
Real-World Testing of the Self Grasping Hand, a Novel Adjustable Passive Prosthesis: A Single Group Pilot Study



Abstract
:1. Introduction
2. Results
2.1. Participants
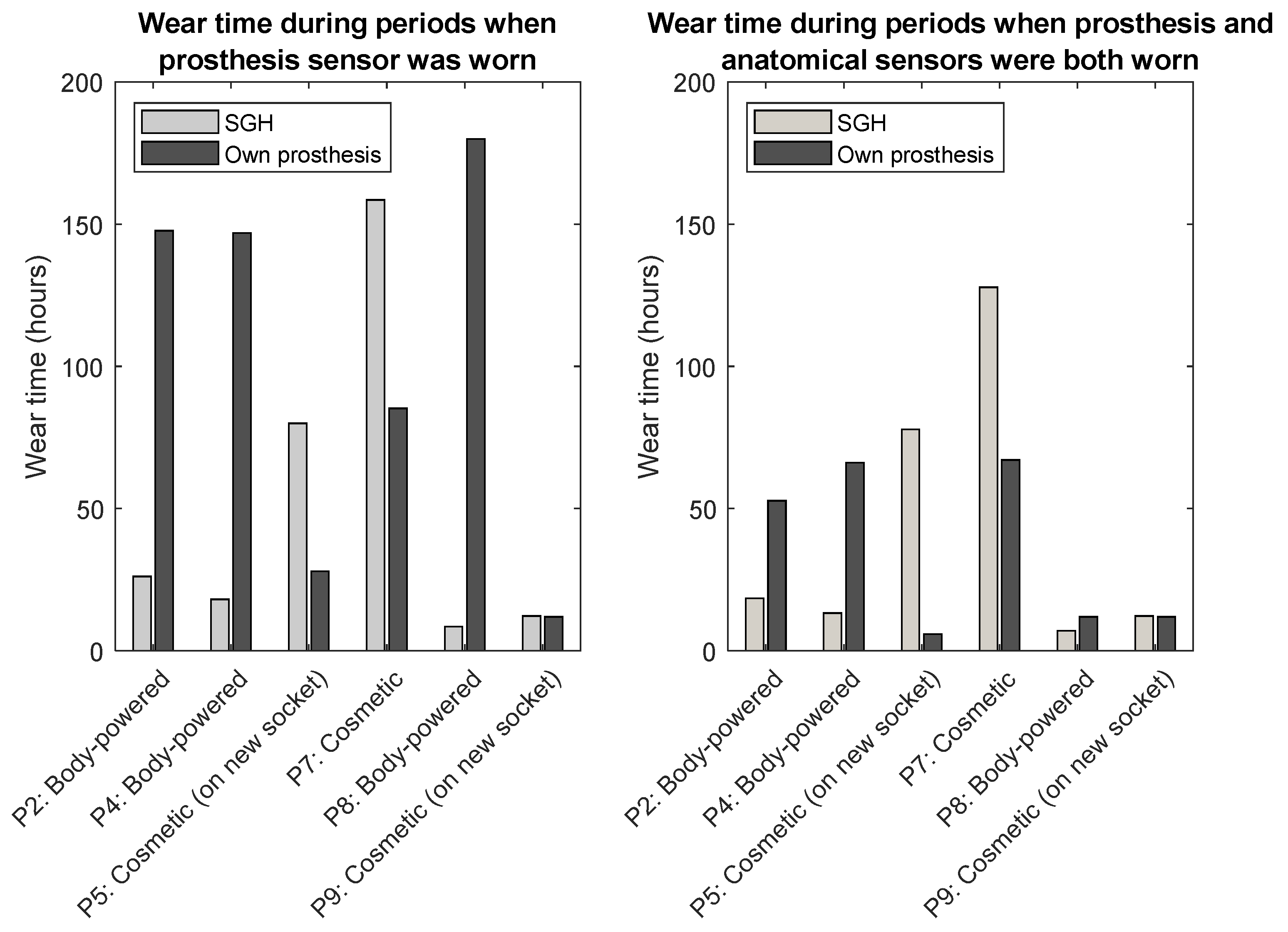
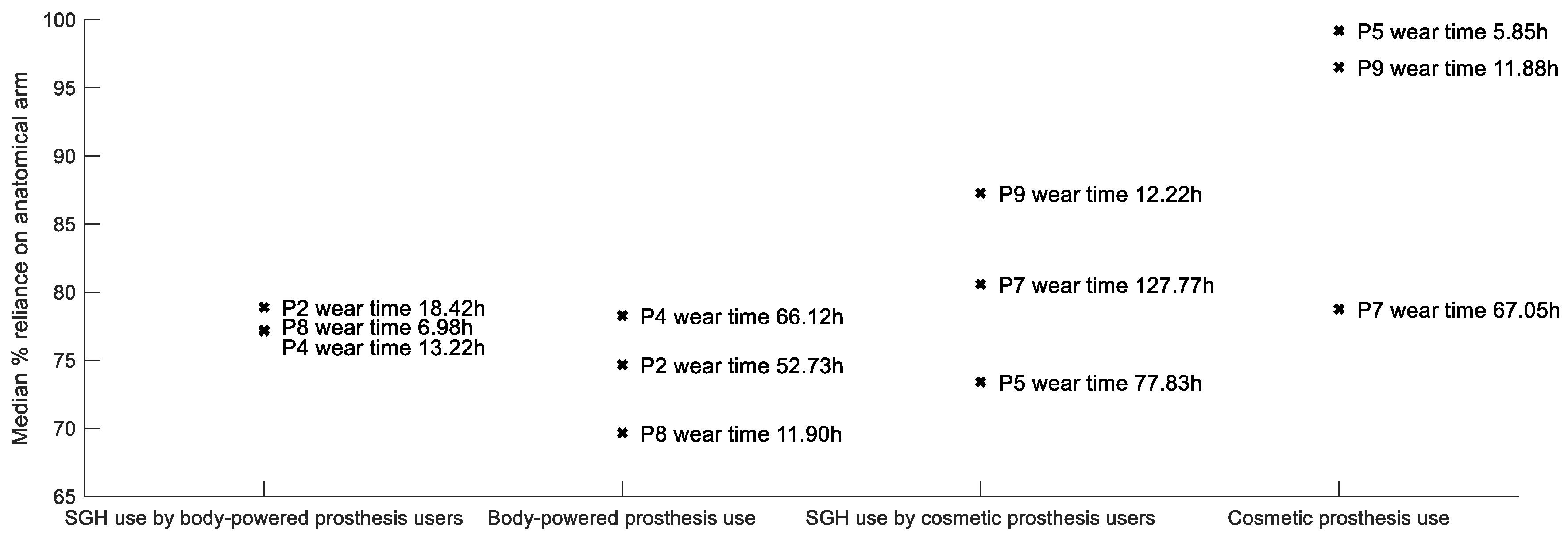
2.2. Prosthesis Wear Time
2.3. Patient-Reported Outcome Measures
2.4. Adverse Events
2.5. Feasibility Outcomes
2.5.1. Recruitment and Retention
2.5.2. Acceptability, Reliability, and Data Retrieved from Activity Monitors
3. Discussion
4. Materials and Methods
- rates of recruitment over the nine-month study period, retention over the two-week trial period, and attendance at the follow-up appointment
- whether participants fully adhered to the study protocol, including testing the SGH at home and work over two weeks, completion of activity diaries and Patient Reported Outcome Measures (PROMs), and whether the activity monitors were worn as directed and performed reliably throughout the trial, and
- adverse events (e.g., breakages, malfunctions of prosthesis or activity monitor).
5. Conclusions
6. Patents
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- National Academies of Sciences Engineering and Medicine. The Promise of Assistive Technology to Enhance Activity and Work Participation; The National Academies Press: Washington, DC, USA, 2017. [Google Scholar]
- Maat, B.; Smit, G.; Plettenburg, D.; Breedveld, P. Passive prosthetic hands and tools: A literature review. Prosthet. Orthot. Int. 2018, 42, 66–74. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burger, H.; Marinček, Č. Upper limb prosthetic use in Slovenia. Prosthet. Orthot. Int. 1994, 18, 25–33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Biddiss, E.; Beaton, D.; Chau, T. Consumer design priorities for upper limb prosthetics. Disabil. Rehabil. Assist. Technol. 2007, 2, 346–357. [Google Scholar] [CrossRef]
- Soltanian, H.; De Bese, G.; Beasley, R.W. Passive hand prostheses. Hand Clin. 2003, 19, 177–183. [Google Scholar] [CrossRef]
- Maat, B. Design and Evaluation of a New Passive Adjustable Prosthetic Hand Comprising a Novel Control Method. Master’s Thesis, Delft University of Technology, Delft, The Netherlands, 2015. [Google Scholar]
- Smit, G.; Maat, B.; Plettenburg, D.; Breedveld, P. A Self-Grasping Hand Prosthesis. In Proceedings of the Myoelectric Controls and Upper Limb Prosthetics Symposium, Fredericton, NB, Canada, 15–18 August 2017. [Google Scholar]
- Chadwell, A.; Chinn, N.; Kenney, L.; Karthaus, Z.J.; Mos, D.; Smit, G. An evaluation of contralateral hand involvement in the operation of the Delft Self-Grasping Hand, an adjustable passive prosthesis. PLoS ONE 2021, 16, e0252870. [Google Scholar] [CrossRef]
- Chadwell, A.; Kenney, L.; Granat, M.; Thies, S.; Head, J.S.; Galpin, A. Visualisation of upper limb activity using spirals: A new approach to the assessment of daily prosthesis usage. Prosthet. Orthot. Int. 2018, 42, 37–44. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kyberd, P.J.; Wartenberg, C.; Sandsjö, L.; Jönsson, S.; Gow, D.; Frid, J.; Almström, C.; Sperling, L. Survey of Upper-Extremity Prosthesis Users in Sweden and the United Kingdom. JPO J. Prosthet. Orthot. 2007, 19, 55–62. [Google Scholar] [CrossRef]
- Chadwell, A.; Kenney, L.; Granat, M.H.; Thies, S.; Head, J.; Galpin, A.; Baker, R.; Kulkarni, J. Upper limb activity in myoelectric prosthesis users is biased towards the intact limb and appears unrelated to goal-directed task performance. Sci. Rep. 2018, 8, 11084. [Google Scholar] [CrossRef] [PubMed]
- Burger, H.; Franchignoni, F.; Heinemann, A.; Kotnik, S.; Giordano, A. Validation of the orthotics and prosthetics user survey upper extremity functional status module in people with unilateral upper limb amputation. J. Rehabil. Med. 2008, 40, 393–399. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deijs, M.; Bongers, R.M.; Ringeling-van Leusen, N.D.M.; Van Der Sluis, C.K. Flexible and static wrist units in upper limb prosthesis users: Functionality scores, user satisfaction and compensatory movements. J. Neuroeng. Rehabil. 2016, 13, 26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Resnik, L.; Borgia, M. Reliability and Validity of Outcome Measures for Upper Limb Amputation. JPO J. Prosthet. Orthot. 2012, 24, 192–201. [Google Scholar] [CrossRef]
- Schneller, M.B.; Bentsen, P.; Nielsen, G.; Brønd, J.C.; Ried-Larsen, M.; Mygind, E.; Schipperijn, J. Measuring children’s physical activity: Compliance using skin-taped accelerometers. Med. Sci. Sports Exerc. 2017, 49, 1261–1269. [Google Scholar] [CrossRef] [Green Version]
- Chadwell, A.; Kenney, L.; Granat, M.; Thies, S.; Galpin, A.; Head, J. Upper limb activity of twenty myoelectric prosthesis users and twenty healthy anatomically intact adults. Sci. Data 2019, 6, 199. [Google Scholar] [CrossRef] [PubMed]
- Brønd, J.C.; Andersen, L.B.; Arvidsson, D. Generating ActiGraph Counts from Raw Acceleration Recorded by an Alternative Monitor. Med. Sci. Sports Exerc. 2017, 49, 2351–2360. [Google Scholar] [CrossRef]
- Heinemann, A.W.; Bode, R.; O’Reilly, C. Development and measurement properties of the Orthotics and Prosthetics Users’ Survey (OPUS): A comprehensive set of clinical outcome instruments. Prosthet. Orthot. Int. 2003, 27, 191–206. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shirley Ryan Ability Lab. OPUS UP Scoring Guide. Rehabilitation Measures Database 2016. Available online: https://www.sralab.org/sites/default/files/2017-12/OPUS%20UP%20Scoring%20Guide%206%20June%202016.pdf (accessed on 12 December 2019).
- Gallagher, P. Trinity Amputation and Prosthesis Experience Scales–Revised (TAPES-R). 2011. Available online: http://psychoprosthetics.ie/assets/TAPES_2011_Sept_2011.pdf (accessed on 12 December 2019).
- Gallagher, P.; Franchignoni, F.; Giordano, A.; MacLachlan, M. Trinity amputation and prosthesis experience scales: A psychometric assessment using classical test theory and rasch analysis. Am. J. Phys. Med. Rehabil. 2010, 89, 487–496. [Google Scholar] [CrossRef] [PubMed]
- Heinemann, A.W.; Conelly, L.; Ehrlich-Jones, L.; Fatone, S. Outcome instruments for prosthetics: Clinical applications. Phys. Med. Rehabil. Clin. 2014, 25, 179–198. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | |
|---|---|
| Sex, n (%) | |
| Male | 5 (55.5%) |
| Female | 4 (44.5%) |
| Age, years, mean (SD) 1 | 45.9 (14.9) |
| Range | 19–62 |
| Years since amputation, mean (SD) | 31.1 (21.5) |
| Range | 0.75–62 |
| Years using current prosthesis, mean (SD) | 8.4 (1.17) |
| Range | 0.33–45 |
| Cause of amputation, n (%) | |
| Congenital | 5 (55.5%) |
| Injury | 2 (22.2%) |
| Infection | 2 (22.2%) |
| Type of prosthesis used (at the time of testing), n (%) | |
| Passive | 4 (44.5%) |
| Body-powered | 5 (55.5%) |
| Occupation category, n | |
| Manager | 1 |
| Professional | 1 |
| Technician/Trade | 2 |
| Community and personal service | 1 |
| Clerical | 1 |
| Machinery operator/driver | 1 |
| University student | 1 |
| Home duties | 1 |
| Item | Not Able | Very Difficult | Slightly Difficult | Easy | Very Easy | N/A or Missing | Raw Score Mean (SD) 2 | Using SGH (%) 1 |
|---|---|---|---|---|---|---|---|---|
| 1. Wash face | 0 | 0 | 0 | 0 | 7 | 1 | 4.0 (0) | 0.0% |
| 2. Put toothpaste on brush and brush teeth | 1 | 0 | 2 | 2 | 3 | 0 | 2.8 (1.4) | 50.0% |
| 3. Brush/comb hair | 0 | 0 | 1 | 1 | 4 | 2 | 3.4 (0.9) | 16.7% |
| 4. Put on and remove t-shirt | 1 | 0 | 2 | 2 | 3 | 0 | 3.0 (1.4) | 62.5% |
| 5. Button shirt with front buttons | 1 | 0 | 3 | 1 | 1 | 2 | 1.8 (1.6) | 0.0% |
| 6. Attach end zipper and zip jacket | 4 | 0 | 2 | 0 | 0 | 2 | 0.8 (1.1) | 66.7% |
| 7. Put on socks | 1 | 0 | 1 | 3 | 2 | 1 | 3.2 (0.8) | 28.6% |
| 8. Tie shoelaces | 3 | 0 | 1 | 2 | 0 | 2 | 2.0 (1.4) | 66.7% |
| 9. Drink from a paper cup | 0 | 0 | 3 | 0 | 3 | 2 | 2.9 (1.1) | 50.0% |
| 10. Use fork or spoon | 3 | 0 | 0 | 1 | 2 | 2 | 2.2 (2.0) | 66.7% |
| 11. Cut meat with knife and fork | 4 | 0 | 2 | 1 | 0 | 1 | 1.2 (1.3) | 85.7% |
| 12. Pour from a 12 oz can | 0 | 1 | 1 | 2 | 3 | 1 | 2.7 (1.4) | 42.9% |
| 13. Write name legibly | 0 | 0 | 0 | 2 | 5 | 1 | 3.6 (0.5) | 0.0% |
| 14. Use scissors | 2 | 0 | 2 | 1 | 1 | 1 | 2.2 (1.3) | 28.6% |
| 15. Open door with knob | 0 | 1 | 1 | 2 | 3 | 1 | 2.5 (1.7) | 42.9% |
| 16. Use a key in a lock | 1 | 0 | 0 | 1 | 6 | 0 | 3.3 (1.4) | 12.5% |
| 17. Carry laundry basket | 0 | 0 | 1 | 5 | 1 | 1 | 3.0 (0.6) | 85.7% |
| 18. Dial a touch-tone phone | 0 | 2 | 1 | 1 | 4 | 0 | 3.1 (1.1) | 25.0% |
| 19. Use a hammer and nail | 2 | 0 | 0 | 1 | 0 | 5 | 1.5 (2.1) | 0.0% |
| 20. Fold a bath towel | 0 | 0 | 0 | 4 | 1 | 3 | 2.8 (1.9) | 80.0% |
| 21. Open an envelope | 0 | 1 | 0 | 4 | 1 | 2 | 2.9 (0.9) | 50.0% |
| 22. Stir in a bowl | 1 | 0 | 3 | 1 | 0 | 3 | 2.0 (1.1) | 60.0% |
| 23. Put on and take off prosthesis | 0 | 0 | 3 | 3 | 3 | 0 | 3.0 (0.9) | 0.0% |
| Participant Number | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| SGH Aspects (Maximum = 3) | 1 | 2 | 3 1 | 4 | 5 1,2 | 7 1 | 8 | 9 1,2 | Mean |
| Colour | 2 | 3 | 2 | 2 | 3 | 2 | 2 | 2 | 2.3 |
| Shape | 2 | 3 | 2 | 3 | 2 | 1 | 2 | 1 | 2.0 |
| Appearance | 2 | 3 | 2 | 3 | 3 | 1 | 3 | 1 | 2.3 |
| Aesthetics Subtotal | 2.2 | ||||||||
| Weight | 2 | 3 | 3 | 3 | 2 | 2 | 2 | 1 | 2.3 |
| Usefulness | 2 | 1 | 1 | 2 | 2 | 1 | 1 | 2 | 1.5 |
| Reliability | 2 | 2 | 1 | 1 | 2 | 1 | 2 | 2 | 1.6 |
| Fit | 2 | 3 | 2 | 3 | 3 | 3 | 3 | 2 | 2.6 |
| Comfort | 2 | 1 | 2 | 3 | 3 | 3 | 3 | 2 | 2.4 |
| Function Subtotal | 2.1 | ||||||||
| Overall Prosthesis Satisfaction rating (maximum = 10) | 6 | 5 | 3 | 8 | 7 | 3 | 2 | 6 | 5.0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
O’Brien, L.; Montesano, E.; Chadwell, A.; Kenney, L.; Smit, G. Real-World Testing of the Self Grasping Hand, a Novel Adjustable Passive Prosthesis: A Single Group Pilot Study. Prosthesis 2022, 4, 48-59. https://0-doi-org.brum.beds.ac.uk/10.3390/prosthesis4010006
O’Brien L, Montesano E, Chadwell A, Kenney L, Smit G. Real-World Testing of the Self Grasping Hand, a Novel Adjustable Passive Prosthesis: A Single Group Pilot Study. Prosthesis. 2022; 4(1):48-59. https://0-doi-org.brum.beds.ac.uk/10.3390/prosthesis4010006
Chicago/Turabian StyleO’Brien, Lisa, Elena Montesano, Alix Chadwell, Laurence Kenney, and Gerwin Smit. 2022. "Real-World Testing of the Self Grasping Hand, a Novel Adjustable Passive Prosthesis: A Single Group Pilot Study" Prosthesis 4, no. 1: 48-59. https://0-doi-org.brum.beds.ac.uk/10.3390/prosthesis4010006