In Vitro Feasibility Analysis of a New Sutureless Wound-Closure System Based on a Temperature-Regulated Laser and a Transparent Collagen Membrane for Laser Tissue Soldering (LTS)

 , ,
, , {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Results
2.1. Structural Analysis of the Membrane
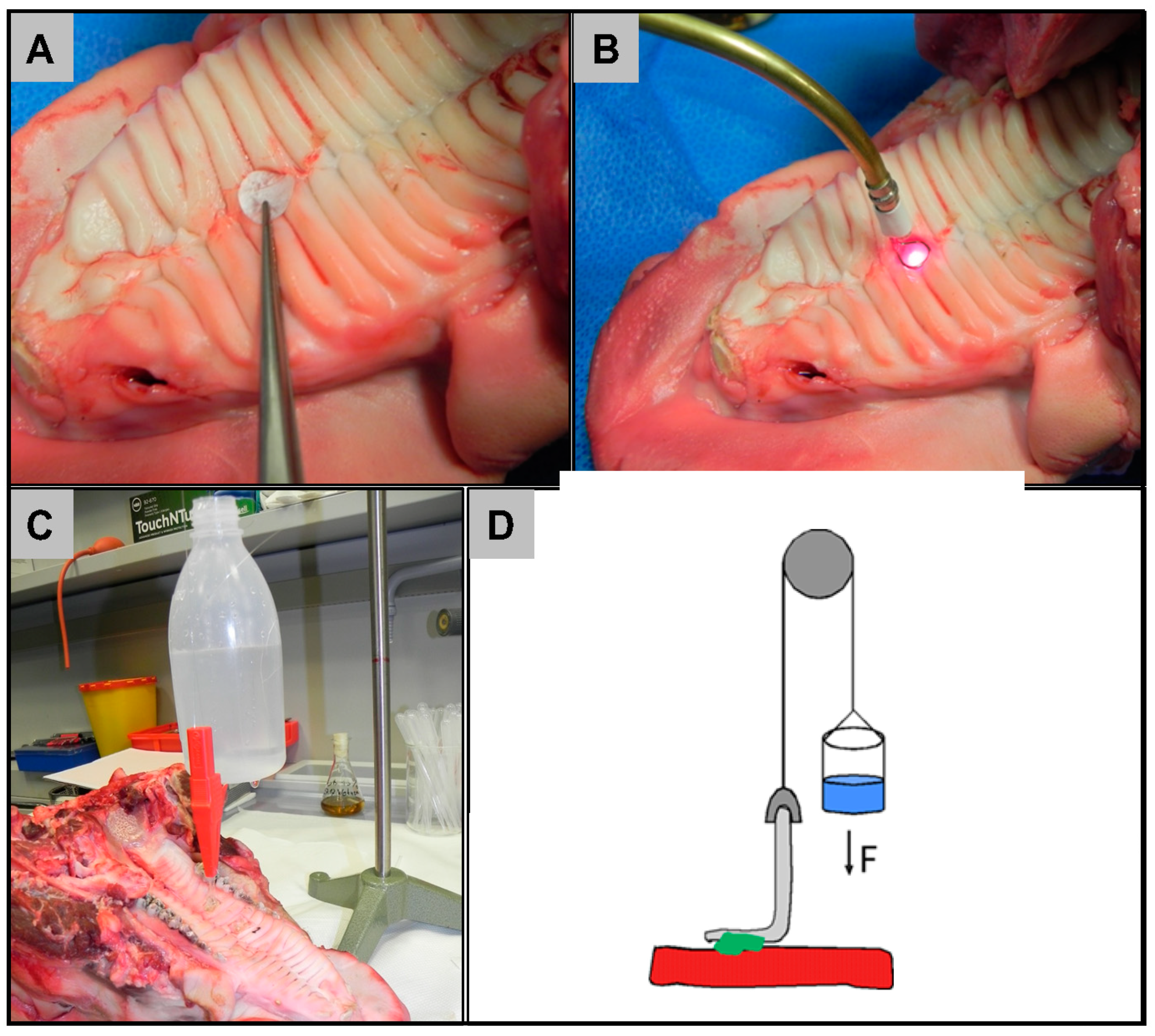
2.2. Ex Vivo Feasibility Test
2.3. In Vitro Cytocompatibility Assessment
3. Discussion
4. Materials and Methods
4.1. Transparent Pericardium-Derived Collagen Membrane
4.2. Bio-Adhesive
4.3. Laser Construction
4.4. Ex Vivo Feasibility Tests
4.5. Cell Culture
4.6. In Vitro Cytocompatibility Assessment
4.7. Reference Materials and Controls for the In Vitro Cytocompatibility Assessment
4.8. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Moloy, P.J. Reconstruction of intermediate sized mucosal defects with the pectoralis major myofascial flap. J. Otolaryngol. 1989, 18, 32–35. [Google Scholar] [PubMed]
- Hao, S.P. Reconstruction of oral defects with the pedicled buccal fat pad flap. Otolaryngol. Head Neck Surg. Off. J. Am. Acad. Otolaryngol. Head Neck Surg. 2000, 122, 863–867. [Google Scholar] [CrossRef]
- Tezel, E. Buccal mucosal flaps: A review. Plast. Reconstr. Surg. 2002, 109, 735–741. [Google Scholar] [CrossRef] [PubMed]
- Markiewicz, M.R.; Lukose, M.A.; Margarone, J.E., 3rd; Barbagli, G.; Miller, K.S.; Chuang, S.K. The oral mucosa graft: A systematic review. J. Urol. 2007, 178, 387–394. [Google Scholar] [CrossRef]
- Sowjanya, N.P.; Rao, N.; Bhushan, N.V.V.S.; Krishnan, G. Versitality of the Use of Collagen Membrane in Oral Cavity. J. Clin. Diagn. Res. 2016, 10, Zc30–Zc33. [Google Scholar] [CrossRef]
- Maiorana, C.; Beretta, M.; Pivetti, L.; Stoffella, E.; Grossi, G.B.; Herford, A.S. Use of a Collagen Matrix as a Substitute for Free Mucosal Grafts in Pre-Prosthetic Surgery: 1 Year Results From a Clinical Prospective Study on 15 Patients. Open Dent. J. 2016, 10, 395–410. [Google Scholar] [CrossRef] [Green Version]
- Gao, Z.R.; Hao, Z.Q.; Li, Y.; Im, M.J.; Spence, R.J. Porcine Dermal Collagen as a Wound Dressing for Skin Donor Sites and Deep Partial Skin Thickness Burns. Burns: J. Int. Soc. Burn Inj. 1992, 18, 492–496. [Google Scholar] [CrossRef]
- Patino, M.G.; Neiders, M.E.; Andreana, S.; Noble, B.; Cohen, R.E. Cellular inflammatory response to porcine collagen membranes. J. Periodontal Res. 2003, 38, 458–464. [Google Scholar] [CrossRef]
- Chattopadhyay, S.; Raines, R.T. Collagen-Based Biomaterials for Wound Healing. Biopolymers 2014, 101, 821–833. [Google Scholar] [CrossRef] [Green Version]
- Griffin, T.J.; Hur, Y.; Bu, J. Basic Suture Techniques for Oral Mucosa. Clin. Adv. Periodontics 2011, 1, 221–232. [Google Scholar] [CrossRef]
- Burkhardt, R.; Lang, N.P. Influence of suturing on wound healing. Periodontology 2000 2015, 68, 270–281. [Google Scholar] [CrossRef] [PubMed]
- McNally, K.; Welch, A.J. Laser Tissue Welding. In Biomedical Photonics Handbook; CRC Press: Boca Raton, FL, USA, 2014; pp. 1043–1087. [Google Scholar]
- Kirsch, A.J.; Canning, D.A.; Zderic, S.A.; Hensle, T.W.; Duckett, J.W. Laser soldering technique for sutureless urethral surgery. Tech. Urol. 1997, 3, 108–113. [Google Scholar]
- Bass, L.S.; Treat, M.R. Laser tissue welding: A comprehensive review of current and future clinical applications. Lasers Surg. Med. 1995, 17, 315–349. [Google Scholar] [CrossRef] [PubMed]
- Norman, G.; Rabi, Y.; Assia, E.; Katzir, A. In vitro conjunctival incision repair by temperature-controlled laser soldering. J. Biomed. Opt. 2009, 14, 064016. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tal, K.; Strassmann, E.; Loya, N.; Ravid, A.; Kariv, N.; Weinberger, D.; Katzir, A.; Gaton, D.D. Corneal cut closure using temperature-controlled CO2 laser soldering system. Lasers Med. Sci. 2015, 30, 1367–1371. [Google Scholar] [CrossRef] [PubMed]
- Noguera, G.; Lee, W.S.; Castro-Combs, J.; Chuck, R.S.; Soltz, B.; Soltz, R.; Behrens, A. Novel laser-activated solder for sealing corneal wounds. Investig. Ophthalmol. Vis. Sci. 2007, 48, 1038–1042. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suh, D.D.; Schwartz, I.P.; Canning, D.A.; Snyder, H.M.; Zderic, S.A.; Kirsch, A.J. Comparison of dermal and epithelial approaches to laser tissue soldering for skin flap closure. Lasers Surg. Med. 1998, 22, 268–274. [Google Scholar] [CrossRef]
- Wider, T.M.; Libutti, S.K.; Greenwald, D.P.; Oz, M.C.; Yager, J.S.; Treat, M.R.; Hugo, N.E. Skin closure with dye-enhanced laser welding and fibrinogen. Plast. Reconstr. Surg. 1991, 88, 1018–1025. [Google Scholar] [CrossRef]
- Kirsch, A.J.; Duckett, J.W.; Snyder, H.M.; Canning, D.A.; Harshaw, D.W.; Howard, P.; Macarak, E.J.; Zderic, S.A. Skin flap closure by dermal laser soldering: A wound healing model for sutureless hypospadias repair. Urology 1997, 50, 263–272. [Google Scholar] [CrossRef]
- Kirsch, A.J.; Chang, D.T.; Kayton, M.L.; Newhouse, J.; Libutti, S.K.; Treat, M.R.; Connor, J.P.; Hensle, T.W. Sutureless rabbit bladder mucosa patch graft urethroplasty using diode laser and solder. J. Urol. 1995, 153, 1303–1307. [Google Scholar] [CrossRef]
- Brosh, T.; Simhon, D.; Halpern, M.; Ravid, A.; Vasilyev, T.; Kariv, N.; Nevo, Z.; Katzir, A. Closure of skin incisions in rabbits by laser soldering II: Tensile strength. Lasers Surg. Med. 2004, 35, 12–17. [Google Scholar] [CrossRef]
- Steinstraesser, L.; Wehner, M.; Trust, G.; Sorkin, M.; Bao, D.; Hirsch, T.; Sudhoff, H.; Daigeler, A.; Stricker, I.; Steinau, H.U.; et al. Laser-mediated fixation of collagen-based scaffolds to dermal wounds. Lasers Surg. Med. 2010, 42, 141–149. [Google Scholar] [CrossRef] [PubMed]
- Lauto, A.; Foster, L.J.R.; Ferris, L.; Avolio, A.; Zwaneveld, N.; Poole-Warren, L.A. Albumin-genipin solder for laser tissue repair. Lasers Surg. Med. 2004, 35, 140–145. [Google Scholar] [CrossRef]
- Poppas, D.P.; Wright, E.J.; Guthrie, P.D.; Shlahet, L.T.; Retik, A.B. Human albumin solders for clinical application during laser tissue welding. Lasers Surg. Med. 1996, 19, 2–8. [Google Scholar] [CrossRef]
- Tabakoglu, H.O.; Gulsoy, M. In vivo comparison of near infrared lasers for skin welding. Lasers Med. Sci. 2010, 25, 411–421. [Google Scholar] [CrossRef]
- Scherr, D.S.; Poppas, D.P. Laser tissue welding. Urol. Clin. N. Am. 1998, 25, 123–135. [Google Scholar] [CrossRef]
- Eyal, O.; Katzir, A. Thermal feedback control techniques for transistor-transistor logic triggered CO2 laser used for irradiation of biological tissue utilizing infrared fiber-optic radiometry. Appl. Opt. 1994, 33, 1751–1754. [Google Scholar] [CrossRef] [PubMed]
- Wehner, M.; Aden, M.; Toedter, N.; Rosenkranz, B. Two-wavelength approach for control of coagulation depth during laser tissue soldering. In Proceedings of the Optical Interactions with Tissue and Cells XXVI, San Francisco, CA, USA, 8–10 February 2015; Volume 9321. [Google Scholar]
- Wehner, M.; Betz, P.; Aden, M. Influence of laser wavelength and beam profile on the coagulation depth in a soft tissue phantom model. Lasers Med. Sci. 2019, 34, 335–341. [Google Scholar] [CrossRef] [Green Version]
- Gueldenpfennig, T.; Houshmand, A.; Najman, S.; Stojanovic, S.; Korzinskas, T.; Smeets, R.; Gosau, M.; Pissarek, J.; Emmert, S.; Jung, O.; et al. The Condensation of Collagen Leads to an Extended Standing Time and a Decreased Pro-inflammatory Tissue Response to a Newly Developed Pericardium-based Barrier Membrane for Guided Bone Regeneration. In Vivo 2020, 34, 985–1000. [Google Scholar] [CrossRef]
- Rastogi, S.; Modi, M.; Sathian, B. The Efficacy of Collagen Membrane as a Biodegradable Wound Dressing Material for Surgical Defects of Oral Mucosa: A Prospective Study. J. Oral Maxil. Surg. 2009, 67, 1600–1606. [Google Scholar] [CrossRef]
- Pal, U.S.; Singh, R.K.; Mohammad, S.; Yadav, R.K. Use of collagen in extraoral wounds. J. Maxill. Oral Surg. 2009, 8, 261–264. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jung, O.; Smeets, R.; Porchetta, D.; Kopp, A.; Ptock, C.; Muller, U.; Heiland, M.; Schwade, M.; Behr, B.; Kroger, N.; et al. Optimized in vitro procedure for assessing the cytocompatibility of magnesium-based biomaterials. Acta Biomater. 2015, 23, 354–363. [Google Scholar] [CrossRef] [PubMed]
- DIN EN ISO 10993-5: Biologische Beurteilung von Medizinprodukten—Teil 5: Prüfungen auf In-Vitro-Zytotoxizität (ISO 10993-5:2009); German Version of EN ISO 10993-5:2009; International Organisation for Standardization, Beuth Verlag: Berlin, Germany, 2019.
- Mathew, A.L.; Pai, K.M.; Sholapurkar, A.A.; Vengal, M. The prevalence of oral mucosal lesions in patients visiting a dental school in Southern India. Indian J. Dent. Res. 2008, 19, 99–103. [Google Scholar] [PubMed]
- Nazir, M.A. Prevalence of periodontal disease, its association with systemic diseases and prevention. Int. J. Health Sci. 2017, 11, 72–80. [Google Scholar]
- Matteini, P.; Ratto, F.; Rossi, F.; de Angelis, M.; Cavigli, L.; Pini, R. Hybrid nanocomposite films for laser-activated tissue bonding. J. Biophotonics 2012, 5, 868–877. [Google Scholar] [CrossRef]
- Esposito, G.; Rossi, F.; Puca, A.; Albanese, A.; Sabatino, G.; Matteini, P.; Lofrese, G.; Maira, G.; Pini, R. An experimental study on minimally occlusive laser-assisted vascular anastomosis in bypass surgery: The importance of temperature monitoring during laser welding procedures. J. Biol. Regul. Homeost. Agents 2010, 24, 307–315. [Google Scholar]
- Matteini, P.; Cicchi, R.; Ratto, F.; Kapsokalyvas, D.; Rossi, F.; de Angelis, M.; Pavone, F.S.; Pini, R. Thermal transitions of fibrillar collagen unveiled by second-harmonic generation microscopy of corneal stroma. Biophys. J. 2012, 103, 1179–1187. [Google Scholar] [CrossRef] [Green Version]
- Isola, G.; Polizzi, A.; Santonocito, S.; Alibrandi, A.; Ferlito, S. Expression of Salivary and Serum Malondialdehyde and Lipid Profile of Patients with Periodontitis and Coronary Heart Disease. Int. J. Mol. Sci. 2019, 20, 6061. [Google Scholar] [CrossRef] [Green Version]
- Isola, G.; Lo Giudice, A.; Polizzi, A.; Alibrandi, A.; Patini, R.; Ferlito, S. Periodontitis and Tooth Loss Have Negative Systemic Impact on Circulating Progenitor Cell Levels: A Clinical Study. Genes 2019, 10, 1022. [Google Scholar] [CrossRef] [Green Version]
- Mishra, M.K. Concise Encyclopedia of Biomedical Polymers and Polymeric Biomaterials; CRC Press: Boca Raton, FL, USA, 2017. [Google Scholar]







© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Birkelbach, M.A.; Smeets, R.; Fiedler, I.; Kluwe, L.; Wehner, M.; Trebst, T.; Hartjen, P. In Vitro Feasibility Analysis of a New Sutureless Wound-Closure System Based on a Temperature-Regulated Laser and a Transparent Collagen Membrane for Laser Tissue Soldering (LTS). Int. J. Mol. Sci. 2020, 21, 7104. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms21197104
Birkelbach MA, Smeets R, Fiedler I, Kluwe L, Wehner M, Trebst T, Hartjen P. In Vitro Feasibility Analysis of a New Sutureless Wound-Closure System Based on a Temperature-Regulated Laser and a Transparent Collagen Membrane for Laser Tissue Soldering (LTS). International Journal of Molecular Sciences. 2020; 21(19):7104. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms21197104
Chicago/Turabian StyleBirkelbach, Moritz Alexander, Ralf Smeets, Imke Fiedler, Lan Kluwe, Martin Wehner, Tilmann Trebst, and Philip Hartjen. 2020. "In Vitro Feasibility Analysis of a New Sutureless Wound-Closure System Based on a Temperature-Regulated Laser and a Transparent Collagen Membrane for Laser Tissue Soldering (LTS)" International Journal of Molecular Sciences 21, no. 19: 7104. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms21197104