
Decades of Progress in Allogeneic Stem Cell Transplantation for Multiple Myeloma


1
Division of Hematology and Medical Oncology, NYU Grossman School of Medicine, Perlmutter Cancer Center, NYU Langone Health, New York, NY 10012, USA
2
Department of Molecular Biotechnology and Health Sciences, University of Torino, 40138 Torino, Italy
3
IRCCS Azienda Ospedaliero Universitaria di Bologna, 40138 Bologna, Italy
4
Stem Cell Transplant Center, AOU Citta’ della Salute e della Scienza, 40138 Turin, Italy
*
Author to whom correspondence should be addressed.
Hemato 2021, 2(1), 89-102; https://0-doi-org.brum.beds.ac.uk/10.3390/hemato2010005
Submission received: 11 January 2021
/
Revised: 14 February 2021
/
Accepted: 15 February 2021
/
Published: 20 February 2021
(This article belongs to the Special Issue Immunotherapy in Myeloma: A Theme Issue in Honor of Prof. Dr. Gösta Gahrton)
Abstract
:Allogeneic hematopoietic cell transplantation in multiple myeloma has evolved over the decades. Myeloablative regimens have been replaced by the reduced intensity and non-myeloablative conditionings to reduce treatment-related toxicity and mortality while sparing graft-vs.-myeloma effects. Newer agents with potent anti-myeloma activity are not mutually exclusive and the combination with an allograft may improve long-term outcomes in this incurable disease especially in high-risk patients. Allografting may also be a platform for other promising new cell therapies such as CAR T-cells, NK-, and CAR NK-cells. These studies are warranted in the context of clinical trials. This review highlights the progress that has been made over the decades and possible future roles of allografting in the treatment landscape of multiple myeloma
1. Introduction
In 1955, Main and Prehn by giving mice lethal irradiation and marrow from an H2 incompatible strain were able to avoid the rejection of a subsequent skin graft from the same donor strain [1]. It would be later proved that the survival of the graft was due to the persistence of donor cells leading to “tolerance”. These experiments contributed to lay the foundation stone of the currently most established form of cell immunotherapy: allogeneic bone marrow transplantation. In the late 1950s, the first attempts to treat hematologic patients with irradiation and intravenous infusion of marrow from healthy donors were reported and, in 1970, approximately 200 patients had been treated. Unfortunately, all attempts had failed [2]. However, the perseverance of E.D. Thomas and his group led to the first successful reports in patients with leukemia and aplastic anemia in the mid-1970s [3,4]. Since then a history of tremendous breakthroughs unfolded in the field of allogeneic bone marrow transplantation and cell immunotherapy.
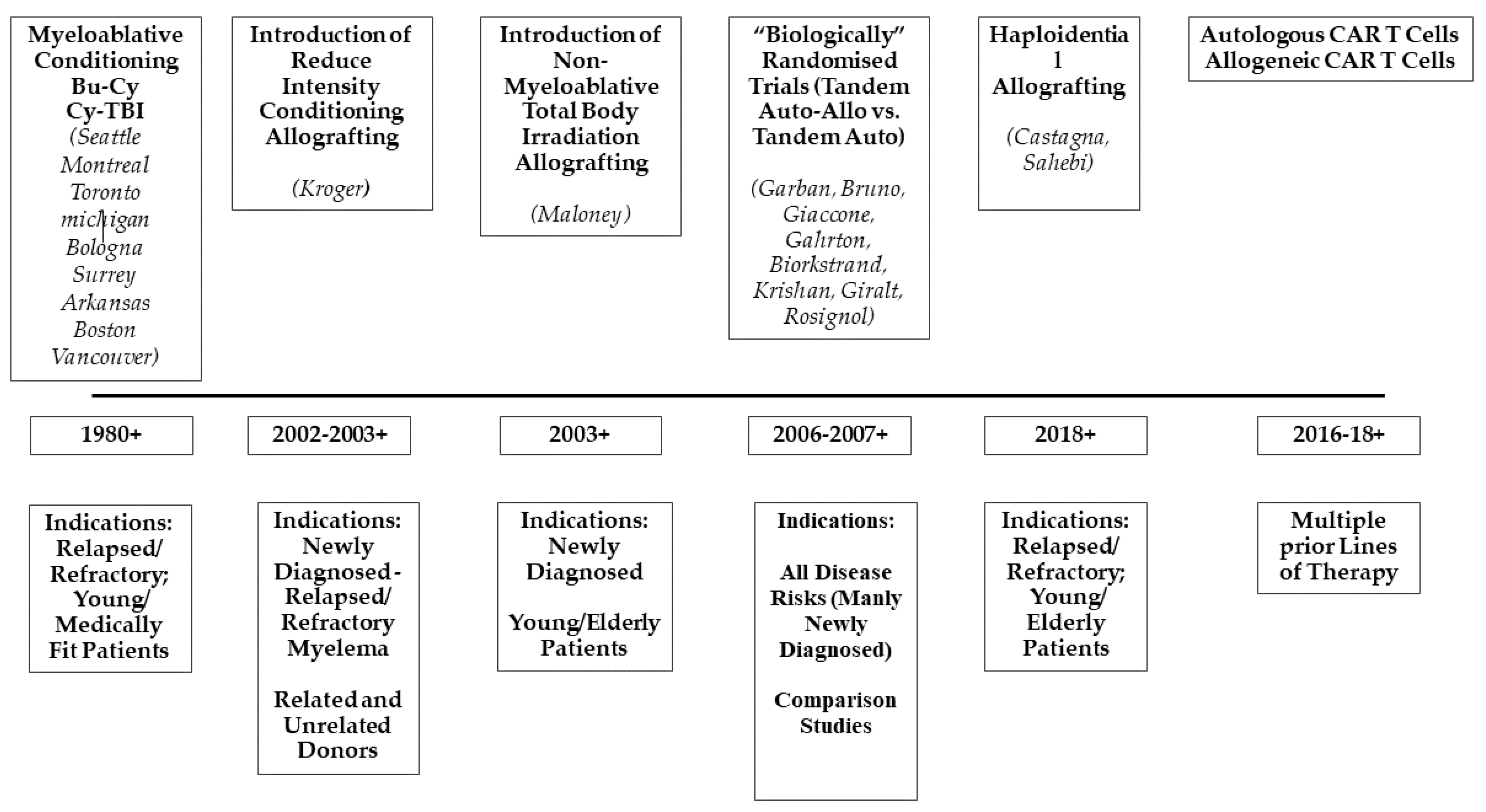
The role of allograting in multiple myeloma (MM) has always been hotly debated though it remains the only potentially curative treatment. Initially, high rates of transplant toxicity and long-term risk of relapse have prevented its widespread use. However, over time, many factors, such as greatly improved supportive care and reduced toxicity conditioning regimens, combined to significantly reduce the risk of lethal complications. So, nowadays, as for all other therapies for MM, disease recurrence is the major cause of treatment failure. In this review, we highlight the progress that has been made over the past decades, and the potential current role of allografting in combination with potent anti-MM agents and other cell therapies such as CAR T and CAR NK therapies (Figure 1).
2. The First Reports: Myeloablative Conditionings and Their Toxicity
The very first experiences were reported by D Thomas from Seattle in 1957, as part of a transplant series of six patients with hematologic malignancies [4]. All patients died, and only one showed signs of engraftment. In the mid-’80s a few other centers presented case reports with encouraging results. Impressive was the report by Garthon et al. from the Karolinska Institute, in 1983, where a woman with refractory MM was treated with an allograft [5]. The patient achieved complete remission (CR) that lasted for longer than 3 years. Though the patient was not cured, the interest in allografting for MM was growing. The reports from the late 1980s/early 1990s included only myeloablative conditioning regimens. Cyclophosphamide was used in association with total body irradiation (TBI) or busulfan, or melphalan with TBI [6,7,8,9,10,11,12,13,14,15,16,17]. At that time, these conditions were limited to young medically fit patients. However, in MM patients, transplant-related mortality (TRM) up to 60% was clearly higher if compared to other diseases. Reasons for these unacceptable toxicity rates were somehow difficult to find. The profound immunodeficiency typical of all plasma cell dyscrasias may have been responsible for the TRM observed in MM. Most representative reports are illustrated in Table 1. Among them, the US intergroup trial (S9321) was of particular interest given its prospective design comparing autografting with myeloablative allografting [10]. This study enrolled newly diagnosed MM patients and compared early vs. late autografting, but also included a third arm that allowed patients, under the age of 55, with HLA-identical siblings to undergo myeloablative allografts. This arm was prematurely closed given an excessively high early TRM of 53% in the first 36 patients enrolled. However, after a follow-up of 7 years, overall survival (OS) was overlapping in both autologous and allogeneic recipients with progression-free survival (PFS) of 15% and 22%, respectively. However, while the risk of relapse progressively continued in the autograft patients, OS for the allograft cohort reached a plateau with follow up extending to 10 years. Despite the higher risk of toxicity, the conclusion drawn by the Authors was that allografting was the only curative treatment for MM.
Over the years, toxicity appeared to be gradually reducing. A retrospective registry analysis from the European Bone Marrow Transplant (EBMT) group reported a significant improvement in OS in the late 1990s owing to a reduction in transplant-related mortality [18]. Six-hundred-ninety patients, median age 44 years, who underwent myeloablative allografts were divided into two groups depending on the year of transplant: 1983 through 1993 versus 1994 through 1998. TRM rates at 6 months and 2 years were lower in the period 1994–1998 than between 1983–1993, 21% versus 38% and 30% versus 46%, respectively. Reduced toxicity correlated with better OS and PFR at 3 years from 35% to 55% and from 7 to 19 months for the period 1994–1998. Undoubtedly, the reduction in TRM was at least partly due to improved supportive care and better patient and donor selections.
Overall, the retrospective nature of most of these studies prevented determining the real role of myeloablative allografting in MM. Of note, most patients were heavily pretreated, had the chemo-resistant disease at transplant, and received a variety of conditionings and GvHD prophylaxes. Despite selection bias, however, it was clear that better clinical outcomes were associated with patients with chemo-sensitive MM. In most studies, only 10–25% of patients eventually became long-term disease-free survivors, but those were potentially cured.
3. The Concept of Tandem Autologous-Allogeneic Transplantation and Reduced-Intensity Conditioning Regimens
The use of myeloablation prior to transplant was commonly limited to young medically fit patients. This prevented many elderly patients from receiving potentially curative treatment for their hematological malignancy. In the late 1990s, investigators were prompted to explore highly immunosuppressive, but less myelosuppressive, conditionings that could establish stable donor engraftment, reduce transplant-related organ toxicities, and spare graft-vs.-tumor effects (Table 2). A series of pioneering preclinical studies, soon translated into clinical practice, was carried out by the Seattle group where it was shown that stable donor engraftment could be obtained with a combination of low dose non- myeloablative TBI (200 cGy) and fludarabine, followed by unmanipulated G-CSF mobilized donor peripheral blood stem cells and potent immunosuppression with cyclosporine and mycophenolate mofetil [19]. However, the risk of engraftment failure and rejection was higher in those patients, including MM patients, who had not received prior intensive chemotherapy for the treatment of their underlying malignancies. The hypothesis that the risk of graft-failure and the TRM of myeloablative conditionings could be circumvented by introducing a tandem approach of an autologous transplant followed, 2–4 months later, by a non-myeloablative TBI based allograft was clinically investigated. The rationale for this tandem autologous-allogeneic approach was to separate in time the high-dose cytoreduction with melphalan (200 mg/m2) and the curative graft-vs.-myeloma with the potential of drastically reducing TRM and mortality. Of note, the burden of tumor eradication was almost totally shifted to donor-derived T cells. Initially, the Seattle group reported 52 newly diagnosed MM patients, treated with this tandem modality, with a complete remission rate of 48% while PFS and OS were 48% and 69% respectively [20]. The same tandem concept was also developed by Kroger et al. in Germany with the conditioning of melphalan, fludarabine, and anti-thymocyte globulin using both related and unrelated donors [21,22]. In the early 2000s, the tandem autologous-allogeneic approach was the only innovative procedure in the armamentarium of MM treatments that could be clinically investigated. Thus, before the era of so-called new drugs with potent anti-myeloma effects, prospective randomized clinical trials comparing allografting after non-myeloablative/reduced-intensity conditioning and double autologous transplantation were designed. The concept of Mendelian or genetic randomization was applied. This concept relies on the biological process through which offspring inherit genetic traits half from each parent. One in four siblings is then expected to have a potential HLA-identical sibling donor. Comparing by the intention-to-treat analysis patients with HLA-identical siblings, who could be assigned to allografting, and those without such siblings, who could only receive an autograft, was a surrogate for an unbiased randomization.
A first such study comparing two trials on high-risk MM, in the light of elevated serum β2-microglobulin and del(13), was initially reported by the French group [23,24]. All patients received an autograft (melphalan 220 mg/m2). Sixty-five with HLA-identical sibling donors were then treated with an allograft after a regimen combining busulfan, fludarabine, and high-dose anti-thymocyte globulin. Outcomes were compared with 219 high-risk patients who received a second autograft (melphalan 220 mg/m2). TRM and response rates did not significantly differ. After a median follow-up of 2 years, OS and event-free survival (EFS) were 35% and 25%, and 41% and 30% for the double autologous and the autologous-allogeneic groups, respectively. This study was criticized for the use of high dose anti-thymocyte globulin that, though probably reduced the incidence of chronic graft vs. host disease to 7%, prevented potentially curative GvM. The first study which showed superior results with the auto-allo tandem approach was reported by the Italian group [25,26]. Two-hundred-forty-five consecutive newly diagnosed myeloma patients, up to 65 years, diagnosed between 1998–2004 were included. Patients received VAD-based regimens followed by standard autograft (melphalan 200 mg/m2). Eighty patients with HLA-identical siblings were offered non-myeloablative TBI conditioning followed by an allograft. Eighty-two patients without HLA-identical siblings were assigned to receive a second autograft after high-dose or intermediate doses of melphalan (140–200 mg/m2, and 100 mg/m2, respectively). In the first report, at a median follow-up of 45 months, OS and EFS were significantly longer in patients with donors: 80 vs. 54 months and 35 vs. 29 months. Having an HLA-identical sibling was the only independent variable significantly associated with longer OS and EFS. Overall, in patients who completed the assigned treatments as per protocol arms, TRM was 10% and 2%, respectively. Median OS was not reached in the tandem auto-allo group and was 58 months in the tandem autologous group. EFS was 43 and 33 months, respectively. In the latest update, more than 7 years from diagnosis, the median OS was not reached in the auto/allo group vs. 4.2 years in the tandem auto group (p = 0.001) [26]. The long-term follow-up is a major strength of the study through the number of patients enrolled in the two cohorts is low. The Spanish study PETHEMA [27] enrolled only 25 patients in the auto-allo arm who were compared to 85 patients who received auto-auto. In this study design, only patients who did not reach CR or near CR after the autograft were eligible to either the allograft or a second autograft in the light of the availability of an HLA-identical sibling donor. Conditioning regimens used for the allograft were melphalan and fludarabine, while for the second autograft was cyclophosphamide, BCNU, etoposide (CBV), or high-dose melphalan. The difference was not statistically significant between the two arms, though the median time for PFS and OS were superior in the auto-allo cohort. The HOVON-50 study [28,29] enrolled 260 patients. One hundred-twenty-two had an HLA-identical sibling donor. Ninety-nine out of the 122 patients with a donor were treated with an auto/allo approach, whereas patients without a donor received a tandem auto/auto or maintenance with thalidomide after the first autograft. By intention to treat analysis, no significant differences in PFS or OS between the two groups at 8 or 10 years. However, when only the 99 patients who completed the protocol receiving the allograft (n = 99) were compared to the 122 who continued maintenance or received a second auto, there was a significant advantage in PFS for the allo patients at 8 years, this did not translate into a significantly better OS. The largest multicenter prospective study is the BMT-CTN 0102 trial [30]. It accrued 710 patients under the age of 70 years of age; 625 had the standard-risk disease. One hundred-fifty-six (83%) of 189 patients with the standard-risk disease were treated with the auto-allo (200 cGy TBI) in the light of absence/presence of an HLA-identical sibling donor; and 366 (84%) of 436 without donors tandem auto/auto (high-dose melphalan, 200 mg/m2). Primary endpoints in standard-risk myeloma (β2 microglobulin < 3.0 mg/L and absence of deletion 13 by classic karyotyping) were OS and PFS. In the initial report, there was no statistically significant difference in 3-year PFS or OS between the two cohorts. In a recent update [31], there was still no significant difference between PFS and OS at 6 and 10 years, respectively, in standard-risk patients whereas allo patients with high-risk disease had better long-term clinical outcomes. The second-largest multicenter study, the EBMT study [32,33], included 357 patients from 23 European centers. Patients younger than 70 years of age with an HLA-identical sibling were allocated to auto-allo (n = 108) and those without to tandem auto (n = 249). Trial results were first published in 2011 [32] and updated in 2013 [33] with a median follow-up of 96 months. PFS and OS were significantly superior in the auto-allo cohort as compared to the single auto or tandem auto at that time (22% vs. 12% (p = 0.027, and 49% vs. 36% (p = 0.030), at 96 months). The reason for the superior PFS and OS in the auto-allo cohort was a lower relapse rate despite higher TRM. Of note, at a follow-up of 36 months, there was no significant difference in PFS or OS indicating that long-term follow-up is necessary to see the benefits of the allograft. By protocol analysis, comparing the patients who had received the auto-allo transplant (n = 92) with those who received tandem auto (n = 104), the same differences were confirmed.
Importantly, two meta-analyses which included some of these studies were carried out [34,38]. In the first one, published in 2013, Armeson et al. used a comprehensive search strategy of published and unpublished reports including six clinical trials. Their findings showed that in the upfront management of MM, auto-allo was associated with higher TRM and CR rates without improvement in clinical outcomes (OS and PFS) [34,38]. However, the most recent meta-analysis employed an individual patient data analysis that included the Italian study, the Spanish PETHEMA, the EBMT—NMAM2000, and BMT-CTN studies for a total of 1338 patients, 439 in the auto-allo group and 899 in the auto-auto group respectively [38]. At a median follow-up of 118.5 months, 5-year OS, and 10-year OS were 62% vs. 59%, and 44% vs. 36% at 10 years (p = 0.01) for auto-allo and tandem auto respectively, whereas 5-year PFS and 10-year PFS were 30.1% vs. 23.4% (p = 0.01) and 18.7% vs. 14.4% (p = 0.06) for auto-allo and tandem auto. Overall, this individual patient data analysis showed a significantly longer PFS and OS with the auto-allo approach. However, the study also stresses the importance of a long follow-up to evaluate the difference between the two transplant modalities. Moreover, the advantage of the allo-auto approach may partly be due to a long-term effect of GvM, but, most likely, to the synergy of the residual donor T cells at relapse and the rescue with novel anti-myeloma agents with immune-modulatory activities.
4. Haplo-Identical Transplantation
The use of post-transplant cyclophosphamide (PT-Cy) to selectively deplete allo-reactive T cells has allowed to considerably increase the number of haploidentical-HCT. The encouraging clinical findings reported in other malignancies prompted investigators to evaluate the role of haploidentical-HCT also in relapsed/refractory myeloma [35,36,39]. Castagna et al. reported on a series of 30 heavily pretreated MM patients who received haplo-HCT with PT-Cy as GVHD pro-phylaxis. Cumulative incidences of relapse/progression and non-relapse mortality at 18 months were 42% and 10%, respectively. Cumulative incidences of grade II-IV acute GVHD and chronic GVHD were 29% and 7%. After a median follow-up of 25 months, 18-month progression-free survival (PFS) and overall survival (OS) were 33% and 63%, respectively [39]. A larger series was reported in a retrospective EBMT/CIBMTR study that included 96 patients, transplanted between 2008 and 2016, who had relapsed and all had received a prior autologous transplant. PT-Cy was administered to 73 patients and the remaining patients received non-PT-Cy-based GVHD prophylaxis regimens. After a median follow-up of 2 years, 2-year progression-free survival (PFS) was 17%, and overall survival (OS) was 48%. At 2 years, the cumulative risk of relapse/progression was 56%, and 1-year non-relapse mortality (NRM) was 21%. Incidence of grade II-IV acute GVHD and chronic GVHD were 39% and 46%, respectively [35]. Though patient series were rather heterogeneous, chemo-refractory disease at transplantation was invariably associated with lower clinical outcomes. However, both studies showed an association between the use of PT-Cy and substantially improved OS, encouraging further studies of haploidentical-HCT in patients with MM. These encouraging results also led to further investigation. In a recent study, the hypothesis that natural killer (NK) cell alloreactivity may reduce MM relapse in the setting of a haploidentical-HCT was evaluated. A prospective phase 2 study using a killer cell immunoglobulin-like receptor (KIR)-ligand mismatched haploidentical donor included 12 patients with poor-risk MM. The graft source was bone marrow. The primary endpoint was 1.5-year PFS. All patients relapsed within a median time of 90 days leading to a premature study termination in the light of predefined stopping rules. In this small patient series with chemo-refractory MM, NK cell KIR mismatch was not superior to conventional allo-SCT [36].
5. Allografting in Refractory/Relapsed Myeloma and High-Risk Disease
The emergence of new agents with potent anti-myeloma activity and the conflicting results of allografting in newly diagnosed myeloma patients with the tandem auto-allo approach did not allow to identify a definite role for allografting in the upfront setting, and an allograft became more commonly used in the setting of relapsed/refractory disease [37,40,41,42]. Moreover, in the early 2000s disease stratification by cytogenetics analysis was not routinely carried out, and, at that time, the only del13q- was thought to be primarily associated with poor prognosis. Among others [37,40,41,42], a significant study was reported by Patriarca et al. where the Authors compared 79 patients who received an allograft at first relapse with 90 patients, without an available HLA-identical donor, who were then treated with combinations of bortezomib and immunomodulatory drugs. Patients who received an allograft showed a significantly better 7-year OS and PFS of 31% and 9% compared to 18% and 0%, respectively [43,44]. Of note, this study was an updated analysis of a previous report where clinical outcomes were not different between the 2 cohorts of patients stressing once more that long-term follow-up is needed to evaluate the potential effects of an allograft [43,44]. Several other studies have been reported [37,40,41,42]. However, the often relatively small numbers of the patient series, the retrospective nature, and a not standardized maintenance approach make it difficult to define the real role of allografting in the setting of refractory/relapsed patients. However, in the attempt to reach a consensus on clinical recommendations, members from four scientific societies (including the International Myeloma Working Group, the American Society of Blood and Marrow Transplantation and Cell Therapies (ASBMT), the European Society of Blood and Marrow Transplantation (EBMT), and the Blood and Marrow Transplant Clinical Trials Network) agreed that allografting should be considered in patients with early relapse (less than 24 months from diagnosis) after first-line treatment with an autograft or in those patients with high-risk features such as poor cytogenetics and plasma cell leukemia [45]. Preferably, patients should be enrolled in well-designed prospective trials.
Currently, cytogenetic abnormalities are routinely evaluated to establish prognosis in MM patients at diagnosis and at different follow-up timepoints. Aberrations such as del17p, t (4; 14), t (14; 16), gain (1q), and del8p have clearly been associated with poor clinical outcomes. Unfortunately, these aberrations were not known when most biological randomized studies, before the era of new drugs, were designed in newly diagnosed patients. Del13q was initially the first chromosomal abnormality that was associated with poor outcome but is now primarily considered a surrogate marker of other aberrations. Whether GvM, especially if combined with anti-myeloma agents, may overcome the poor prognosis determined by certain cytogenetic aberrations remain a matter of debate. In an update of the EBMT–NMAM2000 study, del13q-pos patients in the autograft cohort did worse than del13q-neg patients. However, there was no difference in clinical outcomes between del13q-neg patients and del13q-pos patients in the auto-allo cohort shoeing that GvM might overcome the negative effects of this aberration [33]. More recently, a phase 3 trial by Knop et al. compared tandem auto-auto vs. auto-allo (with reduced-intensity conditioning) in patients with newly diagnosed MM and del13q. The availability or absence of an HLA-identical matched donor determined the nature of the second transplant. The primary endpoint was PFS by intention-to-treat analysis. At a median follow-up of 91 months, median PFS was 34 vs. 21 months in the auto-allo cohort vs. tandem auto (p = 0.003), whereas OS was 70.2 versus 71.8 months (p = 0.856), respectively. However, in patients carrying both del13q and del17p, median PFS and OS were 37.5 and 61.5 months in the auto-allo (n = 19) vs. 6.1 and 23.4 months in the tandem auto cohort (p = 0.0002 and 0.032). These findings suggest a survival benefit for the first-line allografting in high-risk MM [46]. In another interesting report by Kröger et al. [47], 16 out of 73 patients carrying del17p13 and/or t (4; 14) who had received tandem auto-allo (reduced-intensity conditioning) experienced similar 5-year PFS as those without such aberrations (24% vs. 30%, respectively, p = 0.70) suggesting that GvM might overcome the poor prognostic impact associated with chromosomal abnormalities.
6. Allogeneic Transplantation and Novel Agents: An Immunological Synergy
Most of the randomized trials comparing auto-allo vs. auto-auto in the upfront setting were designed before the era of new drugs. However, multiple treatment choices became available at the time of relapse as newer agents, over the years, were approved for MM patients. Giaccone et al. reported for the first time the observation that OS after relapse was significantly longer in the auto-allo cohorts as compared to tandem auto [26]. These preliminary findings were also confirmed by Gahrton et al. in an update of the EBMT- NMAM 2000 experience [33]. A larger retrospective analysis was carried out at the Center for International Blood and Marrow Transplant Research (CIBMTR) [48]. Htut et al. compared post-relapse OS after auto-allo vs. tandem auto in patients prospectively reported to the CIBMTR between 2000 and 2010. Overall, after a median follow-up of 8.5 years, 404 patients (72%) had relapsed in the auto-auto cohort and 178 (67%) in the auto-allo cohort group. Interestingly, at six months after the second transplant, in the auto-allo group, 46% of the total relapses had already occurred as compared to 26% in the auto-auto group. However, 6-year post-relapse OS was 44% in the auto-allo group and 35% in the auto-auto group (p = 0.05). Of note, by multivariate analysis, both groups had a similar risk of death during the first year after relapse, nonetheless, for time points beyond 1 year, the auto-allo group had significantly superior OS (p = 0.005). The recurrent observation that there appears to be a synergy between donor-derived T cells and the immunologic effects of several anti-myeloma agents may partly be explained by recent functional studies. Wolschke et al. showed that lenalidomide enhances both NK and T cell-mediated anti-myeloma activity after allografting; while Kneppers et al. showed that lenalidomide increases HLA-DR + T cell subsets indicating T cell activation [49,50].
7. Minimal Residual Disease (MRD) and Graft-vs.-Myeloma
GvM, potentially curative for MM, consists of an immunological response of donor T cells against myeloma cells through the recognition of possibly disease-specific antigens. This evidence was initially documented by the achievement of CR following discontinuation of immunosuppression or after the infusion of donor T cells in patients with post-transplant relapse [13,51,52]. Some Investigators, however, reported that the strongest predictors for response to donor lymphocyte infusions were acute and chronic GvHD [53,54,55,56] indicating that GvHD and GvM may share the same antigenic targets (Figure 2). Bruno et al., however, reported that the development of chronic GVHD was not correlated with CR rates and response duration [26] suggesting that subclinical long-term graft-vs.-host reactions may occur in the absence of GVHD. Flow cytometry and PCR methods are more sensitive than standard immunofixation to evaluate the death of response and may help to identify treatment algorithms capable of eradicating the disease [57,58]. Thus, the application of studies on MRD is currently expanding [58]. The possible achievement of molecular remission (MR) by PCR methods is further evidence for GvM. High rates of prolonged MR, a reliable indicator of maximal reduction and potential disease eradication, were initially reported after myeloablative conditioning [59,60]. The predictive value of molecular monitoring after a myeloablative allograft was assessed by a European Group for Blood and Marrow Transplantation (EBMT) longitudinal study on patients who reached clinical CR [60]. Of 48 evaluable patients, 16 (33%) attained durable post-transplant PCR-negativity after transplantation, whereas 13 (27%) remained persistently PCR-positive and 19 (40%) showed a mixed pattern. The cumulative risk of relapse at 5 years was 0% for PCR-negative patients, 33% for PCR-mixed patients, and 100% for PCR-positive patients [60]. More recently, durable MR has also been reported with non-myeloablative conditioning where the burden of tumor eradication is completely shifted toward donor T cells and their ability to generate graft-vs.-myeloma effects. After a remarkable median follow-up of 12 years in a cohort of 26 patients treated with the tandem auto-non myeloablative allo approach, Ladetto et al. reported that the achievement of MR by nested-PCR was significantly associated with better long-term OS and EFS [61]. Not only median durations of both OS and EFS had not been reached at follow-up, but some patients had been disease-free and off-therapy up to 20 years (Figure 3). It is interesting to notice that in the EBMT study the occurrence of MR was observed in the early post-transplant follow-up whereas after the non-myeloablative conditioning patients usually achieved MR later, up to one-year post-transplant. This phenomenon may be explained by the immediate cytoreductive effect of high dose conditionings, which mainly included 12 Gy TBI or high-dose busulphan, as compared with the low dose TBI (2 Gy) non-myeloablative conditioning. Overall, these studies report MR rates second to no other treatment approaches in MM.
8. Graft-vs.-Myeloma Effects: The New Frontiers
In recent years, chimeric antigen receptor (CAR) T-cell therapy has changed the immunotherapy paradigm of relapsed/refractory MM with unprecedented overall response rates [62,63,64]. However, patients appear to ultimately relapse despite obtaining initial high CR rates and none of these current autologous therapies have been approved. Importantly, main issues such as long-term clinical outcomes, toxicities, and management of complications limit their widespread use. Moreover, autologous CAR T therapies have major limitations such as lengthy vein-to-vein turnaround time and manufacturing constraints. Thus, allogeneic CAR T therapies may then offer an alternative to these limitations. Genetically engineered “off-the-shelf” allogeneic CAR T cells may dramatically change the current CAR T-cell scenario in the future. Allogeneic CAR T cell therapies use healthy donor T cells, may decrease cost, and enable broader availability [65]. Notwithstanding, allogeneic CAR-T bears the intrinsic risk for GVHD. Thus, sophisticated technology such as TALEN- and CRISPR-based gene editing has been introduced to manufacture allogeneic CAR-T with off-the-shelf availability [66,67]. Overall, the current role of CAR-T in the treatment paradigm of MM remains to be investigated. Simpler structures and multi-target approaches may dramatically improve efficacy and safety. Long-term outcome analyses and specific detection and evaluation of CAR-T dynamics in vivo are essential to allow deeper knowledge of their potentials. Cytogenetic high-risk features, patient selection, timing of infusion during the disease phase are other factors to be strictly considered to define their role. Currently, these strategies are being investigated in preclinical and early clinical trial settings and may reshape the indications of allografting, which so far remains the most established form of cell immunotherapy with well-documented graft-vs.-leukemia/tumor effects.
9. Conclusions
Over the last two decades, dramatic improvements have been made in the treatment of MM. It is widely assumed that recent results of large randomized trials undoubtedly affirm the role of ASCT with novel potent anti-myeloma agents combined both in the pre-transplant induction and in the post-transplant maintenance/consolidation phases. Nonetheless, the disease remains fatal and in ultra-high/high-risk patients clinical outcomes are very poor with survival rates of few years. Given the remarkable concomitant reduction in toxicity of allografting in recent years, there are still areas to thoroughly investigate where the potential GVM could be of benefit for MM patients. The inclusion in control trials would be recommended. Unfortunately, large prospective control studies evaluating the combination of new drugs with allo-HSCT have never been appropriately designed. The real effects of well-designed strategies combining allografting and newer agents will regretfully remain unknown. In patient subsets where long-term disease control cannot be expected even with the current wide armamentarium of treatment options, allografting may play an important role to increase the chance of better long-term survival. Clinical trials should be considered in young newly diagnosed ultra-high-risk/high-risk patients and in those who relapse early (18 months), regardless of baseline prognostic features, from first-line treatment. In the future, an “allo” platform may be exploited in the context of other cell therapies such as donor-derived CAR T-cells and NK cell infusions or immunotherapies such as bispecific T cell engagers and bispecific killer cell engagers to evoke stronger anti-tumor effects in appropriate high risk/relapsed patient populations.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Main, J.M.; Prehn, R.T. Success skin homografts after the administration of high dosage X radiation and homologous bone marrow. J. Natl. Cancer Inst. 1955, 15, 1023–1029. [Google Scholar]
- Buckner, C.D.; Clift, R.A.; Fefer, A.; Neiman, P.; Storb, R.; Thomas, E.D. Human marrow transplantation--current status. Prog. Hematol. 1973, 8, 299–324. [Google Scholar]
- Thomas, E.; Storb, R.; Clift, R.A.; Fefer, A.; Johnson, F.L.; Neiman, P.E.; Lerner, K.G.; Glucksberg, H.; Buckner, C.D. Bone-marrow transplantation (first of two parts). N. Engl. J. Med. 1975, 292, 832–843. [Google Scholar] [CrossRef]
- Thomas, E.D. The Nobel Prize in Physiology or Medicine 1990. In Les Prix Nobel, the Nobel Prizes 1990; Frängsmyr, T., Ed.; Nordstedts Tryckeri AB: Stockholm, Sweden, 1991; pp. 219–221. [Google Scholar]
- Gahrton, G.; Ringden, O.; Lönnqvist, B.; Lindquist, R.; Ljungman, P. Bone marrow transplantation in three patients with multiple myeloma. Acta Med. Scand. 1986, 219, 523–527. [Google Scholar] [CrossRef]
- Tura, S. Bone marrow transplantation in multiple myeloma: Current status and future perspectives. Bone Marrow Transpl. 1986, 1, 17–20. [Google Scholar]
- Gahrton, G.; Tura, S.; Ljungman, P.; Belanger, C.; Brandt, L.; Cavo, M.; Facon, T.; Granena, A.; Gore, M.; Gratwohl, A.; et al. Allogeneic bone marrow transplantation in multiple myeloma. N. Engl. J. Med. 1991, 325, 1267–1273. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bensinger, W.I.; Buckner, C.D.; Anasetti, C.; Clift, R.; Storb, R.; Barnett, T.; Chaunett, T.; Shulman, H.; Appelbaum, F.R. Allogeneic marrow transplantation for multiple myeloma: An analysis of risk factors on outcome. Blood 1996, 88, 2787–2793. [Google Scholar] [CrossRef] [Green Version]
- Gahrton, G.; Tura, S.; Ljungman, P.; Biadé, J.; Brandt, L.; Cavo, M.; Façon, T.; Gratwohl, A.; Hagenbeek, A.; Jacobs, P.; et al. Prognostic factors in allogeneic bone marrow transplantation for multiple myeloma. J. Clin. Oncol. 1995, 13, 1312–1322. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barlogie, B.; Kyle, R.A.; Anderson, K.C.; Greipp, P.R.; Lazarus, H.M.; Hurd, D.D.; McCoy, J.; Moore Jr, D.F.; Dakhil, S.R.; Lanier, K.S.; et al. Standard chemotherapy compared with high-dose chemoradiotherapy for multiple myeloma: Final results of phase III US Intergroup Trial S9321. J. Clin. Oncol. 2006, 24, 929–936. [Google Scholar] [CrossRef]
- Bensinger, W.I.; Maloney, D.; Storb, R. Allogeneic hematopoietic cell transplantation for multiple myeloma. Semin. Hemalol. 2001, 38, 243–249. [Google Scholar]
- Reece, D.E.; Shepherd, J.D.; Klingemann, H.G.; Sutherland, H.J.; Nantel, S.H.; Barnett, M.J.; Spinelli, J.J.; Phillips, G.L. Treatment of myeloma using intensive therapy and allogeneic bone marrow transplantation. Bone Marrow Transpl. 1995, 15, 117–123. [Google Scholar]
- Alyea, E.; Weller, E.; Schlossman, R.; Canning, C.; Webb, I.; Doss, D.; Mauch, P.; Marcus, K.; Fisher, D.; Freeman, A.; et al. T-cell-depleted allogeneic bone marrow transplantation followed by donor lymphocyte infusion in patients with multiple myeloma: Induction of graft-versus-myeloma effect. Blood 2001, 98, 934–939. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kulkarni, S.; Powles, R.L.; Treleaven, J.G.; Singhal, S.; Saso, R.; Horton, C.; Killick, S.; Tait, D.; Ramiah, V.; Mehta, J. Impact of previous high-dose therapy on outcome after allografting for multiple myeloma. Bone Marrow Transpl. 1999, 23, 675–680. [Google Scholar] [CrossRef]
- Le Blanc, R.; Montminy-Métivier, S.; Bélanger, R.; Busque, L.; Fish, D.; Roy, D.-C.; Kassis, J.; Boileau, J.; Lavallée, R.; Bélanfer, F.; et al. Allogeneic transplantation for multiple myeloma: Further evidence for a GVHD-associated graft-versus-myeloma effect. Bone Marrow Transpl. 2001, 28, 841–848. [Google Scholar] [CrossRef] [Green Version]
- Couban, S.; Stewart, A.K.; Loach, D.; Panzarella, T.; Meharchand, J. Autologous and allogeneic transplantation for multiple myeloma at a single centre. Bone Marrow Transpl. 1997, 19, 783–789. [Google Scholar] [CrossRef] [Green Version]
- Varterasian, M.; Janakiraman, N.; Karanes, C.; Aberlla, E.; Uberti, J.; Dragovic, J.; Raman, S.B.K.; Al-Katib, A.; Du, W.; Silver, S.M.; et al. Transplantation in patients with multiple myeloma: A multicenter comparative analysis of peripheral blood stem cell and allogeneic transplant. Am. J. Clin. Oncol. 1997, 20, 462–466. [Google Scholar] [CrossRef]
- Gahrton, G.; Svensson, H.; Cavo, M.; Apperley, J.; Bacigalupo, A.; Björkstrand, B.; Blade, J.; Cornelissen, J.; De Laurenzi, A.; Façon, T.; et al. Progress in allogeneic bone marrow and peripheral blood stem cell transplantation for multiple myeloma: A comparison between transplants performed 1983–93 and 1994–98 at European Group for Blood and Marrow Transplantation centres. Br. J. Haematol. 2001, 113, 209–216. [Google Scholar] [CrossRef] [PubMed]
- McSweeney, P.A.; Niederwieser, D.; Shizuru, J.A.; Sandmaier, B.M.; Molina, A.J.; Maloney, D.G.; Chauncey, T.R.; Gooley, T.A.; Hegenbart, U.; Nash, R.A.; et al. Hematopoietic cell transplantation in older patients with hematologic malignancies: Replacing high-dose cytotoxic therapy with graft-versus-tumor effects. Blood 2001, 97, 3390–3400. [Google Scholar] [CrossRef] [Green Version]
- Maloney, D.G.; Molina, A.J.; Sahebi, F.; Stockerl-Goldstein, K.E.; Sandmaier, B.M.; Bensinger, W.; Storer, B.; Hegenbart, U.; Somlo, G.; Chauncey, T.; et al. Allografting with nonmyeloablative conditioning following cytoreductive autografts for the treatment of patients with multiple myeloma. Blood 2003, 102, 3447–3454. [Google Scholar] [CrossRef] [Green Version]
- Kröger, N.; Schwerdtfeger, R.; Kiehl, M.; Sayer, H.G.; Renges, H.; Zabelina, T.; Fehse, B.; Tögel, F.; Wittkowsky, G.; Kuse, R.; et al. Autologous stem cell transplantation followed by a dose-reduced allograft induces high complete remission rate in multiple myeloma. Blood 2002, 100, 755–760. [Google Scholar] [CrossRef]
- Kröger, N.; Sayer, H.G.; Schwerdtfeger, R.; Kiehl, M.; Nagler, A.; Renges, H.; Zabelina, T.; Fehse, B.; Ayuk, F.; Wittkowsky, G.; et al. Unrelated stem cell transplantation in multiple myeloma after a reduced- intensity conditioning with pretransplantation antithymocyte globulin is highly effective with low transplantation-related mortality. Blood 2002, 100, 3919–3924. [Google Scholar] [CrossRef] [Green Version]
- Garban, F.; Attal, M.; Michallet, M.; Hulin, C.; Bourhis, J.H.; Yakoub-Agha, I.; Lamy, T.; Marit, G.; Maloisel, F.; Berthou, C.; et al. Prospective comparison of autologous stem cell transplantation followed by dose-reduced allograft (IFM99-03 trial) with tandem autologous stem cell transplantation (IFM99-04 trial) in high-risk de novo multiple myeloma. Blood 2006, 107, 3474–3480. [Google Scholar] [CrossRef] [Green Version]
- Moreau, P.; Garban, F.; Attal, M.; Michallet, M.; Marit, G.; Hulin, C.; Benboubker, L.; Doyen, C.; Mohty, M.; Yakoub-Agha, I.; et al. Long-term follow-up results of IFM99-03 and IFM99-04 trials comparing nonmyeloablative allotransplantation with autologous transplantation in high-risk de novo multiple myeloma. Blood 2008, 112, 3914–3915. [Google Scholar] [CrossRef]
- Bruno, B.; Rotta, M.; Patriarca, F.; Mordini, N.; Allione, B.; Carnevale-Schianca, F.; Giaccone, L.; Sorasio, R.; Omedé, P.; Baldi, I.; et al. A Comparison of allografting with autografting for newly diagnosed myeloma. N. Engl. J. Med. 2007, 356, 1110–1120. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giaccone, L.; Storer, B.; Patriarca, F.; Rotta, M.; Sorasio, R.; Allione, B.; Carnevale-Schianca, F.; Festuccia, M.; Brunello, L.; Omedè, P.; et al. Long-term follow-up of a comparison of nonmyeloablative allografting with autografting for newly diagnosed myeloma. Blood 2011, 117, 6721–6727. [Google Scholar] [CrossRef] [Green Version]
- Rosiñol, L.; Perez-Simón, J.A.; Sureda, A.; Rubia, J.D.L.; De Arriba, F.; Lahuerta, J.J.; González, J.D.; Diaz-Mediavilla, J.; Hernández, B.; García-Frade, J.; et al. A prospective PETHEMA study of tandem autologous transplantation versus autograft followed by reduced-intensity conditioning allogeneic transplantation in newly diagnosed multiple myeloma. Blood 2008, 112, 3591–3593. [Google Scholar] [CrossRef] [Green Version]
- Lokhorst, H.M.; Van Der Holt, B.; Cornelissen, J.J.; Kersten, M.J.; Van Oers, M.; Raymakers, R.; Minnema, M.C.; Zweegman, S.; Janssen, J.J.; Zijlmans, M.; et al. Donor versus no-donor comparison of newly diagnosed myeloma patients included in the HOVON-50 multiple myeloma study. Blood 2012, 119, 6219–6225. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lokhorst, H.M.; Van Der Holt, B.; Cornelissen, J.J.; Kersten, M.J.; Van Oers, M.; Raymakers, R.; Minnema, M.C.; Zweegman, S.; Bos, G.; Schaap, N.; et al. Reduced relapse rate in upfront tandem autologous/reduced-intensity allogeneic transplantation in multiple myeloma only results in borderline non-significant prolongation of progression-free but not overall survival. Haematologica 2015, 100, e508–e510. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krishnan, A.; Pasquini, M.C.; Logan, B.; Stadtmauer, E.A.; Vesole, D.H.; Alyea, E.; Antin, J.H.; Comenzo, R.; Goodman, S.; Hari, P.; et al. Autologous haemopoietic stem-cell transplantation followed by allogeneic or autologous haemopoietic stem-cell transplantation in patients with multiple myeloma (BMT CTN 0102): A phase 3 biological assignment trial. Lancet Oncol. 2011, 12, 1195–1203. [Google Scholar] [CrossRef] [Green Version]
- Giralt, S.A.; Costa, L.J.; Maloney, D.; Krishnan, A.; Fei, M.; Antin, J.H.; Brunstein, C.; Geller, N.; Goodman, S.; Hari, P.; et al. Tandem autologous-autologous versus autologous-allogeneic hematopoietic stem cell transplant for patients with multiple myeloma: Long-term follow-up results from the Blood and Marrow Transplant Clinical Trials Network 0102 Trial. Biol. Blood Marrow Transpl. 2020, 26, 798–804. [Google Scholar] [CrossRef]
- Björkstrand, B.; Iacobelli, S.; Hegenbart, U.; Gruber, A.; Greinix, H.; Volin, L.; Narni, F.; Musto, P.; Beksac, M.; Bosi, A.; et al. Tandem autologous/reduced-intensity conditioning allogeneic stem-cell transplantation versus autologous transplantation in myeloma: Long-term follow-up. J. Clin. Oncol. 2011, 29, 3016–3022. [Google Scholar] [CrossRef]
- Gahrton, G.; Iacobelli, S.; Björkstrand, B.; Hegenbart, U.; Gruber, A.; Greinix, H.; Volin, L.; Narni, F.; Carella, A.M.; Beksac, M.; et al. Autologous/reduced-intensity allogeneic stem cell transplantation vs autologous transplantation in multiple myeloma: Long-term results of the EBMT-NMAM2000 study. Blood 2013, 121, 5055–5063. [Google Scholar] [CrossRef] [Green Version]
- Armenson, K.E.; Hill, E.G.; Costa, L.J. Tandem autologous vs autologous plus reduced intensity allogeneic transplantation in the upfront management of multiple myeloma: Meta-analysis of trials with biological assignment. Bone Marrow Transpl. 2013, 48, 562–567. [Google Scholar] [CrossRef]
- Sahebi, F.; Garderet, L.; Kanate, A.S.; Eikema, D.J.; Knelange, N.S.; Alvelo, O.F.D.; Koc, Y.; Blaise, D.; Bashir, Q.; Moraleda, J.M.; et al. Outcomes of Haploidentical Transplantation in Patients with elapsed Multiple Myeloma: An EBMT/CIBMTR Report. Biol. Blood Marrow Transpl. 2019, 25, 335–342. [Google Scholar] [CrossRef] [Green Version]
- Jaiswal, S.R.; Chakrabarti, S. Natural killer cell-based immunotherapy with CTLA4Ig-primed donor lymphocytes following haploidentical transplantation. Immunotherapy 2019, 11, 1221–1230. [Google Scholar] [CrossRef] [PubMed]
- Sobh, M.; Michallet, M.; Gahrton, G.; Iacobelli, S.; Van Biezen, A.; Schönland, S.O.; Petersen, E.; Schaap, N.; Bonifazi, F.; Volin, L.; et al. Allogeneic hematopoietic cell transplantation for multiple myeloma in Europe: Trends and outcomes over 25 years. A study by the EBMT Chronic Malignancies Working Party. Leukemia 2016, 30, 2047–2054. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Costa, L.J.M.; Iacobelli, S.; Pasquini, M.C.; Modi, R.; Giaccone, L.; Blade, J.; Schonland, S.; Evangelista, A.; Perez-Simon, J.A.; Hari, P.; et al. Long-term survival of 1338 MM patients treated with tandem autologous vs. autologous-allogeneic transplantation. Bone Marrow Transpl. 2020, 55, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Castagna, L.; Mussetti, A.; DeVillier, R.; Dominietto, A.; Marcatti, M.; Milone, G.; Maura, F.; De Philippis, C.; Bruno, B.; Furst, S.; et al. Haploidentical allogeneic hematopoietic cell transplantation for multiple myeloma using post-transplantation cyclophosphamide graft-versus-host disease prophylaxis. Biol. Blood Marrow Transpl. 2017, 23, 1549–1554. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Efebera, Y.A.; Qureshi, S.R.; Cole, S.M.; Saliba, R.; Pelosini, M.; Patel, R.M.; Koca, E.; Mendoza, F.L.; Wang, M.; Shah, J.; et al. Reduced-intensity allogeneic hematopoietic stem cell transplantation for relapsed multiple myeloma. Biol. Blood Marrow Transpl. 2010, 16, 1122–1129. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karlin, L.; Arnulf, B.; Chevret, S.; Ades, L.; Robin, M.; De Latour, R.P.; Malphettes, M.; Kabbara, N.; Asli, B.; Rocha, V.; et al. Tandem autologous non-myeloablative allogeneic transplantation in patients with multiple myeloma relapsing after a first high dose therapy. Bone Marrow Transpl. 2010, 46, 250–256. [Google Scholar] [CrossRef] [Green Version]
- Shimoni, A.; Hardan, I.; Ayuk, F.; Schilling, G.; Atanackovic, D.; Zeller, W.; Yerushalmi, R.; Zander, A.R.; Kröger, N.; Nagler, A. Allogenic hematopoietic stem-cell transplantation with reduced-intensity conditioning in patients with refractory and recurrent multiple myeloma. Cancer 2010, 116, 3621–3630. [Google Scholar] [CrossRef]
- Patriarca, F.; Einsele, H.; Spina, F.; Bruno, B.; Isola, M.; Nozzoli, C.; Nozza, A.; Sperotto, A.; Morabito, F.; Stuhler, G.; et al. Allogeneic stem cell transplantation in multiple myeloma relapsed after autograft: A multicenter retrospective study based on donor availability. Biol Blood Marrow Transpl. 2012, 18, 617–626. [Google Scholar] [CrossRef] [Green Version]
- Patriarca, F.; Bruno, B.; Einsele, H.; Spina, F.; Giaccone, L.; Montefusco, V.; Isola, M.; Nozzoli, C.; Nozza, A.; Morabito, F.; et al. Long-term follow-up of a Donor versus No-Donor Comparison in patients with multiple myeloma in first relapse after failing autologous transplantation. Biol. Blood Marrow Transpl. 2018, 24, 406–409. [Google Scholar] [CrossRef] [Green Version]
- Giralt, S.A.; Garderet, L.; Durie, B.; Cook, G.; Gahrton, G.; Bruno, B.; Hari, P.; Lokhorst, H.; McCarthy, P.; Krishnan, A.; et al. American Society of Blood and Marrow Transplantation, European Society of Blood and Marrow Transplantation, Blood and Marrow Transplant Clinical Trials Network, and International Myeloma Working Group Consensus Conference on salvage hematopoietic cell transplantation in patients with relapsed multiple myeloma. Biol. Blood Marrow Transpl. 2015, 21, 2039–2051. [Google Scholar]
- Knop, S.; Engelhardt, M.; Liebisch, P.; Meisner, C.; Holler, E.; Metzner, B.; Peest, D.; Kaufmann, M.; Bunjes, D.; Straka, C.; et al. Allogeneic transplantation in multiple myeloma: Long-term follow-up and cytogenetic subgroup analysis. SSRN Electron. J. 2019, 33, 2710–2719. [Google Scholar]
- Kröger, N.; Badbaran, A.; Zabelina, T.; Ayuk, F.; Wolschke, C.; Alchalby, H.; Klyuchnikov, E.; Atanackovic, D.; Schilling, G.; Hansen, T.; et al. Impact of high-risk cytogenetics and achievement of molecular remission on long-term freedom from disease after autologous-allogeneic tandem transplantation in patients with multiple myeloma. Biol. Blood Marrow Transpl. 2013, 19, 398–404. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Htut, M.; D’Souza, A.; Krishnan, A.; Bruno, B.; Zhang, M.-J.; Fei, M.; González-Díaz, M.; Copelan, E.; Ganguly, S.; Hamadani, M.; et al. Autologous/Allogeneic hematopoietic cell transplantation versus tandem autologous transplantation for multiple myeloma: Comparison of long-term postrelapse survival. Biol. Blood Marrow Transpl. 2018, 24, 478–485. [Google Scholar] [CrossRef] [Green Version]
- Kneppers, E.; Van Der Holt, B.; Kersten, M.J.; Zweegman, S.; Meijer, E.; Huls, G.; Cornelissen, J.J.; Janssen, J.J.; Huisman, C.; Cornelisse, P.B.; et al. Lenalidomide maintenance after nonmyeloablative allogeneic stem cell transplantation in multiple myeloma is not feasible: Results of the HOVON 76 Trial. Blood 2011, 118, 2413–2419. [Google Scholar] [CrossRef] [PubMed]
- Wolschke, C.; Stübig, T.; Hegenbart, U.; Schönland, S.O.; Heinzelmann, M.; Hildebrandt, Y.; Ayuk, F.; Atanackovic, D.; Dreger, P.; Zander, A.; et al. Postallograft lenalidomide induces strong NK cell–mediated antimyeloma activity and risk for T cell-mediated GvHD: Results from a phase I/II dose-finding study. Exp. Hematol. 2013, 41, 134–142.e3. [Google Scholar] [CrossRef]
- Libura, J.; Hoffmann, T.; Passweg, J.R.; Gregor, M.; Favre, G.; Tichelli, A.; Gratwohl, A. Graft-versusmyeloma after withdrawal of immunosuppression following allogeneic peripheral stem cell transplantation. Bone Marrow Transpl. 1999, 24, 925–927. [Google Scholar] [CrossRef] [Green Version]
- Verdonck, L.F.; Lokhorst, H.M.; Dekker, A.W.; Nieuwenhuis, H.K.; Petersen, E.J. Graft-versus-myeloma effect in two cases. Lancet 1996, 347, 800–801. [Google Scholar] [CrossRef]
- Lokhorst, H.M.; Schattenberg, A.; Cornelissen, J.J.; Thomas, L.L.M.; Verdonck, L.F. Donor leukocyte infusions are effective in relapsed multiple myeloma after allogeneic bone marrow transplantation. Blood 1997, 90, 4206–4211. [Google Scholar] [CrossRef]
- Lokhorst, H.M.; Schattenberg, A.; Cornelissen, J.J.; van Oers, M.H.J.; Fibbe, W.; Van De Donk, N.W.C.J.; Verdonck, L.F. Donor lymphocyte infusions for relapsed multiple myeloma after allogeneic stem-cell transplantation: Predictive factors for response and long-term outcome. J. Clin. Oncol. 2000, 18, 3031–3037. [Google Scholar] [CrossRef]
- Lokhorst, H.; Wu, K.; Verdonck, L.F.; Laterveer, L.L.; Van De Donk, N.W.C.J.; Van Oers, M.H.J.; Cornelissen, J.J.; Schattenberg, A.V. The occurrence of graft-versus-host disease is the major predictive factor for response to donor lymphocyte infusions in multiple myeloma. Blood 2004, 103, 4362–4364. [Google Scholar] [CrossRef] [Green Version]
- Van de Donk, N.W.; Kröger, N.; Hegenbart, U.; Corradini, P.; Miguel, J.F.S.; Goldschmidt, H.; Perez-Simon, J.A.; Zijlmans, M.; Raymakers, R.A.; Montefusco, V.; et al. Prognostic factors for donor lymphocyte infusions following nonmyeloablative allogeneic stem cell transplantation in multiple myeloma. Bone Marrow Transpl. 2006, 37, 1135–1141. [Google Scholar] [CrossRef] [Green Version]
- Rawstron, A.C.; Davies, F.E.; DasGupta, R.; Ashcroft, A.J.; Patmore, R.; Drayson, M.T.; Owen, R.G.; Jack, A.S.; Child, J.A.; Morgan, G.J. Flow cytometric disease monitoring in multiple myeloma: The elationship between normal and neoplastic plasma cells predicts outcome after transplantation. Blood 2002, 100, 3095–3100. [Google Scholar] [CrossRef] [Green Version]
- Costa, L.J.; Derman, B.A.; Bal, S.; Sidana, S.; Chhabra, S.; Silbermann, R.; Ye, J.C.; Cook, G.; Cornell, R.F.; Holstein, S.A.; et al. International harmonization in performing and reporting minimal residual disease assessment in multiple myeloma trials. Leukemia 2021, 35, 18–30. [Google Scholar] [CrossRef]
- Corradini, P.; Voena, C.; Tarella, C.; Astolfi, M.; Ladetto, M.; Palumbo, A.; Van Lint, M.T.; Bacigalupo, A.; Santoro, A.; Musso, M.; et al. Molecular and clinical remissions in multiple myeloma: Role of autologous and allogeneic transplantation of hematopoietic cells. J. Clin. Oncol. 1999, 17, 208–215. [Google Scholar] [CrossRef]
- Corradini, P.; Cavo, M.; Lokhorst, H.; Martinelli, G.; Terragna, C.; Majolino, I.; Valagussa, P.; Boccadoro, M.; Samson, D.; Bacigalupo, A.; et al. Molecular remission after myeloablative allogeneic stem cell transplantation predicts a better relapse-free survival in patients with multiple myeloma. Blood 2003, 102, 1927–1929. [Google Scholar] [CrossRef] [Green Version]
- Ladetto, M.; Ferrero, S.; Drandi, D.; Festuccia, M.; Patriarca, F.; Mordini, N.; Cena, S.; Benedetto, R.; Guarona, G.; Ferrando, F.; et al. Prospective molecular monitoring of minimal residual disease after non-myeloablative allografting in newly diagnosed multiple myeloma. Leukemia 2016, 30, 1211–1214. [Google Scholar] [CrossRef] [Green Version]
- Garfall, A.L.; Maus, M.V.; Hwang, W.T.; Lacey, S.F.; Mahnke, Y.D.; Melenhorst, J.J.; Zheng, Z.; Vogl, D.T.; Cohen, A.D.; Weiss, B.M.; et al. Chimeric Antigen Receptor T Cells against CD19 for Multiple Myeloma. N. Engl. J. Med. 2015, 373, 1040–1047. [Google Scholar] [CrossRef]
- Cohen, A.D.; Garfall, A.L.; Stadtmauer, E.A.; Melenhorst, J.J.; Lacey, S.F.; Lancaster, E.; Vogl, D.T.; Weiss, B.M.; Dengel, K.; Nelson, A.; et al. B cell maturation antigen-specific CAR T cells are clinically active in multiple myeloma. J. Clin. Investig. 2019, 129, 2210–2221. [Google Scholar] [CrossRef] [Green Version]
- Raje, N.; Berdeja, J.; Lin, Y.; Chhabra, S.; Silbermann, R.; Ye, J.C.; Cook, G.; Cornell, R.F.; Holstein, S.A.; Shi, Q.; et al. Anti-BCMA CAR T-Cell Therapy bb2121 in Relapsed or Refractory Multiple Myeloma. N. Engl. J. Med. 2019, 380, 1726–1737. [Google Scholar] [CrossRef]
- Depil, S.; Duchateau, P.; Grupp, S.A.; Mufti, G.; Poirot, L. “Off-the-shelf” allogeneic CAR T cells: Development and challenges. Nat. Rev. Drug Discov. 2020, 19, 185–199. [Google Scholar] [CrossRef]
- Gagelmann, N.; Riecken, K.; Wolschke, C.; Berger, C.; Ayuk, F.A.; Fehse, B.; Kröger, N. Development of CAR-T cell therapies for multiple myeloma. Leukemia 2020, 34, 2317–2332. [Google Scholar] [CrossRef]
- Wagner, V.; Gil, J. T cells engineered to target senescence. Nature 2020, 583, 37–38. [Google Scholar] [CrossRef]
Figure 1.
Timeline of allografting and cell therapies over the decades in multiple myeloma.
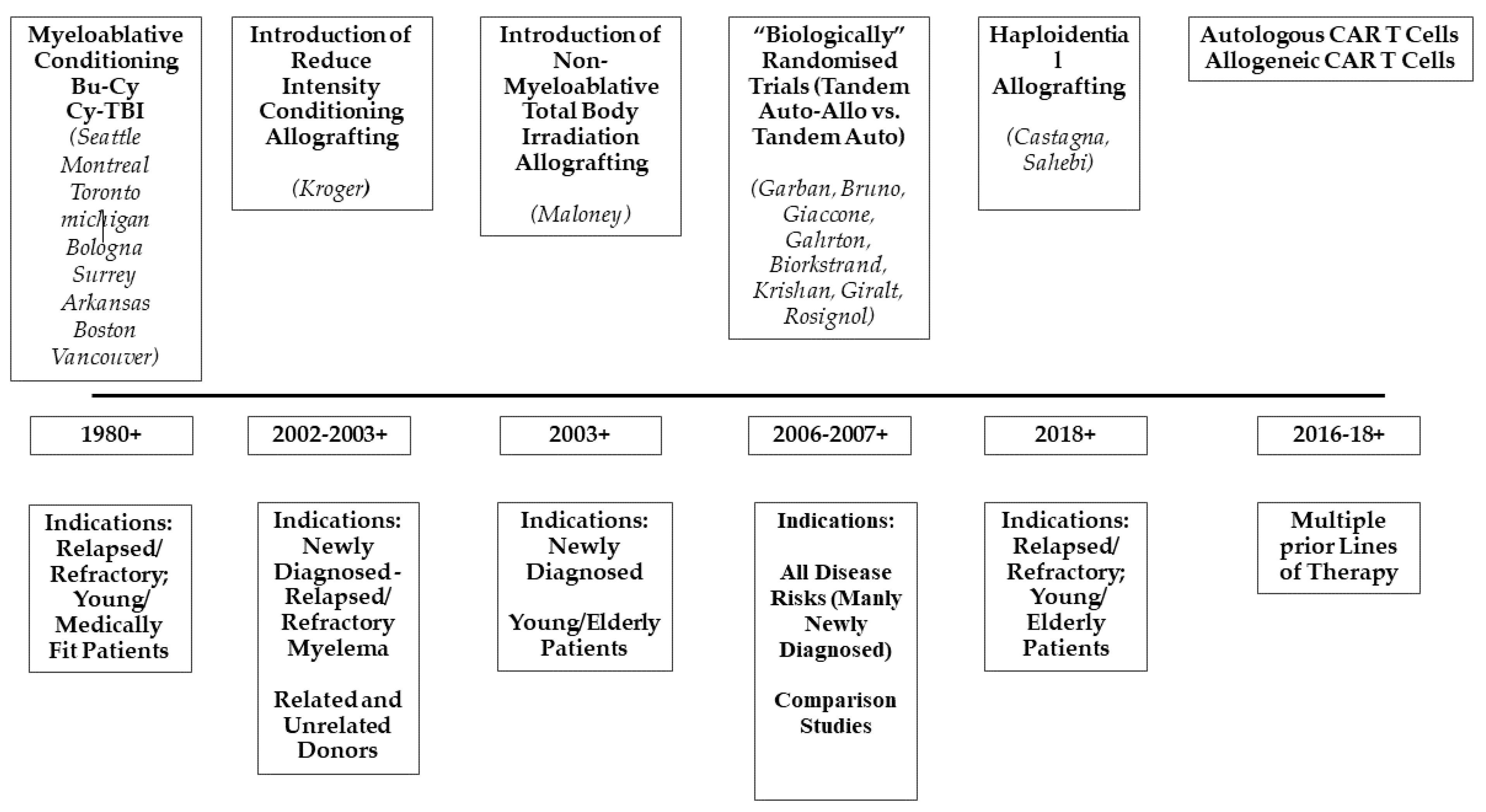
Figure 2.
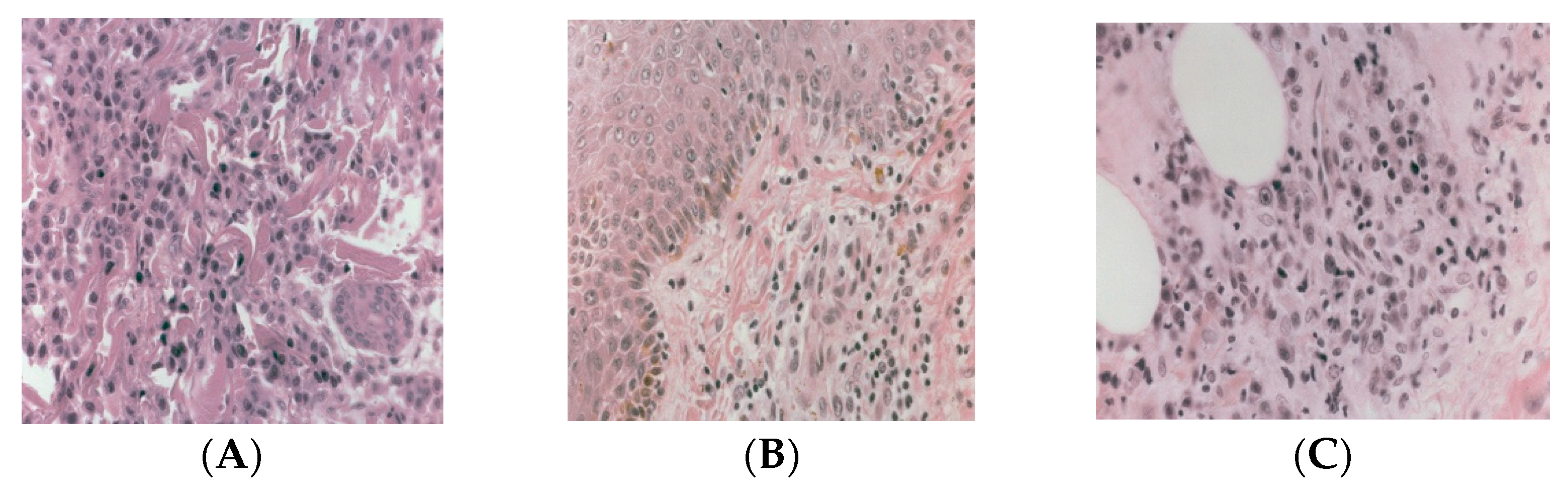
Graft-vs.-myeloma effect by histology (H&E staining). (A) biopsy proven myeloma cutis at day +19 post-allograft; (B) biopsy proven skin graft-vs.-host disease at day +45; (C) biopsy of myeloma cutis at day +60 showing lymphocyte infiltration and dying plasma cells. (Courtesy of Dr. D. Novero).
Figure 2.
Graft-vs.-myeloma effect by histology (H&E staining). (A) biopsy proven myeloma cutis at day +19 post-allograft; (B) biopsy proven skin graft-vs.-host disease at day +45; (C) biopsy of myeloma cutis at day +60 showing lymphocyte infiltration and dying plasma cells. (Courtesy of Dr. D. Novero).
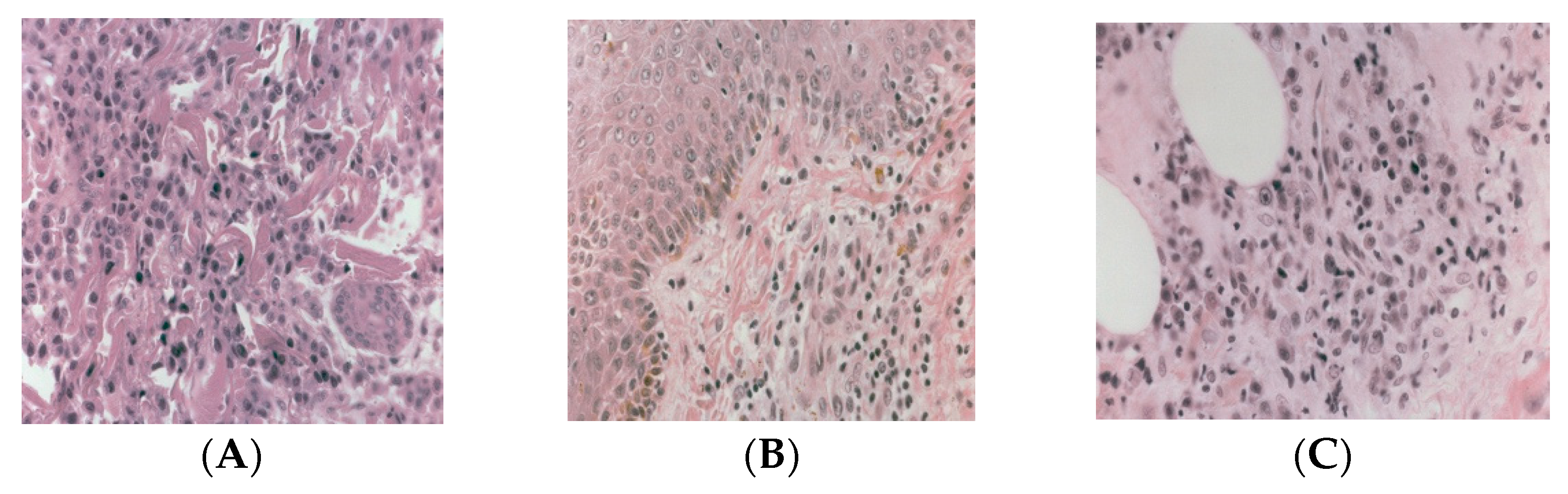
Figure 3.
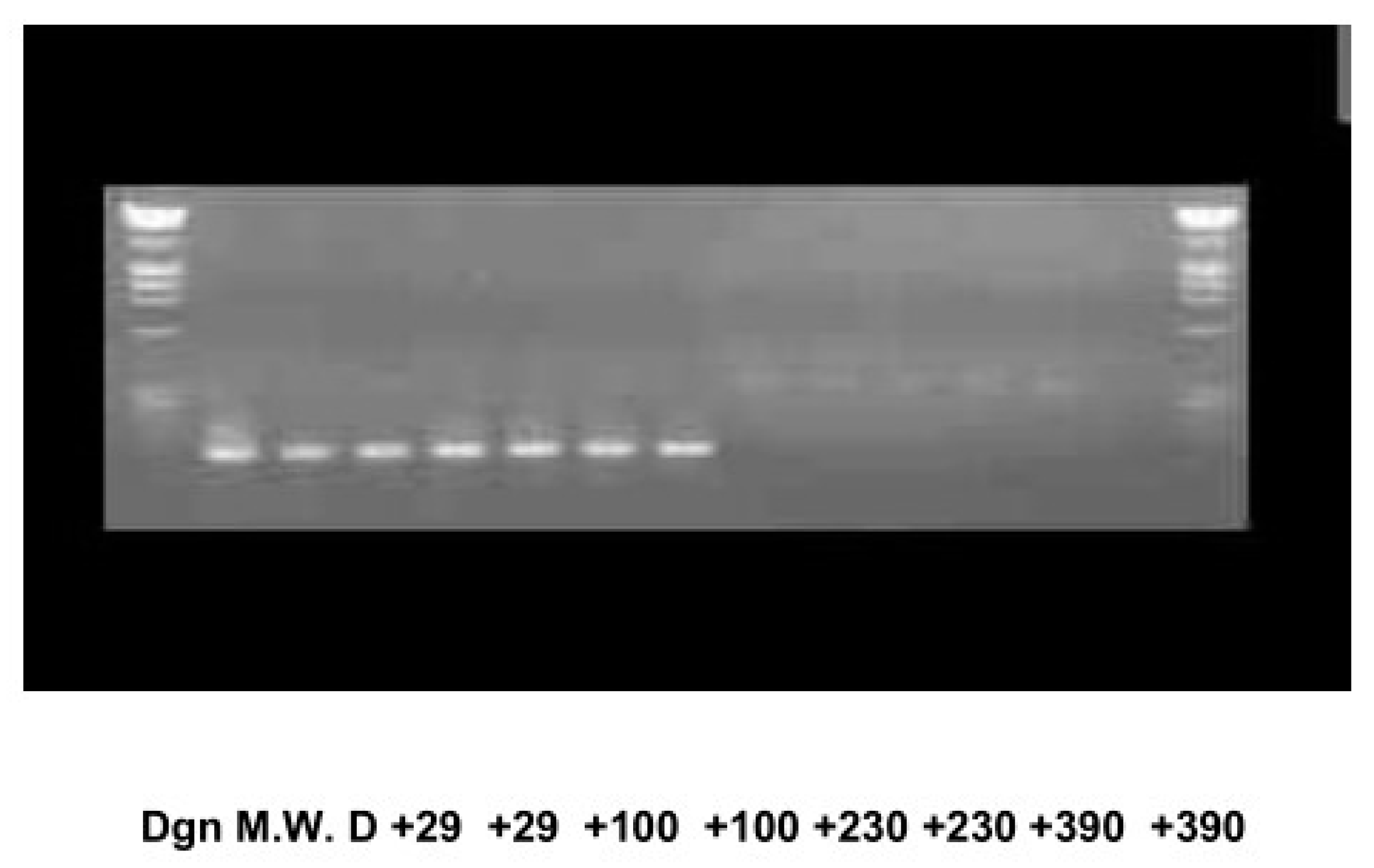
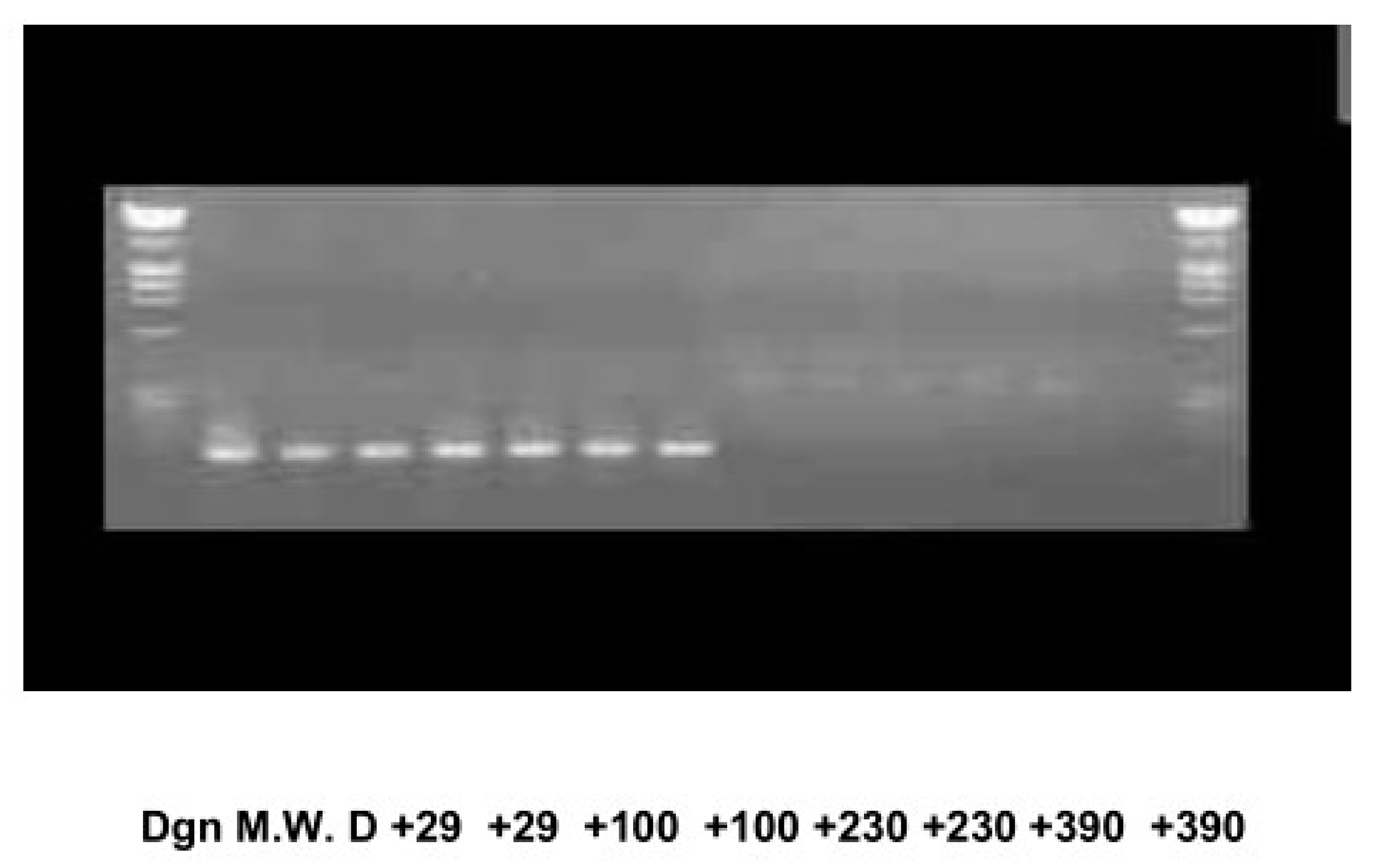
Graft-vs.-myeloma (GvM) and minimal residual disease (MDR) by nested PCR analysis. The patient reached molecular remission (sensitivity 1/106) in peripheral blood at one-year post-allograft and later in the bone marrow indicative of ongoing GvM. The patient has remained in continuous MDR negative remission for 20 years (Courtesy of Drs. M. Ladetto and D. Drandi) [61].
Figure 3.
Graft-vs.-myeloma (GvM) and minimal residual disease (MDR) by nested PCR analysis. The patient reached molecular remission (sensitivity 1/106) in peripheral blood at one-year post-allograft and later in the bone marrow indicative of ongoing GvM. The patient has remained in continuous MDR negative remission for 20 years (Courtesy of Drs. M. Ladetto and D. Drandi) [61].

{kind=link}
{kind=link}
{kind=link}
Table 1.
Myeloablative conditioning regimens for allografting in multiple myeloma.
| Reference | Conditioning | Transplant-Related Mortality % | Complete Remission % | Overall Survival % |
|---|---|---|---|---|
| 11 | Mel (100 mg/m2), TBI (12 Gy) | 53 (at 1 year) | --- | 39 (at 7 years) |
| 12 | Bu, Cy, ±TBI | 48 (at day 100) 63 (at 1 year) | 34 | 22 (at 5 years) |
| 13 | Cy, TBI Bu, Cy Mel (100 mg/m2), TBI | 19 (at day 100) | 62 | 47 (at 3 years) |
| 14 | Cy, TBI (14Gy) Bu, Cy | 10 | --- | 55 (at 2 years) |
| 15 | Mel (110 mg/m2), TBI (10.5Gy) Cy, TBI Cy, Mel Bu, Cy | 54 | 37 | 36 (at 3 years) |
| 16 | Cy, TBI (12Gy) Mel (140 mg/m2), TBI (10.5Gy) Bu, Cy Others | 22 | 57 | 32 (at 40 months) |
| 17 | Mel (160 mg/m2), TBI (12Gy) Cy, TBI (12Gy) Bu, Cy | 59 | 50 | 32 (at 3 years) |
| 18 | Cy, TBI Mel, TBI Bu, Cy, TBI Others | 25 | --- | 40 (at 3 years) |
Abbreviations: Bu: Busulfan; Cy: cyclophosphamide; TBI: total body irradiation; Mel: melphalan.
Table 2.
Allografting in multiple myeloma after the introduction of non-myeloablative/reduced intensity conditionings.
Table 2.
Allografting in multiple myeloma after the introduction of non-myeloablative/reduced intensity conditionings.
| Reference | Type of Conditioning/Study Design | Transplant-Related Mortality | Event Free Survival or Progression-Free Survival | Overall Survival |
|---|---|---|---|---|
| [21] | Non-myeloablative/Prospective Phase II Auto-Allo in Newly Diagnosed MM | 0% at 100 days | NR | 78% at 552 days |
| [22] | Reduced-Intensity/Prospective Phase II Auto-Allo in Newly Diagnosed MM | 11% at 100 days | 70% at 13 months | 76% at 13 months |
| [23] | Reduced Intensity/Prospective Phase II Auto-Allo from Unrelated Donors | 10% at 100 days | 53% at 2 years | 74% at 2 years |
| [24,25] | Reduced Intensity/Prospective Comparison Auto-Allo vs. Tandem Auto in High Risk Newly Diagnosed MM | 11% vs. NR | 19 vs. 22 months | 34 vs. 49 months |
| [26,27] | Non-myeloablative/Prospective Randomised Auto-Allo vs. Tandem Auto in Newly Diagnosed MM | 16% vs. 2% at 6.5 years | 35 vs. 29 months | 80 vs. 54 months |
| [28] | Reduced Intensity/Prospective Comparison Auto-Allo vs. Tandem Auto in High Risk Newly Diagnosed MM | 16% vs. 5% | Not reached vs. 31 months | Not reached vs. 58 months |
| [29,30] | Non-myeloablative/Prospective Randomised Auto-Allo vs. Tandem Auto in Newly Diagnosed MM | 16% vs. 3% at 8 years | 25% vs. 18% at 8 years 27% vs. 15% at 8 years | 42% vs. 33% at 10 years 42% vs. 29% at 10 years |
| [31,32] | Non-myeloablative/Prospective Randomised Auto-Allo vs. Tandem Auto in Newly Diagnosed MM | 20% vs. 9% at 6 years 20% vs. 11% at 10 years | 22% vs. 25% at 6 years 18% vs. 19% at 10 years | 59% vs. 60% at 6 years 44% vs. 43% at 10 years |
| [33,34] | Non-myeloablative/Prospective Randomised Auto-Allo vs. Tandem Auto in Newly Diagnosed MM | NR | 43% vs. 39% at 3 years 22% vs. 12% at 8 years | 75% vs. 68% at 3 years 49% vs. 36% at 8 years 48% vs. 27% at 10 years |
| [35] | Multiple regimens/Retrospective Haploidentical Allografting in MM Relapsed/Refractory Patients | 10% at 18 months | 33% at 18 months | 63% at 18 months |
| [36] | Multiple regimens/Retrospective Haploidentical Allografting in MM Relapsed/Refractory Patients | 21% at 1 year | 17% at 2 year | 48% at 2 year |
| [37] | Multiple regimens/Prospective Randomised Auto-Allo vs. Tandem Auto in MM Patients in First Relapse | 27% at 5 years | NR | 31% vs. 9% at 7 years |
Abbreviations: MM multiple myeloma, NR: not reported.
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Bruno, B.; Lia, G.; Bonifazi, F.; Giaccone, L. Decades of Progress in Allogeneic Stem Cell Transplantation for Multiple Myeloma. Hemato 2021, 2, 89-102. https://0-doi-org.brum.beds.ac.uk/10.3390/hemato2010005
AMA Style
Bruno B, Lia G, Bonifazi F, Giaccone L. Decades of Progress in Allogeneic Stem Cell Transplantation for Multiple Myeloma. Hemato. 2021; 2(1):89-102. https://0-doi-org.brum.beds.ac.uk/10.3390/hemato2010005
Chicago/Turabian StyleBruno, Benedetto, Giuseppe Lia, Francesca Bonifazi, and Luisa Giaccone. 2021. "Decades of Progress in Allogeneic Stem Cell Transplantation for Multiple Myeloma" Hemato 2, no. 1: 89-102. https://0-doi-org.brum.beds.ac.uk/10.3390/hemato2010005