Optimizing PSMA Radioligand Therapy for Patients with Metastatic Castration-Resistant Prostate Cancer. A Systematic Review and Meta-Analysis

 , ,
, , 
Abstract
:1. Introduction
2. Results
2.1. Overall Findings
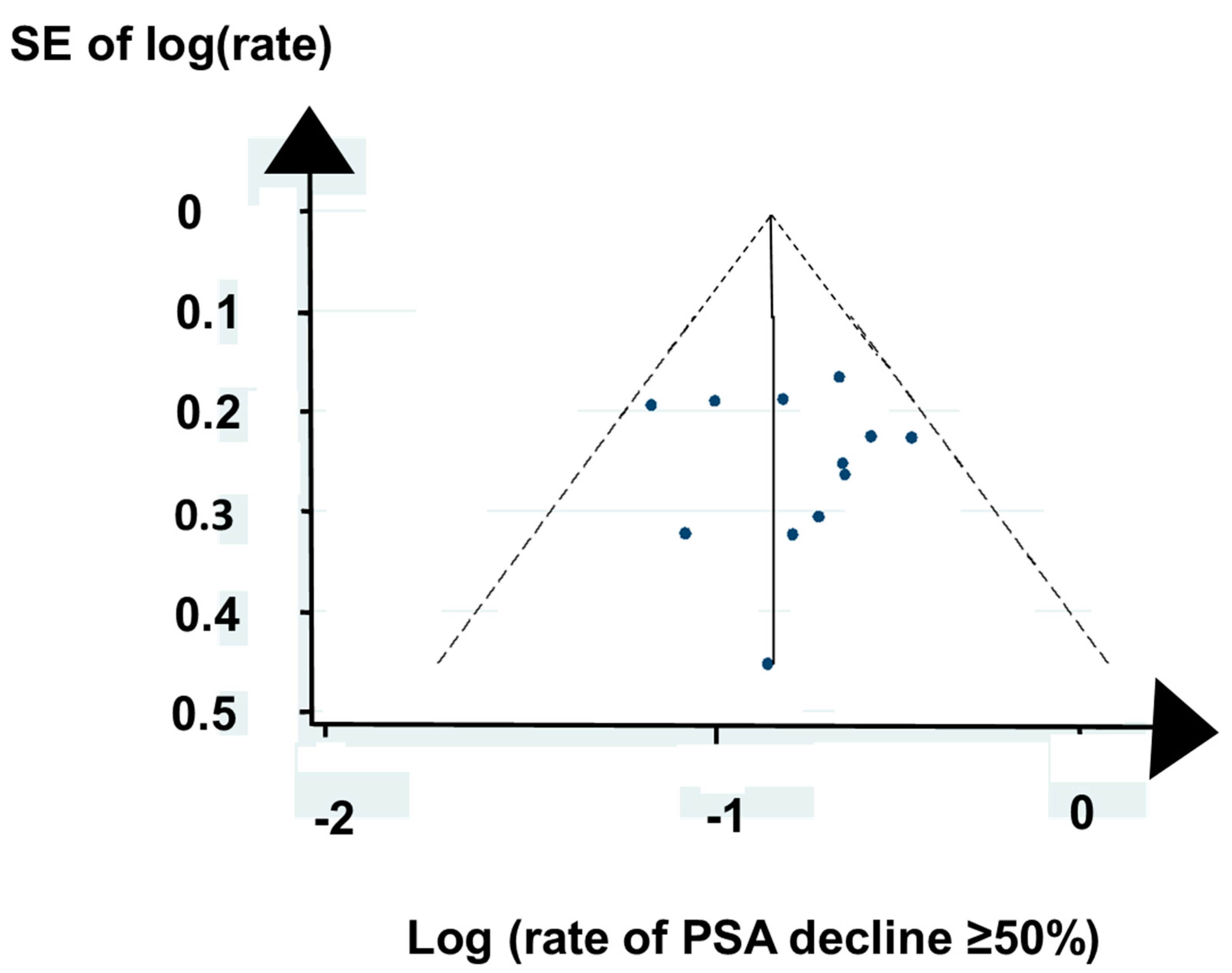
2.2. Bias
2.3. Patients
2.4. Cancer
2.5. Restaging
2.6. Radioligand
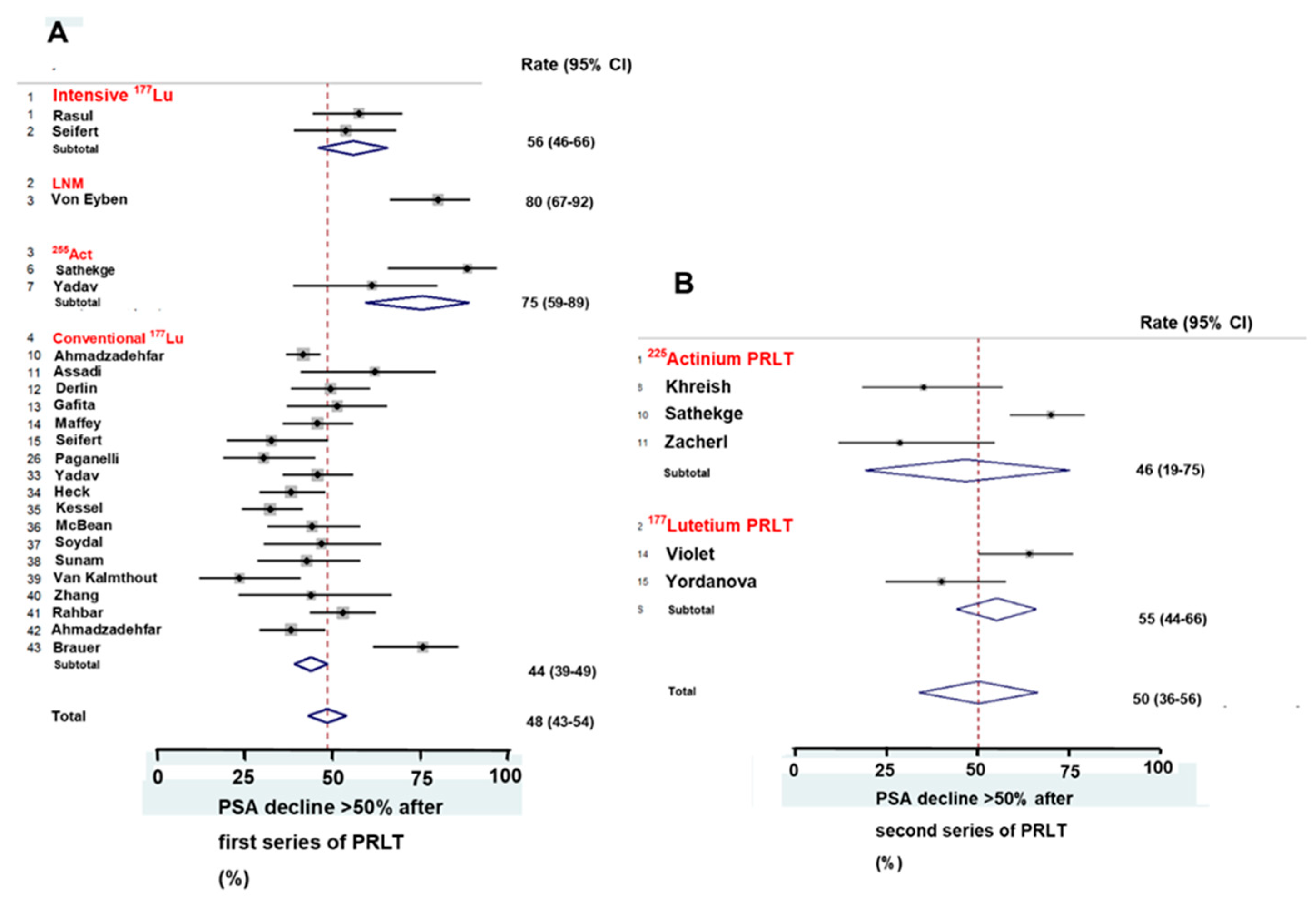
2.7. Response
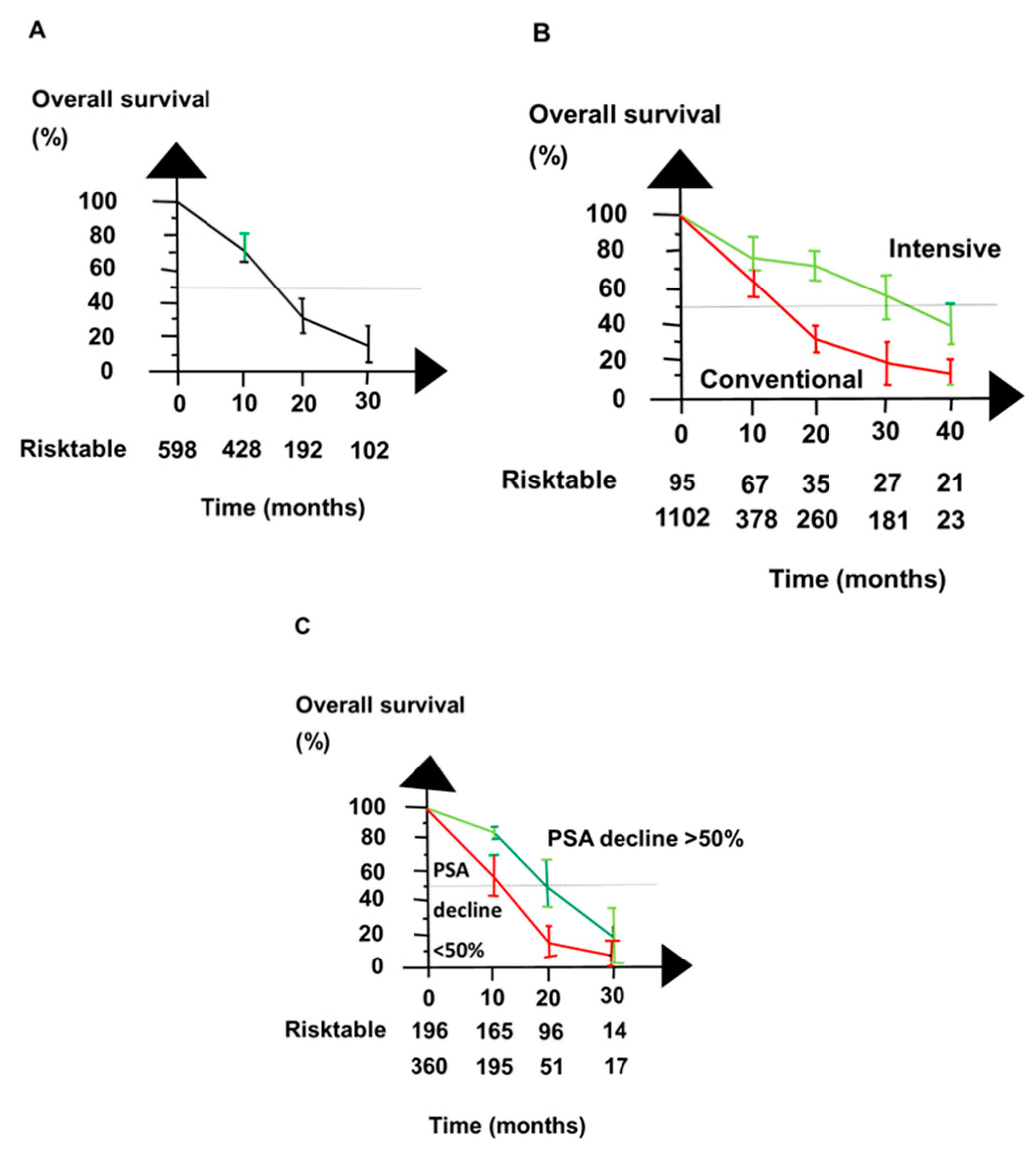
2.8. Survival
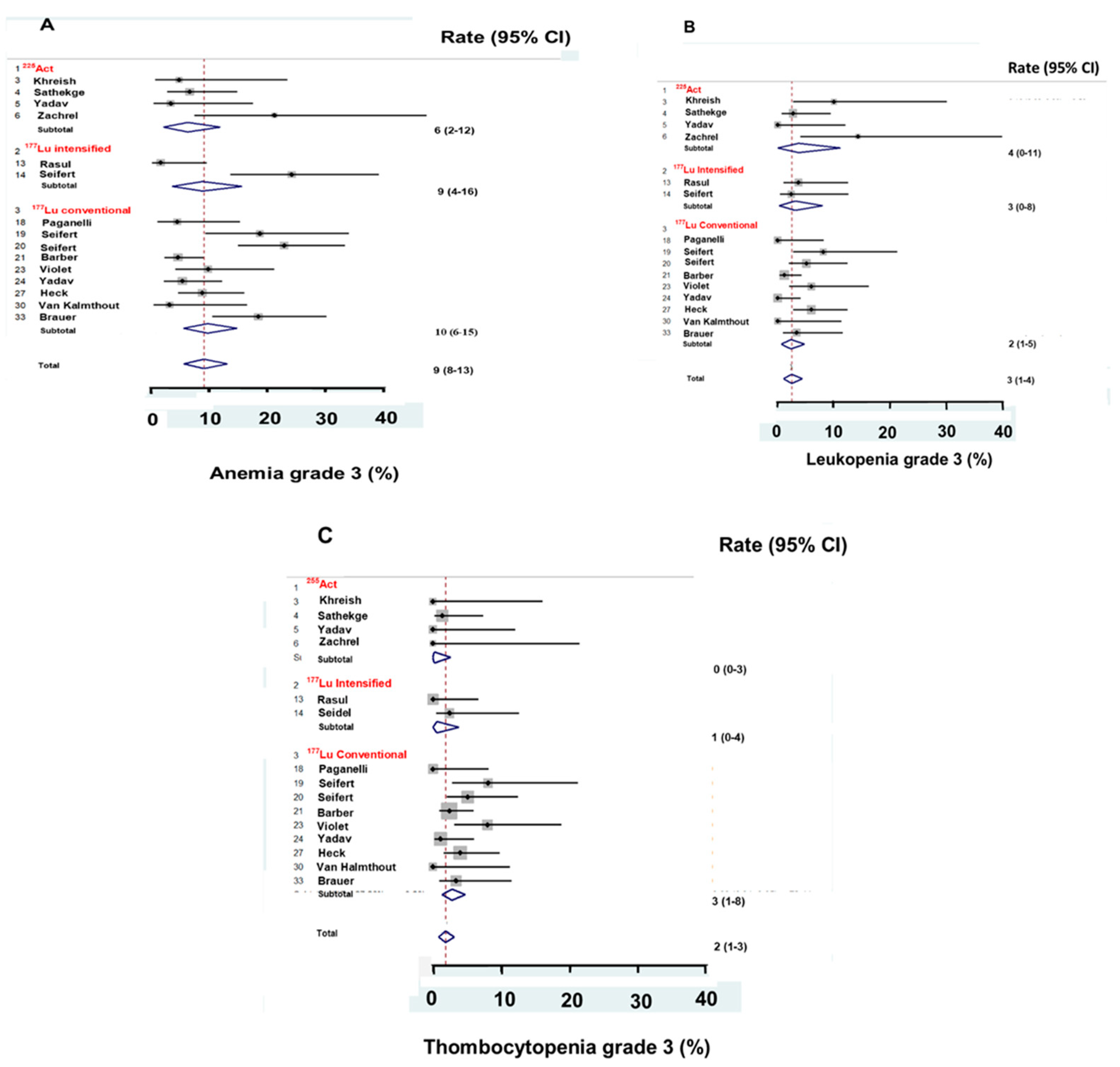
2.9. Adverse Effects
3. Discussion
4. Material and Methods
4.1. Hypothesis
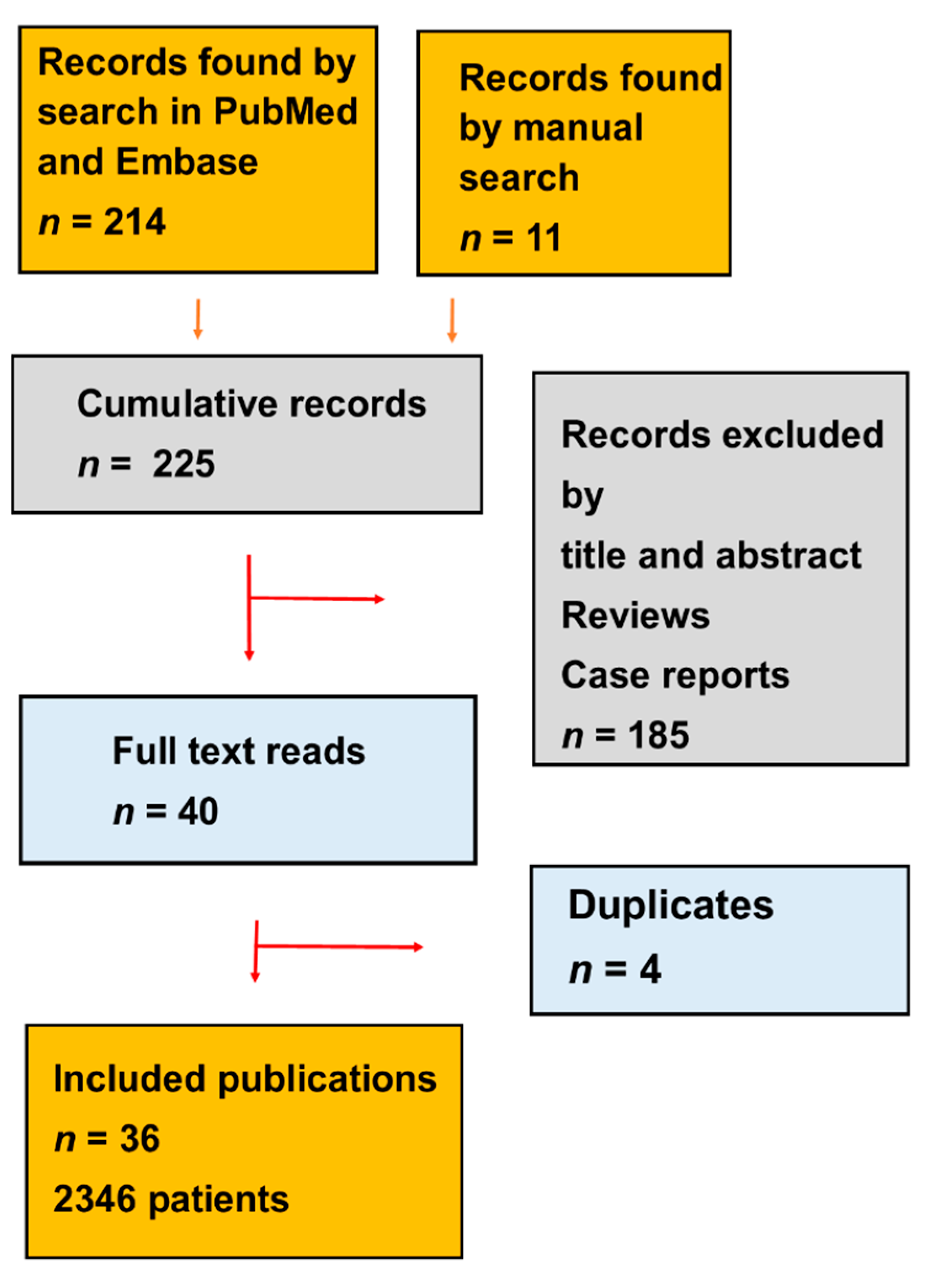
4.2. Search Strategy
4.3. Statistical Analysis
4.4. Ethical Approval
Author Contributions
Funding
Conflicts of Interest
References
- George, D.J.; Sartor, O.; Miller, K.; Saad, F.; Tombal, B.; Kalinovsky, J.; Jiao, X.; Tangirala, K.; Sternberg, C.N.; Higano, C.S. Treatment patterns and outcomes in patients with metastatic castration-resistant prostate cancer in a real-world clinical practice setting in the United States. Clin. Genitourin. Cancer 2020. [Google Scholar] [CrossRef]
- von Eyben, F.E.; Roviello, G.; Kiljunen, T.; Uprimny, C.; Virgolini, I.; Kairemo, K.; Joensuu, T. Third-line treatment and (177)Lu-PSMA radioligand therapy of metastatic castration-resistant prostate cancer: A systematic review. Eur. J. Nucl. Med. Mol. Imaging 2018, 45, 496–508. [Google Scholar] [CrossRef] [Green Version]
- Hofman, M.; Emmett, L.; Sandhu, S.; Iravani, A.; Joshwa, A.; Goh, J.; Patterson, D.; Tan, S.; Kirkwood, S.; Ng, S.; et al. ASCO20. A randomized phase II trial of 177Lu-PSMA 617 (Lu-PSMA) theranostics versus cabazitaxel in metastatic castration-resistant prostate cancer (mCRPC) progressing after docetaxel: Initial results (ANZUP protocol 1603). J. Clin. Oncol. 2020. [Google Scholar] [CrossRef]
- Gillessen, S.; Attard, G.; Beer, T.M.; Beltran, H.; Bjartell, A.; Bossi, A.; Briganti, A.; Bristow, R.G.; Chi, K.N.; Clarke, N.; et al. Management of patients with advanced prostate cancer: Report of the Advanced Prostate Cancer Consensus Conference 2019. Eur. Urol. 2020, 77, 508–547. [Google Scholar]
- von Eyben, F.E.; Kulkarni, H.R.; Baum, R.P. Metastatic extent predicts survival as patients with metastatic castration-resistant prostate cancer are treated with (177)Lu-PSMA radioligand therapy. Theranostics 2020, 10, 4900–4902. [Google Scholar] [CrossRef] [PubMed]
- Ahmadzadehfar, H.; Rahbar, K.; Baum, R.; Seifert, R.; Kalevi, K.; Bogemen, M.; Kulkarni, H.; Zhang, J.; Gerke, C.; Fimmers, R.; et al. Prior therapies as prognostic factors of overall survival in metastatic castration-resistant prostate cancer patients treated with [177 Lu] Lu-PSMA-617. A WARMTH multicenter study (the 617 trial). Eur. J. Nucl. Med. Mol. Imaging 2020. [Google Scholar] [CrossRef] [PubMed]
- Assadi, M.; Rezaei, S.; Jafari, E.; Rekabpour, S.J.; Ravanbod, M.R.; Zohrabi, F.; Amini, A.; Keshmiri, S.; Dadgar, H.; Ahmadzadehfar, H. Potential application of lutetium-177-labeled prostate-specific membrane antigen-617 radioligand therapy for metastatic castration-resistant prostate cancer in a limited resource environment: Initial clinical experience after 2 years. World J. Nucl. Med. 2020, 19, 15–20. [Google Scholar] [CrossRef]
- Derlin, T.; Sommerlath Sohns, J.M.; Schmuck, S.; Henkenberens, C.; von Klot, C.A.J.; Ross, T.L.; Bengel, F.M. Influence of short-term dexamethasone on the efficacy of (177) Lu-PSMA-617 in patients with metastatic castration-resistant prostate cancer. Prostate 2020, 80, 619–631. [Google Scholar] [CrossRef] [Green Version]
- Gafita, A.; Fendler, W.P.; Hui, W.; Sandhu, S.; Weber, M.; Esfandiari, R.; Calais, J.; Rauscher, I.; Rathke, H.; Tauber, R.; et al. Efficacy and safety of (177)Lu-labeled prostate-specific membrane antigen radionuclide treatment in patients with diffuse bone marrow involvement: A multicenter retrospective study. Eur. Urol. 2020, 78, 148–154. [Google Scholar] [CrossRef]
- Khreish, F.; Ebert, N.; Ries, M.; Maus, S.; Rosar, F.; Bohnenberger, H.; Stemler, T.; Saar, M.; Bartholoma, M.; Ezziddin, S. (225)Ac-PSMA-617/(177)Lu-PSMA-617 tandem therapy of metastatic castration-resistant prostate cancer: Pilot experience. Eur. J. Nucl. Med. Mol. Imaging 2020, 47, 721–728. [Google Scholar] [CrossRef]
- Khreish, F.; Kochems, N.; Rosar, F.; Sabet, A.; Ries, M.; Maus, S.; Saar, M.; Bartholoma, M.; Ezziddin, S. Response and outcome of liver metastases in patients with metastatic castration-resistant prostate cancer (mCRPC) undergoing (177)Lu-PSMA-617 radioligand therapy. Eur. J. Nucl. Med. Mol. Imaging 2020. [Google Scholar] [CrossRef]
- Maffey-Steffan, J.; Scarpa, L.; Svirydenka, A.; Nilica, B.; Mair, C.; Buxbaum, S.; Bektic, J.; von Guggenberg, E.; Uprimny, C.; Horninger, W.; et al. The (68)Ga/(177)Lu-theragnostic concept in PSMA-targeting of metastatic castration-resistant prostate cancer: Impact of post-therapeutic whole-body scintigraphy in the follow-up. Eur. J. Nucl. Med. Mol. Imaging 2020, 47, 695–712. [Google Scholar] [CrossRef] [Green Version]
- Paganelli, G.; Sarnelli, A.; Severi, S.; Sansovini, M.; Belli, M.L.; Monti, M.; Foca, F.; Celli, M.; Nicolini, S.; Tardelli, E.; et al. Dosimetry and safety of (177)Lu PSMA-617 along with polyglutamate parotid gland protector: Preliminary results in metastatic castration-resistant prostate cancer patients. Eur. J. Nucl. Med. Mol. Imaging 2020. [Google Scholar] [CrossRef] [PubMed]
- Rasul, S.; Hacker, M.; Kretschmer-Chott, E.; Leisser, A.; Grubmuller, B.; Kramer, G.; Shariat, S.; Wadsak, W.; Mitterhauser, M.; Hartenbach, M.; et al. Clinical outcome of standardized (177)Lu-PSMA-617 therapy in metastatic prostate cancer patients receiving 7400 MBq every 4 weeks. Eur. J. Nucl. Med. Mol. Imaging 2020, 47, 713–720. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rathke, H.; Holland-Letz, T.; Mier, W.; Flechsig, P.; Mavriopoulou, E.; Rohrich, M.; Kopka, K.; Hohenfellner, M.; Giesel, F.L.; Haberkorn, U.; et al. Response prediction of (177)Lu-PSMA-617 radioligand therapy using prostate-specific antigen, chromogranin A, and lactate dehydrogenase. J. Nucl. Med. 2020, 61, 689–695. [Google Scholar] [CrossRef]
- Sathekge, M.; Bruchertseifer, F.; Vorster, M.; Lawal, I.O.; Knoesen, O.; Mahapane, J.; Davis, C.; Reyneke, F.; Maes, A.; Kratochwil, C.; et al. Predictors of overall and disease-free survival in metastatic castration-resistant prostate cancer patients receiving (225)Ac-PSMA-617 radioligand therapy. J. Nucl. Med. 2020, 61, 62–69. [Google Scholar] [CrossRef]
- Seifert, R.; Kessel, K.; Boegemann, M.; Kohler, M.; Roll, W.; Stegger, L.; Weckesser, M.; Rahbar, K. Additional local therapy for liver metastases in patients with metastatic castration-resistant prostate cancer receiving systemic PSMA-targeted therapy. J. Nucl. Med. 2020, 61, 723–728. [Google Scholar] [CrossRef] [PubMed]
- Seifert, R.; Seitzer, K.; Herrmann, K.; Kessel, K.; Schafers, M.; Kleesiek, J.; Weckesser, M.; Boegemann, M.; Rahbar, K. Analysis of PSMA expression and outcome in patients with advanced prostate cancer receiving (177)Lu-PSMA-617 radioligand therapy. Theranostics 2020, 10, 7812–7820. [Google Scholar] [CrossRef] [PubMed]
- Seifert, R.; Kessel, K.; Schlack, K.; Weber, M.; Herrmann, K.; Spanke, M.; Fendler, W.P.; Hadaschik, B.; Kleesiek, J.; Schafers, M.; et al. PSMA PET total tumor volume predicts outcome of patients with advanced prostate cancer receiving [(177)Lu]Lu-PSMA-617 radioligand therapy in a bicentric analysis. Eur. J. Nucl. Med. Mol. Imaging 2020. [Google Scholar] [CrossRef] [PubMed]
- Seifert, R.; Kessel, K.; Schlack, K.; Weckesser, M.; Bogemann, M.; Rahbar, K. Radioligand therapy using [(177)Lu]Lu-PSMA-617 in mCRPC: A pre-VISION single-center analysis. Eur. J. Nucl. Med. Mol. Imaging 2020. [Google Scholar] [CrossRef] [Green Version]
- Violet, J.; Sandhu, S.; Iravani, A.; Ferdinandus, J.; Thang, S.P.; Kong, G.; Kumar, A.R.; Akhurst, T.; Pattison, D.A.; Beaulieu, A.; et al. Long-term follow-up and outcomes of retreatment in an expanded 50-patient single-center phase II prospective trial of (177)Lu-PSMA-617 theranostics in metastatic castration-resistant prostate cancer. J. Nucl. Med. 2020, 61, 857–865. [Google Scholar] [CrossRef] [PubMed]
- Yadav, M.P.; Ballal, S.; Bal, C.; Sahoo, R.K.; Damle, N.A.; Tripathi, M.; Seth, A. Efficacy and safety of 177Lu-PSMA-617 radioligand therapy in metastatic castration-resistant prostate cancer patients. Clin. Nucl. Med. 2020, 45, 19–31. [Google Scholar] [CrossRef] [PubMed]
- Yadav, M.P.; Ballal, S.; Sahoo, R.K.; Tripathi, M.; Seth, A.; Bal, C. Efficacy and safety of (225)Ac-PSMA-617 targeted alpha therapy in metastatic castration-resistant prostate cancer patients. Theranostics 2020, 10, 9364–9377. [Google Scholar] [CrossRef] [PubMed]
- Yordanova, A.; Linden, P.; Hauser, S.; Feldmann, G.; Brossart, P.; Fimmers, R.; Essler, M.; Holdenrieder, S.; Ahmadzadehfar, H. The value of tumor markers in men with metastatic prostate cancer undergoing [(177) Lu]Lu-PSMA therapy. Prostate 2020, 80, 17–27. [Google Scholar] [CrossRef]
- Zacherl, M.J.; Gildehaus, F.J.; Mittlmeier, L.; Boening, G.; Gosewisch, A.; Wenter, V.; Schmidt-Hegemann, N.S.; Belka, C.; Kretschmer, A.; Casuscelli, J.; et al. First clinical results for PSMA targeted alpha therapy using (225)Ac-PSMA-I&T in advanced mCRPC patients. J. Nucl. Med. 2020. [Google Scholar] [CrossRef]
- Aghdam, R.A.; Amoui, M.; Ghodsirad, M.; Khoshbakht, S.; Mofid, B.; Kaghazchi, F.; Tavakoli, M.; Pirayesh, E.; Ahmadzadehfar, H. Efficacy and safety of (177)Lutetium-prostate-specific membrane antigen therapy in metastatic castration-resistant prostate cancer patients: First experience in West Asia—A prospective study. World. J. Nucl. Med. 2019, 18, 258–265. [Google Scholar]
- Barber, T.W.; Singh, A.; Kulkarni, H.R.; Niepsch, K.; Billah, B.; Baum, R.P. Clinical outcomes of (177)Lu-PSMA radioligand therapy in earlier and later phases of metastatic castration-resistant prostate cancer grouped by previous taxane chemotherapy. J. Nucl. Med. 2019, 60, 955–962. [Google Scholar] [CrossRef] [Green Version]
- Grubmuller, B.; Senn, D.; Kramer, G.; Baltzer, P.; D’Andrea, D.; Grubmuller, K.H.; Mitterhauser, M.; Eidherr, H.; Haug, A.R.; Wadsak, W.; et al. Response assessment using (68)Ga-PSMA ligand PET in patients undergoing (177)Lu-PSMA radioligand therapy for metastatic castration-resistant prostate cancer. Eur. J. Nucl. Med. Mol. Imaging 2019, 46, 1063–1072. [Google Scholar] [CrossRef] [Green Version]
- Gupta, M.; Choudhury, P.S.; Rawal, S.; Karthikeyan, G.; Talwar, V.; Dutta, K.D.; Singh, A. Safety profile and therapeutic efficacy of one cycle of Lu177-PSMA in end-stage metastatic castration-resistant prostate cancer patients with low performance status. Nucl. Med. Mol. Imaging 2019, 53, 423–431. [Google Scholar] [CrossRef]
- Heck, M.M.; Tauber, R.; Schwaiger, S.; Retz, M.; D’Alessandria, C.; Maurer, T.; Gafita, A.; Wester, H.J.; Gschwend, J.E.; Weber, W.A.; et al. Treatment outcome, toxicity, and predictive factors for radioligand therapy with (177)Lu-PSMA-I&T in metastatic castration-resistant prostate cancer. Eur. Urol. 2019, 75, 920–926. [Google Scholar]
- Kessel, K.; Seifert, R.; Schafers, M.; Weckesser, M.; Schlack, K.; Boegemann, M.; Rahbar, K. Second line chemotherapy and visceral metastases are associated with poor survival in patients with mCRPC receiving (177)Lu-PSMA-617. Theranostics 2019, 9, 4841–4848. [Google Scholar] [CrossRef] [PubMed]
- McBean, R.; O’Kane, B.; Parsons, R.; Wong, D. Lu177-PSMA therapy for men with advanced prostate cancer: Initial 18 months experience at a single Australian tertiary institution. J. Med. Imaging Radiat. Oncol. 2019. [Google Scholar] [CrossRef] [PubMed]
- Sathekge, M.; Bruchertseifer, F.; Knoesen, O.; Reyneke, F.; Lawal, I.; Lengana, T.; Davis, C.; Mahapane, J.; Corbett, C.; Vorster, M.; et al. (225)Ac-PSMA-617 in chemotherapy-naive patients with advanced prostate cancer: A pilot study. Eur. J. Nucl. Med. Mol. Imaging 2019, 46, 129–138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soydal, C.; Araz, M.; Urun, Y.; Nak, D.; Ozkan, E.; Kucuk, N.O. Prognostic importance of PSA response in patients who received Lutetium-177 PSMA treatment for castration resistant prostate cancer. Q. J. Nucl. Med. Mol. Imaging 2019. [Google Scholar] [CrossRef]
- Suman, S.; Parghane, R.V.; Joshi, A.; Prabhash, K.; Bakshi, G.; Talole, S.; Banerjee, S.; Basu, S. Therapeutic efficacy, prognostic variables and clinical outcome of (177)Lu-PSMA-617 PRLT in progressive mCRPC following multiple lines of treatment: Prognostic implications of high FDG uptake on dual tracer PET-CT vis-a-vis Gleason score in such cohort. Br. J. Radiol. 2019, 92, 20190380. [Google Scholar] [CrossRef]
- van Kalmthout, L.; Braat, A.; Lam, M.; van Leeuwaarde, R.; Krijger, G.; Ververs, T.; Mehra, N.; Bins, A.; Hunting, J.; de Keizer, B. First experience with 177Lu-PSMA-617 therapy for advanced prostate cancer in the Netherlands. Clin. Nucl. Med. 2019, 44, 446–451. [Google Scholar] [CrossRef]
- von Eyben, F.E.; Singh, A.; Zhang, J.; Nipsch, K.; Meyrick, D.; Lenzo, N.; Kairemo, K.; Joensuu, T.; Virgolini, I.; Soydal, C.; et al. (177)Lu-PSMA radioligand therapy of predominant lymph node metastatic prostate cancer. Oncotarget 2019, 10, 2451–2461. [Google Scholar] [CrossRef]
- Yordanova, A.; Linden, P.; Hauser, S.; Meisenheimer, M.; Kurpig, S.; Feldmann, G.; Gaertner, F.C.; Essler, M.; Ahmadzadehfar, H. Outcome and safety of rechallenge [(177)Lu]Lu-PSMA-617 in patients with metastatic prostate cancer. Eur. J. Nucl. Med. Mol. Imaging 2019, 46, 1073–1080. [Google Scholar] [CrossRef]
- Zhang, J.; Kulkarni, H.R.; Singh, A.; Schuchardt, C.; Niepsch, K.; Langbein, T.; Baum, R.P. (177)Lu-PSMA-617 radioligand therapy in metastatic castration-resistant prostate cancer patients with a single functioning kidney. J. Nucl. Med. 2019, 60, 1579–1586. [Google Scholar] [CrossRef]
- Kesavan, M.; Turner, J.H.; Meyrick, D.; Yeo, S.; Cardaci, G.; Lenzo, N.P. Salvage radiopeptide therapy of advanced castrate-resistant prostate cancer with Lutetium-177-labeled prostate-specific membrane antigen: Efficacy and safety in routine practice. Cancer Biother. Radiopharm. 2018, 33, 274–281. [Google Scholar] [CrossRef]
- Rahbar, K.; Boegemann, M.; Yordanova, A.; Eveslage, M.; Schafers, M.; Essler, M.; Ahmadzadehfar, H. PSMA targeted radioligandtherapy in metastatic castration resistant prostate cancer after chemotherapy, abiraterone and/or enzalutamide. A retrospective analysis of overall survival. Eur. J. Nucl. Med. Mol. Imaging 2018, 45, 12–19. [Google Scholar] [CrossRef] [PubMed]
- Ahmadzadehfar, H.; Schlolaut, S.; Fimmers, R.; Yordanova, A.; Hirzebruch, S.; Schlenkhoff, C.; Gaertner, F.C.; Awang, Z.H.; Hauser, S.; Essler, M. Predictors of overall survival in metastatic castration-resistant prostate cancer patients receiving [(177)Lu]Lu-PSMA-617 radioligand therapy. Oncotarget 2017, 8, 103108–103116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brauer, A.; Grubert, L.S.; Roll, W.; Schrader, A.J.; Schafers, M.; Bogemann, M.; Rahbar, K. 177Lu-PSMA-617 radioligand therapy and outcome in patients with metastasized castration-resistant prostate cancer. Eur. J. Nucl. Med. Mol. Imaging 2017, 44, 1663–1670. [Google Scholar] [CrossRef] [PubMed]
- Hofman, M.S.; Emmett, L.; Violet, J.; Lawrence, N.J.; Stockler, M.; Francis, R.J.; Iravani, A.; Williams, S.; Azad, A.; Martin, A.; et al. TheraP: A randomized phase 2 trial of (177) Lu-PSMA-617 theranostic treatment vs cabazitaxel in progressive metastatic castration-resistant prostate cancer (Clinical Trial Protocol ANZUP 1603). BJU Int. 2019, 124 (Suppl. 1), 5–13. [Google Scholar] [CrossRef] [Green Version]
- Satapathy, S.; Mittal, B.R.; Sood, A. Visceral metastases as predictors of response and survival outcomes in patients of castration-resistant prostate cancer treated with 177Lu-labeled prostate-specific membrane a antigen radioligand therapy: A systematic review and meta-analysis. Clin. Nucl. Med. 2020. [Google Scholar] [CrossRef]
- Scher, H.I.; Morris, M.J.; Stadler, W.M.; Higano, C.; Basch, E.; Fizazi, K.; Antonarakis, E.S.; Beer, T.M.; Carducci, M.A.; Chi, K.N.; et al. Trial design and objectives for castration-resistant prostate cancer: Updated recommendations from the Prostate Cancer Clinical Trials Working Group 3. J. Clin. Oncol. 2016, 34, 1402–1418. [Google Scholar] [CrossRef] [Green Version]
- Kratochwil, C.; Fendler, W.P.; Eiber, M.; Baum, R.; Bozkurt, M.F.; Czernin, J.; Delgado Bolton, R.C.; Ezziddin, S.; Forrer, F.; Hicks, R.J.; et al. EANM procedure guidelines for radionuclide therapy with (177)Lu-labelled PSMA-ligands ((177)Lu-PSMA-RLT). Eur. J. Nucl. Med. Mol. Imaging 2019, 46, 2536–2544. [Google Scholar] [CrossRef]
- von Eyben, F.E.; Picchio, M.; von Eyben, R.; Rhee, H.; Bauman, G. (68)Ga-labeled prostate-specific membrane antigen ligand positron emission tomography/computed tomography for prostate cancer: A systematic review and meta-analysis. Eur. Urol. Focus 2018, 4, 686–693. [Google Scholar] [CrossRef] [Green Version]
- Perera, M.; Papa, N.; Roberts, M.; Williams, M.; Udovicich, C.; Vela, I.; Christidis, D.; Bolton, D.; Hofman, M.S.; Lawrentschuk, N.; et al. Gallium-68 prostate-specificmMembrane antigen positron emission tomography in advanced prostate cancer-Updated diagnostic utility, sensitivity, specificity, and distribution of prostate-specific membrane antigen-avid lesions: A systematic review and meta-analysis. Eur. Urol. 2020, 77, 403–417. [Google Scholar]
- Violet, J.; Jackson, P.; Ferdinandus, J.; Sandhu, S.; Akhurst, T.; Iravani, A.; Kong, G.; Kumar, A.R.; Thang, S.P.; Eu, P.; et al. Dosimetry of (177)Lu-PSMA-617 in metastatic castration-resistant prostate cancer: Correlations between pretherapeutic imaging and whole-body tumor dosimetry with treatment outcomes. J. Nucl. Med. 2019, 60, 517–523. [Google Scholar] [CrossRef] [Green Version]
- Hofman, M.S.; Lawrentschuk, N.; Francis, R.J.; Tang, C.; Vela, I.; Thomas, P.; Rutherford, N.; Martin, J.M.; Frydenberg, M.; Shakher, R.; et al. Prostate-specific membrane antigen PET-CT in patients with high-risk prostate cancer before curative-intent surgery or radiotherapy (proPSMA): A prospective, randomised, multicentre study. Lancet 2020, 395, 1208–1216. [Google Scholar] [CrossRef]
- Thang, S.P.; Violet, J.; Sandhu, S.; Iravani, A.; Akhurst, T.; Kong, G.; Ravi Kumar, A.; Murphy, D.G.; Williams, S.G.; Hicks, R.J.; et al. Poor outcomes for patients with metastatic castration-resistant prostate cancer with low prostate-specific membrane antigen (PSMA) expression deemed ineligible for (177)Lu-labelled PSMA radioligand therapy. Eur. Urol. Oncol. 2019, 2, 670–676. [Google Scholar] [CrossRef] [PubMed]
- Adnan, A.; Basu, S. Comparison of dual-tracer PET and CT features to conventional risk categories in assessing response to (177)Lu-PSMA-617 therapy for metastatic prostate adenocarcinoma with urinary bladder involvement. J. Nucl. Med. Technol. 2020, 48, 148–153. [Google Scholar] [CrossRef] [PubMed]
- Kratochwil, C.; Bruchertseifer, F.; Giesel, F.L.; Weis, M.; Verburg, F.A.; Mottaghy, F.; Kopka, K.; Apostolidis, C.; Haberkorn, U.; Morgenstern, A. 225Ac-PSMA-617 for PSMA-targeted alpha-radiation therapy of metastatic castration-resistant prostate cancer. J. Nucl. Med. 2016, 57, 1941–1944. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rathke, H.; Giesel, F.L.; Flechsig, P.; Kopka, K.; Mier, W.; Hohenfellner, M.; Haberkorn, U.; Kratochwil, C. Repeated (177)Lu-labeled PSMA-617 radioligand therapy using treatment activities of up to 9.3 GBq. J. Nucl. Med. 2018, 59, 459–465. [Google Scholar] [CrossRef] [Green Version]
- Iacovelli, R.; Ciccarese, C.; Bria, E.; Romano, M.; Fantinel, E.; Bimbatti, D.; Muraglia, A.; Porcaro, A.B.; Siracusano, S.; Brunelli, M.; et al. The cardiovascular toxicity of abiraterone and enzalutamide in prostate cancer. Clin. Genitourin. Cancer 2018, 16, e645–e653. [Google Scholar] [CrossRef]
- Scher, H.I.; Fizazi, K.; Saad, F.; Taplin, M.E.; Sternberg, C.N.; Miller, K.; de Wit, R.; Mulders, P.; Chi, K.N.; Shore, N.D.; et al. Increased survival with enzalutamide in prostate cancer after chemotherapy. N. Engl. J. Med. 2012, 367, 1187–1197. [Google Scholar] [CrossRef] [Green Version]
- Zippel, C.; Ronski, S.C.; Bohnet-Joschko, S.; Giesel, F.L.; Kopka, K. Current status of PSMA-radiotracers for prostate cancer: Data analysis of prospective trials listed on ClinicalTrials.gov. Pharmaceuticals (Basel) 2020, 13. [Google Scholar] [CrossRef] [Green Version]
- Jones, W.; Griffiths, K.; Barata, P.C.; Paller, C.J. PSMA theranostics: Review of the current status of PSMA-targeted imaging and radioligand therapy. Cancers (Basel) 2020, 12. [Google Scholar] [CrossRef]
- Mayor, N.; Sathianathen, N.J.; Buteau, J.; Koschel, S.; Anton Juanilla, M.; Kapoor, J.; Azad, A.; Hofman, M.S.; Murphy, D.G. Prostate-specific membrane antigen theranostics in advanced prostate cancer: An evolving option. BJU Int. 2020. [Google Scholar] [CrossRef]
- Rahbar, K.; Bodei, L.; Morris, M.J. Is the vision of radioligand therapy for prostate cancer becoming a reality? An overview of the phase III VISION trial and its importance for the future of theranostics. J. Nucl. Med. 2019, 60, 1504–1506. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prive, B.M.; Janssen, M.J.R.; van Oort, I.M.; Muselaers, C.H.J.; Jonker, M.A.; de Groot, M.; Mehra, N.; Verzijlbergen, J.F.; Scheenen, T.W.J.; Zamecnik, P.; et al. Lutetium-177-PSMA-I&T as metastases directed therapy in oligometastatic hormone sensitive prostate cancer, a randomized controlled trial. BMC Cancer 2020, 20, 884. [Google Scholar]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gotzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. Ann. Intern. Med. 2009, 151, W65–W94. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parmar, M.K.; Torri, V.; Stewart, L. Extracting summary statistics to perform meta-analyses of the published literature for survival endpoints. Stat. Med. 1998, 17, 2815–2834. [Google Scholar] [CrossRef]
- Tobias, V. Meta-analysis of p values. Stata Techn. Bull. 1999, 49, 15–17. [Google Scholar]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| (A) | |||||||
| Author | No of Patients | Patient Characteristics | |||||
| Median age (years) | Sites of metastases | ||||||
| LN | Bones | Lungs | Liver | Other | |||
| Ahmadzadehfar [6] | 416 | 72 | 30 | 221 | 69 | 87 | 10 |
| Assadi [7] | 25 | 70 | NR | NR | NR | NR | NR |
| Derlin [8] | 71 | 72 | 24 | 39 | 3 | 9 | 0 |
| Gafita [9] | 43 | 72 | 0 | 33 | 5 | 5 | 0 |
| Khreish [10] | 20 | 72 | 0 | 14 | 2 | 2 | 0 |
| Khreish [11] | 28 | NR | 0 | 0 | 0 | 28 | 0 |
| Maffey [12] | 32 | NR | 5 | 24 | 1 | 2 | 0 |
| Paganelli [13] | 43 | 73 | 1 | 28 | 7 | 7 | 0 |
| Rasul [14] | 54 | 72 | 8 | 37 | 4 | 5 | 0 |
| Rathke [15] | 100 | 70 | 0 | 65 | 12 | 11 | 0 |
| Sathekge [16] | 73 | 69 | 7 | 60 | 2 | 4 | 0 |
| Seifert [17] | 31 | 73 | 0 | 0 | 0 | 31 | 0 |
| Seifert [20] | 78 | 71 | 0 | 46 | 14 | 18 | 0 |
| Violet [21] | 50 | 71 | 2 | 38 | 5 | 5 | 0 |
| Yadav [22] | 90 | 70 | 1 | 78 | 3 | 3 | 5 |
| Yadav [23] | 28 | 1 | 21 | 3 | 3 | 0 | |
| Yordanova [24] | 137 | 71 | 4 | 81 | 28 | 24 | 0 |
| Zacherl [25] | 14 | 75 | 0 | 10 | 3 | 1 | 1 |
| Aghdam [26] | 14 | 70 | 0 | 11 | 0 | 1 | 2 |
| Barber [27] | 167 | 70 | 19 | 102 | 18 | 18 | 10 |
| Grubmuller [28] | 38 | 72 | 8 | 24 | 3 | 3 | 0 |
| Gupta [29] | 22 | NR | NR | NR | NR | NR | |
| Heck [30] | 100 | 72 | 3 | 62 | 17 | 18 | 0 |
| Kessel [31] | 54 | 72 | 0 | 51 | 24 | 24 | 0 |
| McBean [32] | 50 | 0 | 41 | 4 | 5 | 0 | |
| Sathekge [33] | 17 | 65 | 3 | 12 | 1 | 0 | 1 |
| Soydal [34] | 30 | 68 | NR | NR | NR | NR | NR |
| Suman [35] | 40 | 63 | 8 | 23 | 0 | 9 | 0 |
| Van Kalmthout [36] | 30 | 70 | NR | NR | NR | NR | NR |
| Von Eyben [37] | 45 | 61 | 45 | 0 | 0 | 0 | 0 |
| Yordanova [38] | 30 | 72 | 0 | 23 | 4 | 3 | 0 |
| Zhang [39] | 16 | 65 | 2 | 11 | 1 | 1 | 0 |
| Kesavan [40] | 22 | 2 | 12 | 1 | 2 | 0 | |
| Rahbar [41] | 104 | 70 | 0 | 70 | 18 | 16 | 0 |
| Ahmadzadehfar [42] | 100 | NR | 0 | 66 | 18 | 16 | 0 |
| Brauer [43] | 59 | 72 | 0 | 30 | 9 | 20 | 0 |
| Tot no patients | 2346 | 176 | 1342 | 286 | 399 | 40 | |
| Percentage | 8 | 60 | 12 | 18 | 2 | ||
| (B) | |||||||
| Author | Characteristics of Patients | Radioligand Therapy | Outcomes | ||||
| Median PSA (ng/mL) | Dose per cycle (GBq) | Interval between cycles (weeks) | PSA decline > 50% (%) | Median OS (months) | |||
| Ahmadzadehfar [6] | 215 | 6.9 | NR | NR | 11.1 | ||
| Assadi [7] | 135 | 3.7–7.4 | NR | 62 | 15.5 | ||
| Derlin [8] | 385 | 6–7.4 | 6–8 | 48 | NR | ||
| Gafita [9] | 1000 | NR | NR | 22 | 11.6 | ||
| Khreish [10] | 215 | 6.9 | NR | 65 | 12 | ||
| Khreish [11] | 539 | 6.5 | 6 | 57 | 12 | ||
| Maffey [12] | NR | 6 | 6–10 | 50 | 12 | ||
| Paganelli [13] | 56.5 | 3.7–5.5 | 10 | 31 | NR | ||
| Rasul [14] | 72 | 7.4 | 4 | 58 | 28 | ||
| Rathke [15] | 59 | NR | 8 | 35 | NR | ||
| Sathekge [16] | 57 | 6 | 8 | 70 | 18 | ||
| Seifert [17] | 363 | 7.5 | |||||
| Seifert [20] | NR | 6/7.5 | 7.5 | 44 | 12 | ||
| Violet [21] | 190 | 7.5 | 8 | 64 | 13.3 | ||
| Yadav [22] | 333 | 7.8–8.7 | NR | 45.5 | 14 | ||
| Yadav [23] | 221 | NR | NR | 39 | 17 | ||
| Yordanova [24] | 208 | 6.2 | 7.5 | NR | 17 | ||
| Zacherl [25] | 112 | 7.8 MBq | 8 | 50 | NR | ||
| Aghdam [26] | 95 | 5.7 | NR | 45.4 | NR | ||
| Barber [27] | 120 | 6.3 | NR | 48 | 18 | ||
| Grubmuller [28] | 61 | 7.4 | 4 | 47.4 | 24 | ||
| Gupta [29] | 143 | 7.4 | NR | 22.7 | NR | ||
| Heck [30] | 165 | 7.4 | 6–10 | 38 | 12 | ||
| Kessel [31] | 294 | 6.2 | 25 | 9.9 | |||
| McBean [32] | 137 | 5.9 | NR | 45 | NR | ||
| Sathekge [33] | NR | 7.5 (MBq) | 88 | NR | |||
| Soydal [34] | 260 | 6 | 6–8 | 33 | 12 | ||
| Suman [35] | NR | 4.4–5.6 | 10–12 | 42.5 | 12 | ||
| Van Kalmthout [36] | 200 | 6 | 6 | 57 | 11.3 | ||
| Von Eyben [37] | 23 | 4.6 | 8 | 80 | >30 | ||
| Yordanova [38] | 208 | 6.1 | NR | 40 | 12 | ||
| Zhang [39] | 60 | 6.4 | 8 | 44 | 15 | ||
| Kesavan [40] | 20.5 | 5.5 | 8 | 40 | NR | ||
| Rahbar [41] | 361 | 6.1 | 8 | 33 | 14 | ||
| Ahmadzadehfar [42] | 206 | NS | 8 | 38 | 15 | ||
| Brauer [43] | NS | 6.1 | NR | 53 | 8 | ||
| Clinical Characteristic | Publications | Number of Patients | Meta-Analytic p Values | |
|---|---|---|---|---|
| Patients | Previous chemotherapy | [6,25,27,34] | 321 | 2.8 × 10−6 |
| Performance status | [4,6] | 536 | 1.4 × 10−6 | |
| Cancer | Site of metastases | [5,27] | 343 | 7.1 × 10−5 |
| Serum alkaline phosphatase | [38,41,43] | 4.1 × 10−4 | ||
| PRLT | Second series of PRLT | [37,38] | 75 | 4.5 × 10−4 |
| Response | PSA decline ≥ 50% | [4,30,31,34,41,42] | 480 | 1.5 × 10−10 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
von Eyben, F.E.; Bauman, G.; von Eyben, R.; Rahbar, K.; Soydal, C.; Haug, A.R.; Virgolini, I.; Kulkarni, H.; Baum, R.; Paganelli, G. Optimizing PSMA Radioligand Therapy for Patients with Metastatic Castration-Resistant Prostate Cancer. A Systematic Review and Meta-Analysis. Int. J. Mol. Sci. 2020, 21, 9054. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms21239054
von Eyben FE, Bauman G, von Eyben R, Rahbar K, Soydal C, Haug AR, Virgolini I, Kulkarni H, Baum R, Paganelli G. Optimizing PSMA Radioligand Therapy for Patients with Metastatic Castration-Resistant Prostate Cancer. A Systematic Review and Meta-Analysis. International Journal of Molecular Sciences. 2020; 21(23):9054. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms21239054
Chicago/Turabian Stylevon Eyben, Finn Edler, Glenn Bauman, Rie von Eyben, Kambiz Rahbar, Cigdem Soydal, Alexander R. Haug, Irene Virgolini, Harshad Kulkarni, Richard Baum, and Giovanni Paganelli. 2020. "Optimizing PSMA Radioligand Therapy for Patients with Metastatic Castration-Resistant Prostate Cancer. A Systematic Review and Meta-Analysis" International Journal of Molecular Sciences 21, no. 23: 9054. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms21239054