1. Introduction
Hyperglycemia is a common condition in critically ill patients. Transient hyperglycemia in this context is usually referred to as “stress hyperglycemia” [
1,
2,
3]: In contrast to hyperglycemia due to type 2 diabetes mellitus, stress hyperglycemia is primarily caused by hepatic gluconeogenesis and glycogenolysis [
4]. Patients admitted to an intensive care unit (ICU) represent an inhomogeneous collective and hyperglycemia might need a differential evaluation depending on the underlying disorder.
Hyperglycemic derailment is known to be associated with adverse outcome and increased mortality in patients suffering from an acute myocardial infarction (AMI) [
5]. In these patients there is an ongoing debate whether increased glucose concentration constitutes an independent risk factor or depicts only a severity parameter of illness in certain circumstances. Of note, the association between stress hyperglycemia and mortality in AMI patients is at least more pronounced in non-diabetic patients, and it was speculated that patients with pre-existing diabetes mellitus undergo cellular adaptation to hyperglycemia as reactive oxygen species production by the mitochondria is reduced [
6,
7].
In septic patients severe hyperglycemia (blood glucose >200 mg/dL) but not mild hyperglycemia (141–199 mg/dL) was recently reported to be associated with increased mortality [
8]. Up to a certain degree, stress hyperglycemia is thought to be adaptive to hemodynamic changes in patients suffering from sepsis [
9]: Sufficient glucose supply is essential for all cells. As sepsis leads to hypo-perfusion and glucose uptake depends on a concentration gradient, an increase in blood glucose levels is a physiologic and necessary response mechanism to hypo-perfusion [
10]. Whereas in the early 2000s tight glucose control in septic patients was thought to be beneficial, it could be shown in large, prospective trials that intensive glucose control is even detrimental for these patients [
11,
12,
13]. Therefore, in septic patients, stress hyperglycemia is considered a beneficial response of the organism and only liberal management of high glucose, avoiding glucose concentrations leading to fluid shifts by serum osmolality changes, is recommended [
14]. It is well known that patients suffering from diabetes are at increased risk for infection and sepsis due to humoral defects and impaired host response [
15,
16,
17]. Even though, and in contrast to AMI patients, septic patients with known diabetes mellitus do not reveal increased mortality as reported by van Vught et al. and Esper et al. [
8,
18].
Both, septic and AMI patients are frequently admitted to ICUs, but a detailed assessment of these collectives is needed. We therefore compared associations of severe hyperglycemia and mortality in ICU patients suffering from either AMI or sepsis with and without pre-diagnosed diabetes mellitus.
2. Results
In total, 2551 patients were investigated. Among these, 572 were admitted to the ICU due to sepsis and 1979 patients because of an AMI. Mean follow-up time was 2135 ± 45 days. Baseline characteristics are shown in
Table 1. Patients admitted for sepsis were of similar age (68 (58–77) vs. 69 (59–77) years,
p = 0.18) but were clinically sicker as mirrored by both, higher SAPS2 (54 ± 20 vs. 33 ± 16;
p < 0.001) and APACHE (26 ± 8 vs. 16 ± 8;
p < 0.001) scores compared to patients admitted for AMI. Further, heart rate was higher in septic patients (118 ± 18 vs. 91 ± 20 bpm (beats per minute);
p < 0.001) and they evidenced more pronounced laboratory organ failure, higher white blood cell count (16.5 ± 14.1 vs. 11.2 ± 4.7;
p < 0.001) and lactate concentration (4.4 ± 4.9 vs. 2.1 ± 3.3 mmol/L;
p < 0.001) on the admission day as shown in
Table 1.
As continuous variable, maximum glucose concentration on the day of admission was associated in a Cox regression analysis with mortality in the overall cohort (HR = 1.006, 95% CI: 1.004–1.009;
p < 0.001) and in patients suffering from AMI (HR = 1.101, 95% CI: 1.075–1.127;
p < 0.001) but only in trend in patients admitted to an ICU for sepsis (HR 1.030, 95% CI: 0.998–1.062;
p = 0.07) (
Table 2).
To further analyze effects of severe hyperglycemia (i.e., a glucose concentration above 200 mg/dL) we split our cohort in two groups based on this cut-off. In the overall cohort, patients with severe hyperglycemia were older (71 (63–78) vs. 69 (57–77) years;
p < 0.001), more obese (BMI 28 ± 5 vs. 27 ± 4;
p < 0.01) and sicker (APACHE2 score 24 ± 10 vs. 19 ± 9;
p < 0.01; SAPS2 score 47 ± 20 vs. 39 ± 20;
p < 0.01). Patients suffering from severe hyperglycemia evidenced higher lactate concentrations (4.1 ± 5.8 vs. 2.4 ± 3.1;
p < 0.001), higher heart rate (107 ± 24 vs. 98 ± 23 bpm;
p < 0.001) and more pronounced laboratory multi-organ failure as shown in
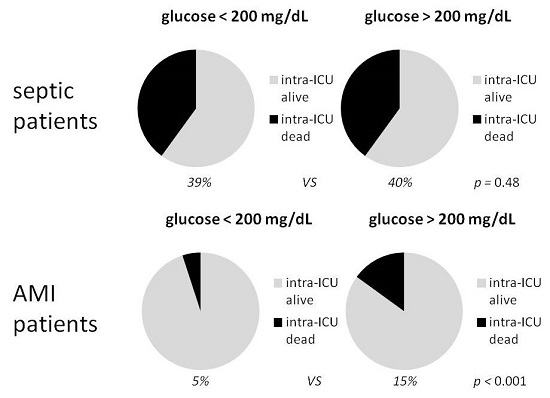
Table 3. In our overall population, severe hyperglycemia (>200 mg/dL) was associated with increased mortality both intra-ICU (23% vs. 13%;
p < 0.001) and long-term (HR = 1.74, 95% CI: 1.44–2.09;
p < 0.001) (
Table 4 and
Figure 1).
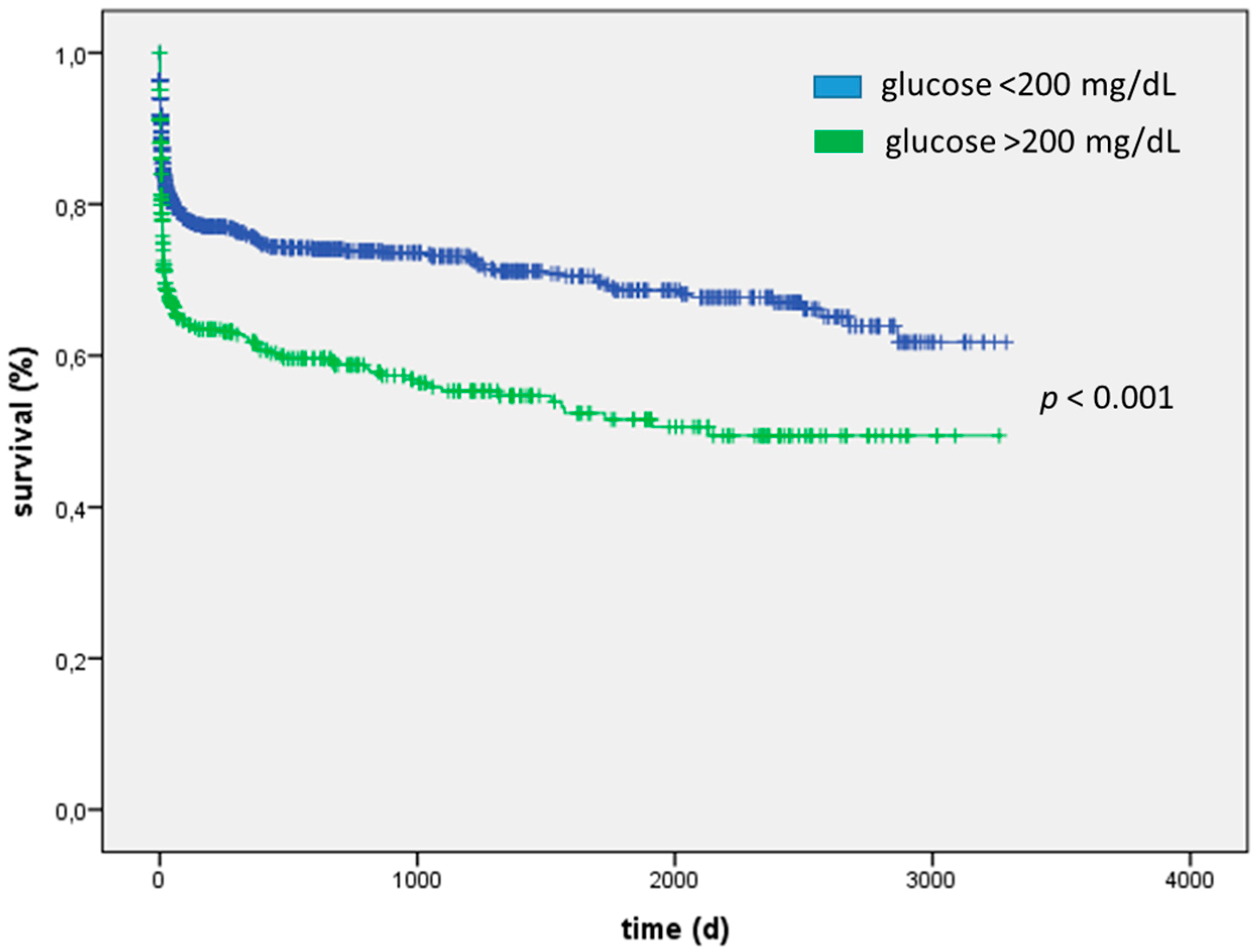
For patients admitted for sepsis, severe hyperglycemia was not associated with increased mortality, neither short-term (40% vs. 39%;
p = 0.5) nor long-term (HR = 1.13, 95% CI: 0.89–1.44;
p = 0.32) (
Table 4 and
Figure 2). AUC for blood glucose concentration was low (AUC 0.52, 95% CI: 0.49–0.56). Interestingly, in sepsis, severe hyperglycemic patients were of equal age compared with those without severe hyperglycemia (68 (59–77) vs. 68 (55–76) years;
p = 0.21) and whereas APACHE2 score was higher (28 ± 8 vs. 26 ± 8;
p = 0.02) SAPS2 scores (55 ± 20 vs. 53 ± 20;
p = 0.25) did not differ between the groups indicating a clinically similarly sick collective. Further biomarkers of renal (creatinine 184 (114–317) vs. 180 (112–292) µmol/L;
p = 0.46) and liver failure (ALAT 0.7 (0.4–1.2) vs. 0.7 (0.3–1.4) µmol/(l*s),
p = 0.69; ASAT 1.1 (0.5–2.9) vs. 1.0 (0.4–2.5) µmol/(l*s),
p = 0.34) and blood lactate concentration (4.8 ± 5.3 vs. 4.1 ± 4.8 mmol/L;
p = 0.17) and heart rate (119 ± 23 vs. 118 ± 22 bpm;
p = 0.65) were similar (
Table 5).
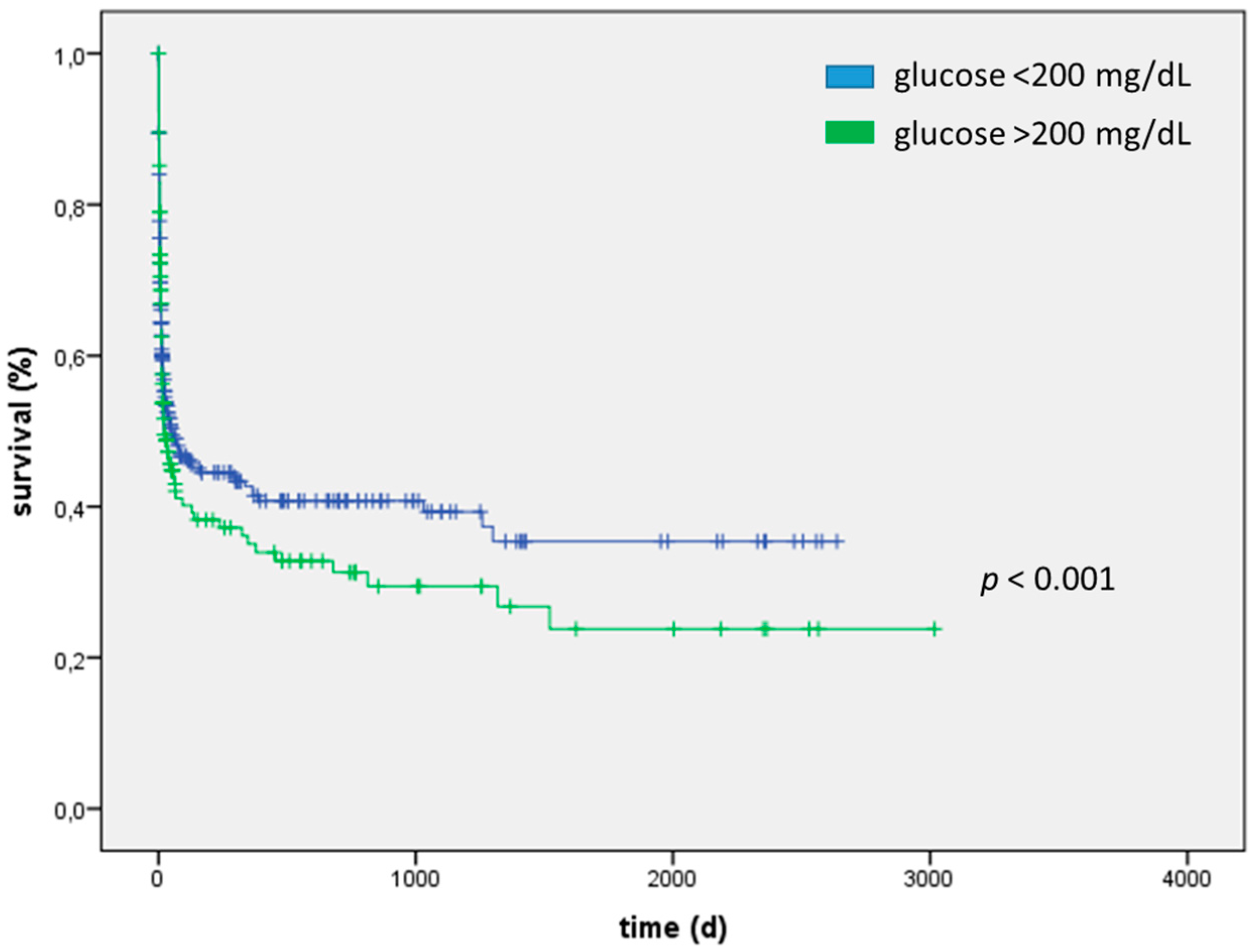
Myocardial inarction patients with severe hyperglycemia at admission day evidenced a significantly increased mortality both short-term (15%; vs. 5%
p < 0.001) and long-term (HR = 2.19, 95% CI: 1.66–2.89;
p < 0.001) (
Table 4 and
Figure 3). ROC analysis for blood glucose concentration was performed for patients suffering from AMI (AUC 0.70, 95% CI: 0.67–0.72). Myocardial infarction patients with severe hyperglycemia were older (73 (65–79) vs. 68 (57–77) years;
p < 0.001), more obese (BMI 29 ± 5 vs. 28 ± 4;
p < 0.001) and clinically sicker (APACHE2 score 21 ± 9 vs. 16 ± 8;
p < 0.001; SAPS2 score 41 ± 18 vs. 32 ± 16;
p < 0.001). Blood lactate concentration (3.7 ± 6.1 vs. 1.8 ± 1.9 mmol/L;
p < 0.001), heart rate (101 ± 22 vs. 92 ± 20 bpm;
p < 0.001) and white blood cell count (13.2 ± 4.9 vs. 11.2 ± 5.2 G/L;
p < 0.001) and markers of multi-organ failure were significantly higher in patients with severe hyperglycemia as shown in
Table 6. Of note, patients suffering from severe hyperglycemia were more likely to have pre-diagnosed type 2 diabetes (29% vs. 10%;
p < 0.001).
A medical history of type 2 diabetes (
n = 337; 13%) was not associated with increased mortality: Neither intra-ICU (15% vs. 15%;
p = 0.93) nor long term (HR = 1.140, 95% CI: 0.91–1.44;
p = 0.26) in the overall cohort, nor in any of the sub-cohorts of AMI patients (HR = 0.82, 95% CI: 0.49–1.38;
p = 0.53) and septic patients (HR = 1.29, 95% CI: 0.79–2.09;
p = 0.32), although diabetic patients had higher blood glucose concentrations (213 ± 76 vs. 175 ± 70 mg/dL;
p < 0.001), were older (72 (65–78) vs. 68 (57–77) years;
p < 0.001), more obese (BMI 29 ± 4 vs. 28 ± 5;
p < 0.001) and clinically sicker (APACHE2 score 22 ± 10 vs. 20 ± 10;
p = 0.02; SAPS2 score 43 ± 21 vs. 40 ± 20;
p = 0.06) (
Table 7).
Of note, those patients with severe hyperglycemia-indicating at least an increased risk for diabetes- and/or a known medical history of type 2 diabetes taken together, evidenced significantly increased short-term (22% vs. 13%; p < 0.001) and long-term mortality (HR = 1.76, 95% CI: 1.47–2.11; p < 0.001) in the overall cohort, as well as in the AMI sub-group (intra-ICU 13% vs. 5%; p < 0.001) long-term HR = 2.13, 95% CI: 1.61–2.80; p < 0.001), but not in septic patients (intra-ICU 38% vs. 41%; p = 0.53; long term HR = 1.24, 95% CI: 0.98–1.57; p = 0.08).
We further investigated the role of hypoglycemia on the day of admission. In AMI patients 1.2% and in septic patients 5.4% suffered from hypoglycemia on admission day. We investigated associations of hypoglycemia, defined as glucose concentration below 50 mg/dL, with mortality. In patients suffering from sepsis hypoglycemia was associated with both long-term (HR = 2.39, 95% CI: 1.51–3.77; p < 0.001) and intra-ICU (68% vs. 38%; p = 0.002). In AMI patients hypoglycemia was associated with adverse long-term outcome (HR = 3.12, 95% CI: 1.38–7.03; p = 0.006) and with intra-ICU mortality at least in trend (19% vs. 8%; p = 0.12). To exclude an effect of hypoglycemia on the associations between severe hyperglycemia and outcome we excluded patients suffering from hypoglycemia: In septic patients long term mortality (HR = 1.15, 95% CI: 0.90–1.48; p = 0.27) and short-term mortality (39% vs. 38%; p = 0.77) were not associated with severe hyperglycemia whereas in patients suffering from AMI severe hyperglycemia was associated with both short-term (14% vs. 5%; p < 0.001) and long-term mortality (HR = 2.19, 95% CI: 1.65–2.90; p < 0.001).
3. Discussion
Severe hyperglycemia (blood glucose concentration >200 mg/dL) was associated with adverse outcome in the overall cohort and in patients suffering from myocardial infarction, but not in septic patients. We therefore think that hyperglycemia should be considered and handled differently in those patient collectives.
It has been proven recently that even a single peak of hyperglycemia can exaggerate oxidative stress, induce cell apoptosis as well as endothelial dysfunction and stimulate coagulation and platelet aggregation [
19,
20,
21,
22,
23]. We therefore decided to report and investigate effects of the maximum blood glucose concentration on the day of admission to ICU.
Hyperglycemia is well known to be associated with adverse outcomes as well as reduced left ventricular (LV) function in AMI patients [
24,
25]. It is not clear until now, to what extent these associations are causal and in which way hyperglycemia itself contributes to adverse outcome. Furthermore, hyperglycemia is known to be associated with ischemia-reperfusion injury, increased infarct size in an animal model and tight glycemic control was reported to increase regenerative potential of infarcted myocardium [
26,
27,
28]. In our study, AMI patients exhibiting severe hyperglycemia had significantly elevated SAPS2 and APACHE scores compared to those without severe hyperglycemia (APACHE2 score 21 ± 9 vs. 16 ± 8;
p < 0.001; SAPS2 score 41 ± 18 vs. 32 ± 16;
p < 0.001) indicating sicker patients in which tissue perfusion is impaired. This finding could be interpreted as evidence for the hypothesis that glucose concentration primarily mirrors illness severity. An investigation of a possible causative relationship between hyperglycemia and adverse outcome is beyond the scope of this study: further, prospective studies and experimental efforts are needed.
In septic patients, maximum glucose concentration on the day of admission was only in trend associated with mortality. Even severe hyperglycemia was not associated with adverse outcome in those patients. In accordance, patients suffering from sepsis and severe hyperglycemia were of similar age compared to septic patients with a blood glucose concentration <200 mg/dL, and did not evidence higher blood lactate concentrations, increased laboratory markers of multi-organ failure and SAPS2. We think this further supports the notion that hyperglycemia in sepsis, i.e., stress hyperglycemia, should not be considered harmful, as stated before by Tiruvoipati et al. [
9]. In this condition, hyperglycemia should primarily be seen as an adaptive mechanism to hypo-perfusion to ensure sufficient glucose supply for peripheral cells by facilitating glucose uptake–a passive mechanism–by increasing blood glucose concentration [
10]. Lesur et al. postulated that the stress response of septic patients is different to non-septic ICU patients’ levels [
29]. In addition, this would be in accordance to prospective studies, e.g., NICE-SUGAR, which could even show an adverse outcome for tight glucose control in septic patients [
11].
For blood glucose concentration a U-shaped relationship with outcome was shown in critically ill in several previous studies [
30,
31,
32]. In our cohort hypoglycemia was associated with adverse outcome for both septic and AMI patients. Still, after exclusion of patients suffering from hypoglycemia the associations we reported in this study between severe hyperglycemia and sepsis or AMI, remained unaltered.
In our study, cohort a medical history of type 2 diabetes was not associated with increased mortality neither intra-ICU nor long both in AMI and septic patients. This goes in line with the findings of Wang and co-workers who could show that although diabetes leads to contractile and metabolic abnormalities during normoxia, there is no association between diabetes and increased susceptibility to injury due to ischemia [
33]. On the other hand, whereas in short term optimal intensive care treatment might outplay possible detrimental effects of diabetes, in the long-term we would expect adverse outcome in patients suffering from diabetes mellitus. Only 13% of our cohort, representing a typical cohort of medical ICU-patients, was pre-diagnosed with diabetes. We therefore speculate that the neutral effect of pre-diagnosed diabetes mellitus in the long-term might be due to under-diagnosis of type 2 diabetes in our cohort, as prevalence in patients aged 65 and older is known to be as high as 25% (and rising) [
34]. Due to the retrospective design of our study, we could not further elucidate this hypothesis as neither oral glucose tolerance test results nor Hba1c levels were available for analysis. This speculation is in contrast to findings of Ishihara et al. who could show—for their cohort of AMI patients—that patients with stress hyperglycemia did not show increased prevalence of diabetes at the time of presentation by means of oral glucose tolerance test (OGTT) [
35]. Of note, OGTT might underdiagnose diabetes compared to Hba1c and stress hyperglycemia might still be associated with higher risk for developing diabetes [
36,
37].
As others reported that patients evidencing stress hyperglycemia are known to be at higher risk for impaired fasting glucose and developing diabetes, we aimed to find out if patients with a known medical history of diabetes and/or severe hyperglycemia on the admission day had adverse outcome [
38,
39]: This was true for the overall cohort and AMI patients (intra-ICU mortality 13% vs. 5%;
p < 0.001; long-term mortality HR = 2.13, 95% CI: 1.61–2.80;
p < 0.001) but could not be shown for septic patients (intra-ICU mortality 41% vs. 38%;
p = 0.53; long term mortality HR = 1.24, 95% CI: 0.98–1.57;
p = 0.08). This of course does not proof a relationship of stress hyperglycemia and diabetes but we strongly believe that this further under-strikes a primarily beneficial role of hyperglycemia in septic patients. On the other hand, in patients suffering from AMI, severe hyperglycemia might mirror both the severity of the acute event, as well as the patients’ comorbidities, such as diabetes, and therefore identify patients at high risk for death.


 ,
, 




{kind=link}
{kind=link}
{kind=link}
{kind=link}