Advances in the Knowledge of the Underlying Airway Remodeling Mechanisms in Chronic Rhinosinusitis Based on the Endotypes: A Review


Abstract
:1. Introduction
2. Current Perceptions in CRS Classification
2.1. Type 2 Chronic Rhinosinusitis
2.2. Non-Type 2 Chronic Rhinosinusitis
3. Tissue Remodeling
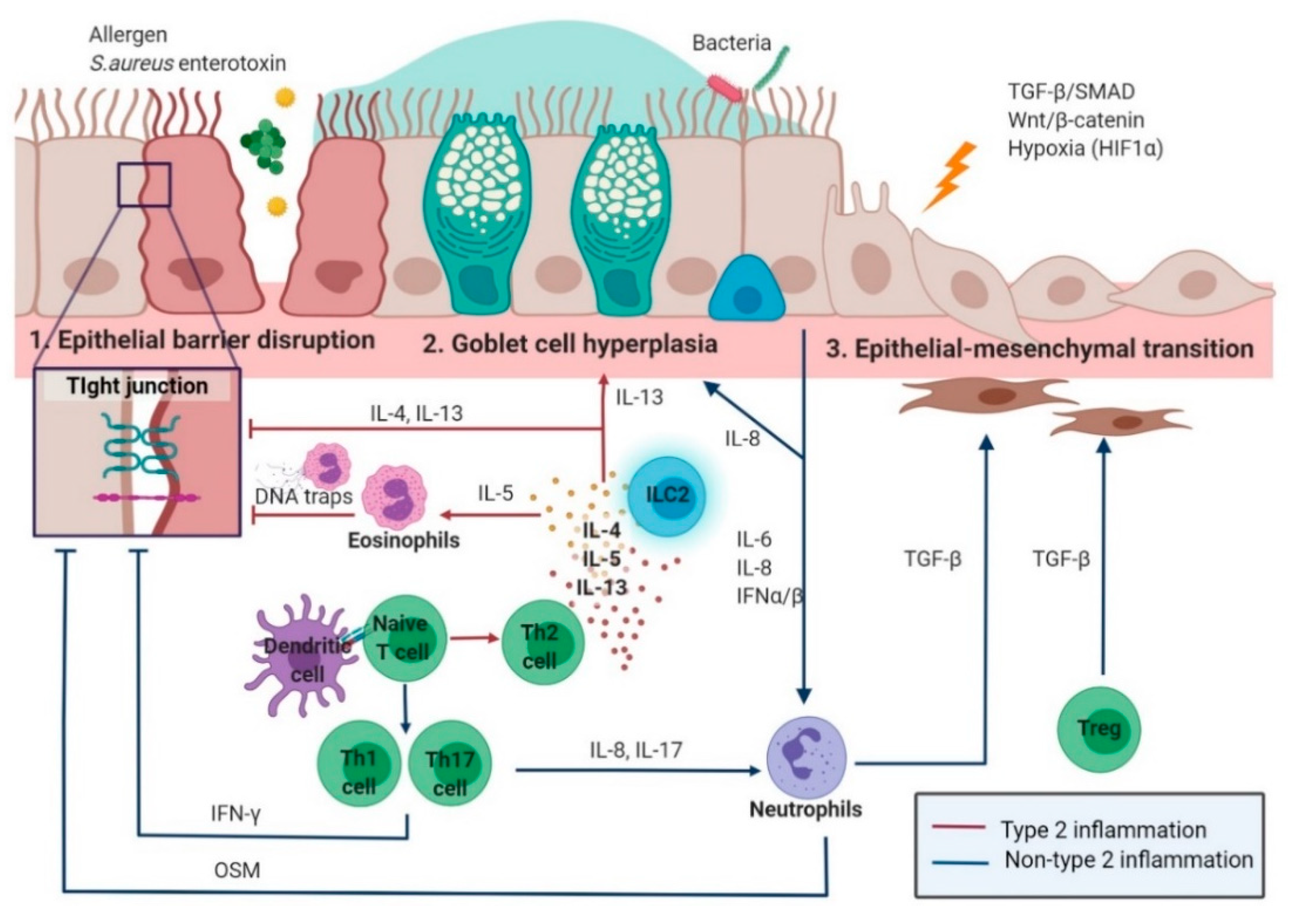
3.1. Epithelial Remodeling
3.1.1. Type 2 Inflammation in Epithelial Remodeling
3.1.2. Non-Type 2 Inflammation in Epithelial Remodeling
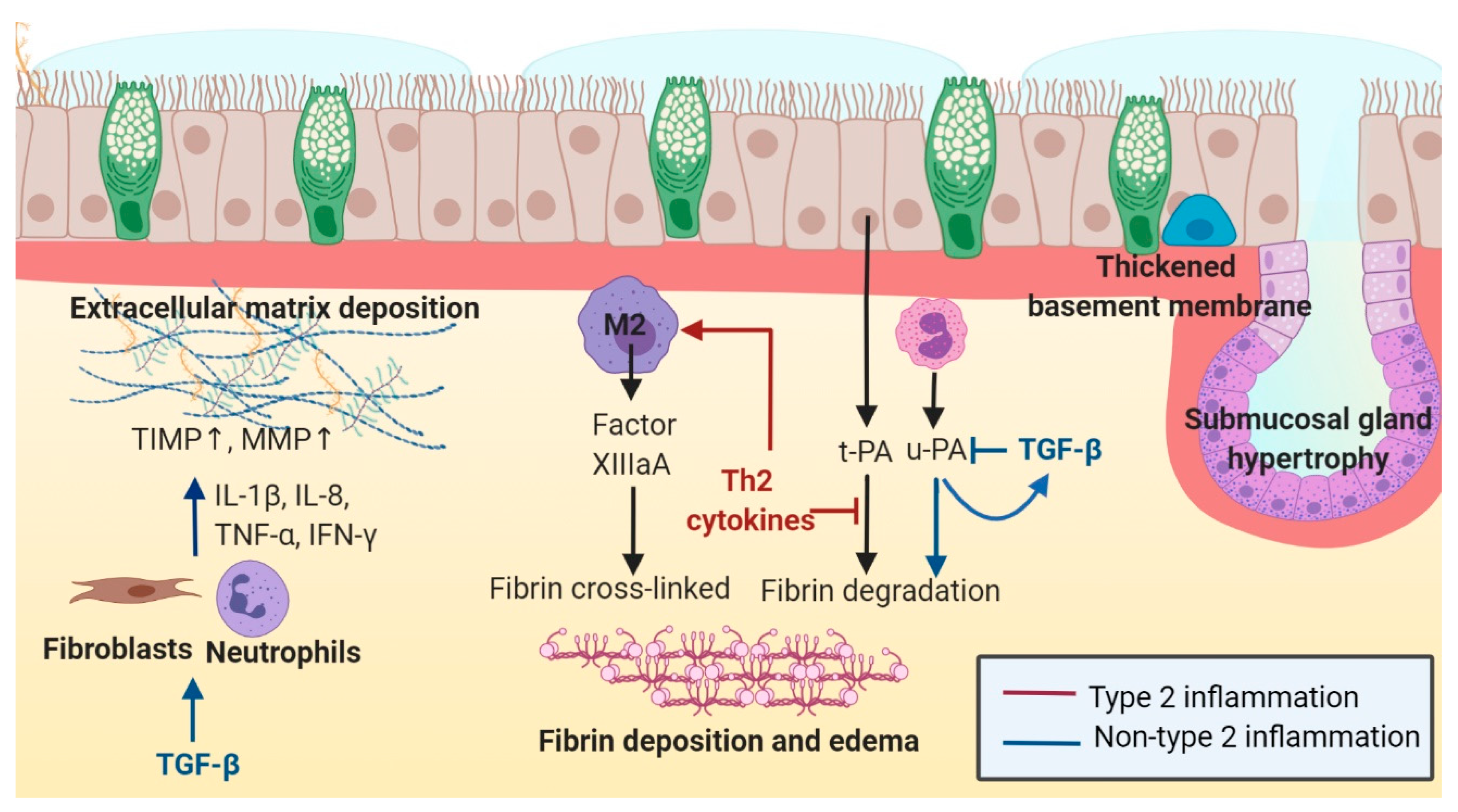
3.2. Subepithelial Remodeling
3.2.1. Type 2 Inflammation in Subepithelial Remodeling
3.2.2. Non-Type 2 Inflammation in Subepithelial Remodeling
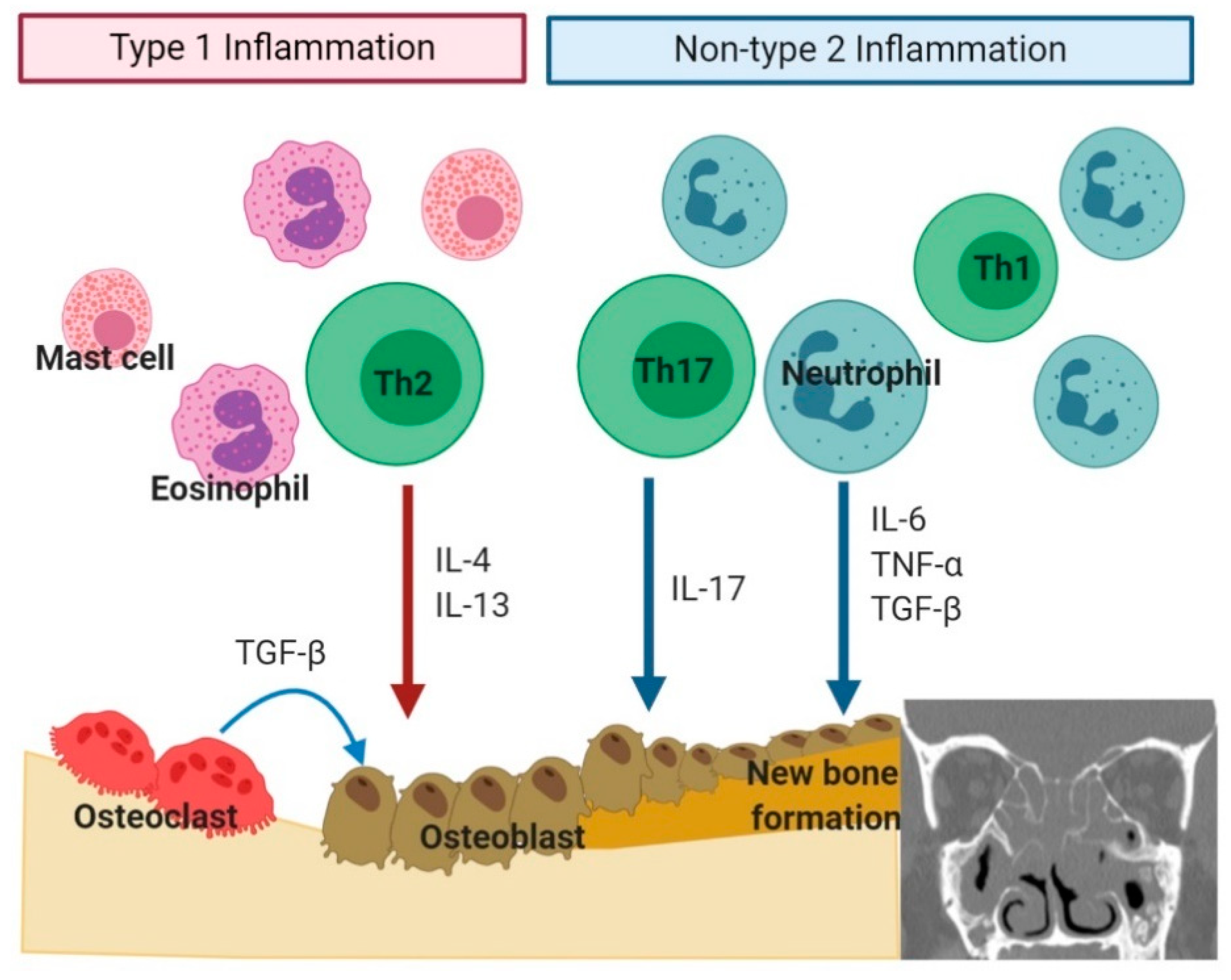
3.3. Bone Remodeling
3.3.1. Type 2 Inflammation in Bone Remodeling
3.3.2. Non-Type 2 Inflammation in Bone Remodeling
4. Conclusions
Funding
Conflicts of Interest
Abbreviations
| CRS | Chronic rhinosinusitis |
| AR | Allergic rhinitis |
| BMT | Basement membrane thickening |
| CCL | Chemokine (C-C motif) ligand |
| CRSsNP | Chronic rhinosinusitis without nasal polyp |
| CRSwNP | Chronic rhinosinusitis with nasal polyp |
| CXCL | Chemokine (C-X-C motif) ligand |
| ECM | Extracellular matrix |
| EMT | Epithelial-mesenchymal transition |
| ERK | Extracellular signal-regulated kinase |
| HDAC | Histone deacetylase |
| HIF-1α | Hypoxia-inducible factor -1α |
| IFN-γ | Interferon-γ |
| IgE | Immunoglobulin E |
| IL | Interleukin |
| ILC1s | Type 1 innate lymphoid cells |
| ILC2s | Type 2 Innate lymphoid cells |
| ILC3s | Type 3 innate lymphoid cells |
| MMP | Matrix metalloproteinase |
| MPO | Myeloperoxidase |
| MUC5AC | Mucin 5AC |
| MUC5B | Mucin 5B |
| OSM | Oncostatin |
| P-gp | P-glycoprotein |
| RUNX2 | Runt-related transcription factor 2 |
| S.aureus | Staphylococcus aureus |
| SIRT1 | Sirtuin 1 |
| TGF-β | Transforming growth factor-β |
| Th1 | Type 1 T helper |
| Th17 | Type 17 T helper |
| Th2 | Type 2 T helper |
| TIMP | Tissue inhibitors of metalloproteinases |
| TNF-α | Tumor necrosis factor α |
| tPA | Tissue plasminogen activator |
| Tregs | Regulatory T cells |
| TSLP | Thymic stromal lymphopoietin |
| uPA | Urokinase-type plasminogen activator |
| α-SMA | Smooth muscle actin |
References
- Fokkens, W.J.; Lund, V.J.; Hopkins, C.; Hellings, P.W.; Kern, R.; Reitsma, S.; Toppila-Salmi, S.; Bernal-Sprekelsen, M.; Mullol, J.; Alobid, I.; et al. European Position Paper on Rhinosinusitis and Nasal Polyps 2020. Rhinology 2020, 58, 1–464. [Google Scholar] [CrossRef]
- McCormick, J.P.; Thompson, H.M.; Cho, D.-Y.; Woodworth, B.A.; Grayson, J.W. Phenotypes in Chronic Rhinosinusitis. Curr. Allergy Asthma Rep. 2020, 20, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Meltzer, E.O.; Hamilos, D.L.; Hadley, J.A.; Lanza, D.C.; Marple, B.F.; Nicklas, R.A.; Bachert, C.; Baraniuk, J.; Baroody, F.M.; Benninger, M.S.; et al. Otolaryngology-Head and Neck Surgery. Otolaryngol. Neck Surg. 2004, 131, 1–62. [Google Scholar] [CrossRef]
- Akdis, C.A.; Bachert, C.; Cingi, C.; Dykewicz, M.S.; Hellings, P.W.; Naclerio, R.M.; Schleimer, R.P.; Ledford, D.K. Endotypes and phenotypes of chronic rhinosinusitis: A PRACTALL document of the European Academy of Allergy and Clinical Immunology and the American Academy of Allergy, Asthma & Immunology. J. Allergy Clin. Immunol. 2013, 131, 1479–1490. [Google Scholar] [CrossRef] [Green Version]
- Bachert, C.; Akdis, C.A. Phenotypes and Emerging Endotypes of Chronic Rhinosinusitis. J. Allergy Clin. Immunol. Pr. 2016, 4, 621–628. [Google Scholar] [CrossRef]
- Van Zele, T.; Claeys, S.; Gevaert, P.; Van Maele, G.; Holtappels, G.; Van Cauwenberge, P.; Bachert, C. Differentiation of chronic sinus diseases by measurement of inflammatory mediators. Allergy 2006, 61, 1280–1289. [Google Scholar] [CrossRef]
- Brescia, G.; Zanotti, C.; Parrino, D.; Barion, U.; Marioni, G. Nasal polyposis pathophysiology: Endotype and phenotype open issues. Am. J. Otolaryngol. 2018, 39, 441–444. [Google Scholar] [CrossRef]
- Cao, P.-P.; Li, H.-B.; Wang, B.-F.; Wang, S.-B.; You, X.-J.; Cui, Y.-H.; Wang, D.-Y.; Desrosiers, M.; Liu, Z. Distinct immunopathologic characteristics of various types of chronic rhinosinusitis in adult Chinese. J. Allergy Clin. Immunol. 2009, 124, 478–484.e2. [Google Scholar] [CrossRef]
- Cho, S.-W.; Kim, D.W.; Kim, J.-W.; Lee, C.H.; Rhee, C.-S. Classification of chronic rhinosinusitis according to a nasal polyp and tissue eosinophilia: Limitation of current classification system for Asian population. Asia Pac. Allergy 2017, 7, 121–130. [Google Scholar] [CrossRef] [Green Version]
- Delemarre, T.; Holtappels, G.; De Ruyck, N.; Zhang, N.; Nauwynck, H.; Bachert, C.; Gevaert, E. Type 2 inflammation in chronic rhinosinusitis without nasal polyps: Another relevant endotype. J. Allergy Clin. Immunol. 2020, 146, 337–343. [Google Scholar] [CrossRef]
- Beers, M.F.; Morrisey, E.E. The three R’s of lung health and disease: Repair, remodeling, and regeneration. J. Clin. Investig. 2011, 121, 2065–2073. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hough, K.P.; Curtiss, M.L.; Blain, T.J.; Liu, R.-M.; Trevor, J.; Deshane, J.S.; Thannickal, V.J. Airway Remodeling in Asthma. Front. Med. 2020, 7, 191. [Google Scholar] [CrossRef] [PubMed]
- Samitas, K.; Carter, A.; Kariyawasam, H.H.; Xanthou, G. Upper and lower airway remodelling mechanisms in asthma, allergic rhinitis and chronic rhinosinusitis: The one airway concept revisited. Allergy 2017, 73, 993–1002. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bassiouni, A.; Chen, P.G.; Wormald, P.-J. Mucosal remodeling and reversibility in chronic rhinosinusitis. Curr. Opin. Allergy Clin. Immunol. 2013, 13, 4–12. [Google Scholar] [CrossRef]
- Husain, Q.; Sedaghat, A. Understanding and clinical relevance of chronic rhinosinusitis endotypes. Clin. Otolaryngol. 2019, 44, 887–897. [Google Scholar] [CrossRef]
- Wang, X.; Zhang, N.; Bo, M.; Holtappels, G.; Zheng, M.; Lou, H.; Wang, H.; Zhang, L.; Bachert, C. Diversity of T H cytokine profiles in patients with chronic rhinosinusitis: A multicenter study in Europe, Asia, and Oceania. J. Allergy Clin. Immunol. 2016, 138, 1344–1353. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tan, B.K.; Klingler, A.I.; Poposki, J.A.; Stevens, W.W.; Peters, A.T.; Suh, L.A.; Norton, J.; Carter, R.G.; Hulse, K.E.; Harris, K.E.; et al. Heterogeneous inflammatory patterns in chronic rhinosinusitis without nasal polyps in Chicago, Illinois. J. Allergy Clin. Immunol. 2017, 139, 699–703. [Google Scholar] [CrossRef] [Green Version]
- Tomassen, P.; Vandeplas, G.; Van Zele, T.; Cardell, L.O.; Arebro, J.; Olze, H.; Förster-Ruhrmann, U.; Kowalski, M.L.; Olszewska-Ziąber, A.; Holtappels, G.; et al. Inflammatory endotypes of chronic rhinosinusitis based on cluster analysis of biomarkers. J. Allergy Clin. Immunol. 2016, 137, 1449–1456. [Google Scholar] [CrossRef] [Green Version]
- Turner, J.H.; Chandra, R.K.; Li, P.; Bonnet, K.; Schlundt, D.G. Identification of clinically relevant chronic rhinosinusitis endotypes using cluster analysis of mucus cytokines. J. Allergy Clin. Immunol. 2018, 141, 1895–1897.e7. [Google Scholar] [CrossRef] [Green Version]
- Schleimer, R.P. Immunopathogenesis of Chronic Rhinosinusitis and Nasal Polyposis. Annu. Rev. Pathol. Mech. Dis. 2017, 12, 331–357. [Google Scholar] [CrossRef] [Green Version]
- Stevens, W.W.; Peters, A.T.; Tan, B.K.; Klingler, A.I.; Poposki, J.A.; Hulse, K.E.; Grammer, L.C.; Welch, K.C.; Smith, S.S.; Conley, D.B.; et al. Associations Between Inflammatory Endotypes and Clinical Presentations in Chronic Rhinosinusitis. J. Allergy Clin. Immunol. Pr. 2019, 7, 2812–2820. [Google Scholar] [CrossRef]
- Boita, M.; Bucca, C.; Riva, G.; Heffler, E.; Rolla, G. Release of Type 2 Cytokines by Epithelial Cells of Nasal Polyps. J. Immunol. Res. 2016, 2016, 1–7. [Google Scholar] [CrossRef]
- Licona-Limon, P.; Kim, L.K.; Palm, N.W.; Flavell, R.A. TH2, allergy and group 2 innate lymphoid cells. Nat. Immunol. 2013, 14, 536–542. [Google Scholar] [CrossRef]
- Omori, M.; Ziegler, S. Induction of IL-4 expression in CD4(+) T cells by thymic stromal lymphopoietin. J. Immunol. 2007, 178, 1396–1404. [Google Scholar] [CrossRef] [Green Version]
- Saluja, R.; Zoltowska, A.; Ketelaar, M.E.; Nilsson, G. IL-33 and Thymic Stromal Lymphopoietin in mast cell functions. Eur. J. Pharmacol. 2016, 778, 68–76. [Google Scholar] [CrossRef]
- Punnonen, J.; Yssel, H.; Devries, J. The relative contribution of IL-4 and IL-13 to human IgE synthesis induced by activated CD4 or CD8 T cells. J. Allergy Clin. Immunol. 1997, 100, 792–801. [Google Scholar] [CrossRef]
- Hamilos, D.L.; Leung, D.Y.; Wood, R.; Cunningham, L.; Bean, D.K.; Yasruel, Z.; Schotman, E.; Hamid, Q. Evidence for distinct cytokine expression in allergic versus nonallergic chronic sinusitis. J. Allergy Clin. Immunol. 1995, 96, 537–544. [Google Scholar] [CrossRef]
- E Peterson, S.; Poposki, J.A.; Nagarkar, D.R.; Chustz, R.T.; Peters, A.T.; Suh, L.A.; Carter, R.; Norton, J.; Harris, K.E.; Grammer, L.C.; et al. Increased expression of CC chemokine ligand 18 in patients with chronic rhinosinusitis with nasal polyps. J. Allergy Clin. Immunol. 2012, 129, 119–127. [Google Scholar] [CrossRef] [Green Version]
- Poposki, J.A.; Uzzaman, A.; Nagarkar, D.R.; Chustz, R.T.; Peters, A.T.; Suh, L.A.; Carter, R.; Norton, J.; Harris, K.E.; Grammer, L.C.; et al. Increased expression of the chemokine CCL23 in eosinophilic chronic rhinosinusitis with nasal polyps. J. Allergy Clin. Immunol. 2011, 128, 73–81. [Google Scholar] [CrossRef] [Green Version]
- Vickery, T.W.; Ramakrishnan, V.R.; Suh, J.D. The Role of Staphylococcus aureus in Patients with Chronic Sinusitis and Nasal Polyposis. Curr. Allergy Asthma Rep. 2019, 19, 21. [Google Scholar] [CrossRef] [PubMed]
- Lan, F.; Zhang, N.; Holtappels, G.; De Ruyck, N.; Krysko, O.; Van Crombruggen, K.; Braun, H.; Johnston, S.L.; Papadopoulos, N.G.; Zhang, L.; et al. Staphylococcus aureusInduces a Mucosal Type 2 Immune Response via Epithelial Cell–derived Cytokines. Am. J. Respir. Crit. Care Med. 2018, 198, 452–463. [Google Scholar] [CrossRef] [PubMed]
- Hirschberg, A.; Kiss, M.; Kadocsa, E.; Polyanka, H.; Szabo, K.; Razga, Z.; Bella, Z.; Tiszlavicz, L.; Kemeny, L. Different activations of toll-like receptors and antimicrobial peptides in chronic rhinosinusitis with or without nasal polyposis. Eur. Arch. Oto-Rhino-Laryngol. 2016, 273, 1779–1788. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jia, L.; Wu, C. The Biology and Functions of Th22 Cells. Cannabinoids Neuropsychiatr. Disord. 2014, 841, 209–230. [Google Scholar] [CrossRef]
- Bachert, C.; Van Kempen, M.J.P.K.; Höpken, K.; Holtappels, G.; Wagenmann, M. Elevated levels of myeloperoxidase, pro-inflammatory cytokines and chemokines in naturally acquired upper respiratory tract infections. Eur. Arch. Oto-Rhino-Laryngol. 2001, 258, 406–412. [Google Scholar] [CrossRef] [PubMed]
- Georgiev, P.; Charbonnier, L.-M.; Chatila, T.A. Regulatory T Cells: The Many Faces of Foxp3. J. Clin. Immunol. 2019, 39, 623–640. [Google Scholar] [CrossRef]
- Palmer, C.; Mulligan, J.K.; Smith, S.E.; Atkinson, C. The Role of Regulatory T Cells in the Regulation of Upper Airway Inflammation. Am. J. Rhinol. Allergy 2017, 31, 345–351. [Google Scholar] [CrossRef] [Green Version]
- Van Bruaene, N.; DeRycke, L.; Perez-Novo, C.A.; Gevaert, P.; Holtappels, G.; De Ruyck, N.; Cuvelier, C.; Van Cauwenberge, P.; Bachert, C. TGF-β signaling and collagen deposition in chronic rhinosinusitis. J. Allergy Clin. Immunol. 2009, 124, 253–259. [Google Scholar] [CrossRef]
- Stevens, W.W.; Lee, R.J.; Schleimer, R.P.; Cohen, N.A. Chronic rhinosinusitis pathogenesis. J. Allergy Clin. Immunol. 2015, 136, 1442–1453. [Google Scholar] [CrossRef] [Green Version]
- Shi, L.-L.; Xiong, P.; Zhang, L.; Cao, P.-P.; Liao, B.; Lu, X.; Cui, Y.-H.; Liu, Z. Features of airway remodeling in different types of Chinese chronic rhinosinusitis are associated with inflammation patterns. Allergy 2012, 68, 101–109. [Google Scholar] [CrossRef]
- Kountakis, S.E.; Arango, P.; Bradley, D.; Wade, Z.K.; Borish, L. Molecular and Cellular Staging for the Severity of Chronic Rhinosinusitis. Laryngoscope 2004, 114, 1895–1905. [Google Scholar] [CrossRef]
- Hellings, P.W.; Steelant, B. Epithelial barriers in allergy and asthma. J. Allergy Clin. Immunol. 2020, 145, 1499–1509. [Google Scholar] [CrossRef] [PubMed]
- Bankova, L.G.; Barrett, N.A. Epithelial cell function and remodeling in nasal polyposis. Ann. Allergy Asthma Immunol. 2020, 124, 333–341. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davies, D.E. The Role of the Epithelium in Airway Remodeling in Asthma. Proc. Am. Thorac. Soc. 2009, 6, 678–682. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khalmuratova, R.; Park, J.-W.; Shin, H.-W. Immune Cell Responses and Mucosal Barrier Disruptions in Chronic Rhinosinusitis. Immune Netw. 2017, 17, 60–67. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, D.H.; Chu, H.-S.; Lee, J.Y.; Hwang, S.J.; Lee, S.H.; Lee, H.-M. Up-regulation of MUC5AC and MUC5B Mucin Genes in Chronic Rhinosinusitis. Arch. Otolaryngol. Head Neck Surg. 2004, 130, 747–752. [Google Scholar] [CrossRef] [Green Version]
- Kalluri, R.; Weinberg, R.A. The basics of epithelial-mesenchymal transition. J. Clin. Investig. 2009, 119, 1420–1428. [Google Scholar] [CrossRef] [Green Version]
- Hackett, T.-L.; Warner, S.M.; Stefanowicz, D.; Shaheen, F.; Pechkovsky, D.V.; Murray, L.A.; Argentieri, R.; Kicic, A.; Stick, S.M.; Bai, T.R.; et al. Induction of Epithelial–Mesenchymal Transition in Primary Airway Epithelial Cells from Patients with Asthma by Transforming Growth Factor-β1. Am. J. Respir. Crit. Care Med. 2009, 180, 122–133. [Google Scholar] [CrossRef]
- Thiery, J.P.; Acloque, H.; Huang, R.Y.J.; Nieto, M.A. Epithelial-Mesenchymal Transitions in Development and Disease. Cell 2009, 139, 871–890. [Google Scholar] [CrossRef]
- Ponikau, J.U.; A Sherris, D.; Kephart, G.M.; Kern, E.B.; A Gaffey, T.; E Tarara, J.; Kita, H. Features of airway remodeling and eosinophilic inflammation in chronic rhinosinusitis. J. Allergy Clin. Immunol. 2003, 112, 877–882. [Google Scholar] [CrossRef]
- Saitoh, T.; Kusunoli, T.; Yao, T.; Kawano, K.; Kojima, Y.; Miyahara, K.; Onoda, J.; Yokoi, H.; Ikeda, K. Relationship between epithelial damage or basement membrane thickness and eosinophilic infiltration in nasal polyps with chronic rhinosinusitis. Rhinol. J. 2009, 47, 275–279. [Google Scholar] [CrossRef] [Green Version]
- Hwang, C.S.; Park, S.C.; Cho, H.-J.; Park, D.-J.; Yoon, J.-H.; Kim, C.-H. Eosinophil extracellular trap formation is closely associated with disease severity in chronic rhinosinusitis regardless of nasal polyp status. Sci. Rep. 2019, 9, 8061. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soyka, M.B.; Wawrzyniak, P.; Eiwegger, T.; Holzmann, D.; Treis, A.; Wanke, K.; Kast, J.I.; Akdis, C.A. Defective epithelial barrier in chronic rhinosinusitis: The regulation of tight junctions by IFN-γ and IL-4. J. Allergy Clin. Immunol. 2012, 130, 1087–1096. [Google Scholar] [CrossRef] [PubMed]
- Huang, Z.-Q.; Liu, J.; Ong, H.H.; Yuan, T.; Zhou, X.-M.; Wang, J.; Tan, K.S.; Chow, V.T.; Yang, Q.-T.; Shi, L.; et al. Interleukin-13 Alters Tight Junction Proteins Expression Thereby Compromising Barrier Function and Dampens Rhinovirus Induced Immune Responses in Nasal Epithelium. Front. Cell Dev. Biol. 2020, 8, 572749. [Google Scholar] [CrossRef] [PubMed]
- Martens, K.; Seys, S.F.; Alpizar, Y.A.; Schrijvers, R.; Bullens, D.M.; Breynaert, C.; Lebeer, S.; Steelant, B. Staphylococcus aureus enterotoxin B disrupts nasal epithelial barrier integrity. Clin. Exp. Allergy 2021, 51, 87–98. [Google Scholar] [CrossRef] [PubMed]
- Wu, D.; Wei, Y.; Bleier, B.S. Emerging Role of Proteases in the Pathogenesis of Chronic Rhinosinusitis with Nasal Polyps. Front. Cell. Infect. Microbiol. 2018, 7, 538. [Google Scholar] [CrossRef] [Green Version]
- Kouzaki, H.; Matsumoto, K.; Kato, T.; Tojima, I.; Shimizu, S.; Shimizu, T. Epithelial Cell-Derived Cytokines Contribute to the Pathophysiology of Eosinophilic Chronic Rhinosinusitis. J. Interf. Cytokine Res. 2016, 36, 169–179. [Google Scholar] [CrossRef]
- Jiao, J.; Duan, S.; Meng, N.; Li, Y.; Fan, E.; Zhang, L. Role of IFN-γ, IL-13, and IL-17 on mucociliary differentiation of nasal epithelial cells in chronic rhinosinusitis with nasal polyps. Clin. Exp. Allergy 2016, 46, 449–460. [Google Scholar] [CrossRef]
- Ishinaga, H.; Kitano, M.; Toda, M.; D’Alessandro-Gabazza, C.N.; Gabazza, E.; Shah, S.A.; Takeuchi, K. Interleukin-33 induces mucin gene expression and goblet cell hyperplasia in human nasal epithelial cells. Cytokine 2017, 90, 60–65. [Google Scholar] [CrossRef]
- Seshadri, S.; Lu, X.; Purkey, M.R.; Homma, T.; Choi, A.W.; Carter, R.; Suh, L.; Norton, J.; Harris, K.E.; Conley, D.B.; et al. Increased expression of the epithelial anion transporter pendrin/SLC26A4 in nasal polyps of patients with chronic rhinosinusitis. J. Allergy Clin. Immunol. 2015, 136, 1548–1558. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weiss, A.; Attisano, L. The TGFbeta Superfamily Signaling Pathway. Wiley Interdiscip. Rev. Dev. Boil. 2013, 2, 47–63. [Google Scholar] [CrossRef]
- Park, I.-H.; Kang, J.-H.; Shin, J.-M.; Lee, H.-M. Trichostatin A Inhibits Epithelial Mesenchymal Transition Induced by TGF-β1 in Airway Epithelium. PLoS ONE 2016, 11, e0162058. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Li, C.; Zhu, G.; Yuan, W.; Xiao, Z.-A. TGF-β1 Induces Epithelial-Mesenchymal Transition of Chronic Sinusitis with Nasal Polyps through MicroRNA-21. Int. Arch. Allergy Immunol. 2019, 179, 304–319. [Google Scholar] [CrossRef] [PubMed]
- Ms, A.D.; Khalil, S.M.; Lane, A.P. Nasal polyp fibroblasts modulate epithelial characteristics via Wnt signaling. Int. Forum Allergy Rhinol. 2018, 8, 1412–1420. [Google Scholar] [CrossRef]
- Lee, M.; Kim, D.W.; Khalmuratova, R.; Shin, S.-H.; Kim, Y.-M.; Han, D.H.; Kim, H.-J.; Kim, D.-Y.; Rhee, C.-S.; Park, J.-W.; et al. The IFN-γ–p38, ERK kinase axis exacerbates neutrophilic chronic rhinosinusitis by inducing the epithelial-to-mesenchymal transition. Mucosal Immunol. 2019, 12, 601–611. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shin, H.-W.; Cho, K.; Kim, D.W.; Han, D.H.; Khalmuratova, R.; Kim, S.-W.; Jeon, S.-Y.; Min, Y.-G.; Lee, C.H.; Rhee, C.-S.; et al. Hypoxia-inducible Factor 1 Mediates Nasal Polypogenesis by Inducing Epithelial-to-Mesenchymal Transition. Am. J. Respir. Crit. Care Med. 2012, 185, 944–954. [Google Scholar] [CrossRef]
- Lee, M.; Kim, D.W.; Yoon, H.; So, D.; Khalmuratova, R.; Rhee, C.-S.; Park, J.-W.; Shin, H.-W. Sirtuin 1 attenuates nasal polypogenesis by suppressing epithelial-to-mesenchymal transition. J. Allergy Clin. Immunol. 2016, 137, 87–98. [Google Scholar] [CrossRef]
- Milara, J.; Morell, A.; Ballester, B.; Armengot, M.; Morcillo, E.; Cortijo, J. MUC4 impairs the anti-inflammatory effects of corticosteroids in patients with chronic rhinosinusitis with nasal polyps. J. Allergy Clin. Immunol. 2017, 139, 855–862. [Google Scholar] [CrossRef] [Green Version]
- Xia, W.; Bai, J.; Wu, X.; Wei, Y.; Feng, S.; Li, L.; Zhang, J.; Xiong, G.; Fan, Y.; Shi, J.; et al. Interleukin-17A Promotes MUC5AC Expression and Goblet Cell Hyperplasia in Nasal Polyps via the Act1-Mediated Pathway. PLoS ONE 2014, 9, e98915. [Google Scholar] [CrossRef]
- Yan, D.; Ye, Y.; Zhang, J.; Zhao, J.; Yu, J.; Luo, Q. Human Neutrophil Elastase Induces MUC5AC Overexpression in Chronic Rhinosinusitis Through miR-146a. Am. J. Rhinol. Allergy 2020, 34, 59–69. [Google Scholar] [CrossRef]
- Luo, Q.; Zhang, Z.; Liu, D.; Feng, K.; Jin, X.; Zhang, J. Human neutrophil elastase induces MUC5AC overexpression in chronic rhinosinusitis through tumour necrosis factor-α converting enzyme. Acta Oto-Laryngol. 2016, 136, 641–648. [Google Scholar] [CrossRef]
- Wang, X.; Zhao, C.; Ji, W.; Xu, Y.; Guo, H. Relationship of TLR2, TLR4 and tissue remodeling in chronic rhinosinusitis. Int. J. Clin. Exp. Pathol. 2015, 8, 1199–1212. [Google Scholar] [PubMed]
- Molet, S.M.; Hamid, Q.A.; Hamilos, D.L. IL-11 and IL-17 expression in nasal polyps: Relationship to collagen deposition and suppression by intranasal fluticasone propionate. Laryngoscope 2003, 113, 1803–1812. [Google Scholar] [CrossRef] [PubMed]
- Rehl, R.M.; Balla, A.A.; Cabay, R.J.; Hearp, M.L.; Pytynia, K.B.; Joe, S.A. Mucosal Remodeling in Chronic Rhinosinusitis. Am. J. Rhinol. 2007, 21, 651–657. [Google Scholar] [CrossRef] [PubMed]
- Sobol, S.E.; Fukakusa, M.; Christodoulopoulos, P.; Manoukian, J.J.; Schloss, M.D.; Frenkiel, S.; Hamid, Q. Inflammation and Remodeling of the Sinus Mucosa in Children and Adults with Chronic Sinusitis. Laryngoscope 2003, 113, 410–414. [Google Scholar] [CrossRef] [PubMed]
- Zang, H.-R.; Wang, T.; Li, Y.; Li, P.; Zhang, S.-Z.; Fan, E.-Z.; Li, Y. A histopathological study: Chronic rhinosinusitis in adolescents versus adults. Zhonghua Yi Xue Za Zhi 2009, 89, 1975–1978. [Google Scholar] [PubMed]
- Kostamo, K.; Tervahartiala, T.; Sorsa, T.; Richardson, M.; Toskala, E. Metalloproteinase Function in Chronic Rhinosinusitis with Nasal Polyposis. Laryngoscope 2007, 117, 638–643. [Google Scholar] [CrossRef] [PubMed]
- Shapiro, S.D.; Senior, R.M. Matrix Metalloproteinases. Am. J. Respir. Cell Mol. Biol. 1999, 20, 1100–1102. [Google Scholar] [CrossRef] [PubMed]
- Kahveci, O.K.; Derekoy, F.S.; Yilmaz, M.; Serteser, M.; Altuntas, A. The role of MMP-9 and TIMP-1 in nasal polyp formation. Swiss Med. Wkly. 2008, 138, 684–688. [Google Scholar]
- Tos, M.; Mogensen, C. Mucus Production in Chronic Maxillary Sinusitis: A Quantitative Histopathological Study. Acta Oto-Laryngol. 1984, 97, 151–159. [Google Scholar] [CrossRef]
- Ali, M.S.; Wilson, J.A.; Bennett, M.; Pearson, J.P. Mucin gene expression in nasal polyps. Acta Oto-Laryngol. 2005, 125, 618–624. [Google Scholar] [CrossRef]
- Tipirneni, K.E.; Zhang, S.; Cho, D.-Y.; Grayson, J.; Bs, D.F.S.; Mackey, C.; Moore, L.; Cole, D.; Banks, C.G.; Woodworth, B.A. Submucosal gland mucus strand velocity is decreased in chronic rhinosinusitis. Int. Forum Allergy Rhinol. 2018, 8, 509–512. [Google Scholar] [CrossRef] [PubMed]
- Perloff, J.R.; Gannon, F.H.; Bolger, W.E.; Montone, K.T.; Orlandi, R.; Kennedy, D.W. Bone Involvement in Sinusitis: An Apparent Pathway for the Spread of Disease. Laryngoscope 2000, 110, 2095–2099. [Google Scholar] [CrossRef] [PubMed]
- Nonaka, M.; Pawankar, R.; Saji, F.; Yagi, T. Distinct expression of RANTES and GM-CSF by lipopolysaccharide in human nasal fibroblasts but not in other airway fibroblasts. Int. Arch. Allergy Immunol. 1999, 119, 314–321. [Google Scholar] [CrossRef] [PubMed]
- Wang, F.; Yang, Y.; Wu, Q.; Chen, H. Histopathologic analysis in chronic rhinosinusitis: Impact on quality of life outcomes. Am. J. Otolaryngol. 2019, 40, 423–426. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.H.; Kwon, H.J.; Jang, Y.J. Staphylococcus Aureus Increases Cytokine and Matrix Metalloproteinase Expression in Nasal Mucosae of Patients with Chronic Rhinosinusitis and Nasal Polyps. Am. J. Rhinol. Allergy 2010, 24, 422–427. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.-S.; Langhammer, T.; Westhofen, M.; Lorenzen, J. Relationship between matrix metalloproteinases MMP-2, MMP-9, tissue inhibitor of matrix metalloproteinases-1 and IL-5, IL-8 in nasal polyps. Allergy 2007, 62, 66–72. [Google Scholar] [CrossRef]
- Watelet, J.B.; Claeys, C.; Perez-Novo, C.; Gevaert, P.; Van Cauwenberge, P.; Bachert, C. Transforming growth factor beta1 in nasal remodeling: Differences between chronic rhinosinusitis and nasal polyposis. Am. J. Rhinol. 2004, 18, 267–272. [Google Scholar] [CrossRef]
- Watelet, J.B.; Bachert, C.; Claeys, C.; Van Cauwenberge, P. Matrix metalloproteinases MMP-7, MMP-9 and their tissue inhibitor TIMP-1: Expression in chronic sinusitis vs nasal polyposis. Allergy 2004, 59, 54–60. [Google Scholar] [CrossRef]
- Can, I.H.; Ceylan, K.; Caydere, M.; Samim, E.E.; Ustun, H.; Karasoy, D.S. The expression of MMP-2, MMP-7, MMP-9, and TIMP-1 in chronic rhinosinusitis and nasal polyposis. Otolaryngol. Neck Surg. 2008, 139, 211–215. [Google Scholar] [CrossRef]
- Kim, D.-Y.; Cho, S.H.; Takabayashi, T.; Schleimer, R.P. Chronic Rhinosinusitis and the Coagulation System. Allergy Asthma Immunol. Res. 2015, 7, 421–430. [Google Scholar] [CrossRef] [Green Version]
- Takabayashi, T.; Kato, A.; Peters, A.T.; Hulse, K.E.; Suh, L.A.; Carter, R.; Norton, J.; Grammer, L.C.; Tan, B.K.; Chandra, R.K.; et al. Increased expression of factor XIII-A in patients with chronic rhinosinusitis with nasal polyps. J. Allergy Clin. Immunol. 2013, 132, 584–592. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Takabayashi, T.; Kato, A.; Peters, A.T.; Hulse, K.E.; Suh, L.A.; Carter, R.; Norton, J.; Grammer, L.C.; Cho, S.H.; Tan, B.K.; et al. Excessive Fibrin Deposition in Nasal Polyps Caused by Fibrinolytic Impairment through Reduction of Tissue Plasminogen Activator Expression. Am. J. Respir. Crit. Care Med. 2013, 187, 49–57. [Google Scholar] [CrossRef] [Green Version]
- Sejima, T.; Holtappels, G.; Bachert, C. The Expression of Fibrinolytic Components in Chronic Paranasal Sinus Disease. Am. J. Rhinol. Allergy 2011, 25, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; DeRycke, L.; Holtappels, G.; Wang, X.D.; Zhang, L.; Bachert, C.; Zhang, N. Th2 cytokines orchestrate the secretion of MUC 5 AC and MUC 5B in IL -5-positive chronic rhinosinusitis with nasal polyps. Allergy 2019, 74, 131–140. [Google Scholar] [CrossRef]
- Li, X.; Meng, J.; Qiao, X.; Liu, Y.; Liu, F.; Zhang, N.; Zhang, J.; Holtappels, G.; Luo, B.; Zhou, P.; et al. Expression of TGF, matrix metalloproteinases, and tissue inhibitors in Chinese chronic rhinosinusitis. J. Allergy Clin. Immunol. 2010, 125, 1061–1068. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.W.; Eun, K.M.; Roh, E.Y.; Shin, S.; Park, C.H. Chronic Rhinosinusitis without Nasal Polyps in Asian Patients Shows Mixed Inflammatory Patterns and Neutrophil-Related Disease Severity. Mediat. Inflamm. 2019, 2019, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Park, C.H.; Eun, K.M.; Kim, M.-K.; Cho, D.; A Han, S.; Han, S.-Y.; Seo, Y.; Lee, D.-H.; Cho, S.-H.; Kim, D.W. Comparison Between Signature Cytokines of Nasal Tissues in Subtypes of Chronic Rhinosinusitis. Allergy Asthma Immunol. Res. 2019, 11, 201–211. [Google Scholar] [CrossRef]
- Ball, S.L.; Cockell, S.J.; Wilson, J.A.; Mann, D.A.; Fisher, A.J. Microarray analysis of primary epithelial and fibroblast cells in chronic rhinosinusitis without nasal polyps. Rhinology 2020, 58, 581–587. [Google Scholar] [CrossRef]
- Snidvongs, K.; Sacks, R.; Harvey, R.J. Osteitis in Chronic Rhinosinusitis. Curr. Allergy Asthma Rep. 2019, 19, 24. [Google Scholar] [CrossRef]
- Snidvongs, K.; McLachlan, R.; Chin, D.; Pratt, E.; Sacks, R.; Earls, P.; Harvey, R.J. Osteitic bone: A surrogate marker of eosinophilia in chronic rhinosinusitis. Rhinol. J. 2012, 50, 299–305. [Google Scholar] [CrossRef] [Green Version]
- Cho, S.H.; Min, H.J.; Han, H.X.; Paik, S.S.; Kim, K.R. CT analysis and histopathology of bone remodeling in patients with chronic rhinosinusitis. Otolaryngol. Neck Surg. 2006, 135, 404–408. [Google Scholar] [CrossRef] [PubMed]
- De Campos, C.A.C.; Dolci, E.L.L.; Da Silva, L.; Dolci, J.E.L.; De Campos, C.A.H.; Dolci, R.L.L. Osteitis and mucosal inflammation in a rabbit model of sinusitis. Braz. J. Otorhinolaryngol. 2015, 81, 312–320. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Norlander, T.; Westrin, K.M.; Stierna, P. The Inflammatory Response of the Sinus and Nasal Mucosa During Sinusitis: Implications for Research and Therapy. Acta Oto-Laryngol. 1994, 114, 38–44. [Google Scholar] [CrossRef] [PubMed]
- Mehta, V.; Campeau, N.; Kita, H.; Hagan, J.B. Blood and Sputum Eosinophil Levels in Asthma and Their Relationship to Sinus Computed Tomographic Findings. Mayo Clin. Proc. 2008, 83, 671–678. [Google Scholar] [CrossRef]
- Feldman, R.E.; Lam, A.C.; Sadow, P.M.; Bleier, B.S. P-glycoprotein is a marker of tissue eosinophilia and radiographic inflammation in chronic rhinosinusitis without nasal polyps. Int. Forum Allergy Rhinol. 2013, 3, 684–687. [Google Scholar] [CrossRef] [PubMed]
- Miyake, M.M.; Nocera, A.; Miyake, M.M. P-glycoprotein and chronic rhinosinusitis. World J. Otorhinolaryngol. Head Neck Surg. 2018, 4, 169–174. [Google Scholar] [CrossRef]
- Günel, C.; Feldman, R.E.; Bleier, B.S. Osteitis is Associated with P-Glycoprotein Overexpression in Patients with Chronic Sinusitis without Nasal Polyps. Am. J. Rhinol. Allergy 2014, 28, 99–102. [Google Scholar] [CrossRef]
- Günel, C.; Bleier, B.S.; Bozkurt, G.; Eliyatkin, N. Microarray analysis of the genes associated with osteitis in chronic rhinosinusitis. Laryngoscope 2017, 127, E85–E90. [Google Scholar] [CrossRef]
- Sautter, N.B.; Bs, K.L.D.; A Hausman, F.; Trune, D.R.; Ba, F.A.H. Tissue remodeling gene expression in a murine model of chronic rhinosinusitis. Laryngoscope 2012, 122, 711–717. [Google Scholar] [CrossRef] [Green Version]
- Silfverswärd, C.; Penno, H.; Frost, A.; Nilsson, O.; Ljunggren, O. Expression of markers of activity in cultured human osteoblasts: Effects of interleukin-4 and interleukin-13. Scand. J. Clin. Lab. Investig. 2010, 70, 338–342. [Google Scholar] [CrossRef]
- Oue, S.; Ramezanpour, M.; Paramasivan, S.; Miljkovic, D.; Cooksley, C.M.; Bassiouni, A.; Ou, J.; Psaltis, A.J.; Wormald, P.-J.; Vreugde, S. Increased IL-13 expression is independently associated with neo-osteogenesis in patients with chronic rhinosinusitis. J. Allergy Clin. Immunol. 2017, 140, 1444–1448. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khalmuratova, R.; Lee, M.; Park, J.-W.; Shin, H.-W. Evaluation of Neo-Osteogenesis in Eosinophilic Chronic Rhinosinusitis Using a Nasal Polyp Murine Model. Allergy, Asthma Immunol. Res. 2020, 12, 306–321. [Google Scholar] [CrossRef] [PubMed]
- Khalmuratova, R.; Shin, H.-W.; Kim, D.W.; Park, J.-W. Interleukin (IL)-13 and IL-17A contribute to neo-osteogenesis in chronic rhinosinusitis by inducing RUNX2. EBioMedicine 2019, 46, 330–341. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khalid, A.N.; Hunt, J.; Perloff, J.R.; Kennedy, D.W. The Role of Bone in Chronic Rhinosinusitis. Laryngoscope 2002, 112, 1951–1957. [Google Scholar] [CrossRef]
- Dong, Y.; Zhou, B.; Wang, X.; Huang, Z.; Wang, M.; Li, Y.; Zang, H.; Fan, E.; Li, Y.; Wang, X. Computed tomography and histopathological evaluation of osteitis in rabbit models with rhinosinusitis. Acta Oto-Laryngol. 2016, 137, 534–540. [Google Scholar] [CrossRef]
- Huang, Z.; Hajjij, A.; Li, G.; Nayak, J.V.; Zhou, B.; Hwang, P.H. Clinical predictors of neo-osteogenesis in patients with chronic rhinosinusitis. Int. Forum Allergy Rhinol. 2015, 5, 303–309. [Google Scholar] [CrossRef]
- Karempelis, P.; Karp, E.; Rubin, N.; Hunter, R.; Dunitz, J.; Boyer, H. Risk factors for neo-osteogenesis in cystic fibrosis and non‒cystic fibrosis chronic rhinosinusitis. Int. Forum Allergy Rhinol. 2020, 10, 505–510. [Google Scholar] [CrossRef]
- Dong, D.; Zhao, Y.; Xiao, W.; HongYan, Z.; Jia, L.; Yan, X.; Jia, W. Correlation between bacterial biofilms and osteitis in patients with chronic rhinosinusitis. Laryngoscope 2013, 124, 1071–1077. [Google Scholar] [CrossRef]
- Tuszynska, A.; Krzeski, A.; Postuba, M.; Paczek, L.; Wyczalkowska-Tomasik, A.; Gornicka, B.; Pykalo, R. Inflammatory cytokines gene expression in bone tissue from patients with chronic rhinosinusitis- a preliminary study. Rhinol. J. 2010, 48, 415–419. [Google Scholar]
- Wang, M.; Ye, T.; Liang, N.; Huang, Z.; Cui, S.; Li, Y.; Huang, Q.; Zhou, B. Differing Roles for TGF-β/Smad Signaling in Osteitis in Chronic Rhinosinusitis with and without Nasal Polyps. Am. J. Rhinol. Allergy 2015, 29, e152–e159. [Google Scholar] [CrossRef]
- Callejas-Díaz, B.; Martínez-Antón, A.; Picado, C.; Alobid, I.; Pujols, L.; Valero, A.; Roca-Ferrer, J.; Mullol, J. Corticosteroid treatment regulates mucosal remodeling in chronic rhinosinusitis with nasal polyps. Laryngoscope 2015, 125, E158–E167. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Lou, H.; Wang, X.; Wang, Y.; Fan, E.; Li, Y.; Wang, H.; Bachert, C.; Zhang, L. Effect of budesonide transnasal nebulization in patients with eosinophilic chronic rhinosinusitis with nasal polyps. J. Allergy Clin. Immunol. 2015, 135, 922–929.e6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yu, R.-L.; Zhu, D.-D.; Dong, Z. [Effects of glucocorticoid on tissue remodeling of nasal mucosa of chronic rhinosinusitis with nasal polyposis after endoscopic surgery]. Chin. J. Otorhinolaryngol. Head Neck Surg. 2006, 41, 773–776. [Google Scholar]
- Sommer, J.U.; Schultz, J.D.; Grossbaier, J.; Stern-Straeter, J.; Hörmann, K.; Sauter, A. In vitro effects of doxycycline on inflammatory cytokines and gelatinases in chronic rhinosinusitis. In Vivo 2012, 26, 369–374. [Google Scholar]
- Huvenne, W.; Zhang, N.; Tijsma, E.; Hissong, B.; Huurdeman, J.; Holtappels, G.; Claeys, S.; Van Cauwenberge, P.; Nelis, H.; Coenye, T.; et al. Pilot study using doxycycline-releasing stents to ameliorate postoperative healing quality after sinus surgery. Wound Repair Regen. 2008, 16, 757–767. [Google Scholar] [CrossRef] [PubMed]
- Sassa, K.; Mizushima, Y.; Kobayashi, M. Differential Modulatory Effects of Clarithromycin on the Production of Cytokines by a Tumor. Antimicrob. Agents Chemother. 1999, 43, 2787–2789. [Google Scholar] [CrossRef] [Green Version]
- Numata, T.; Nakayama, K.; Utsumi, H.; Kobayashi, K.; Yanagisawa, H.; Hashimoto, M.; Minagawa, S.; Ishikawa, T.; Hara, H.; Araya, J.; et al. Efficacy of mepolizumab for patients with severe asthma and eosinophilic chronic rhinosinusitis. BMC Pulm. Med. 2019, 19, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Nagase, H.; Ueki, S.; Fujieda, S. The roles of IL-5 and anti-IL-5 treatment in eosinophilic diseases: Asthma, eosinophilic granulomatosis with polyangiitis, and eosinophilic chronic rhinosinusitis. Allergol. Int. 2020, 69, 178–186. [Google Scholar] [CrossRef]
- Flood-Page, P.; Menzies-Gow, A.; Phipps, S.; Ying, S.; Wangoo, A.; Ludwig, M.S.; Barnes, N.; Robinson, D.; Kay, A.B. Anti-IL-5 treatment reduces deposition of ECM proteins in the bronchial subepithelial basement membrane of mild atopic asthmatics. J. Clin. Investig. 2003, 112, 1029–1036. [Google Scholar] [CrossRef] [Green Version]
- Bauer, A.M.; Turner, J.H. Personalized Medicine in Chronic Rhinosinusitis. Immunol. Allergy Clin. N. Am. 2020, 40, 281–293. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Type 2 | Non-Type 2 | |
|---|---|---|
| External stimuli | Allergen, Staphylococcus aureus biofilm/enterotoxin, and Fungi | Pollution and bacteria |
| Effector cells | Eosinophils, Th2 cells, ILC2s, B cells, basophils, and mast cells | Neutrophils, NK cells, Type 1: CD8+ T cells, Th1 cells, and ILC1s Type 3: Th17 cells and ILC3s |
| Primary cytokines | IL-4, IL-5, and IL-13 | Type 1: IFN-γ and IL-12 Type 3: IL-17 and IL-22 |
| Other mediators | IL-25, IL-33, TSLP, and IgE | IL-1β, IL-36, IL-6, IL-8, TGF-β, CXCL1, and CXCL10 |
| Clinical features | Bilateral disease Ethmoid sinus > Maxillary sinus Headache/migraine, anosmia, nasal polyposis, asthma, aspirin-induced respiratory disease | Maxillary sinus > Ethmoid sinus Purulent nasal discharge |
| Tissue remodeling features | Barrier disruption, basal membrane thickening, and stromal edema | Basal membrane thickening, goblet cell hyperplasia, fibrosis, and collagen deposition |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, K.; Tai, J.; Lee, S.H.; Kim, T.H. Advances in the Knowledge of the Underlying Airway Remodeling Mechanisms in Chronic Rhinosinusitis Based on the Endotypes: A Review. Int. J. Mol. Sci. 2021, 22, 910. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms22020910
Lee K, Tai J, Lee SH, Kim TH. Advances in the Knowledge of the Underlying Airway Remodeling Mechanisms in Chronic Rhinosinusitis Based on the Endotypes: A Review. International Journal of Molecular Sciences. 2021; 22(2):910. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms22020910
Chicago/Turabian StyleLee, Kijeong, Junhu Tai, Sang Hag Lee, and Tae Hoon Kim. 2021. "Advances in the Knowledge of the Underlying Airway Remodeling Mechanisms in Chronic Rhinosinusitis Based on the Endotypes: A Review" International Journal of Molecular Sciences 22, no. 2: 910. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms22020910