

Non-Invasive Sensory Input Results in Changes in Non-Painful and Painful Sensations in Two Upper-Limb Amputees

1
Center for Neuroplasticity and Pain (CNAP), Department of Health Science and Technology (SUND), Aalborg University, 9260 Gistrup, Denmark
2
Department of Biomedical Engineering, Indiana University—Purdue University Indianapolis, Indianapolis, IN 46202, USA
*
Author to whom correspondence should be addressed.
Prosthesis 2024, 6(1), 1-23; https://0-doi-org.brum.beds.ac.uk/10.3390/prosthesis6010001
Submission received: 31 August 2023
/
Revised: 9 December 2023
/
Accepted: 13 December 2023
/
Published: 19 December 2023
(This article belongs to the Special Issue Innovations in the Control and Assessment of Prosthetic Arms)
Abstract
:Designs of active prostheses attempt to compensate for various functional losses following amputation. Integration of sensory feedback with the functional control re-enables sensory interaction with the environment through the prosthetic. Besides the functional and sensory loss, amputation induces anatomical and physiological changes of the sensory neural pathways, both peripherally and centrally, which can lead to phantom limb pain (PLP). Additionally, referred sensation areas (RSAs) likely originating from peripheral nerve sprouting, regeneration, and sensory reinnervation may develop. RSAs might provide a non-invasive access point to sensory neural pathways that project to the lost limb. This paper aims to report on the sensory input features, elicited using non-invasive electrical stimulation of RSAs that over time alleviated PLP in two upper-limb amputees. The distinct features of RSAs and sensation evoked using mechanical and electrical stimuli were characterized for the two participants over a period of 7 and 9 weeks, respectively. Both participants received transradial and transhumeral amputation following traumatic injuries. In one participant, a relatively low but stable number of RSAs provided a large variety of types of evoked phantom hand (PH) sensations. These included non-painful touch, vibration, tingling, stabbing, pressure, warmth/cold as well as the perception of various positions and movements of the phantom hand upon stimulation. Discomforting and painful sensations were induced with both mechanical and electrical stimuli. The other participant had a relatively large number of RSAs which varied over time. Stimulation of the RSAs provided mostly non-painful sensations of touch in the phantom hand. Temporary PLP alleviation and a change in the perception of the phantom hand from a tight to a more open fist were reported by both participants. The specificity of RSAs, dynamics in perception of the sensory input, and the associated alleviation of PLP could be effectively exploited by designs of future active prostheses. As such, techniques for the modulation of the sensory input associated with paradigms from interaction with the environment may add another dimension of protheses towards integrating personalized therapy for PLP.
1. Introduction
Amputation leads to physiological changes in the sensory–motor wiring in the periphery as well as changes centrally. Beyond the functional consequences, amputation also manifests a complex pattern of psychological change and presents as a complex disability [1,2,3,4]. Besides the functional and sensory loss, amputation could also lead to the development of phantom limb pain (PLP) [5,6]. Although it is not clear what mechanisms lead to PLP, evidence suggests that the use of prostheses and artificially generated sensory input alleviates PLP [3,7,8,9,10,11,12,13,14].
The design of prostheses attempts to address both the medical and social aspects of the disability by restoring the lost function to some degree while providing an aesthetically acceptable outward appearance. Significant progress has been made in the recent decades in manufacturing mechatronic devices that resemble the human hand while providing some degree of functional restoration and movement. The challenge of controlling a multi-degree of freedom-actuated prosthesis has partially been addressed by interfaces exploiting various physiological signals that aim to provide a more natural and intuitive manipulation of complex geometry objects [15,16].
Integrating sensory feedback marked a milestone defining active prostheses. The dexterity and fine motor control embodied by the human hand heavily relies on the integration and closed loop feedback using sensory information. Depriving the nervous system of its natural sensory input, following amputation, leads to a less-optimal state. Control of a prosthetic hand is typically limited by features of the artificial actuators, such as number/configuration and precision/speed. Further limitation is added by the use of the substitute physiological signals in an open loop control in current commercial designs of prostheses. Inclusion of a sensory percept in the control interface contributed significantly to a more efficient interaction of the active prostheses with the environment [17,18,19,20,21,22,23,24,25,26]. The mode of delivering sensory feedback associated with prosthetic devices varies from substitution [27,28,29] and redirection [30] techniques to a more natural somatotopical sensory feedback using direct peripheral nerve stimulation [15,16,17,18,19] or stimulation of referred sensation areas [31,32]. Referred sensation areas are underrated in current applications of prosthetic devices, given the potential that they may have in somatotopical sensory feedback [33,34]. Despite technological advances, the user’s perception still lacks refinement. Adaptation and customization when addressing personalization in the design of prosthesis are currently not widely available in the market, resulting in a relatively high rate of usage drop-off [3,4,35].
Physiological changes following amputation are likely caused by a lack of sensory input [36,37,38,39,40,41,42]. Given the ability of peripheral nerves to grow if severed, sensory neural pathways that innervated the lost limb regenerate to reinnervate nearby sensors from specific areas on the stump, leading to sensations projecting to the phantom limb when activated [29,30,31,37,40,41,42,43,44,45,46,47]. These referred sensation areas (RSAs) might be reached using mechanical or electrical stimulation to provide a wide variety of high-quality sensory sensations using non-invasive stimulation modalities. The quality and quantity of the non-invasive natural sensory feedback provided through the referred sensation areas once quantified and characterized could be exploited once adapted to an appropriate interactive state of the active prostheses to generate appropriate sensory feedback from the prosthetic to the user. This new interaction with the prosthetic limb could improve embodiment of the prosthetic and improve its functional integration with the amputee. Addressing individualized therapy in the complex pattern of disability following amputation is a first step towards the development of the RSAs as a therapeutic intervention for PLP or development of its use with advanced sensorized prosthetic limbs.
This paper aims to report on features of the perceived non-painful and painful sensations, with dynamic effects on the phantom limb pain, induced using non-invasive electrical stimulation of RSAs in two upper-limb amputees. Both participants were victims of traumatic injury and were received well prior to this study. One participant was a transradial amputee, with the amputation taking place approximately 11 cm above the wrist. The other participant was a transhumeral amputee, with the amputation just above the elbow. The two participants were enrolled in the EPIONE project, a multicenter project that aimed to investigate the non-invasive natural sensory feedback related to the missing limb as a possible alternative therapy for phantom limb pain through a set of psychophysical measures [48,49]. The overarching hypothesis of the project was that a maladaptive cortex following the loss of peripheral sensory/motor feedback was the underlying mechanisms that presented as PLP. It further hypothesized that reestablishing sensory feedback from the periphery in concert with active central drive can reverse the maladaptation of the cortex which thereby alleviates pain. This framework informs the experimental design of the project.
2. Materials and Methods
The current experiment was carried out under the framework of the EPIONE consortium and clinical trials protocol (EU FP7-HEALTH-2013-INNOVATION, project number 602547 EPIONE, ClinicalTrials.gov NCT02488668) [44,45]. The protocol was designed to evaluate psychophysical measures during four phases: baseline (determination of RSAs), entry (EEG and MRI baseline measures), intervention (sensation characterization and therapy), and outcome (EEG and MRI outcome measures). Each phase had specific sets of questionnaires (BPI, POMS, NPSI, PGIC, PHQ9). The protocol sessions and procedures were scheduled and performed using a custom-made computerized psychophysical testing platform.
In the present work, we report on a subset of the study coming from two participants with upper-limb amputation. The participants attended the study for periods of 7 and 9 weeks, respectively, out of a 9-week experimental protocol at Aalborg University. Experimental sessions were scheduled for each participant as illustrated in Figure 1 (a follow-up phase not included). During baseline and entry phases, maps of RSAs were determined with mechanical stimuli (light brush and glass ball). Based on these RSA maps, thresholds for sensation and discomfort evoked using electrical stimuli that projected to the phantom hand for various configurations for position of electrodes were investigated. The locations and types of sensation were than characterized for the chosen configuration of electrodes under single- and multi-channel electrical stimulation. Both ramping and steady-state stimulation were explored. During the therapy phase, characterization of evoked sensation continued in parallel with the delivery of steady-state stimuli for therapy for randomized single- and multi-channel electrical stimulation.
2.1. Participants
Participant (P1) was a 36-year-old female with a left-side transhumeral amputation. Participant (P2) was a 35-year-old male with a left-side transradial amputation. A traumatic injury led to amputation in both cases. Participant P1 had never used a prosthetic device. Participant P2 regularly used a prosthetic hand, serving only an aesthetical function.
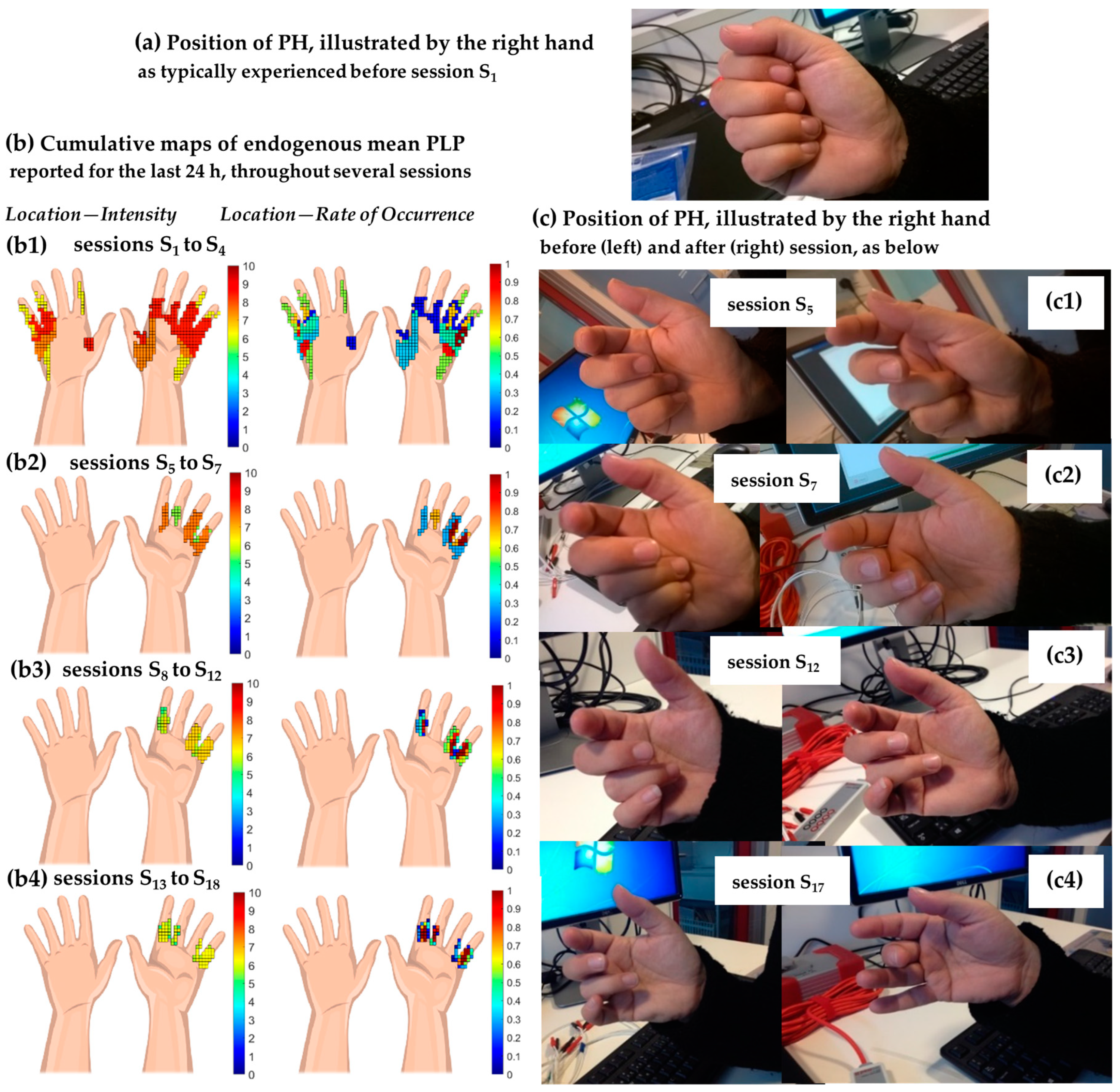
P1’s amputation site was approximately 3 cm above the elbow. The phantom hand was perceived as an appendage directly extending from the amputation site (i.e., no forearm perceived) and with a posture similar to that of a tight fist (Figure 2). Mental control of the phantom hand was very limited, requiring intense focus that resulted in relatively small movements of the fingers. P1 experienced a mean value of PLP within 24 h of 7.9 on a visual analog scale for painful sensations (0 = no pain, 10 = worst imaginable pain, referred to as a VASP), which was reported in the pre-screening/recruitment session. PLP affected the root of the fingers (all fingers on palmar side, including the first and second phalanx, as well as little and ring fingers extending down the ulnar side on the dorsal side) and the thenar and hypothenar regions on the palmar side. Continuous pain was described as burning, squeezing, pins and needles, tingling, and pressure of 5, 9, 9, 7, and 2 on VASP, respectively. Spontaneous pain like stabbing (9 on VASP) was regularly experienced for between 8 and 12 h (more than 20 times) within 24 h. PLP was highly influenced by the weather (cold weather determined an increase in pain level and increased fingers’ clenching). No pain medication was prescribed for daily use.
P2’s amputation site was approximately 11 cm above the wrist. The participant reported a mean value of PLP within 24 h of 7.9 on VASP at the pre-screening/recruitment session. Continuous pain like burning, squeezing, pins and needles, tingling, and pressure score of 8 on VASP were reported, affecting the entire phantom hand. Spontaneous pain like electric shock and stabbing (6 and 8 on VASP) was experienced for less than 1 h (between one and five times) within 24 h. PLP was not influenced by other factors. No pain medication was prescribed for daily use.
Both participants signed a written consent form prior to participation in the experiment. The EPIONE protocol for non-invasive electrical stimulation at Aalborg University was approved by the Ethics Committee of Region Nordjylland (Den Videnskabstetiske Komité for Region Nordjylland, N-20140061).
2.1.1. Generating RSA Maps and Reference System
A reference system was used to track RSAs and electrodes for consecutive sessions, adapted for both participants (Appendix B, Figure A1a). A reference line was defined using two points identified using specific scars at or near the amputation site and anatomical landmarks (e.g., acromioclavicular point). The reference line served to calculate the transverse and longitudinal distances of the RSA center along the arm. Additional lines normal to the reference line were drawn to form a grid (segments of 50 mm and 10 mm) when needed, assisting in reporting location, size, and orientation of the RSAs and electrodes. The RSA was approximated as an ellipse, defined using coordinates of the center (identified using the distance along and the normal to the reference line), size (major and minor diameters), and orientation (the angle formed by the long axis of the ellipse to the reference line).
The scanning procedure for the mapping of the location of the RSAs with mechanical stimuli beginning at the amputation site. Tactile stimuli were applied with a brush (width of 5 mm) in parallel tracks moving proximal along the stump and the arm. The brush movements had a rate of approximately two scans per second, covering a distance of approximately 20 mm, and a lateral shift with a speed of 5 to 10 mm per second. Pressure stimuli were delivered using a 350 mm diameter glass ball that moved in a circular pattern at a rate of approximate one circular scan per second. The lateral shift of the scan was at a speed similar to that of the brush scan. The participant was asked to verbally report on the location, type, and intensity of both painful and non-painful sensations evoked on the phantom limb. The participant was additionally asked to score the strength of the evoked sensation using a visual analogue scale for non-painful sensation (0 = no sensation and 10 = most intense imaginable non-painful sensation, referred to as a VASS). If the stimulation evoked pain, the participant was asked to score the pain using a VASP score for painful sensations (0 = no pain and 10 = worst imaginable pain).
2.1.2. Surface Electrical Stimulation
Electrical stimuli were applied through two round (25 × 25 mm) or oval (40 × 64 mm) PALS electrodes (PALS® Axelgaard, Axelgaard Manufacturing Co., Ltd., Fallbrook, CA, USA). Stimuli were delivered in bursts/trains of bipolar, charge-balanced rectangular pulses with a pulse width (Pw) between 100 and 600 μs, a frequency (F) between 10 and 120 Hz, and an amplitude (I) between 5 and 80 mA. An ISIS Neurostimulator (Inomed®, inomed Medizintechnik GmbH, Emmendingen, Germany) was used to deliver these stimuli. The burst stimulation had a default stimulation cycle with the stimulus (Ton) with pause (Toff) periods of one second each.
Stimuli were delivered to up to six channels (time-division multiplexed, two electrodes per channel) through the ISIS Neurostimulator controlled using a custom-written software. Electrodes were placed for each channel so that one electrode covered one or more of the RSAs and the counter electrode was placed in close proximity (e.g., no more than 5 cm between the edges of electrodes) with no RSA; alternatively, both electrodes were placed on one or more RSAs. Configurations for which electrodes were placed sequentially along perpendicular directions were tested as well.
An investigation of sensation and discomfort thresholds was performed for each position of the electrodes (two electrodes per channel), during the baseline phase. This procedure was eventually repeated if needed. Ramp stimuli were delivered as bursts that had an intensity starting from 1 mA and increasing with each stimulation cycle, for each combination of pulse width and frequency (e.g., chosen values of Pw of 100, 200, 300, and 400 μs and frequency of 10, 50, and 120 Hz yielded 12 combinations). Each stimulus for each combination was delivered three times, for better threshold estimates, resulting in a total number of, e.g., 36 stimuli. These stimuli were delivered in a randomized order. The participant was instructed to press a button when the sensation threshold was reached upon the delivery of a ramp stimulus. Upon acknowledgment of this choice, the ramp stimulus continued with increasing intensity until the discomfort threshold was reached.
Sensation characterization for single-channel stimulation was performed by delivering ramp stimuli with intensities between the sensation and discomfort threshold (i.e., the working interval). The participant was instructed to press a button when the ramp stimulus reached an intensity that induced the most intense and distinct sensation. Sensation characterization for multi-channel stimulation was performed by delivering steady-state stimuli with intensities chosen as a percentage (e.g., 70%) within the working interval for each channel. The duration of stimulation was defined using a number of cycles (i.e., on-off period of a burst).
For single-channel stimulation, a stimulus was considered to have a higher energy than another stimulus (i.e., a referred stimulus) if it had a pulse width, frequency, or intensity higher than that of the referred stimulus. Multi-channel stimuli with stimulus intensities over the middle value of the working intervals were considered to be high-energy stimuli, whereas those below the middle values were considered low-energy stimuli.
Electrical stimuli inducing a meaningful and pleasant sensation in the PH were selected for the therapy phase. The term ‘meaningful and pleasant’ means any sensation normally perceived by the hand as not discomforting nor painful.
2.1.3. Maps of Sensations Evoked in the Phantom Hand
During the sensation characterization, the participant was asked to draw the location (area) and report the intensity (on VASS, eventually VASP if painful sensation was experienced) and attributes (i.e., text describing sensation) corresponding to the sensation evoked in the PH using the electrical stimulus. Cumulative maps showing location-intensity and location-rate of occurrence over a period including a variety of stimuli were built based on the location, with intensity maps corresponding to each stimulus. Cumulative map for location-intensity showed the highest intensity reported for a corresponding location. Cumulative map for location-rate of occurrence reported in normalized units and the number of reports of induced sensation in the PH for the given location divided by the total number of the stimuli delivered corresponding to the given period of analysis.
3. Results
3.1. Participant P1, Left-Transhumeral Amputee
Participant P1 was not aware of the presence of the referred sensation areas on the stump and did not experience sensations induced in the phantom hand using electrical or mechanical stimuli before participating in this study.
3.1.1. Identification of the RSA Map
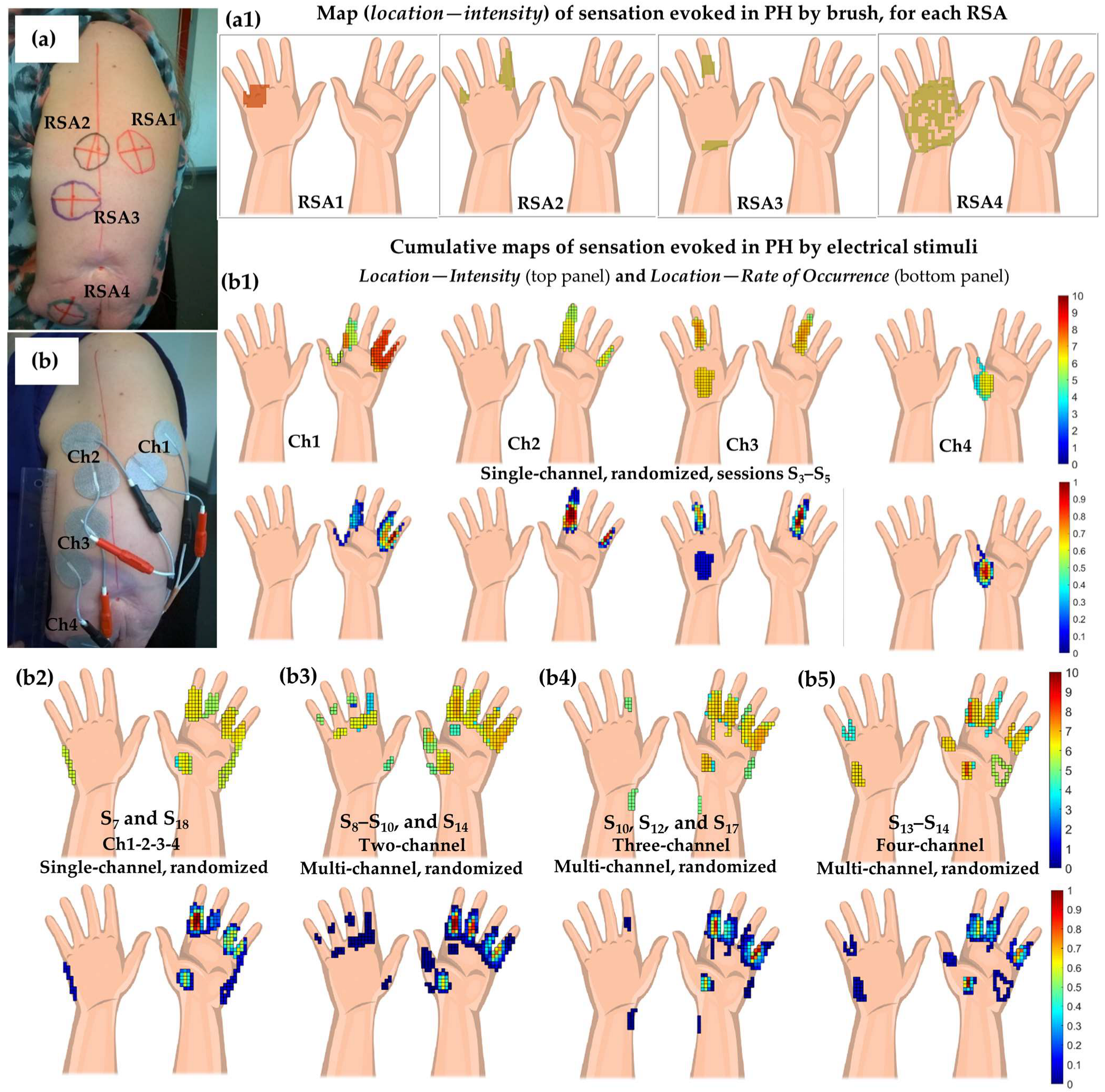
Four RSAs were detected with a light brush during session S1 (Figure 2a and Table A1). The RSAs were relatively stable over time, maintaining the location on the stump and the type of sensation evoked in the phantom hand when repeating the same detection procedure in sessions S3, S5, and S6. Approximately the same location and sensation evoked were determined using light pressure applied with the glass ball during session S3. A reference line was defined using the acromioclavicular point and a point given using a scar on the stump (Figure 2a and Figure A1, Appendix B).
3.1.2. Placement of Electrodes and Delivery of Electrical Stimuli
Electrodes (2.5 × 2.5 cm, PALS) corresponding to four channels (Ch1-4) were placed according to the map of RSAs identified using tactile mechanical stimuli (brush) during the session S1 and remained unchanged throughout the experiment (Figure 2b). One electrode was placed directly on one RSA, and the counter electrode was placed adjacent at approximately 2 cm between the edges of the electrodes. Thresholds for sensation and discomfort were determined in session S1 for each channel and repeated on S16. The repeated measure was due to a report of redness and tenderness at the stump areas below the electrodes. Characterization of the sensation evoked using single-channel stimulation, one channel at a time, was performed in sessions S3, S4, and S5 (Figure 2(b1)). Single-channel stimulation with all channels randomized was performed during session S7 and repeated in S18 (Figure 2(b2)). Characterization of the sensation evoked using multi-channel stimulation was performed in session S8 and S9 (two channels), S10 (two and three channels), S12 (three channels), S13 (four channels), S14 (two and four channels), S17 (one, two, and three channels) as shown in Figure 2(b3–b5).
Steady-state electrical stimuli (bursts of Ton and Toff of 1 s each) that induced meaningful and pleasant sensations (i.e., normal non-painful cutaneous and proprioceptive sensations), selected during the procedure of characterization of sensation, were applied during the therapy phase. Up to 70 series of 20 s per session were delivered. Stimuli were delivered as random single-channel stimulation during session S8, S17, and S18, as random multi-channel stimulation during session S9 (two channels), S10 (two and three channels), S12, S13 (three channels), and S14 (two, three, and four channels), and again as random single-channel stimulation during sessions S17 and S18.
3.1.3. Induced Sensations Evoked in the Phantom Hand Using Electrical Stimulation
The sensation evoked on the phantom hand using electrical stimulation reached all four submodalities of somatosensation (mechanoreception, thermoreception, nociception, and proprioception). Cutaneous (mechanoreceptive, thermoreceptive, and nociceptive) and proprioceptive sensations were elicited by 73% and 62% of the electrical stimuli delivered.
Sensation evoked using single-channel stimulation differed from that evoked using mechanical stimulation in both cutaneous and proprioceptive sensations (Table A1 and Table A2). The greatest difference was observed for RSA4 (painful sensation evoked on the dorsal side of phantom hand using tactile stimuli delivered with a brush on the RSA4) and Ch4 (non-painful sensation like tingling and muscle contraction on the thenar area). Repetition of single-channel stimulation, within the same session for Ch1 or at different sessions for Ch1-4, produced a different type of evoked sensations for specific stimuli (Table A2, Ch1-4). Multi-channel stimulation evoked sensations in a pattern resembling summation of the sensations evoked using single-channel stimulation (Figure 2(b1–b5) and Table A2). However, the perception of a more flexible and lively phantom hand (i.e., like PH “comes to life” in both perception and movements) and sensations of heaviness (as both pleasant and discomfort), warmth and/or cold were additionally reported as mostly specific to two-channel and three-channel multi-channel stimulation and less for four-channel multi-channel stimulation (Table A2, four-channel multi-channel vs. two-channel and three-channel multi-channel stimulation).
P1 often reported a complex pattern for the sensation evoked in the phantom hand. The type and location of the evoked sensation had a dynamic dependency on the energy and duration of the stimulus during and after both ramp and steady-state electrical stimuli.
For example, ramp stimulation on Ch1 with a current increasing from 5 to 9 mA in 20 steps (Pw of 400 µs and F of 10 Hz) induced, initially, a knocking sensation in the ring (F4) and little (F5) fingers. As the current increased, the F4 and F5 rotated and pulled out (similar to dislocation) from their root (Table A2, Ch1, entry 8). Stimulating on Ch2 with a current increasing from 5 to 15 mA (Pw of 100 µs and F of 10 Hz) induced tingling and stabbing sensations in the F5 and index finger (F2), respectively. Furthermore, a progressive flexion of the F2 (to full-closed position) with the increasing current was observed (Table A2, Ch2, entry 2). On the same channel, increasing the current from 5 to 13 mA (Pw of 100 µs and F of 70 Hz) induced tingling in the F2 and F5 with a progressive extension of F2 (to full-stretched position) and adduction towards the middle finger (F3) just before the stimulus offset (Table A2, Ch2, entry 3). Current increasing from 3 to 7 mA (Pw of 200 µs and F of 70 Hz) induced tingling in the F2 and F5 and flexion (from an initial slightly flexed position) to full closure in the first part of the ramp. The sensation changed to extension in the second part of the ramp, reaching a full-stretched position towards the stimulus offset (Table A2, Ch2, entry 6). A sensation of warmth (like warm water running down the finger) and a light stretch was reported as occurring towards the end of the ramp stimulus (I from 3 to 7 mA, Pw of 400 µs, and F of 30 Hz, Table A2, Ch3, entry 8). This stimulus initially induced tingling on the F3 and on the central aspects of both dorsal and palmar sides of the PH. Furthermore, steady-state four-channel multi-channel stimulation over a period of 20 s with 10, 5, 8, 15 mA (Pw of 200 µs and F of 70 Hz), initially, was felt as diffuse tingling in the F1 and F2. As stimulation continued, diffuse tingling was felt in the F3 and followed by the F4 and some on the F5 very close to the end of the stimulus. Stimulation with steady-state stimuli on three channels Ch2, Ch3, and Ch4 with I of 7, 5, and 8 mA, respectively, Pw of 400 µs and F of 10 Hz, induced after the stimulus onset tingling in the F2 at 4.2 on VASS and heaviness in the entire phantom hand. The phantom hand was perceived as becoming increasingly heavy as the stimulus continued. Close to the stimulus offset, this sensation reached a level of discomfort (Table A2, multi-channel on three channels, entry 9). The sensation of uncomfortable heaviness contrasted with that evoked using two-channel stimulation on Ch2 and Ch3 with I of 13 and 9 mA, respectively (Pw of 200 µs, F of 10 Hz), where the sensation of heaviness was perceived as pleasant and relaxing (Table A2, multi-channel on two channels, entry 1).
3.1.4. Perception of the Phantom Hand over Time
The participant often reported experiencing the sensations evoked in the phantom hand as ‘bringing the phantom hand to life’. It was perceived as ‘unusual and strange’. It demanded effort and focus from the participant when describing these sensations as the participant attempted to hide the phantom hand during her daily activities. Proprioceptive sensations often lasted after cessation of the stimulation, necessitating longer and longer breaks between consecutive stimulations to ensure ‘washout’ of the sensation and improve characterization of the sensation with the consequent stimulation periods. The participant experienced a strange and urging need to grasp the phantom hand when ‘coming to life’. This was often reported in the baseline phase when experiencing a new posture of the PH, discomfort, close-to-pain-threshold sensations, or unrealistic perception of the PH following stimulation. The unrealistic perception of the PH was reported when electrical stimuli induced unusual sensations (reported in Table A2), such as being touched by a crawling spider or a distorted phantom hand (e.g., F3 and F4 changed places, a finger rotates with the tendency to dislocate and/or to move away from the phantom hand, abnormal position of the F1 away from the PH and close to electrodes on the stump).
At the beginning of session S1, the usual perception of the phantom hand was described as a tight fist, with very limited mental control for opening and closing the hand (intense focus required for small movements of fingers). The thumb (F1), F2, and F3 were reported in a more open position at the beginning of session S5. By the end of the session, opening of these three fingers progressed, followed by a slight opening of the F4 and F5 at the end of session S7. Opening of the hand continued (with a slight regression of F4 between S7 and S12) towards the end of session S17. The mental control of the phantom hand greatly improved, allowing almost full stretch of the fingers and rotation of the wrist. At the end of session S18, part of the phantom hand, starting with the F5, F4 and continuing with the palmar and dorsal side of the hand towards the ulnar side of the wrist, could no longer be perceived (the participant reported that part of the PH vanished; it could no longer be felt). The reported ‘missing’ part of the phantom hand added to the unusual perception by participant P1 of the ‘hand coming to life’, inducing a slightly ambiguous effect. The participant could not tell whether this was positive or negative (the participant wondered ‘why my phantom hand was not there’, instead of ‘finally, I could not perceive part of my phantom hand’, as the experimenters would have expected).
3.1.5. Perception of Phantom Limb Pain over Time
Cumulative maps for the mean value of intensity for the last 24 h (reported at the beginning of each session, on VASP scale), location, and rate of occurrence (normalized units) for phantom limb pain reported for sessions S1 to S4, S5 to S7, S8 to S12, and S13 to S18 are illustrated in Figure 3(b1–b4), respectively. The cumulative maps show the maximal intensity of PLP for the corresponding location within the period reported, and the maps for rate of occurrence (normalized scale) show how often PLP was reported for a given location. As the phantom hand opened throughout the course of the study, both the mean values for 24 h of PLP intensity and the affected area (location) of cumulative maps on the phantom hand had a decreasing trend from 8.6 to 6.3 on the VASP scale, and from 36% to 6% of the total hand area, respectively.
3.2. Participant P2, Left-Transradial Amputee
3.2.1. Identification of the RSA Map
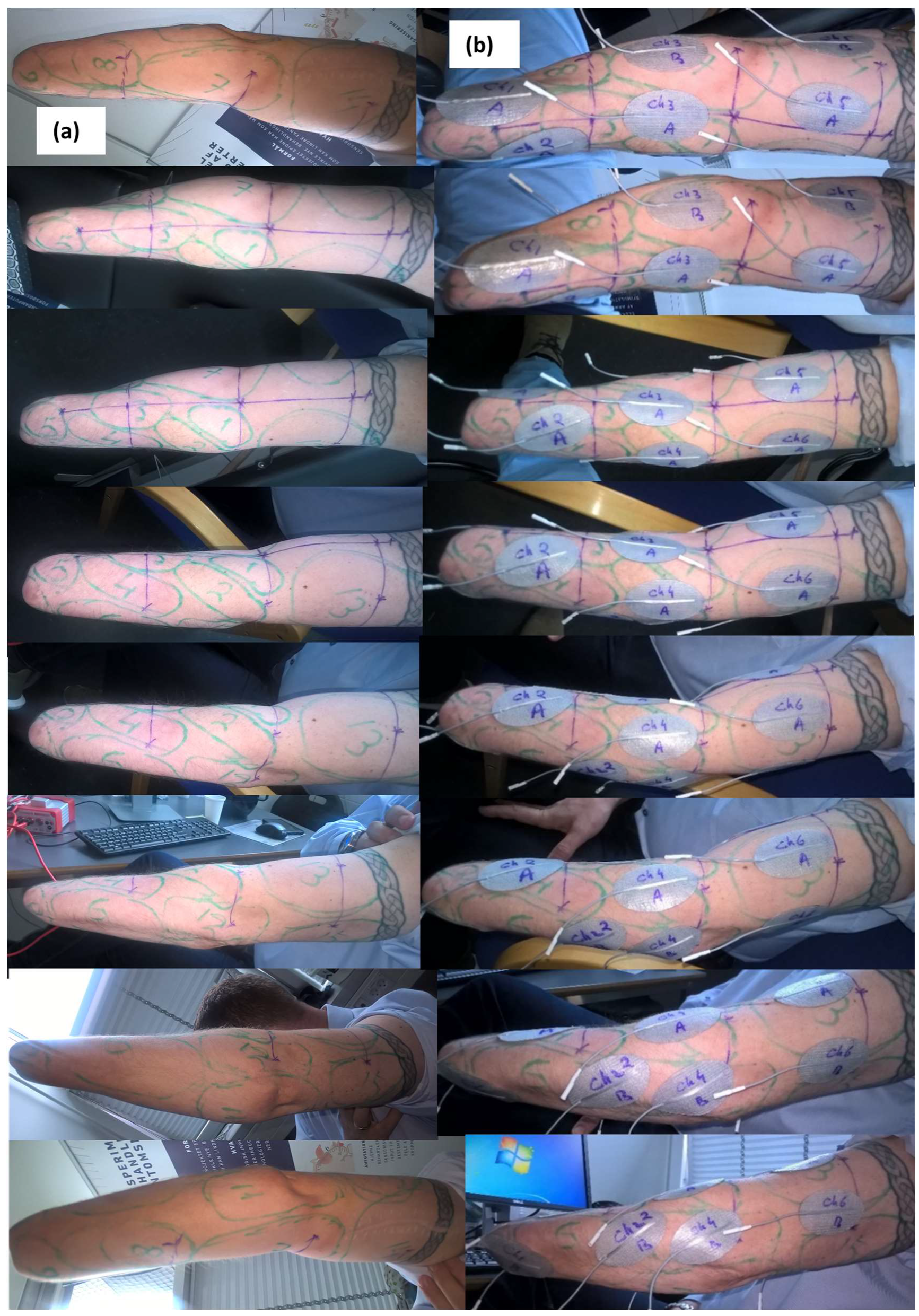
Referred sensation areas were investigated with tactile stimuli (brush) during session S1, S2, S3, S4, S5, and S12 identifying 12, 20, 15, 12, 15, and 14 RSAs, respectively. The RSAs had diameters ranging from 35 to 120 mm, as shown in Figure 4 and Figure A1 (Appendix B). The only sensation evoked in the phantom hand was that of touch (Figure A1(c1,c2), Appendix B). Testing the stump during session S5 with light pressure applied through the glass ball showed that the RSAs location on the stump and sensation evoked in the phantom hand was similar to that mapped and evoked using tactile stimuli (brush), respectively. A reference system was drawn on the stump/arm every session (Figure A1a, Appendix B).
3.2.2. Placement of Electrodes and Delivery of Electrical Stimuli
Electrodes (PALS 40 × 64 mm) were placed in a two-channel and four-channel configuration according to maps of RSAs identified using mechanical stimulation (brush) during sessions S1, S2, S3, and S4, testing thresholds and types of evoked sensations. Placement of electrodes was extended to six-channel and five-channel configuration during sessions S5 and S12, respectively, following changes in the RSAs maps (Figure A1b,d, Appendix B). Additional threshold estimation for single-channel stimulation was performed in session S7 and S10. The five-channel configuration from session S12 was used in the remaining sessions throughout the study. Electrodes were placed in an attempt to cover the RSAs in a balanced way, without exceeding 5 cm between electrodes for the same channel (Figure A1b, Appendix B).
Stimuli of Pw between 100 and 500 µs and F between 20 and 120 Hz were delivered as a ramp and as steady-state. The ramp stimulation (bursts with increasing current intensity for 15 cycles, Ton and Toff of 1 s each) was used for threshold determination and sensation characterization for single-channel stimulation. The steady-state stimulation (bursts with constant current intensity for 15 cycles, Ton and Toff of 1 s each) was used for sensation characterization for multi-channel stimulation. Thresholds for sensation and discomfort were determined throughout sessions S1 to S5 and S12 for each channel. For the six-channel configuration, established during session S5, the characterization of sensation evoked with stimulation was performed on (a) a single-channel during sessions S8 (Ch1 to Ch4, randomized) and during session S11 (Ch1 to Ch6, randomized); (b) multi-channel stimulation on four channels (Ch1 to Ch4) during session S10; and (c) multi-channel stimulation on five channels (Ch1 to Ch5) during session S11. Ch6 had a minor contribution during tests, and it was not included. For the five-channel configuration established during session S12, characterization of sensation evoked using stimulation was performed on multi-channel stimulation on all five channels at low energy during S12 and with high energy levels during S16 and S17. The duration of steady-state stimulation during sensation characterization for sessions S16 and S17 was of 150 cycles (Ton of 2 s and Toff of 0.2 s), a tenfold increase as compared to the duration of 15 cycles which was used for sensation characterization during previous sessions.
The steady-state electrical stimuli that produced meaningful and pleasant sensations, selected during the procedure of characterization of sensation, were applied during the therapy phase in up to 28 series (bursts of Ton of 2 s and Toff of 0.2, for 150 to 300 cycles for each stimulus). Stimuli were delivered on all five channels defined using the electrode configuration from session S12 as random single-channel stimulation during session S15; as random multi-channel (low level energy, Pw between 100 and 400 µs, F of 30 and 50 Hz, I from 12 to 20 mA) during session S13, S14, and S15; and as random multi-channel (high-level energy, Pw between 300 and 400 µs, F of 30 and 50 Hz, I from 17 to 32 mA) during sessions S16 and S17.
3.2.3. Sensations Evoked in the Phantom Hand Using Electrical Stimulation
- Only the sensation of touch was induced in the phantom hand in all cases, except in sessions S16 and S17 (maps of intensity and location shown in Figure A2, Appendix B).
- Stimulating on five channels with higher energy during sessions S16 and S17 added the sensation of warmth, tingling, and pricking.
- Stimulation with a high-energy level induced a more intense sensation in the phantom hand and extendedthe map for the location of sensation perceived when the duration of stimulus exceeded 40 min.
3.2.4. Perception of the Phantom Hand over Time
Even though no proprioceptive sensation was reported during procedures for sensation characterization, opening of the phantom hand (F1, F2, and F5) was reported during and after therapy sessions S13, S14, S16, and S17 (Figure 5). Opening of the phantom hand lasted between two and three hours after the end of the session and returned back to the tight-fist position. At the beginning of these sessions, the phantom hand was perceived, regularly, as a tight fist. This opening effect was not observed during the therapy session S15, where single-channel stimulation (23 series of 100 cycles) was randomly combined with multi-channel stimulation (10 series of 150 cycles).
3.2.5. Perception of Phantom Limb Pain over Time
The participant P2 had a relatively constant level of pain, 8 on VASP. It suddenly decreased to 6.5 after approximately 35 min of almost continuous stimulation (steady-state, bursts with Ton of 2 s and Toff of 0.2 s) in session S16. The reduction in pain lasted for approximately three hours after the stimulation session. The pain level decreased again from 8 to 6 on VASP in session S17, lasting almost four hours. During session S17, after approximately 30 min of stimulation, the participant reported a sensation of warmth and sensation of intense activity in the phantom hand described as a ‘boiling bubble’. The ‘bubble’ burst after approximately 5 min followed by PLP decrease.
4. Discussions
Methodological considerations. Performing the experiment was challenging in that each participant required the methodology to be adapted and customized. Various factors conditioned the outcome of the experiment, limiting the parameters, number, and duration of stimuli investigated, as well as location for delivery of these stimuli. These factors point towards the need of a more efficient means to quickly identify the referred sensation areas, with various stimuli, and their stimulus- and time-dependent characteristics. Reporting maps of RSAs determined using mechanical stimuli is methodologically convenient in that the point-wise dependency between application of the stimulus and type of sensation evoked allows for effective construction of the 2D map of RSAs for a given time. Constructing RSAs maps for electrical stimulation may be more challenging. Current is injected in the tissue through two points/areas, with a given course depending on the size, placement, and orientation of electrodes (as well as on parameters of the stimulus), making such maps multidimensional. The complex pattern of sensation induced using electrical stimulation of increasing intensities reported by the participant P1 emphasizes this aspect. By increasing the intensity of the stimulus, the volume of the current distributed in the tissue that meets conditions for stimulation increases as well. This may possibly lead to activation of additional neural fibers wiring the referred sensation areas. A dynamic pattern of sensation may thus be induced in the PH. Conversely, injecting the same current through electrodes of greater surface size would change the width and the depth of current distribution, possibly leading, as well, to a change of the type of sensation evoked. Furthermore, changes in the pattern of sensation induced in the PH following a prolonged stimulation (including altered PH perception and pain alleviation with delayed onset as shown in the case of participant P2) may involve various mechanisms along the neural circuit connecting the periphery with the brain, in addition to an expanded volume of stimulated tissue under the electrode due to increased energy of the stimulus. The effects of exposure of the neural tissue to an electrical stimulus is not limited to a single stimulus delivery. The total charge injected by delivering stimuli of various parameters over multiple trials and sessions spanning several days may have an accumulating effect and initiate adaptive neural responses, possibly affecting thresholds and inducing sensitization over time along the activated neural circuit. Sensation and discomfort thresholds were intently investigated once for each channel in a session during the baseline phase; however, they were repeated if needed at another phase of the experiment to estimate the working interval for the stimuli delivered during the procedure of sensation characterization. This estimation served avoiding delivering discomforting/painful stimuli and reduced the duration of a ramp stimulus by eliminating stimuli with intensities below the sensation threshold. Given the specificity (e.g., number and time-stability of RSAs, number of channels and channel configuration, types of sensations evoked in the PH) for each participant, characterization of sensation spanned over several sessions using stimuli with intensities based on thresholds estimated in the first phase of the experiment (effects of charge accumulation that is presumably relative low). However, the working range, defined using the sensation and discomfort thresholds, for multi-channel stimulation may have a non-linear relationship to that of single-channel stimulation, given the difference in the total charge injected into the tissue volume and the distribution of the current injected in case of a given configuration of electrodes defined for the corresponding tissue volume. Neither thresholds for multi-channel stimulation nor the time variability of thresholds of RSAs with each session were analyzed in this study. Values for current intensities in multi-channel stimulation were estimated based on the working range for single channels identified in the first phase of the study. Furthermore, the cumulative maps for sensation evoked in the PH reported data over several sessions, not counting possible effects of varying thresholds between sessions. A more complex characterization of referred sensation areas (e.g., temporal and spatial variability of thresholds, search procedures for optimal configuration of electrodes, time of exposure to stimuli, non-linearity for complex multi-channel and modulated stimuli delivery) calls for challenging methodological procedures that are to be considered in further studies investigating sensory feedback. The combination of technological advancement in wearable devices and prostheses may highly improve the detection of optimal stimuli, both mechanical and electrical, adaptively selecting in both time and space the contrasting pleasant and discomfort or painful evoked sensation.
Providing sensory feedback through RSAs. A relatively low and time-invariant and a relatively high and time-variant number of referred sensation areas were identified in participant P1 and P2, respectively, when using mechanical stimuli. Painful sensation was induced with mechanical stimulation of one referred sensation area and discomfort and sensations close to pain were induced with electrical stimulation in participant 1, whereas no painful sensations were induced in participant 2, either with mechanical or electrical stimuli. The sensation induced with electrical stimuli reached a wide representation of the four sub-modalities of somatosensation in participant P1, for relatively low duration of the stimulus and a mixed high- and low–high energy level for single- and multi-channel stimulation, respectively. In participant P2, almost continuous multi-channel stimulation with low-energy and a tenfold increase in duration (compared to that used in case of P1) applied during therapy led to the perception of a more open PH at the end of session S13, S14, S16, and S17 compared to that from the beginning of the corresponding session, even though no proprioceptive sensation was reported for the given stimuli during the procedure of sensation characterization. Although, the same was not observed in session S15 when single-channel stimulation was applied. By further increasing the energy of the stimulus, evoked sensation of warmth, tingling, and pins and needles, as well as PLP reduction, with delayed onset from 8 to 6 on VASP were reported in the phantom hand, as compared to the sensation of touch being solely evoked and there being no effect on PLP reported for stimuli with low-energy and low-duration. A similar complex image of the stimulation process, with both mechanical and electrical stimuli, was reported for other participants in the EPIONE study [43,44,45]. Pressure and tactile stimuli induced different maps of RSAs, with both painful and non-painful sensation evoked when applied on the same spot in the case of a participant with brachial plexus avulsion, followed by amputation [43]. Electrical stimuli evoked sensations different to those evoked using mechanical stimuli when electrodes were applied at or in the vicinity of the RSAs detected using mechanical stimuli. Even more, electrical stimuli applied through a pair of electrodes placed at two orthogonal positions during a test (i.e., rotating the placement of electrodes at 90 degrees) induced different sensations in the phantom hand. The participant reported, as well, experiencing the sensation of ‘phantom hand and arm coming to life’ during and between sessions. An immediate modulating effect of the given stimuli with both increasing or decreasing PLP was reported. In the case of a participant with transpelvic amputation, mechanical and electrical stimuli and electrical stimulation induced both pleasant and painful sensations in the phantom leg with lasting effects of minutes, inducing the perception of the phantom leg and foot as ‘coming to live’, possibly affecting the profile of PLP within and between sessions [44]. The development of maps of RSAs to a relatively large number over several sessions was observed in the case of a participant with bilateral toe amputation, with a relatively narrow representation of the sensations induced using mechanical and electrical stimuli [45]. Furthermore, in a study using contextual modulated electrical stimulation a participant with bilateral amputation reported complex dynamics of the sensations evoked when stimulating bilaterally, and evoked sensation and modulation of the pain profile in the contralateral phantom hand when stimulating RSAs on the ipsilateral stump [46].
5. Conclusions
Sensations evoked in the phantom hand using surface electrical stimulation of the referred sensation areas on the stump was characterized in two amputees, showing contrasting features. Both subjects reported a temporary modulation in their perception of their phantom hand (from ‘closed fist’ to ‘open hand’) that also was associated with a decrease in their experienced phantom limb pain, however, presenting differently. RSAs were dissimilarly stable or dynamic over time, adding to the particular manifestation of various stimuli and yet not fully knowing the nature (peripheral and/or central) of these areas in amputees.
Design of prostheses may cover parts of the stump, including referred sensation areas sensitive to pressure/tactile stimuli. Integrating knowledge of such negative effects (discomfort or pain) to prosthesis design may increase comfort for daily use of prostheses. Prostheses may offer, as well, a frame for contextual modulation in intensity/energy and time of electrical stimuli, better exploiting the dynamic effects they produce in the phantom hand, affecting the profile of the phantom limb pain and mobility and perception of the phantom hand. Even though mechanisms of phantom limb pain alleviation using artificially generated sensory input are not well understood, correlating a selective sensory input evoked using surface electrical stimulation with the daily use of prosthesis may add a new dimension in the design of active prosthesis towards personalized therapy.
Author Contributions
Conceptualization, W.J., K.Y. and E.R.L.; methodology, W.J. and E.R.L.; software, E.R.L.; investigation, W.J. and E.R.L.; writing—original draft preparation, W.J. and E.R.L.; writing—review and editing, W.J., K.Y. and E.R.L. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by EU FP7-HEALTH-2013-INNOVATION, project no. 602547 EPIONE.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of Region Nordjylland (Den Videnskabstetiske Komité for Region Nordjylland, N-20140061).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Conflicts of Interest
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Abbreviations
| EEG | Electroencephalography |
| MRI | Magnetic resonance imaging |
| BPI | Brief Pain Inventory |
| POMS | Profile of Mood States |
| NPSI | Neuropathic Pain Symptom Inventory |
| PGIC | Patient Global Impression of Change |
| PHQ9 | Patient Health Questionnaire |
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table A1.
Referred sensation areas and sensations induced in the phantom hand (PH) using mechanical stimulus (light brush).
Table A1.
Referred sensation areas and sensations induced in the phantom hand (PH) using mechanical stimulus (light brush).
| RSA | Induced Sensation (Cutaneous/Proprioceptive) |
|---|---|
| redRSA1brush | Tingling on upper left quadrant of dorsal side hand (VASS 7.1)/Fingers flexed, PH rotated with palmar side upwards |
| blackRSA2brush | Tingling, itching on F2, F5 dorsal side (VASS 6.1)/Fingers extended, PH rotated with dorsal side upwards |
| violetRSA3brush | Tingling on dorsal side of F3 and hand wrist (VASS 6.9)/Fingers extend; hand wrist extends; PH with dorsal side upwards |
| greenRSA4brush | Painful sensation on the entire dorsal side of hand (VASP 5.5)/Fingers flex; position |
Intensity of sensation evoked in the phantom hand reported by placing the cursor on a linear VASS scale for sensation (0 no sensation and 10 most intense sensation imagined); painful sensation reported on VASP scale for pain (0 no pain and 10 worst imaginable pain). Sensation described as cutaneous (mechanoreceptive, thermoreceptive, and nociceptive) and proprioceptive.
Table A2.
Sensations induced in the phantom hand (PH) using electrical stimuli.
| IThS–ThD/Pw/F | Induced Sensation (Cutaneous/Proprioceptive) |
|---|---|
| Ramp stimulus, as bursts/trains of pulses (rectangular and balanced bipolar) with Ton of 1 s and Toff of 1 s, with an increasing intensity of the current between the sensation threshold (ThS) and discomfort threshold (ThD). The participant stopped the ramp stimulus at the intensity (I) at which best perception of induced sensation was observed. The current intensity, sensation and discomfort thresholds, the pulse width, and the frequency of the stimulus IThS–ThD/Pw/F were expressed in milliamperes, microseconds and hertz, respectively. Single-channel stimulation (one channel at a time, randomized stimuli, twice for each set of parameters) for sensation characterization (SC) during sessions S3, S4, and S5. Repeated (randomized single channels) during session S7. | |
| RSA1—Ch1 | Session S3 |
| 1713–19/100/10 | Tingling, pricking F4 and F5, palmar side (VASS 7.1)/Fingers extended; Repeated at 24 mA13–25 Tingling, pricking F2 and F5 (VASS 4.4)/F2 felt like hanging and relaxed with no connection with PH; Session S7: Repeated at 25 mA15–25, Stabbing F4 and F5/Fingers rotated inwards towards each other, strange sensation |
| 1611–17/100/30 | Intense tingling F4 and F5, palmar side (VASS 6.8)/Fingers had less intense cyclic movement flexion-extension and rotation; Repeated at 19 mA9–21, F2 touch sensation (VASS 4.9); Session S7: Repeated at 18 mA11–25 Tingling F5 and F5 (VASS 4.7)/F4 and F5 moved towards each other (adduction) |
| 1911–19/100/70 | Intense tingling, diffuse around F4, F5 palmar side (VASS 6.5) and weak in F2; Repeated at 18 mA11–21 F2 touch sensation and F1 tingling (VASS 5.8), followed by a more diffuse perception of PH; Session S7: Repeated at 22 mA11–25 Tingling F4 and F5 (VASS 6.2)/Fingers flexed, F4 and F5 started from a flex position and flexed further to full closure and moved towards each other (adduction) |
| 117–17/200/10 | Pricking on entire hand, tingling on root of F5, palmar side (VASS 7.5); Session S7: Repeated at 16 mA9–17 Tingling F4, F5 (VASS 6)/F2 in a slight flexed position at stimulus onset and flexed more as stimulus increased and extended back to initial position towards stimulus offset |
| 117–11/200/30 | Tingling, pricking on root of F4 and F5, palmar side (VASS 6.8)/F4 stretched (pulling like sensation rather than extending); Session S7: Repeated at 12 mA7–15 Stabbing F4 and root of F5 (VASS 5.6)/F4 and F5 moved towards each other (adduction) |
| 107–11/200/70 | Tingling, intense pricking on entire F4 and F5 (VASS 8.2), slight irritating (not painful); Session S7: Repeated at 11 mA7–15 Tingling F2 (VASS 5.1) and/or on the stump under electrodes, cannot differentiate |
| 95–9/400/10 | Pricking root of F4, F5 palmar side (VASS 5.8)/Knocking like sensation in F4 from stimulus onset than pricking and F4 had tendency to rotate/dislocate from root; Session S7: Repeated at 9 mA5–11 Tingling, pricking F4 (mostly) and F5 (VASS 5.9) |
| 75–7/400/30 | Tingling, pricking on F4 (VASS 6.6); after stimulus offset it felt like relaxing effect after a hard workout/F4 stretched; Session S7: Repeated at 8 mA5–11 Tingling, stabbing F4, F5 (VASS 5.4)/F4 and F5 slightly flexed |
| 85–9/400/70 | Tingling, itching F4, F5 palmar side (VASS 7.6); perception of default sensation of PH was much more intense during this stimulus; Session S7: Repeated at 7 mA5–11 Tingling F4 (VASS 5.9), irritating |
| RSA2—Ch2 | Session S3 |
| 155–15/100/10 | Tingling F5 and stabbing F2, palmar side (VASS 5.4)/F2 flexed progressively with ramp stimulus; Session S7: Repeated at 19 mA7–25 F5 stabbing, knocking (VASS 3.9) |
| 135–15/100/30 | Tingling, pricking F5 and F2, palmar side (VASS 4.9)/F2 lightly stretched; Session S7: Repeated at 12 mA5–21 Could not feel much (VASS 1) |
| 135–13/100/70 | Pricking F5 and F2, palmar side (VASS 5.5)/F2 was in a flexed position before stimulus, it started to extend to a complete stretched position and moved towards F3 (adduction); Session S7: Repeated at 14 mA7–19 Tingling F2 and medial edge of hand (VASS 5.9), phantom hand felt cold |
| 105–11/200/10 | Very diffuse sensation, pricking F5 and pressure on F2 (VASS 6.4); Session S7: Repeated at 6 mA3–7 Pricking F2 (VASS 5.8), it felt like there were two index fingers; in one felt pricking whereas the other one stretched to full extension, very strange sensation |
| 93–9/200/30 | Pricking F5 and F2, palmar side (VASS 6.4)/F2 was in a slight flexed position before stimulus, it started to extend to a complete stretched position towards the end of the ramp; Session S7: Repeated at 9 m3–11 Tingling, pricking F2 (VASS 5) |
| 73–7/200/70 | Tingling F5 and F2, palmar side (VASS 5)/F2 was slightly flexed before stimulus, after stimulus onset F2 flexed further towards a closed position than it extended to a full stretched position towards the end of the ramp; Session S7: Repeated at 9 mA3–11 Tingling F5 (VASS 5.9)/F2 felt heavy and moved slightly |
| 63–7/400/10 | Diffuse, tingling, pricking, and stabbing F2, and pricking F5 palmar side (VASS 5.9), F2 slight discomfort; Session S7: Repeated at 10 mA5–11 Tingling F2-F5 (VASS 6.1) |
| 73–7/400/30 | Diffuse, tingling, pricking F5 and F2, palmar side (VASS 5.5)/F2 slightly extended; Session S7: Repeated at 6 mA3–7 Pricking F2 (VASS 5.8) |
| 73–7/400/70 | Tingling, pricking F5 and F2, palmar side (VASS 5.9)/F2 was in a slightly flexed position before stimulus onset than F2 extended with increasing ramp stimulus close towards a full stretched position; Sensation of cold on the stump under electrodes at stimulus offset; Session S7: Repeated at 7 mA3–9 Pricking F2 (VASS 6.5) |
| RSA3—Ch3 | Session S4 |
| 137–13/100/10 | Tingling and vibration F3, palmar side (VASS 6.5)/Fingers stretched, F3 sensation of touch, more diffuse sensation tingling on F2, F4, and F5, difficult to explain; Session S7: Repeated at 17 mA7–19 Pricking F2 (VASS 5.8)/F2 moved towards F3 (adduction) |
| 135–13/100/30 | Tingling and vibration F3, palmar side (VAS 4.9)/Fingers extended to almost full extent (stretched); Session S7: Repeated at 12 mA7–19 Tingling, pricking F2 (VASS 5.4)/F2 stretched |
| 115–11/100/70 | Tingling and itch sensation on F3 both palmar and dorsal sides (VAS 5.1)/F3 felt like it attempted to move away from the itch source; Session S7: Repeated at 14 mA5–19 Tingling, pricking, stabbing F2 (VASS 6) |
| 83–11/200/10 | Tingling F3, both palmar and dorsal sides (VAS 6.1)/F3 flexed; Session S7: Repeated at 10 mA3–11 Sticking, knocking, diffuse F2 (VASS 5.8) |
| 83–9/200/30 | Tingling F3, both palmar and dorsal sides (VAS 5.6)/F3 extended (stretched); Session S7: Repeated at 10 mA3–13 Sticking in most of the phantom hand, however, most intense on F3 (VASS 5.4)/F2 to F5 slight movements, strange, interesting/exciting |
| 93–9/200/70 | Intense tingling in F3, palmar and dorsal sides (VAS 6.7)/F3 light extension/stretch; Session S7: Repeated at 9 mA3–11 Tingling F2 (VASS 6.5)/F2 stretched at proximal (and not at the distant) interphalangeal joint |
| 63–7/400/10 | Light stretch with knocking sensation as slight discomfort in F3, both palmar and dorsal sides (VAS 7.4); Session S7: Repeated at 8 mA3–9 Pricking F2 (VASS 6) |
| 63–7/400/30 | Tingling F3, both palmar and dorsal sides, and central on dorsal side of hand (VAS 6.8)/F3 lightly stretched and sensation like warm water running down the finger was felt towards the end of the ramp stimulus |
| 63–7/400/70 | Tingling as spinning F3, both palmar and dorsal sides, (VAS 7)/F3 lightly stretched; Session S7: Repeated at 6 mA3–7 Very diffuse sensation, could not describe (VASS 5.5) |
| RSA4—Ch4 | Session S5 |
| 1911–25/100/10 | Tingling and vibration F1, palmar and dorsal (VAS 3.7)/F1 moved towards F2 (adduction); Session S7: Repeated at 2111–25 F1 thenar tingling (VAS 1.9) |
| 189–19/100/30 | Tingling and vibration F1, palmar side (VAS 3.7)/F1 moved towards F2 (adduction), seemed like F1 was positioned close to the stimulating electrode, away from the phantom hand; Session S7: Repeated at 1911–25 F1(thenar area) spinning and muscle contraction (VAS 5) |
| 2011–25/100/70 | Diffuse tingling and vibration F1, palmar side (VAS 4.3)/F1 moved towards F2 (adduction, sensation of muscle contraction, adductor pollicis), light discomfort; Session S7: Repeated at 249–25 F1(thenar area) spinning and muscle contraction (VAS 5) |
| 157–19/200/10 | Diffuse tingling, vibration, provoking sticking and knocking F1, palmar side (VAS 4.8); Session S7: Repeated at 207–23 F1(thenar area) tingling with weak muscle contraction (VAS 3.5) |
| 115–13/200/30 | Tingling, sticking and knocking F1, palmar side (VAS 4.9); Session S7: Repeated at 185–21 F1 tingling and thenar muscle contraction (VAS 4.6) |
| 147–17/200/70 | Tingling, stinging F1, palmar side (VAS 5.9), strange and diffuse sensation; Session S7: Repeated at 145–19 F1 thenar tingling (VAS 4.6) |
| 125–13/400/10 | Diffuse sensation F1 (VAS 6.5), difficult to evaluate/F1 adductor muscle contraction, with adduction and rotation of F1; Session S7: Repeated at 143–15 F1(thenar area) tingling and muscle contraction (VAS 4.1) |
| 115–11/400/30 | Diffuse sensation on F1 palmar side (VAS 5.8), difficult to evaluate; Session S7: Repeated at 113–13 F1 (thenar area) tingling and muscle contraction (VAS 5.5) |
| 105–11/400/70 | Diffuse tingling, stinging F1 (VAS 6.4); Session S7: Repeated at 115–13 F1 thenar area tingling (VAS 5.7) |
| Multi-channel | Session S5, Four-channel stimulation Steady state stimuli of 20 s duration (Bursts/pulse trains, Ton 1 s and Toff 1 s) |
| 10-7-10-15100/10 | Diffuse, no definite sensation felt on PH/The entire PH moved slightly |
| 18-11-12-20100/10 | Diffuse tingling F1, F2 itchy (VAS 6.2)/F2 extended slightly, F1 contraction of adductor pollicis, entire PH slightly moved |
| 10-5-8-15100/10 | Diffuse tingling F1, F2 palmar side (VAS 6.2)/F2 extension, F1 contraction of adductor pollicis, the other fingers slightly moved |
| 15-7-10-15100/30 | Diffuse tingling on hypothenar region, stinging and tingling on palmar side of F3 (most intense) and F4, and light tingling on F2 and F5 (VAS 6) |
| 17-11-12-18100/30 | Diffuse and very intense tingling, equally on F1 (thenar region), F2, F3, F4, and F5, palmar side (VAS 6.4); it felt like the brain was overloaded with this sensation and at the end of the stimulus a strong sensation of relief was perceived |
| 15-7-7-15100/70 | Tingling F1 (thenar region), F2, F3, F4, and F5, palmar side (VAS 6.4) perceived as very pleasant relaxing sensation similar to that of massage |
| 18-11-10-20100/70 | Tingling, stinging F2, F3, F4, and F5, and tingling on hypothenar region (VAS 5.8)/All fingers slightly stretched (extension) |
| 8-7-6-10200/10 | Diffuse tingling F2, F3, F4, and F5 (VAS 5.3)/The four fingers slightly moved/extended and on F1 muscle contractions (thenar region) like sensation was felt; after stimulus offset F2 and F3 felt rapidly to the initial flexed position, for F4 and F5 it took longer to fall back to the initial flexed position |
| 10-10-10-17200/10 | Diffuse spinning F2 and tingling, stinging F4 and F5 (VAS 6.6)/F3 flexed and on F1 small muscle contractions (thenar region) like sensation |
| 8-5-5-8200/30 | Diffuse sensation of all finger flexion and muscle contraction on fingers (VAS 5.1) |
| 10-8-8-11200/30 | Diffuse tingling in all fingers, slight discomfort (VAS 6.8) |
| 8-4-5-10200/70 | Tingling on stinging on all finger (VAS 6.3)/F2 moves slightly lateral |
| 10-5-8-15200/70 | Diffuse tingling and stinging in all fingers (F1–F5); first felt on F1 and F2 than F3 followed by F4 and some on F5 |
| 6-4-4-7400/10 | Tingling, stinging, and knocking on F1, F2, and F3 perceived as slight discomfort/F4 and F5 moves away, lateral, from F3 |
| 8-5-5-11400/10 | Knocking and tingling on all fingers (for F1 on thenar region), discomforting close to pain level. |
| 5-4-4-7400/30 | Tingling and spinning on all fingers (VAS 6.2); on F2 dorsal side a needle like sensation (not painful) was perceived |
| 6-3-4-9400/70 | Diffuse and intense spinning on all fingers (VAS 5.5)/All fingers small muscle contractions (like flexing fingers, without fingers movement) |
| Multi-channel Session S8, S9, S10, and S12 Two-channel and three-channel stimulation; steady-state stimuli of 20 s duration (Bursts/pulse trains, Ton of 1 s and Toff of 1 s). Most of the evoked sensations when stimulating on two or three channels (random choice of stimulation parameters) were close/similar to that of summation of sensation evoked with stimulation on a single channel. However, the following deviated considerably from this pattern. | |
| Two-channel stimulation | |
| 13-/-9-/200/70 | /F2 moved away from the other fingers |
| 23-/-17-/100/70 | /F2 moved away from F3 (abduction) |
| 8-/-5-/400/10 | Very strange sensation, could not explain |
| 15-13-/-/200/10 | /F5 rotated (provoking sensation) and seemed that it took F4 in this type of movement |
| 7-/-4-/400/70 | Intense stinging, tingling F1 on palmar side, intense tingling at root of F2–F4 on dorsal side (VASS 6.7) |
| 17-11-/-/100/70 | Tingling F2 on palmar side, sensation of touch similar to that given by a crawling spider on dorsal side of phantom hand, very discomforting |
| 10-/-/-11200/70 | /F1 moved towards F2 (adduction), F2 and F3 felt very heavy at the root |
| /-13-9-/200/10 | Knocking and tingling F2 (VASS 5.4)/Entire phantom hand felt very heavy, relaxed like tiredness after intense physical effort |
| /-17-17-/100/70 | Stinging F2, tingling F3 and F5 (VASS 6.2)/F3 felt heavy |
| 23-/-/-23100/70 | Tingling F1 to F5 (VASS 6.7)/F1 muscle contraction, F3 felt heavy |
| 12-/-/-14200/10 | Tingling F1, light stinging F2 to F5 (VASS 5.4)/F1 muscle contraction, F1 to F5 and felt heavy |
| /-12-12-/100/30 | /Perception of PH completely different than usual, F2 and F3 changed place; it reversed when stimulation ceased |
| /-4-5-/400/30 | Stinging and itchy F2, intense burning sensation in F1 close to discomfort |
| /-6-7-/400/30 | Tingling and stinging F2, F1 stinging (VASS 5.7)/F1 felt very heavy |
| /-6-7-/400/10 | Tingling and stinging F2, stinging F1 (VASS 6.4)/F1 felt very heavy |
| 10-5-/-/200/30 | Tingling and stinging F5 at discomfort, tingling F2, F3, and F5 as well, shadowed by F5 |
| 10-9-/-/400/10 | Stinging F5 discomfort/F5 rotated |
| 13-/-9-/200/70 | /F2 moved away from the other fingers |
| 17-2-/-/100/30 | Tingling F3 (VASS 6.3)/F3 felt very heavy |
| /-/-5-7400/30 | Stinging and tingling F1 and F3 (VASS 4.3)/F3 felt very heavy |
| /-/-11-18200/30 | Tingling, pricking F2 and F3, numbness F2 (VASS 6.3)/F1 muscle contractions, F2 felt very heavy |
| /-/-17-23100/10 | Pricking F3 (VASS 4.5)/F2 felt heavy |
| /-/-11-16100/70 | Intense itching F1 (thenar region) (VASS 4.4) |
| Three-channel stimulation | |
| 19-15-12-/100/10 | /F5 rotates, discomfort |
| 13-11-/-18200/30 | Tingling entire palmar side, discomfort |
| 17-11-11-/100/70 | Tingling F5, F3, and F2 (VASS 5.9)/F2 and F3 moved away from each other (abduction) |
| 8-7-5-/400/10 | Stinging F2 and F3 (VASS 6)/F3 flexed and spread apart from F2 (flexion and abduction) |
| 10-5-7-12200/30 | Tingling F1, F3, and F5 and stinging F2 (VASS 5.5)/F1 muscle contraction (adductor pollicis, no movement) and entire hand felt very heavy (Note: see effect of removing Ch1 from multi-channel stimulation on four-channel to three-channel stimulation, as below) |
| /-5-7-12200/30 | Tingling F2 (VASS 4.1)/F3 and F5 felt very heavy |
| /-15-12-17100/10 | Tingling F1 and F2 (VASS 3.7)/F5 felt heavy |
| /-22-17-23100/10 | Tingling F1 (VAS 3.9)/F1 muscle contraction (no movement of F1), F2, F3, and F5 felt heavy |
| /-7-5-8400/10 | Tingling F2 (VASS 4.5)/The entire phantom hand became heavy, it felt even more heavy as the stimulation continued; close to the stimulation offset this sensation reached a close to discomfort level (e.g., longer stimulation would be discomfort, whereas shorter stimulation non-painful) |
| /-5-7-12400/30 | Stinging F1, F2 to F5 warm and light burning sensation (VASS 6.8) |
| /-12-12-17100/30 | Tingling F1 (thenar) and F5 (VASS 4)/F2 and F5 felt heavy |
| /-13-9-20200/10 | F5 painful stinging/F1 (thenar) muscle contraction |
| /-9-11-18200/30 | Tingling F5 (VASS 5.9)/F1 (thenar) muscle contraction, F5 felt heavy |
| /-6-/-11200/70 | Tingling F1 (thenar) and F5 (VASS 4.3)/F5 felt heavy |
| /-7-6-11400/70 | Tingling F2, less intense F3, very intense F5 (VASS 5.2)/F1 (thenar) muscle contraction, F5 felt heavy |
| 23-/-/-23100/30 | Tingling F4 and sensation of pressure like clamping/squeezing F5 (VASS 5.6)/F1 (thenar) muscle contraction |
| 15-/-/-20200/10 | Tingling F1 (thenar) (VASS 5.7)/F1 (thenar) muscle contraction, F3, F4 and F5 felt heavy |
Appendix B
Figure A1.
(a) Reference system for reporting location and size of RSAs in upper-limb amputees enrolled in the EPIONE protocol. For participant P2 with transradial amputation, the reference line was drawn through the point R2 (middle of the antecubital fossa, regarded as the origin of the reference system) and a point R3 (defined using a scar on the stump at the amputation site) so that it reaches the acromioclavicular point (R1) when straightening the arm (in a position imagined with PH facing upwards). Three grid lines, segmented at 50 mm, normal to the reference line were drawn, dividing the reference line in two segments of 100 mm in the middle, one of 70 mm on the top, and one of 30 mm at the bottom. For participant P1 with the transhumeral amputation, the reference line was drawn through the point R1 and R3 (defined using a scar on the stump at the amputation site). The origin of the reference system was R3. The RSA reported through this reference system was approximated with an ellipse defined using center coordinates (distances along and normal to the reference line), major and minor diameters, and angle formed with the long axis of the ellipse to the reference line (see inset for the sign of these measures). The stump/arm was approximated with a cylinder. The surface of the cylinder in 3D was mapped to the 2D plane (surface at the amputation site rolled out in prolongation of the cylinder surface) showing the maps of RSAs and position of electrodes relative to these maps. Variations of referred sensation areas and cumulative maps for participant P2 are illustrated in the panels (b1,b2,c1,c2) and (d) as follows: (b1) The six-channel configuration for position of electrodes relative to the map of RSAs identified during session S5 (as shown on images from Figure 4a); this configuration of electrodes was used from session S5 to session S11. (b2) The five-channel configuration for position of electrodes relative to the map of RSAs identified during session S12; this configuration of electrodes was used from session S12 to session S19. (c) Cumulative maps for intensity (VASS scale, 0 no sensation, 10 most intense sensation perceivable, colorbar) and location (top panel) and rate of occurrence (normalized units, colorbar) of sensation evoked using the light brush (test with light pressure applied with the glass ball showed similar maps) during (c1) session S5 and (c2) session S12. Only sensation of touch was induced using brush/pressure; drawings at scale relative to grid lines, reference line, and the points R1 and R3. (d) Maps of RSAs identified with the light brush during sessions S1, S2, S3, and S4.
Figure A1.
(a) Reference system for reporting location and size of RSAs in upper-limb amputees enrolled in the EPIONE protocol. For participant P2 with transradial amputation, the reference line was drawn through the point R2 (middle of the antecubital fossa, regarded as the origin of the reference system) and a point R3 (defined using a scar on the stump at the amputation site) so that it reaches the acromioclavicular point (R1) when straightening the arm (in a position imagined with PH facing upwards). Three grid lines, segmented at 50 mm, normal to the reference line were drawn, dividing the reference line in two segments of 100 mm in the middle, one of 70 mm on the top, and one of 30 mm at the bottom. For participant P1 with the transhumeral amputation, the reference line was drawn through the point R1 and R3 (defined using a scar on the stump at the amputation site). The origin of the reference system was R3. The RSA reported through this reference system was approximated with an ellipse defined using center coordinates (distances along and normal to the reference line), major and minor diameters, and angle formed with the long axis of the ellipse to the reference line (see inset for the sign of these measures). The stump/arm was approximated with a cylinder. The surface of the cylinder in 3D was mapped to the 2D plane (surface at the amputation site rolled out in prolongation of the cylinder surface) showing the maps of RSAs and position of electrodes relative to these maps. Variations of referred sensation areas and cumulative maps for participant P2 are illustrated in the panels (b1,b2,c1,c2) and (d) as follows: (b1) The six-channel configuration for position of electrodes relative to the map of RSAs identified during session S5 (as shown on images from Figure 4a); this configuration of electrodes was used from session S5 to session S11. (b2) The five-channel configuration for position of electrodes relative to the map of RSAs identified during session S12; this configuration of electrodes was used from session S12 to session S19. (c) Cumulative maps for intensity (VASS scale, 0 no sensation, 10 most intense sensation perceivable, colorbar) and location (top panel) and rate of occurrence (normalized units, colorbar) of sensation evoked using the light brush (test with light pressure applied with the glass ball showed similar maps) during (c1) session S5 and (c2) session S12. Only sensation of touch was induced using brush/pressure; drawings at scale relative to grid lines, reference line, and the points R1 and R3. (d) Maps of RSAs identified with the light brush during sessions S1, S2, S3, and S4.

Figure A2.
Cumulative maps for intensity (VASs; 0 = no sensation, 10 = most intense non-painful sensation perceivable) and location (top panel) and cumulative maps for rate of occurrence (normalized) for a given location (bottom panel) of non-painful sensation evoked in the phantom hand using electrical stimuli. The six-channel configuration for placement of electrodes was used from session S5 to session S11. The five-channel configuration for placement of electrodes was used from session S12 to session S19 (Figure A1) (a) session S8, single-channel stimulation, randomized on Ch1 to Ch4 (b) session S10, multi-channel stimulation, randomized on Ch1 to Ch4 (c) session S11, single-channel stimulation, randomized on Ch1 to Ch6 (d) session S11, multi-channel stimulation, randomized on Ch1 to Ch5 (e) session S12, multi-channel stimulation, randomized on Ch1 to Ch5, with low-energy stimulus (stimulus intensity below the mean value of the interval between sensation threshold and discomfort threshold) (f) session S16 and S17 multi-channel stimulation, randomized on Ch1 to Ch5, with high-energy stimulus (stimulus intensity above the mean value of the interval between sensation threshold and discomfort threshold).
Figure A2.
Cumulative maps for intensity (VASs; 0 = no sensation, 10 = most intense non-painful sensation perceivable) and location (top panel) and cumulative maps for rate of occurrence (normalized) for a given location (bottom panel) of non-painful sensation evoked in the phantom hand using electrical stimuli. The six-channel configuration for placement of electrodes was used from session S5 to session S11. The five-channel configuration for placement of electrodes was used from session S12 to session S19 (Figure A1) (a) session S8, single-channel stimulation, randomized on Ch1 to Ch4 (b) session S10, multi-channel stimulation, randomized on Ch1 to Ch4 (c) session S11, single-channel stimulation, randomized on Ch1 to Ch6 (d) session S11, multi-channel stimulation, randomized on Ch1 to Ch5 (e) session S12, multi-channel stimulation, randomized on Ch1 to Ch5, with low-energy stimulus (stimulus intensity below the mean value of the interval between sensation threshold and discomfort threshold) (f) session S16 and S17 multi-channel stimulation, randomized on Ch1 to Ch5, with high-energy stimulus (stimulus intensity above the mean value of the interval between sensation threshold and discomfort threshold).

References
- Heavey, E. The multiple meanings of ‘disability’ in interviews with amputees. Commun. Med. 2014, 10, 129–139. [Google Scholar] [CrossRef] [PubMed]
- McDonald, C.L.; Bennett, C.L.; Rosner, D.K.; Steele, K.M. Perceptions of ability among adults with upper limb absence: Impacts of learning, identity, and community. Disabil. Rehabil. 2020, 42, 3306–3315. [Google Scholar] [CrossRef] [PubMed]
- Bekrater-Bodmann, R.; Reinhard, I.; Diers, M.; Fuchs, X.; Flor, H. Relationship of prosthesis ownership and phantom limb pain: Results of a survey in 2383 limb amputees. Pain 2020, 162, 630. [Google Scholar] [CrossRef]
- Cordella, F.; Ciancio, A.L.; Sacchetti, R.; Davalli, A.; Cutti, A.G.; Guglielmelli, E.; Zollo, L. Literature Review on Needs of Upper Limb Prosthesis Users. Front. Neurosci. 2016, 10, 209. [Google Scholar] [CrossRef] [PubMed]
- Collins, K.L.; Russell, H.G.; Schumacher, P.J.; Robinson-Freeman, K.E.; O’conor, E.C.; Gibney, K.D.; Yambem, O.; Dykes, R.W.; Waters, R.S.; Tsao, J.W. A review of current theories and treatments for phantom limb pain. J. Clin. Investig. 2018, 128, 2168. [Google Scholar] [CrossRef] [PubMed]
- Erlenwein, J.; Diers, M.; Ernst, J.; Schulz, F.; Petzke, F. Clinical updates on phantom limb pain. Pain Rep. 2021, 6, e888. [Google Scholar] [CrossRef]
- Antfolk, C.; D’Alonzo, M.; Rosén, B.; Lundborg, G.; Sebelius, F.; Cipriani, C. Sensory feedback in upper limb prosthetics. Expert Rev. Med. Devices 2013, 10, 45–54. [Google Scholar] [CrossRef]
- Antfolk, C.; Cipriani, C.; Carrozza, M.C.; Balkenius, C.; Björkman, A.; Lundborg, G.; Rosén, B.; Sebelius, F. Transfer of tactile input from an artificial hand to the forearm: Experiments in amputees and able-bodied volunteers. Disabil. Rehabil. 2013, 8, 249–254. [Google Scholar] [CrossRef]
- Wijk, U.; Carlsson, I.K.; Antfolk, C.; Björkman, A.; Rosén, B. Sensory Feedback in Hand Prostheses: A Prospective Study of Everyday Use. Front. Neurosci. 2020, 14, 663. [Google Scholar] [CrossRef]
- Petersen, B.A.; Nanivadekar, A.C.; Chandrasekaran, S.; Fisher, L.E. Phantom limb pain: Peripheral neuromodulatory and neuroprosthetic approaches to treatment. Muscle Nerve 2018, 59, 154. [Google Scholar] [CrossRef]
- Lathouwers, E.; Díaz, M.A.; Maricot, A.; Tassignon, B.; Cherelle, C.; Cherelle, P.; Meeusen, R.; De Pauw, K. Therapeutic benefits of lower limb prostheses: A systematic review. J. NeuroEng. Rehabil. 2023, 20, 4. [Google Scholar] [CrossRef] [PubMed]
- Rauck, R.L.; Kapural, L.; Cohen, S.P.; North, J.M.; Gilmore, C.A.; Zang, R.H.; Boggs, J.W. Peripheral Nerve Stimulation for the Treatment of Postamputation Pain-A Case Report. Pain Pract. 2012, 12, 649–655. [Google Scholar] [CrossRef] [PubMed]
- Rauck, R.L.; Cohen, S.P.; Gilmore, C.A.; North, J.M.; Kapural, L.; Zang, R.H.; Grill, J.H.; Boggs, J.W. Treatment of Post-Amputation Pain With Peripheral Nerve Stimulation. Neuromodulation 2014, 17, 188–197. [Google Scholar] [CrossRef] [PubMed]
- Dietrich, C.; Nehrdich, S.; Seifert, S.; Blume, K.R.; Miltner, W.H.R.; Hofmann, G.O.; Weiss, T. Leg Prosthesis With Somatosensory Feedback Reduces Phantom Limb Pain and Increases Functionality. Front. Neurol. 2018, 9, 270. [Google Scholar] [CrossRef] [PubMed]
- Trent, L.; Intintoli, M.; Prigge, P.; Bollinger, C.; Walters, L.S.; Conyers, D.; Miguelez, J.; Ryan, T. A narrative review: Current upper limb prosthetic options and design. Disabil. Rehabil. 2020, 15, 604–613. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro, J.; Mota, F.; Cavalcante, T.; Nogueira, I.; Gondim, V.; Albuquerque, V.; Alexandria, A. Analysis of Man-Machine Interfaces in Upper-Limb Prosthesis: A Review. Robotics 2019, 8, 16. [Google Scholar] [CrossRef]
- Roche, A.D.; Bailey, Z.K.; Gonzalez, M.; Vu, P.P.; Chestek, C.A.; Gates, D.H.; Kemp, S.W.P.; Cederna, P.S.; Ortiz-Catalan, M.; Aszmann, O.C. Upper limb prostheses: Bridging the sensory gap. J. Hand. Surg. Eur. Vol. 2023, 48, 182. [Google Scholar] [CrossRef] [PubMed]
- Raspopovic, S.; Valle, G.; Petrini, F.M. Sensory feedback for limb prostheses in amputees. Nat. Mater. 2021, 20, 925–939. [Google Scholar] [CrossRef]
- D’anna, E.; Petrini, F.M.; Artoni, F.; Popovic, I.; Simanić, I.; Raspopovic, S.; Micera, S. A somatotopic bidirectional hand prosthesis with transcutaneous electrical nerve stimulation based sensory feedback. Sci. Rep. 2017, 7, 10930. [Google Scholar] [CrossRef]
- Micera, S. Staying in Touch: Toward the Restoration of Sensory Feedback in Hand Prostheses Using Peripheral Neural Stimulation. IEEE Pulse 2016, 7, 16–19. [Google Scholar] [CrossRef]
- Raspopovic, S.; Cimolato, A.; Panarese, A.; Vallone, F.; del Valle, J.; Micera, S.; Navarro, X. Neural signal recording and processing in somatic neuroprosthetic applications. A review. J. Neurosci. Methods 2020, 337, 108653. [Google Scholar] [CrossRef] [PubMed]
- Schofield, J.S.; Evans, K.R.; Carey, J.P.; Hebert, J.S. Applications of sensory feedback in motorized upper extremity prosthesis: A review. Expert Rev. Med. Devices 2014, 11, 499–511. [Google Scholar] [CrossRef] [PubMed]
- Marinelli, A.; Boccardo, N.; Tessari, F.; Di Domenico, D.; Caserta, G.; Canepa, M.; Gini, G.; Barresi, G.; Laffranchi, M.; De Michieli, L.; et al. Active upper limb prostheses: A review on current state and upcoming breakthroughs. Prog. Biomed. Eng. 2023, 5, 012001. [Google Scholar] [CrossRef]
- Windrich, M.; Grimmer, M.; Christ, O.; Rinderknecht, S.; Beckerle, P. Active lower limb prosthetics: A systematic review of design issues and solutions. Biomed. Eng. Online 2016, 15, 140. [Google Scholar] [CrossRef] [PubMed]
- Middleton, A.; Ortiz-Catalan, M. Neuromusculoskeletal Arm Prostheses: Personal and Social Implications of Living with an Intimately Integrated Bionic Arm. Front. Neurorobot. 2020, 14, 39. [Google Scholar] [CrossRef]
- Basla, C.; Chee, L.; Valle, G.; Raspopovic, S. A non-invasive wearable sensory leg neuroprosthesis: Mechanical, electrical and functional validation. J. Neural Eng. 2022, 19, 16008. [Google Scholar] [CrossRef]
- Lloyd-Esenkaya, T.; Lloyd-Esenkaya, V.; O’Neill, E.; Proulx, M.J. Multisensory inclusive design with sensory substitution. Cogn. Res. 2020, 5, 37. [Google Scholar] [CrossRef]
- Risso, G.; Preatoni, G.; Valle, G.; Marazzi, M.; Lle, N.; Bracher, M. Multisensory stimulation decreases phantom limb distortions and is optimally integrated. iScience 2022, 25, 104129. [Google Scholar] [CrossRef]
- Geng, B.; Jensen, W. Human ability in identification of location and pulse number for electrocutaneous stimulation applied on the forearm. J. Neuroeng. Rehabil. 2014, 11, 97. [Google Scholar] [CrossRef]
- Kuiken, T.A.; Marasco, P.D.; Lock, B.A.; Harden, R.N.; Dewald, J.P.A. Redirection of cutaneous sensation from the hand to the chest skin of human amputees with targeted reinnervation. Proc. Natl. Acad. Sci. USA 2007, 104, 20061–20066. [Google Scholar] [CrossRef]
- Chee, L.; Valle, G.; Preatoni, G.; Basla, C.; Marazzi, M.; Raspopovic, S. Cognitive benefits of using non-invasive compared to implantable neural feedback. Sci. Rep. 2022, 12, 16696. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez, M.; Bismuth, A.; Lee, C.; Chestek, C.A.; Gates, D.H. Artificial referred sensation in upper and lower limb prosthesis users: A systematic review. J. Neural Eng. 2022, 19, 51001. [Google Scholar] [CrossRef] [PubMed]
- Chai, G.; Sui, X.; Li, S.; He, L.; Lan, N. Characterization of evoked tactile sensation in forearm amputees with transcutaneous electrical nerve stimulation. J. Neural Eng. 2015, 12, 066002. [Google Scholar] [CrossRef] [PubMed]
- Osumi, M.; Shimizu, D.; Nishi, Y.; Morioka, S. Electrical stimulation of referred sensation area alleviates phantom limb pain. Restor. Neurol. Neurosci. 2021, 39, 101–110. [Google Scholar] [CrossRef] [PubMed]
- Salminger, S.; Stino, H.; Pichler, L.H.; Gstoettner, C.; Sturma, A.; Mayer, J.A.; Szivak, M.; Aszmann, O.C. Current rates of prosthetic usage in upper-limb amputees—Have innovations had an impact on device acceptance? Disabil. Rehabil. 2022, 44, 3708. [Google Scholar] [CrossRef] [PubMed]
- Flor, H.; Nikolajsen, L.; Staehelin Jensen, T. Phantom limb pain: A case of maladaptive CNS plasticity? Nat. Rev. Neurosci. 2006, 7, 873–881. [Google Scholar] [CrossRef] [PubMed]
- Andoh, J.; Milde, C.; Diers, M.; Bekrater-Bodmann, R.; Trojan, J.; Fuchs, X.; Becker, S.; Desch, S.; Flor, H. Assessment of cortical reorganization and preserved function in phantom limb pain: A methodological perspective. Sci. Rep. 2020, 10, 11504. [Google Scholar] [CrossRef] [PubMed]
- Bramati, I.E.; Rodrigues, E.C.; Simões, E.L.; Melo, B.; Höfle, S.; Moll, J.; Lent, R.; Tovar-Moll, F. Lower limb amputees undergo long-distance plasticity in sensorimotor functional connectivity. Sci. Rep. 2019, 9, 2518. [Google Scholar] [CrossRef]
- Granata, G.; Valle, G.; Di Iorio, R.; Iodice, F.; Petrini, F.M.; Strauss, I.; D’anna, E.; Iberite, F.; Lauretti, L.; Fernandez, E.; et al. Cortical plasticity after hand prostheses use: Is the hypothesis of deafferented cortex “invasion” always true? Clin. Neurophysiol. 2020, 131, 2341–2348. [Google Scholar] [CrossRef]
- Makin, T.R.; Flor, H. Brain (re)organisation following amputation: Implications for phantom limb pain. NeuroImage 2020, 218, 116943. [Google Scholar] [CrossRef]
- Makin, T.R.; Scholz, J.; Henderson Slater, D.; Johansen-Berg, H.; Tracey, I. Reassessing cortical reorganization in the primary sensorimotor cortex following arm amputation. Brain 2015, 138, 2140–2146. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.J.; Zhang, Y.J.; Wang, L.; Sang, L.; Li, L.L.; Li, P.L.; Yin, X.; Qiu, M. Brain Functional Connectivity Plasticity Within and Beyond the Sensorimotor Network in Lower-Limb Amputees. Front. Hum. Neurosci. 2018, 12, 403. [Google Scholar] [CrossRef] [PubMed]
- Lontis, E.R.; Yoshida, K.; Jensen, W. Features of Referred Sensation Areas for Artificially Generated Sensory Feedback—A Case Study. In Proceedings of the 2018 40th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Honolulu, HI, USA, 18–21 July 2018; pp. 3533–3536. [Google Scholar] [CrossRef]
- Lontis, E.R.; Yoshida, K.; Jensen, W. Referred Sensation Areas in Transpelvic Amputee. In Proceedings of the 2019 41st Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Berlin, Germany, 23–27 July 2019; pp. 6458–6461. [Google Scholar] [CrossRef]
- Lontis, E.R.; Yoshida, K.; Jensen, W. Referred Sensation Areas in a Bilateral Toes Amputee. In Proceedings of the 2020 42nd Annual International Conference of the IEEE Engineering in Medicine & Biology Society (EMBC), Montreal, QC, Canada, 20–24 July 2020; pp. 3569–3572. [Google Scholar] [CrossRef]
- Lontis, E.R.; Jensen, W. Referred Sensation Areas in a Bilateral Upper Limb Amputee. In Proceedings of the 45th Annual International Conference of the IEEE Engineering in Medicine and Biology Society 2023, Sydney, Australia, 24–27 July 2023. [Google Scholar]
- Sugiyama, S.; Takasugi, J.; Hirano, Y.; Shimizu, E. A case of thigh amputee supporting immediate plastic changes in the somatosensory cortex: Observation of changes over time in the representation of referred phantom sensation. J. Rehabil. Neurosci. 2022, 22, 221401. [Google Scholar] [CrossRef]
- Yoshida, K.; Malec, L.; Comoglio, C.; Mosier, K.; Lontis, R.; Larsen, K.; Navarro, X.; Jensen, W. Evaluation of the effect of sensory feedback on phantom limb pain in multi-center clinical trial. In Proceedings of the 3rd International Conference on NeuroRehabilitation (ICNR2016), Segovia, Spain, 18–21 October 2016; pp. 725–730. [Google Scholar]
- Jensen, W. Natural sensory feedback for phantom limb pain modulation and therapy. In Proceedings of the 3rd International Conference on NeuroRehabilitation (ICNR2016), Segovia, Spain, 18–21 October 2016; pp. 719–723. [Google Scholar]
Figure 1.
Phases of EPIONE protocol and timeline (in weeks) for sessions for the two participants. In week zero (w0), no procedures were performed. Pre-screening session S0 not included. Baseline and entry sessions for participant P1 were carried out on Mondays and Fridays, and therapy sessions were carried out on all weekdays in week 1, 2 (except Thursday) and in week 3 (except Monday and Tuesday). Baseline and entry sessions for participant P2 were carried out on Mondays and Wednesdays; therapy sessions were carried out on Mondays, Wednesdays, and Fridays in week 1, 2, 3, and 4 (except Friday in this week). The follow-up phase (week 6, 8, and 12) is not represented in the figure.
Figure 1.
Phases of EPIONE protocol and timeline (in weeks) for sessions for the two participants. In week zero (w0), no procedures were performed. Pre-screening session S0 not included. Baseline and entry sessions for participant P1 were carried out on Mondays and Fridays, and therapy sessions were carried out on all weekdays in week 1, 2 (except Thursday) and in week 3 (except Monday and Tuesday). Baseline and entry sessions for participant P2 were carried out on Mondays and Wednesdays; therapy sessions were carried out on Mondays, Wednesdays, and Fridays in week 1, 2, 3, and 4 (except Friday in this week). The follow-up phase (week 6, 8, and 12) is not represented in the figure.

Figure 2.
(a) RSAs identified using tactile stimuli (brush). (a1) Maps of location—intensity of sensation evoked in the phantom hand using brush, for each RSA. For RSA1, 2, and 3 on a VASS (0 = no sensation, 10 = most intense non-painful sensation perceivable) and for RSA 4 on VASP (0 = no pain and 10 = worst imaginable pain), VAS score is presented for each RSA in Appendix A, Table A1. (b) Position of electrodes on and around RSAs, for each channel, and cumulative maps of location-intensity (VASS, colorbar), top panel, and location-rate of occurrence (normalized units, colorbar), bottom panel, of sensation in phantom hand evoked using electrical stimuli; (b1) single-channel stimulation for Ch1, 2, 3, and 4 (left to right); (b2) single-channel stimulation combined, randomized Ch1, 2, 3, and 4 (b3) multi-channel stimulation on two channels, combined; (b4) multi-channel stimulation on three channels, combined; (b5) multi-channel stimulation on four channels, combined. Multi-channel stimulation for a given channel configuration was performed on all possible combinations (e.g., two-channel configuration yielded six combinations).
Figure 2.
(a) RSAs identified using tactile stimuli (brush). (a1) Maps of location—intensity of sensation evoked in the phantom hand using brush, for each RSA. For RSA1, 2, and 3 on a VASS (0 = no sensation, 10 = most intense non-painful sensation perceivable) and for RSA 4 on VASP (0 = no pain and 10 = worst imaginable pain), VAS score is presented for each RSA in Appendix A, Table A1. (b) Position of electrodes on and around RSAs, for each channel, and cumulative maps of location-intensity (VASS, colorbar), top panel, and location-rate of occurrence (normalized units, colorbar), bottom panel, of sensation in phantom hand evoked using electrical stimuli; (b1) single-channel stimulation for Ch1, 2, 3, and 4 (left to right); (b2) single-channel stimulation combined, randomized Ch1, 2, 3, and 4 (b3) multi-channel stimulation on two channels, combined; (b4) multi-channel stimulation on three channels, combined; (b5) multi-channel stimulation on four channels, combined. Multi-channel stimulation for a given channel configuration was performed on all possible combinations (e.g., two-channel configuration yielded six combinations).

Figure 3.
(a) Position of phantom hand (participant with left-side amputation) illustrated with participant P1 using the right hand as typically experienced, before the baseline phase. (b) Cumulative maps, throughout several sessions, of mean values for the last 24 h (evaluated before each session) for PLP intensity (VASP; 0 = no pain, 10 = worst pain imaginable, colorbar) and location (left panel), and PLP rate of occurrence (normalized units, colorbar) for given location (right panel), reported on the phantom hand for (b1) sessions S1 to S4, (b2) sessions S5 to S7, (b3) sessions S8 to S12, and (b4) sessions S13 to S18. (c) Position of phantom hand before and after (c1) session S5, (c2) session S7, (c3) session S12, and (c4) session S17. At the end of session S18, position of the phantom hand remained open as that reported at the end of session S17, illustrated in (c4). However, the participant reported that almost half of the phantom hand (starting from the ulnar side of the wrist and continuing with the little and ring fingers) could no longer be perceived.
Figure 3.
(a) Position of phantom hand (participant with left-side amputation) illustrated with participant P1 using the right hand as typically experienced, before the baseline phase. (b) Cumulative maps, throughout several sessions, of mean values for the last 24 h (evaluated before each session) for PLP intensity (VASP; 0 = no pain, 10 = worst pain imaginable, colorbar) and location (left panel), and PLP rate of occurrence (normalized units, colorbar) for given location (right panel), reported on the phantom hand for (b1) sessions S1 to S4, (b2) sessions S5 to S7, (b3) sessions S8 to S12, and (b4) sessions S13 to S18. (c) Position of phantom hand before and after (c1) session S5, (c2) session S7, (c3) session S12, and (c4) session S17. At the end of session S18, position of the phantom hand remained open as that reported at the end of session S17, illustrated in (c4). However, the participant reported that almost half of the phantom hand (starting from the ulnar side of the wrist and continuing with the little and ring fingers) could no longer be perceived.

Figure 4.
(a) Maps of RSAs for session S5 (a number of 15 RSAs where identified); (b) position of electrodes for six-channel configuration for session S5.
Figure 4.
(a) Maps of RSAs for session S5 (a number of 15 RSAs where identified); (b) position of electrodes for six-channel configuration for session S5.

Figure 5.
Position of phantom hand was experienced by participant P2 as a tight fist at all times before and during the experiment, with the exception of the temporary opening of the phantom hand reported at the end of the sessions S13, S14, S16, and S17. The temporary opening effect of the phantom hand lasted up to three hours. Position of phantom hand at the beginning, as tight fist, and at the end of session, as partially open hand, illustrated by participant P2 with the right hand (participant had amputation of left hand) for (a) session S13, (b) session S14, (c) session S16, and (d) session S17. The phantom hand returned to the usual tight-fist position after the temporary hand-opening effect (hand opening lasting from two to three hours).
Figure 5.
Position of phantom hand was experienced by participant P2 as a tight fist at all times before and during the experiment, with the exception of the temporary opening of the phantom hand reported at the end of the sessions S13, S14, S16, and S17. The temporary opening effect of the phantom hand lasted up to three hours. Position of phantom hand at the beginning, as tight fist, and at the end of session, as partially open hand, illustrated by participant P2 with the right hand (participant had amputation of left hand) for (a) session S13, (b) session S14, (c) session S16, and (d) session S17. The phantom hand returned to the usual tight-fist position after the temporary hand-opening effect (hand opening lasting from two to three hours).

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Lontis, E.R.; Yoshida, K.; Jensen, W. Non-Invasive Sensory Input Results in Changes in Non-Painful and Painful Sensations in Two Upper-Limb Amputees. Prosthesis 2024, 6, 1-23. https://0-doi-org.brum.beds.ac.uk/10.3390/prosthesis6010001
AMA Style
Lontis ER, Yoshida K, Jensen W. Non-Invasive Sensory Input Results in Changes in Non-Painful and Painful Sensations in Two Upper-Limb Amputees. Prosthesis. 2024; 6(1):1-23. https://0-doi-org.brum.beds.ac.uk/10.3390/prosthesis6010001
Chicago/Turabian StyleLontis, Eugen Romulus, Ken Yoshida, and Winnie Jensen. 2024. "Non-Invasive Sensory Input Results in Changes in Non-Painful and Painful Sensations in Two Upper-Limb Amputees" Prosthesis 6, no. 1: 1-23. https://0-doi-org.brum.beds.ac.uk/10.3390/prosthesis6010001