My Health Diary, a School-Based Well-Being Program: A Randomized Controlled Study

 ,
, 

Abstract
:1. Introduction
2. Experimental Section
2.1. The Program
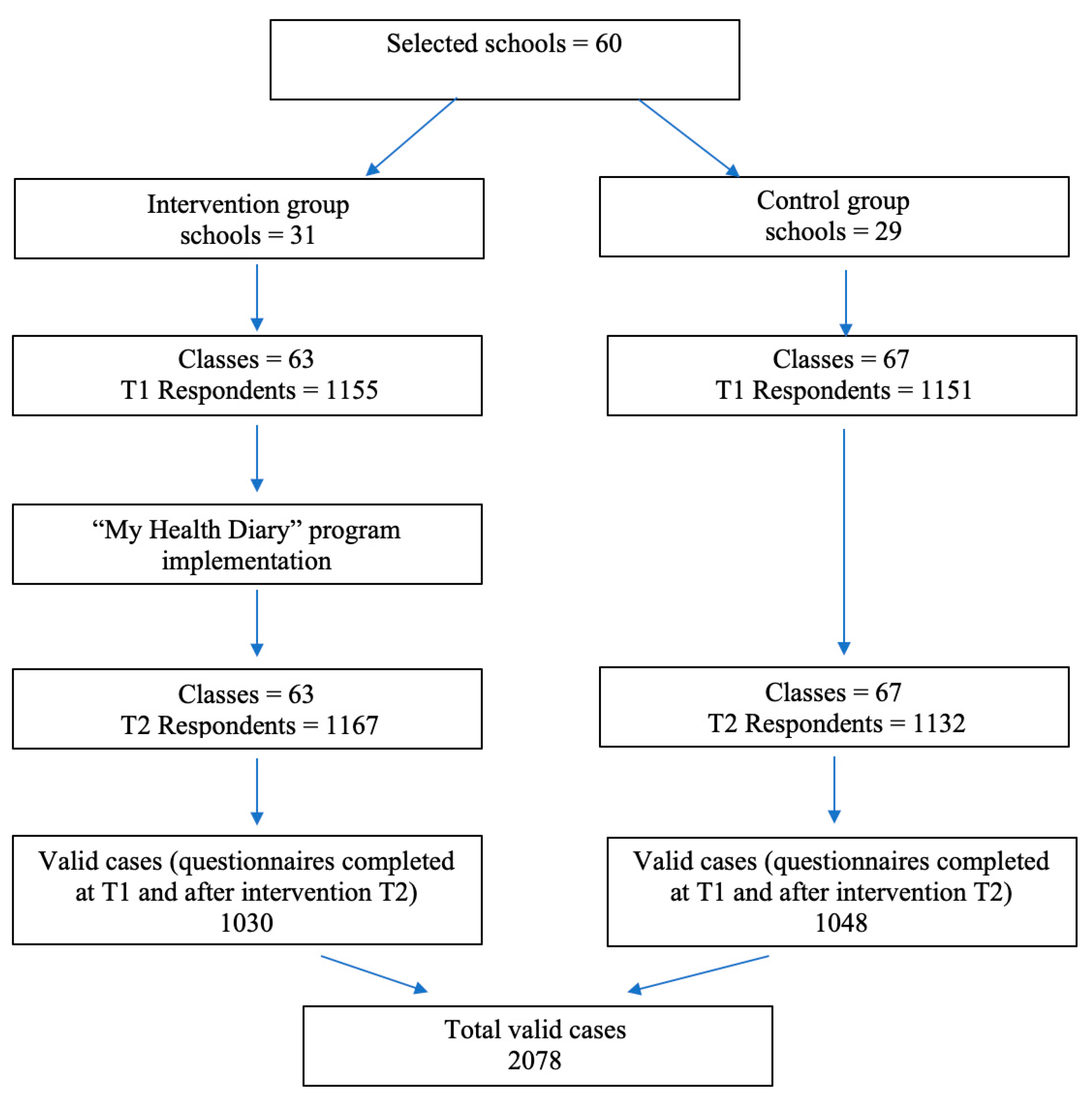
2.2. Participants
2.3. Data Collection
2.4. Measures
2.4.1. Primary Variables
- ▪
- Subjective Psychological Well-being: 4 dimensions (3 items for each dimension and a total of 12 items, on a 6-point Likert scale from 1—strongly disagree to 6—strongly agree: Autonomy, Cronbach’s α T1 = 0.46; T2 = 0.41; e.g., “I have confidence in my opinions, even if they are contrary to the general consensus”; Environmental Mastery, Cronbach’s α T1 = 0.40; T2 = 0.39; e.g., “In general, I feel I am in charge of the situation in which I live”; Positive relations with others, Cronbach’s α T1 = 0.37; T2 = 0.44; e.g., “People would describe me as a giving person, willing to share my time with others”; Self-acceptance, Cronbach’s α T1 = 0.39; T2 = 0.40; e.g., “When I look at the story of my life, I am pleased with how things have turned out”) from the Italian version of the Brief Psychological Well-Being Inventory [48,49,50]. This measure has been used for large-scale national surveys of adolescents [51,52] and was validated on an Italian population [53,54].
- ▪
- Subjective health status: 1 item “How would you rate your health?” (on a 4-point Likert scale: 1—excellent, 2—good, 3—fairly good, 4—poor) from the Italian version of the HBSC (WHO/Europe-Health Behavior in School-aged Children, Copenhagen, Denmark) Questionnaire for 13-year-olds. This item has been used extensively for periodic HBSC surveys of 13-year-olds at international and national levels [55]. Self-rated health is a valid predictor of mortality and morbidity [56].
- ▪
- Psychosomatic symptoms: 7 items (on a 5-point Likert scale: 1—rarely or never, 2—once or twice a month, 3—about every week, 4—more than once a week, and 5—about every day) from the Italian version of the HBSC Questionnaire for 13-year-olds—Symptom Checklist. These items ask students how often in the past 30 days they have suffered from headache/stomach ache/backache, irritability or bad temper, nervousness, sleeping difficulties, dizziness, and feeling low. The HBSC Symptom Checklist has been widely used for periodic HBSC surveys of 13-year-olds at international and national levels [55,57,58].
2.4.2. Secondary Variables
- ▪
- Risk behaviors: cigarette smoking (2 items), alcohol use (2 items), unhealthy eating habits (2 items), physical inactivity in terms of frequency of sedentary behaviors (2 items) from the Italian version of the HBSC Questionnaire for 13-year-olds (on a 4-point Likert scale regarding frequencies of these behaviors in the past 30 days: 1—never, 2—1–3 days, 3—4–5 days, 4—every day). All these items have been commonly used for the HBSC international and national surveys of 13-year-olds for similar health promotion and prevention programs [59,60].
- ▪
- Prosocial Behaviors: Prosocial Behavior Scale by Caprara et al. [61] (15 items, e.g., “I try to help others” on a 3-point Likert scale from 1—never to 3—often; Cronbach’s α T1 = 0.67; T2 = 0.70). This scale has been widely used for national surveys [61,62], including some pre-adolescents [63,64,65]. It is also used to assess the level of adjustment/maladjustment in children aged 7 to 12 years with the indicators of social adaptability [62].
- ▪
- Physical and Verbal Aggression: 20 items (e.g., “I kick and hit or punch”; “I threaten others” on a 3-point Likert scale from 1—never to 3—often; Cronbach’s α T1 = 0.81; T2 = 0.82) from the Physical and Verbal Aggression Scale by Caprara et al. [61]. This scale has been widely used to survey pre-adolescents nationally and internationally [61,63,64,65,66].
2.4.3. Mediator Variables
- ▪
- Emotional and social skills: Self-Efficacy in Regulating Positive Emotions (7 items, e.g., “How well can you rejoice over your successes?”—adolescent version; Cronbach’s α T1 = 0.76; T2 = 0.80) and Negative Emotions (8 items, e.g., “How well can you get over irritation quickly for wrongs you have experienced?”—adolescent version; Cronbach’s α T1 = 0.76; T2 = 0.79), Perceived Empathic Self-Efficacy (12 items, e.g., “How well can you read your friend’s needs?”—adolescent version; Cronbach’s α T1 = 0.86; T2 = 0.89), Perceived Social Self-Efficacy (13 items, e.g., “How well can you live up to what others think or expect of you?”—adolescent version; Cronbach’s α T1 = 0.86; T2 = 0.88) from versions of Bandura’s Self-Efficacy Scales [67] adapted and translated into Italian [68]. All items of the four self-efficacy domains are on a 5-point Likert scale: from 1—not well at all, to 5—very well. These scales have been used in large-scale national surveys of adolescents [69,70] and have good psychometric properties [68], which was confirmed by the reliability indexes in our study.
- ▪
- Satisfaction with school: 4 scales (5 items for each dimension on a 4-point Likert scale from 1—never to 4—always: Relationship with peers, Cronbach’s α T1 = 0.59; T2 = 0.57; e.g., “I feel comfortable with my classmates”; Relationship with teachers, Cronbach’s α T1 = 0.57; T2 = 0.59; e.g., “I can have a good dialog with my teachers”; Interest in study, Cronbach’s α T1 = 0.68; T2 = 0.71; e.g., “I listen with interest to what is being explained to me”; School Self-esteem, Cronbach’s α T1 = 0.66; T2 = 0.63; e.g., “I think I am a good student”) taken from the School Situation Questionnaire (student version, QSS-S) by Santinello and Bertarelli [30]. These scales have been used in large-scale surveys of adolescents at a national level.
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Havighurst, R.J. Human Development and Education; Longmans, Green: Oxford, UK, 1953. [Google Scholar]
- Manning, M.L. Havighurst’s developmental tasks, young adolescents, and diversity. Clear. House 2002, 76, 75–78. [Google Scholar] [CrossRef]
- Arnett, J.J. Adolescence and Emerging Adulthood; Pearson: Boston, MA, USA, 2010. [Google Scholar]
- Brown, B.B.; Prinstein, M.J. (Eds.) Encyclopedia of Adolescence; Academic Press: San Diego, CA, USA, 2011. [Google Scholar]
- Sawyer, S.M.; Afifi, R.A.; Bearinger, L.H.; Blakemore, S.J.; Dick, B.; Ezeh, A.C.; Patton, G.C. Adolescence: A foundation for future health. Lancet 2012, 379, 1630–1640. [Google Scholar] [CrossRef]
- Sawyer, S.M.; Azzopardi, P.S.; Wickremarathne, D.; Patton, G.C. The age of adolescence. Lancet Child Adolesc. Health 2018, 2, 223–228. [Google Scholar] [CrossRef]
- Clausen, J.A. Gender, contexts and turning points in adults’ lives. In Examining Lives in Contexts: Perspectives on the Ecology of Human Development; Moen, P., Elder, G.H., Jr., Lusher, K., Eds.; APA: Washington, DC, USA, 1995; pp. 365–389. [Google Scholar]
- Rutter, M. Transition and turning points in developmental psychopathology: As applied to the age span between childhood and mid-adulthood. Int. J. Behav. Dev. 1996, 19, 603–626. [Google Scholar] [CrossRef]
- Arnett, J.J. Emerging Adulthood: The Winding Road from the Late Teens through the Twenties; Oxford University Press: Oxford, UK, 2004. [Google Scholar]
- Bonino, S.; Cattelino, E.; Ciairano, S. Adolescents and Risks. In Behaviors, Functions and Protective Factors; Springer: Milan, Italy, 2005. [Google Scholar]
- Ciairano, S.; Schuur, W.H.; Bonino, S.; Molinengo, G.; Miceli, R. The use of psychoactive substances among Dutch and Italian adolescents: The contribution of personal and relational resources and vulnerabilities. Eur. J. Dev. Psychol. 2006, 3, 321–337. [Google Scholar] [CrossRef]
- Zins, J.E.; Elias, M.J. Social and Emotional Learning: Promoting the Development of all Students. J. Educ. Psychol. Consult. 2007, 17, 233–255. [Google Scholar] [CrossRef]
- Elias, M.J.; Gordon, J.S. Promoting social and emotional development in childhood and early adolescence. In A Blueprint for Promoting Academic and Social Competence in After-School Programs; Springer: Boston, MA, USA, 2009; pp. 63–77. [Google Scholar]
- Sancassiani, F.; Pintus, E.; Holte, A.; Paulus, P.; Moro, M.F.; Cossu, G.; Lindert, J. Enhancing the emotional and social skills of the youth to promote their well-being and positive development: A systematic review of universal school-based randomized controlled trials. Clin. Pract. Epidemiol. Ment. Health: CP EMH 2015, 11, 21. [Google Scholar] [CrossRef] [Green Version]
- Yirmiya, N. Editorial: The well-being of children: Empirical findings and implications for prevention and intervention. J. Child Psychol. Psychiatry 2007, 48, 741–743. [Google Scholar] [CrossRef]
- WHO. Life Skills Education for Children and Adolescents in Schools; Technical Documents; World Health Organization: Geneva, Switzerland, 1994. [Google Scholar]
- Botvin, G.J. Preventing adolescent drug abuse through Life Skills Training: Theory, methods, and effectiveness. In Social Programs that Work; Crane, J., Ed.; Russell Sage Foundation: New York, NY, USA, 1998; pp. 225–257. [Google Scholar]
- Botvin, G.; Griffin, K.W. Life Skills Training: Empirical findings and future directions. J. Prim. Prev. 2004, 25, 211–232. [Google Scholar] [CrossRef]
- Botvin, G.J.; Griffin, K.W. Life Skills Training: A competence enhancement approach to tobacco, alcohol, and drug abuse prevention. In Handbook of Adolescent Drug Use Prevention: Research, Intervention Strategies, and Practice; Scheier, L.M., Ed.; American Psychological Association: Washington, DC, USA, 2015; pp. 177–196. [Google Scholar] [CrossRef] [Green Version]
- Botvin, G.J. Life Skills Training; Princeton Health Press: White Plains, NY, USA, 2002. [Google Scholar]
- Osher, D.; Kidron, Y.; Brackett, M.; Dymnicki, A.; Jones, S.; Weissberg, R.P. Advancing the science and practice of social and emotional learning: Looking back and moving forward. Rev. Res. Educ. 2016, 40, 644–681. [Google Scholar] [CrossRef]
- Durlak, J.A.; Weissberg, R.P.; Dymnicki, A.B.; Taylor, R.D.; Schellinger, K.B. The impact of enhancing students’ social and emotional learning: A meta-analysis of school-based universal interventions. Child Dev. 2011, 82, 405–432. [Google Scholar] [CrossRef] [PubMed]
- Taylor, R.D.; Oberle, E.; Durlak, J.A.; Weissberg, R.P. Promoting positive youth development through school-based social and emotional learning interventions: A meta-analysis of follow-up effects. Child Dev. 2017, 88, 1156–1171. [Google Scholar] [CrossRef]
- WHO. Health 2020: A European Policy Framework Supporting Action Across Government and Society for Health and Well-Being; WHO Regional Office for Europe: Copenhagen, Denmark, 2013. [Google Scholar]
- WHO. The European Mental Health Action Plan. 2013–2020; WHO Regional Office for Europe: Copenhagen, Denmark, 2015. [Google Scholar]
- OECD. Skills for Social Progress: The Power of Social and Emotional Skills. OECD Skills Studies; OECD Publishing: Paris, France, 2015. [Google Scholar]
- Langford, R.; Bonell, C.P.; Jones, H.E.; Pouliou, T.; Murphy, S.M.; Waters, E.; Campbell, R. The WHO Health Promoting School framework for improving the health and well-being of students and their academic achievement. Cochrane Database Syst. Rev. 2014, 4. [Google Scholar] [CrossRef] [PubMed]
- Moral, B.L.; Romero, N.F.J.; Albiar, A.E.; Cid, L.J.A. The BAPNE Method as a School Intervention and Support Strategy to Improve the School Environment and Contribute to Socioemotional Learning (SEL). Int. J. Innov. Res. Educ. Sci. (IJIRES) 2015, 2, 450–456. [Google Scholar]
- Connor, C.A.; Dyson, J.; Cowdell, F.; Watson, R. Do universal school-based mental health promotion programmes improve the mental health and emotional well-being of young people? A literature review. J. Clin. Nurs. 2018, 27, e412–e426. [Google Scholar] [CrossRef] [Green Version]
- Santinello, M.; Bertarelli, P. La scuola come setting. In Conoscere la Comunità. L’analisi Degli Ambienti di Vita Quotidiana; Prezza, M., Santinello, M., Eds.; Il Mulino: Bologna, Italy, 2002; pp. 257–298. [Google Scholar]
- Cristini, F.; Santinello, M.; Scacchi, L.; Zini, L. Prevenire il consumo di sostanze psicoattive in preadolescenza: I risultati di un programma realizzato a scuola. Psicol. Clin. Svilupp. 2011, 15, 379–406. [Google Scholar]
- WHO. What is the Evidence on School Health Promotion in Improving School Health or Preventing Disease and Specifically What is the Effectiveness of the Health Promoting Schools Approach; WHO Regional Office for Europe: Copenhagen, Denmark, 2006. [Google Scholar]
- Rant, R.H.; Smith, J.A.; Kreiter, S.R.; Krowchuk, D.P. The relationship between early age of onset of initial substance use and engaging in multiple health risk behaviors among young adolescents. Arch. Pediatrics Adolesc. Med. 1999, 153, 286–291. [Google Scholar] [CrossRef] [Green Version]
- Jessor, R. Problem Behavior Theory and Adolescent Health; Springer International Publishing: Cham, Switzerland, 2017. [Google Scholar]
- Cavallo, F.; Lemma, P.; Dalmasso, P.; Vieno, A.; Lazzeri, G.; Galeone, D. Rapporto sui Dati HBSC Italia; Dipartimento di Scienze della Sanità Pubblica e Pediatriche: Torino, Italy, 2014. [Google Scholar]
- Biglan, A.; Brennan, P.A.; Foster, S.L.; Holder, H. Helping Adolescents at Risk: Prevention of Multiple Problem Behaviors; The Guildford Press: London, UK, 2004. [Google Scholar]
- Jackson, C.A.; Henderson, M.; Frank, J.W.; Haw, S.J. An overview of prevention of multiple risk behavior in adolescence and young adulthood. J. Public Health 2012, 34, 31–40. [Google Scholar] [CrossRef] [Green Version]
- Kipping, R.R.; Campbell, R.M.; Arthur, G.J.; Gunnell, D.J.; Hickman, M. Multiple risk behavior in adolescence. J. Public Health 2012, 34, 1–2. [Google Scholar] [CrossRef]
- Nation, M.; Crusto, C.; Wandersman, A.; Kumpfer, K.L.; Seybolt, D.; Morrissey, K.E.; Davino, K. What Works in Prevention. Principles of Effective Prevention Programs. USA Psychol. 2003, 58, 449. [Google Scholar] [CrossRef]
- Dishion, T.J.; Nelson, S.E.; Kavanagh, K. The family check-up with high-risk young adolescents: Preventing early-onset substance use by parent monitoring. Behav. Ther. 2003, 34, 553–571. [Google Scholar] [CrossRef]
- Dishion, T.J.; Shaw, D.; Connell, A.; Gardner, F.; Weaver, C.; Wilson, M. The family check-up with high-risk indigent families: Preventing problem behavior by increasing parents positive behavior support in early childhood. Child Dev. 2008, 79, 1395–1414. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weissberg, R.P.; Kumpfer, K.L.; Seligman, M.E. Prevention that works for children and youth. An introduction. USA Psychol. 2003, 58, 425–432. [Google Scholar] [CrossRef] [PubMed]
- Giannotta, F.; Ciairano, S.; Weichold, K.; Silbereisen, R.; Testa, S. Un intervento di life skills nella scuola media per la prevenzione dell’uso di sostanze. Psicol. Educazione 2008, 2, 325–344. [Google Scholar]
- Giannotta, F.; Settanni, M.; Kliewer, W.; Ciairano, S. Results of an Italian School-Based Expressive Writing Intervention Trial Focused on Peer Problem. J. Adolesc. 2009, 32, 1377–1390. [Google Scholar] [CrossRef]
- Allara, E.; Beccaria, F.; Molinar, R.; Marinaro, L.; Ermacora, A.; Coppo, A.; Faggiano, F. A school-based program to promote well-being in preadolescents: Results from a cluster quasi-experimental controlled study. J. Prim. Prev. 2019, 40, 151–170. [Google Scholar] [CrossRef] [Green Version]
- Beccaria, F.; Ermacora, A.; Marinaro, L.; Roggero, A.; Rabaglietti, E. Health Diary. Well-being promotion among pre-adolescents. [Diario della Salute. Percorsi di promozione del benessere tra i pre-adolescenti]. Sist. Salut. 2018, 62, 221–237. [Google Scholar]
- Galanti, M.R.; Siliquini, R.; Cuomo, L.; Melero, J.C.; Panella, M.; Faggiano, F.; EU-Dap Study Group. Testing anonymous link procedures for follow-up of adolescents in a school-based trial: The EU-DAP pilot study. Prev. Med. 2007, 44, 174–177. [Google Scholar] [CrossRef]
- Zani, B.; Cicognani, E. Le Vie del Benessere: Eventi di Vita e Strategie di Coping; Carocci: Roma, Italy, 1999. [Google Scholar]
- Ryff, C.D.; Keyes, C.L.M. The structure of psychological well-being revisited. J. Personal. Soc. Psychol. 1995, 69, 719–727. [Google Scholar] [CrossRef]
- Ryff, C.D.; Almeida, D.M.; Ayanian, J.S.; Carr, D.S.; Cleary, P.D.; Coe, C.; Williams, D. National Survey of Midlife Development in the United States (MIDUS II), 2004-2006: Documentation of the Psychosocial Constructs and Composite Variables in MIDUS II Project 1; Inter-university Consortium for Political and Social Research: Ann Arbor, MI, USA, 2007. [Google Scholar]
- Sagone, E.; Caroli, M.E. A correlational study on dispositional resilience, psychological well-being, and coping strategies in university students. Am. J. Educ. Res. 2014, 2, 463–471. [Google Scholar] [CrossRef]
- Ruini, C.; Ottolini, F.; Tomba, E.; Belaise, C.; Albieri, E.; Visani, D.; Offidani, E.; Caffo, E.; Fava, G.A. School intervention for promoting psychological well-being in adolescence. J. Behav. Ther. Exp. Psychiatry 2009, 40, 522–532. [Google Scholar] [CrossRef] [PubMed]
- Ruini, C.; Ottolini, F.; Rafanelli, C.; Ryff, C.D.; Fava, G.A. La validazione italiana delle Psychological Well-being Scales (PWB). Riv. Psichiatr. 2003, 38, 117–130. [Google Scholar]
- Sirigatti, S.; Stefanile, C.; Giannetti, E.; Iani, L.; Penzo, I.; Mazzeschi, A. Assessment of factor structure of Ryff’s Psychological Well-Being Scales in Italian adolescents. Boll. Psicol. Appl. 2009, 259, 30–50. [Google Scholar]
- Ravens, S.U.; Kokonyei, G.; Thomas, C. School and health. In Young People’s Health in Context: International Report from the HBSC 2001/2002 Survey. WHO Policy Series: Health Policy for Children and Adolescents. Issue 4; Currie, C., Roberts, C., Morgan, A., Smith, R., Settertobulte, W., Samdal, O., Barnekov, R.V., Eds.; WHO Regional Office for Europe: Copenhagen, Denmark, 2004. [Google Scholar]
- Idler, E.L.; Benyamini, Y. Self-rated health and mortality: A review of twenty-seven community studies. J. Health Soc. Behav. 1997, 38, 21–37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haugland, S.; Wold, B.; Stevenson, J.I.M.; Aaroe, L.E.; Woynarowska, B. Subjective health complaints in adolescence: A cross-national comparison of prevalence and dimensionality. Eur. J. Public Health 2001, 11, 4–10. [Google Scholar] [CrossRef]
- Ravens, S.U.; Erhart, M.; Torsheim, T.; Hetland, J.; Freeman, J.; Danielson, M.; Thomas, C. An international scoring system for self-reported health complaints in adolescents. Eur. J. Public Health 2008, 18, 294–299. [Google Scholar] [CrossRef] [Green Version]
- Faggiano, F.; Vigna, T.F.; Burkhart, G.; Bohrn, K.; Cuomo, L.; Gregori, D. The effectiveness of a school-based substance abuse prevention program: 18-month follow-up of the EU-Dap cluster randomized controlled trial. Drug Alcohol Depend. 2010, 108, 56–64. [Google Scholar] [CrossRef]
- Sloboda, Z.; Stephens, R.C.; Stephens, P.C.; Grey, S.F.; Teasdale, B.; Hawthorne, R.D. The adolescent substance abuse prevention study: A randomized field trial of a universal substance abuse prevention program. Drug Alcohol Depend. 2009, 102, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Caprara, G.V.; Borgogni, L.; Mazzotti, M.; Pastorelli, C. Indicatori precoci della relazione sociale. Eta Evol. 1988, 29, 91–101. [Google Scholar]
- Caprara, G.V.; Manzi, J.; Perugini, M. Investigating guilt in relation to emotionality and aggression. Personal. Individ. Differ. 1992, 13, 519–532. [Google Scholar] [CrossRef]
- Pastorelli, C.; Barbaranelli, C.; Cermak, I.; Rozsa, S.; Caprara, G.V. Measuring emotional instability, prosocial behavior and aggression in pre-adolescents: A cross-national study. Personal. Individ. Differ. 1997, 23, 691–703. [Google Scholar] [CrossRef]
- Caprara, G.V.; Laeng, M. Indicatori e Precursori della Condotta Aggressive; Bulzoni: Roma, Italy, 1988. [Google Scholar]
- Caprara, G.V.; Pastorelli, C. Early emotional instability, prosocial behavior, and aggression: Some methodological aspects. Eur. J. Personal. 1993, 7, 19–36. [Google Scholar] [CrossRef]
- Caprara, G.V.; Pastorelli, C. Toward a reorientation of research on aggression. Eur. J. Personal. 1989, 3, 121–138. [Google Scholar] [CrossRef]
- Bandura, A. Self-Efficacy: The Exercise of Control; W.H. Freeman: New York, NY, USA, 1997. [Google Scholar]
- Caprara, G.V. La Valutazione Dell’autoefficacia; Erikson: Trento, Italy, 2001. [Google Scholar]
- Caprara, G.V.; Delle, F.A.; Steca, P. Determinanti personali del benessere nell’adolescenza: Indicazioni e predittori. Psicol. Clin. Svilupp. 2002, 6, 203–234. [Google Scholar] [CrossRef]
- Gini, G.; Albiero, P.; Benelli, B. Relazione tra bullismo, empatia ed autoefficacia percepita in un campione di adolescenti. Psicol. Clin. Svilupp. 2005, 9, 457–472. [Google Scholar] [CrossRef]
- Diener, E.; Suh, E.M.; Lucas, R.E.; Smith, H.L. Subjective well-being: Three decades of progress. Psychol. Bull. 1999, 125, 276–302. [Google Scholar] [CrossRef]
- Currie, C.; Roberts, C.; Morgan, A.; Smith, R.; Settertobulte, W.; Samdal, O.; Barnekov Rasmussen, V. (Eds.) Young People’s Health in Context: International Report from the HBSC 2001/2002 Survey; WHO Policy Series: Health Policy for Children and Adolescents; Issue 4; WHO Regional Office for Europe: Copenhagen, Denmark, 2004. [Google Scholar]
- Friedman, H.S.; Kern, M.L. Personality, well-being, and health. Annu. Rev. Psychol. 2014, 65, 719–742. [Google Scholar] [CrossRef] [Green Version]
- Inchley, J.; Currie, D.; Young, T.; Torsheim, T.; Augustson, L.; Mathison, F. Health behavior in school-aged children (HBSC) study: International Report from the 2013/2014 survey. Health Policy Child. Adolesc. 2016, 7, 1–277. [Google Scholar]
- Rutter, M. Psychosocial resilience and protective mechanisms. Am. J. Orthopsychiatry 1987, 57, 316–333. [Google Scholar] [CrossRef]
- Crocetti, E.; Rabaglietti, E.; Sica, L.S. Personal Identity in Italy. New Dir. Child Adolesc. Dev. 2012, 138, 87–102. [Google Scholar] [CrossRef]
- Kenzie, K.; Hoyle, R.H. The self-absorption scale: Reliability and validity in non-clinical samples. Personal. Individ. Differ. 2008, 45, 726–731. [Google Scholar] [CrossRef]
- Simsek, O.F. Self-absorption paradox is not a paradox: Illuminating the dark side of self-reflection. Int. J. Psychol. 2013, 48, 1109–1121. [Google Scholar] [CrossRef] [PubMed]
- Berzonsky, M.D.; Branje, S.J.; Meeus, W. Identity-processing style, psychosocial resources, and adolescents’ perceptions of parent-adolescent relations. J. Early Adolesc. 2007, 27, 324–345. [Google Scholar] [CrossRef]
- Bukowski, W.M.; Sippola, L.K.; Hoza, B. Same and other: Interdependency between participation in same- and other-sex friendships. J. Youth Adolesc. 1999, 28, 439–459. [Google Scholar] [CrossRef]
- Poulin, F.; Pedersen, S. Developmental changes in gender composition of friendship networks in adolescent girls and boys. Dev. Psychol. 2007, 43, 1484–1496. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rabaglietti, E.; Ciairano, S. Quality of friendship relationships and developmental tasks in adolescence. Cognition 2008, 12, 183–203. [Google Scholar]
- Marengo, D.; Rabaglietti, E.; Tani, F. Internalizing Symptoms and Friendship Stability: Longitudinal Actor-Partner Effects in Early Adolescent Best Friend Dyads. J. Early Adolesc. 2018, 38, 947–965. [Google Scholar] [CrossRef]
- Gottfredson, D.; Wilson, D. Characteristics of effective school-based substance abuse prevention. Prev. Sci. 2003, 4, 27–38. [Google Scholar] [CrossRef]
- Weichold, K.; Giannotta, F.; Sillberaisen, R.K.; Ciairano, S.; Wenzel, V. Cross-cultural evaluation of a life-skills programme to combat adolescent substance misuse. Sucht Z. Wiss. Prax. 2006, 52, 268–278. [Google Scholar] [CrossRef]
- Junge, C.; Krienke, U.J.; Böhme, K.; Prüß, F.; Sander, A.; Niemann, J.; Langosch, J.M. The transition from primary to secondary school as stressful life event provoking risky drinking behaviors. J. Addict. Dis. 2016, 35, 128–134. [Google Scholar] [CrossRef]
- Giannotta, F.; Settanni, M.; Ciairano, S. Rischio e prevenzione in adolescenza: Dalla teoria all’intervento. In Il Benessere Psicosociale in Adolescenza. Prospettive Multidisciplinari; Albiero, P., Ed.; Carocci: Roma, Italy, 2012; pp. 301–328. [Google Scholar]
- Jessor, R.; Donovan, J.; Costa, F.M. Beyond Adolescent Problem Behavior and Young Adult Development; Cambridge University Press: New York, NY, USA, 1991. [Google Scholar] [CrossRef]
- Pape, H.; Hammert, T. How does Young People’s Alcohol Consumption Change during the Transition to Early Adulthood? A Longitudinal Study of Changes at Aggregate and Individual Level. Addiction 1996, 91, 1345–1357. [Google Scholar] [CrossRef] [PubMed]
- Ciairano, S.; Molinengo, G.; Bonino, S.; Miceli, R. Age of initiation with different substances and relationships with resources and vulnerabilities: A cross-national study. Eur. J. Dev. Psychol. 2009, 6, 666–684. [Google Scholar] [CrossRef] [Green Version]
- Steckler, A.B.; Linnan, L.; Israel, B. Process. Evaluation for Public Health Interventions and Research; Jossey-Bass: San Francisco, CA, USA, 2002; pp. 1–23. [Google Scholar]
- Brinthaupt, T.M.; Lipka, R.P. (Eds.) Understanding Early Adolescent Self and Identity: Applications and Interventions; SUNY Press: Albany, NY, USA, 2012. [Google Scholar]
- Lipsitz, J. Successful Schools for Young Adolescents; Routledge: London, UK, 2019. [Google Scholar] [CrossRef]
- Brigman, G.A.; Webb, L.D.; Campbell, C. Building skills for school success: Improving the academic and social competence of students. Prof. Sch. Couns. 2007, 10. [Google Scholar] [CrossRef]
- Tobler, N.S.; Roona, M.R.; Ochshorn, P.; Marshall, D.G.; Streke, A.V.; Stakepole, K.M. School-Based Drug Prevention Programs: A Meta-Analysis of the Research. J. Prim. Prev. 2000, 18, 71–128. [Google Scholar] [CrossRef]


{kind=link}
| Program Component | Activities | Materials | Duration (h) |
|---|---|---|---|
| Unit 1—My Emotions | Presentation, brainstorming, role-playing, recall of experiences associated with emotions, drawing, class discussion | Colored hats, marking pens, Post-it® notes, papers, posters | 3–4 |
| Unit 2—Beyond Stereotypes | Presentation, group work, game, class discussion | Photos, Identity cards, posters | 2 |
| Unit 3—Becoming Men & Women | Presentation, role-playing, group work, homework, class discussion | Newspapers or magazines, posters | 2–3 |
| Unit 4—Managing my Emotions | Presentation, group work, feedback, class discussion | Marking pens, Post-it® notes, my horoscope card | 2 |
| Unit 5—Others’ Emotions | Presentation, group work, stimulus game, class discussion | Marking pens, Post-it notes, ambiguous image cards | 3–4 |
| Pre-Intervention (Means) | Post-Intervention (Means) | |||||
|---|---|---|---|---|---|---|
| Intervention Group | Control Group | Intervention Group | Control group | |||
| Autonomy | M | 11.3 | 11.07 | 11.02 | 11.02 | Hotelling’s T = 0.000; F (1980;1) = 0.73, p = 0.39 |
| F | 10.9 | 10.7 | 10.7 | 10.8 | ||
| Environmental mastery | M | 12.5 | 12.5 | 12.7 | 12.8 | Hotelling’s T = 0.000; F (1956;1) = 0.86, p = 0.35 |
| F | 12.4 | 12.4 | 12.6 | 12.4 | ||
| Positive relationships with others | M | 12.7 | 12.6 | 12.6 | 12.7 | Hotelling’s T = 0.000; F (1941;1) = 0.17, p = 0.68 |
| F | 13.3 | 12.9 | 13.1 | 13.0 | ||
| Self-acceptance | M | 12.1 | 12.1 | 11.9 | 12.1 | Hotelling’s T = 0.000; F (1992;1) = 0.34, p = 0.56 |
| F | 11.8 | 11.8 | 11.6 | 11.6 | ||
| Pre-Intervention | Post-Intervention | |||
|---|---|---|---|---|
| Intervention Group | Control Group | Intervention Group | Control Group | |
| Never | 43% (430) | 43% (441) | 34% (348) | 34% (356) |
| 1–2 times a month | 29% (296) | 30% (308) | 31% (317) | 36% (379) |
| 1 or more times a week | 27% (276) | 28% (287) | 35% (358) | 29% (306) |
| Pre-Intervention | Post-Intervention | |||
|---|---|---|---|---|
| Intervention Group | Control Group | Intervention Group | Control group | |
| No | 98% (1003) | 97% (1013) | 96% (978) | 94% (975) |
| Yes | 2% (16) | 3% (28) | 4% (45) | 6% (62) |
| Pre-Intervention (Means) | Post-Intervention (Means) | ||||||
|---|---|---|---|---|---|---|---|
| Intervention Group | Control Group | Intervention Group | Control Group | ||||
| Self-efficacy, negative emotions | M | 25.3 | 25.4 | 25.8 | 26.1 | Hotelling’s T = 0.000 F (1962;1) = 0.82, p = 0.09 | |
| F | 23.6 | 23.2 | 23.4 | 23.7 | |||
| Self-efficacy, positive emotions | M | 28.3 | 28.3 | 28.4 | 28.6 | Hotelling’s T = 0.001 F (2014;1) = 2.3, p = 0.13 | |
| F | 29.3 | 29.2 | 29.4 | 29.1 | |||
| Empathic self-efficacy | M | 40.7 | 40.8 | 41.0 | 42.1 | Hotelling’s T = 0.002 F (1939;1) = 3.9, p = 0.048 * | |
| F | 42.5 | 42.1 | 43.0 | 42.3 | |||
| Social self-efficacy | M | 49.8 | 50.6 | 49.9 | 50.9 | Hotelling’s T = 0.002 F (1873;1) = 4.5, p = 0.03 * | |
| F | 47.6 | 47.6 | 48.4 | 47.3 | |||
| School self-esteem | M | 13.7 | 13.9 | 13.8 | 14.0 | Hotelling’s T = 0.000; F (1937;1) = 0.93, p = 0.34 | |
| F | 13.3 | 13.2 | 13.1 | 13.3 | |||
| Interest in study | M | 13.1 | 12.8 | 12.6 | 12.5 | Hotelling’s T = 0.000 F (1913;1) = 0.29, p = 0.58 | |
| F | 13.5 | 13.4 | 12.9 | 13.0 | |||
| Relationship with peers | M | 15.6 | 15.6 | 15.3 | 15.6 | Hotelling’s T = 0.002 F (1939;1) = 5.59, p = 0.02 ** | |
| F | 15.6 | 15.7 | 15.5 | 15.3 | |||
| Relationship with teachers | M | 14.0 | 13.9 | 13.3 | 13.1 | Hotelling’s T = 0.000 F (1908;1) = 0.53, p = 0.47 | |
| F | 14.4 | 14.3 | 13.6 | 13.6 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rabaglietti, E.; Molinengo, G.; Roggero, A.; Ermacora, A.; Marinaro, L.; Beccaria, F. My Health Diary, a School-Based Well-Being Program: A Randomized Controlled Study. Adolescents 2021, 1, 21-35. https://0-doi-org.brum.beds.ac.uk/10.3390/adolescents1010003
Rabaglietti E, Molinengo G, Roggero A, Ermacora A, Marinaro L, Beccaria F. My Health Diary, a School-Based Well-Being Program: A Randomized Controlled Study. Adolescents. 2021; 1(1):21-35. https://0-doi-org.brum.beds.ac.uk/10.3390/adolescents1010003
Chicago/Turabian StyleRabaglietti, Emanuela, Giorgia Molinengo, Antonella Roggero, Antonella Ermacora, Laura Marinaro, and Franca Beccaria. 2021. "My Health Diary, a School-Based Well-Being Program: A Randomized Controlled Study" Adolescents 1, no. 1: 21-35. https://0-doi-org.brum.beds.ac.uk/10.3390/adolescents1010003