

Mid-Term Outcomes of a Modern Zweymüller Monolithic Femoral Stem in Primary Total Hip Arthroplasty


Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Cohort
2.2. Surgical Procedure
2.3. Clinical Evaluation
2.4. Statistical Analyses
3. Results
3.1. Clinical Outcomes
3.2. Complications
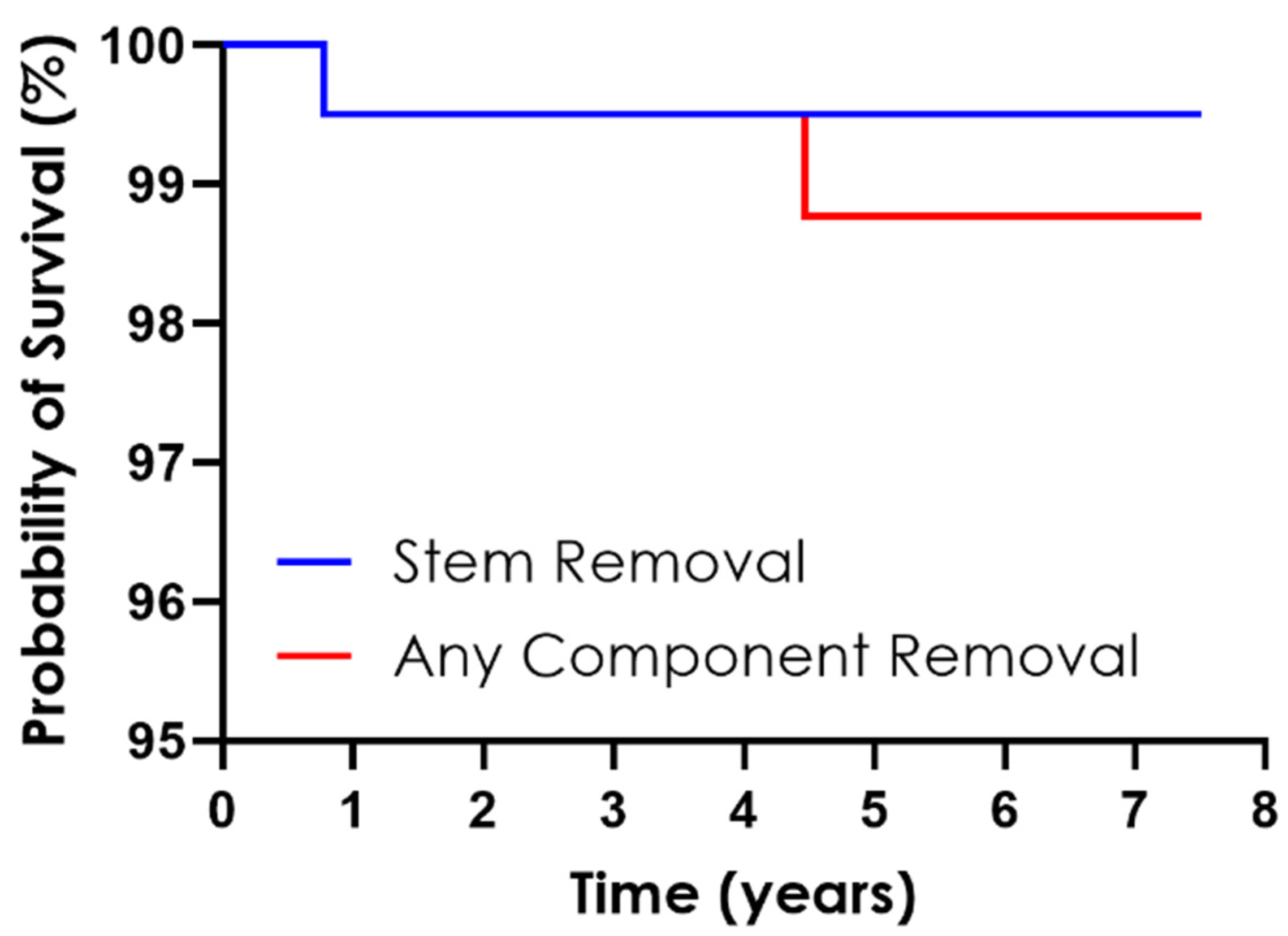
3.3. Stem Survivorship
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Siviero, P.; Veronese, N.; Smith, T.; Stubbs, B.; Limongi, F.; Zambon, S.; Dennison, E.M.; Edwards, M.; Cooper, C.; Timmermans, E.J.; et al. Association Between Osteoarthritis and Social Isolation: Data from the EPOSA Study. J. Am. Geriatr. Soc. 2020, 68, 87–95. [Google Scholar] [CrossRef]
- Rasmussen, M.B.; El-Galaly, A.; Daugberg, L.; Nielsen, P.T.; Jakobsen, T. Projection of Primary and Revision Hip Arthroplasty Surgery in Denmark from 2020 to 2050. Acta Orthop. 2022, 93, 849–853. [Google Scholar] [CrossRef]
- Wang, J.; Deng, Z.; Huang, B.; Zhao, Z.; Wan, H.; Ding, H. The Short-Term Outcomes of Cementless Stem for Hip Arthroplasty in the Elderly Patients: Comparison with Patients < 65 Years. BMC Musculoskelet Disord. 2022, 23, 1070. [Google Scholar] [CrossRef]
- Galante, J.; Rostoker, W.; Lueck, R.; Ray, R.D. Sintered Fiber Metal Composites as a Basis for Attachment of Implants to Bone. J. Bone Jt. Surg. Am. 1971, 53, 101–114. [Google Scholar] [CrossRef]
- Engh, C.A.; O’Connor, D.; Jasty, M.; McGovern, T.F.; Bobyn, J.D.; Harris, W.H. Quantification of Implant Micromotion, Strain Shielding, and Bone Resorption with Porous-Coated Anatomic Medullary Locking Femoral Prostheses. Clin. Orthop. Relat. Res. 1992, 285, 13–29. [Google Scholar] [CrossRef]
- Wang, D.; Li, H.; Zhang, W.; Li, H.; Xu, C.; Liu, W.; Li, J. Efficacy and Safety of Modular versus Monoblock Stems in Revision Total Hip Arthroplasty: A Systematic Review and Meta-Analysis. J. Orthop. Traumatol. 2023, 24, 50. [Google Scholar] [CrossRef]
- Huo, M.H.; Martin, R.P.; Zatorski, L.E.; Keggi, K.J. Total Hip Arthroplasty Using the Zweymuller Stem Implanted without Cement. J. Arthroplast. 1995, 10, 793–799. [Google Scholar] [CrossRef]
- Vervest, T.M.J.S.; Anderson, P.G.; Van Hout, F.; Wapstra, F.-H.; Louwerse, R.T.; Koetsier, J.W.A. Ten to Twelve-Year Results With the Zweymüller Cementless Total Hip Prosthesis. J. Arthroplast. 2005, 20, 362–368. [Google Scholar] [CrossRef] [PubMed]
- Zweymüller, K.A.; Lintner, F.K.; Semlitsch, M.F. Biologic Fixation of a Press-Fit Titanium Hip Joint Endoprosthesis. Clin. Orthop. Relat. Res. 1988, 235, 195–206. [Google Scholar] [CrossRef]
- Roškar, S.; Antolič, V.; Mavčič, B. Surgeon-Stratified Cohort Analysis of 1976 Cementless Zweymüller Total Hip Arthroplasties from a Single Hospital with 23,255 Component Years of Follow-Up. Arch. Orthop. Trauma Surg. 2020, 140, 1275–1283. [Google Scholar] [CrossRef] [PubMed]
- Goldstein, W.M.; Branson, J.J. Posterior-Lateral Approach to Minimal Incision Total Hip Arthroplasty. Orthop. Clin. N. Am. 2004, 35, 131–136. [Google Scholar] [CrossRef]
- Hage, A.; Hage, F. Kaplan-Meier Survival, Actuarial Survival, Censoring, and Competing Events—What Is What? Ann. Thorac. Surg. 2022, 114, 40–43. [Google Scholar] [CrossRef]
- Kunze, K.N.; Fontana, M.A.; MacLean, C.H.; Lyman, S.; McLawhorn, A.S. Defining the Patient Acceptable Symptom State for the HOOS JR and KOOS JR After Primary Total Joint Arthroplasty. J. Bone Jt. Surg. 2022, 104, 345–352. [Google Scholar] [CrossRef]
- Troelsen, A.; Malchau, E.; Sillesen, N.; Malchau, H. A Review of Current Fixation Use and Registry Outcomes in Total Hip Arthroplasty: The Uncemented Paradox. Clin. Orthop. Relat. Res. 2013, 471, 2052–2059. [Google Scholar] [CrossRef]
- Khanuja, H.S.; Vakil, J.J.; Goddard, M.S.; Mont, M.A. Cementless Femoral Fixation in Total Hip Arthroplasty. J. Bone Jt. Surg. 2011, 93, 500–509. [Google Scholar] [CrossRef]
- Inaba, Y.; Kobayashi, N.; Oba, M.; Ike, H.; Kubota, S.; Saito, T. Difference in Postoperative Periprosthetic Bone Mineral Density Changes Between 3 Major Designs of Uncemented Stems: A 3-Year Follow-Up Study. J. Arthroplast. 2016, 31, 1836–1841. [Google Scholar] [CrossRef]
- Liu, B.; Wang, H.; Zhang, N.; Zhang, M.; Cheng, C.-K. Femoral Stems With Porous Lattice Structures: A Review. Front. Bioeng. Biotechnol. 2021, 9, 772539. [Google Scholar] [CrossRef]
- Schmolders, J.; Amvrazis, G.; Pennekamp, P.H.; Strauss, A.C.; Friedrich, M.J.; Wimmer, M.D.; Rommelspacher, Y.; Wirtz, D.C.; Wallny, T. Thirteen Year Follow-up of a Cementless Femoral Stem and a Threaded Acetabular Cup in Patients Younger than Fifty Years of Age. Int. Orthop. (SICOT) 2017, 41, 39–45. [Google Scholar] [CrossRef]
- Delaunay, C.; Kapandji, A.I. Survival Analysis of Cementless Grit-Blasted Titanium Total Hip Arthroplasties. J. Bone Jt. Surg. Br. Vol. 2001, 83-B, 408–413. [Google Scholar] [CrossRef]
- Pisecky, L.; Hipmair, G.; Schauer, B.; Böhler, N. 30-Years of Experience with the Cementless Implanted Alloclassic Total Hip Arthroplasty System—An Ultra-Long-Term Follow-Up. J. Orthop. 2018, 15, 18–23. [Google Scholar] [CrossRef]
- Logroscino, G.; Donati, F.; Campana, V.; Saracco, M. Stemless Hip Arthroplasty versus Traditional Implants: A Comparative Observational Study at 30 Months Follow-Up. HIP Int. 2018, 28, 21–27. [Google Scholar] [CrossRef]
- Tottas, S.; Ververidis, A.; Kougioumtzis, I.; Tilkeridis, K.; Tsigalou, C.; Karaglani, M.; Drosos, G. MINIMA Short Stem Versus Standard Profemur (TL) Stem in Primary Total Hip Replacement: A Comparative Study. Cureus 2022, 14, 23771. [Google Scholar] [CrossRef]
- Calkins, T.E.; Goetz, D.D.; Zalewski, J.T.; Jones, C.A.; Gaumer, P.R.; Ford, M.C.; Toy, P.C.; Crockarell, J.R.; Harkess, J.W.; Mihalko, W.M.; et al. Hip Arthroplasty Femoral Stem Designs and Their Association With Early Postoperative Periprosthetic Femoral Fractures. J. Arthroplast. 2023, 38, 849–854. [Google Scholar] [CrossRef]
- Sershon, R.A.; McDonald, J.F.; Ho, H.; Hamilton, W.G. Periprosthetic Femur Fracture Risk: Influenced by Stem Choice, Not Surgical Approach. J. Arthroplast. 2021, 36, S363–S366. [Google Scholar] [CrossRef]
- Čengić, T. Impact of Cementless Zweymüller Stem Anteversion on Resistance to Periprosthetic Fracture in Total Hip Arthroplasty. Acta Clin. Croat. 2021, 60, 429–434. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Parameter | Total (n = 200) |
|---|---|
| Age at primary THA a (y) | 75 (49–92) |
| Gender Men Women | 86 (43%) 114 (57%) |
| Body mass index a (kg/m2) | 25.1 (16.2–36.3) |
| Indication for THA Osteoarthritis Congenital hip dysplasia Femoral head avascular necrosis Femoral neck fracture | 152 (76.0%) 2 (1.0%) 7 (3.5%) 39 (19.5%) |
| Parameter | Total (n = 200) |
|---|---|
| Surgical side Left Right | 90 (45%) 110 (65%) |
| Hip stem length 131 mm 136 mm 141 mm 146 mm 151 mm 156 mm 161 mm 166 mm | 1 (0.5%) 14 (7.0%) 31 (15.5%) 49 (24.5%) 63 (31.5%) 25 (12.5%) 12 (6.0%) 5 (2.5%) |
| Hip stem neck Short standard Long standard Short extended Long extended | 115 (57.5%) 20 (10.0%) 59 (29.5%) 6 (3.0%) |
| Bearing surface Ceramic on ceramic Metal on ceramic Ceramic on crosslinked polyethylene Metal on crosslinked polyethylene | 13 (6.5%) 1 (0.5%) 185 (92.5%) 1 (0.5%) |
| Accessories Acetabular screws | 2 (1.0%) |
| Parameter | Total |
|---|---|
| Mean follow-up a (y) | 5.4 (0.8–7.5) |
| Intraoperative complications | 0 (0%) |
| HOOS JR score at final follow-up b (n = 188) | 96.3 ± 8.4 (60.0–100.0) |
| HOOS JR score sub-group analysis b 2–5 years follow-up (n = 81) 5–7 years follow-up (n = 94) Greater than 7 years follow-up (n = 13) | 96.1 ± 9.8 (60.0–100.0) 96.1 ± 7.5 (67.5–100.0) 98.3 ± 4.4 (85.3–100.0) |
| Postoperative complications Dislocation Heterotopic ossification Hip pain Thigh pain Vancouver AG fracture Vancouver B2 fracture | 2 (1%) 6 (3%) 1 (0.5%) 1 (0.5%) 1 (0.5%) 1 (0.5%) |
| Revisions Femoral stem loosening Multiple hip dislocations | 1 (0.5%) 1 (0.5%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ciriello, V.; Saracco, M.; Leonardi, E.; Piovani, L.; Fetz-Palazola, A.; Mareno, C.; Logroscino, G. Mid-Term Outcomes of a Modern Zweymüller Monolithic Femoral Stem in Primary Total Hip Arthroplasty. Prosthesis 2024, 6, 53-62. https://0-doi-org.brum.beds.ac.uk/10.3390/prosthesis6010004
Ciriello V, Saracco M, Leonardi E, Piovani L, Fetz-Palazola A, Mareno C, Logroscino G. Mid-Term Outcomes of a Modern Zweymüller Monolithic Femoral Stem in Primary Total Hip Arthroplasty. Prosthesis. 2024; 6(1):53-62. https://0-doi-org.brum.beds.ac.uk/10.3390/prosthesis6010004
Chicago/Turabian StyleCiriello, Vincenzo, Michela Saracco, Enrico Leonardi, Lucio Piovani, Allison Fetz-Palazola, Chase Mareno, and Giandomenico Logroscino. 2024. "Mid-Term Outcomes of a Modern Zweymüller Monolithic Femoral Stem in Primary Total Hip Arthroplasty" Prosthesis 6, no. 1: 53-62. https://0-doi-org.brum.beds.ac.uk/10.3390/prosthesis6010004