu. Rev. Microbiol. 2013, 67, 337–354. [Google Scholar] [CrossRef] [PubMed]
- Dame-Teixeira, N.; de Cena, J.A.; Côrtes, D.A.; Belmok, A.; Dos Anjos Borges, L.G.; Marconatto, L.; Giongo, A.; Kyaw, C.M. Presence of Archaea in dental caries biofilms. Arch. Oral Biol. 2020, 110, 104606. [Google Scholar] [CrossRef] [PubMed]
- Raskin, L.; Stromley, J.M.; Rittmann, B.E.; Stahl, D.A. Group-specific 16S rRNA hybridization probes to describe natural communities of methanogens. Appl. Environ. Microbiol. 1994, 60, 1232–1240. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seng, P.; Drancourt, M.; Gouriet, F.; La Scola, B.; Fournier, P.E.; Rolain, J.M.; Raoult, D. Ongoing revolution in bacteriology: Routine identification of bacteria by matrix-assisted laser desorption ionization time-of-flight mass spectrometry. Clin. Infect. Dis. 2009, 49, 543–551. [Google Scholar] [CrossRef]
- Haldorsen, B.; Giske, C.G.; Hansen, D.S.; Orri Helgason, K.; Kahlmeter, G.; Löhr, I.H.; Matuschek, E.; Österblad, M.; Rantakokko-Jalava, K.; Wang, M.; et al. Performance of the EUCAST disc diffusion method and two MIC methods in detection of Enterobacteriaceae with reduced susceptibility to meropenem: The NordicAST CPE study. J. Antimicrob. Chemother. 2018, 73, 2905. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Cases | Age | Sex | Clinical History of Prosthesis Infection | Routine Bacterial Culture | Methanogen Detection | Previous Antibiotics | Number of Surgeries after Prosthesis Implantation | Infection Evolution (Months) | Prosthesis Ablation | Prosthesis Re-Implantation | Spacer Implantation | Cured | Relapse |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Case 1 | 81 | F | S. aureus and E. coli right knee prosthesis infection | S. aureus | M. oralis | Rifadin + clindamycin + ofloxacin | 2 | 111 | Yes | Yes | YES | Yes | No |
| Case 2 | 78 | M | S. aureus and S. epidermidis right hip prosthesis infection | S. epidermidis | M. oralis | Rifampicin + ofloxacin | 1 | 99 | Yes | No | Yes | No | No |
| Case 3 | 46 | F | S. aureus and S. lugdunensis and Klebsiella pneumoniae and Proteus mirabilis and S. capitis left hip prosthesis infection | P. mirabilis | M. smithii | Imipenem + clindamycin | No | 358 | Yes | Yes | No | No | Yes |
| Case 4 | 74 | M | S. aureus left Knee prosthesis | S. aureus | M. wolinii | Rifampicin + ofloxacin + teicoplanin | 2 | 74 | Yes | Yes | Yes | On going | No |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Djemai, K.; Gouriet, F.; Argenson, J.-N.; Seng, P.; Stein, A.; Drancourt, M. First Detection of Methanogens in Orthopedic Prosthesis Infection: A Four-Case Founding Series. Prosthesis 2022, 4, 38-47. https://0-doi-org.brum.beds.ac.uk/10.3390/prosthesis4010005
Djemai K, Gouriet F, Argenson J-N, Seng P, Stein A, Drancourt M. First Detection of Methanogens in Orthopedic Prosthesis Infection: A Four-Case Founding Series. Prosthesis. 2022; 4(1):38-47. https://0-doi-org.brum.beds.ac.uk/10.3390/prosthesis4010005
Chicago/Turabian StyleDjemai, Kenza, Frédérique Gouriet, Jean-Noël Argenson, Piseth Seng, Andreas Stein, and Michel Drancourt. 2022. "First Detection of Methanogens in Orthopedic Prosthesis Infection: A Four-Case Founding Series" Prosthesis 4, no. 1: 38-47. https://0-doi-org.brum.beds.ac.uk/10.3390/prosthesis4010005