Serum miR-373-3p and miR-194-5p Are Associated with Early Tumor Progression during FOLFIRINOX Treatment in Pancreatic Cancer Patients: A Prospective Multicenter Study

 , , ,
, , ,
Abstract
:1. Introduction
2. Results
2.1. Patient Characteristics
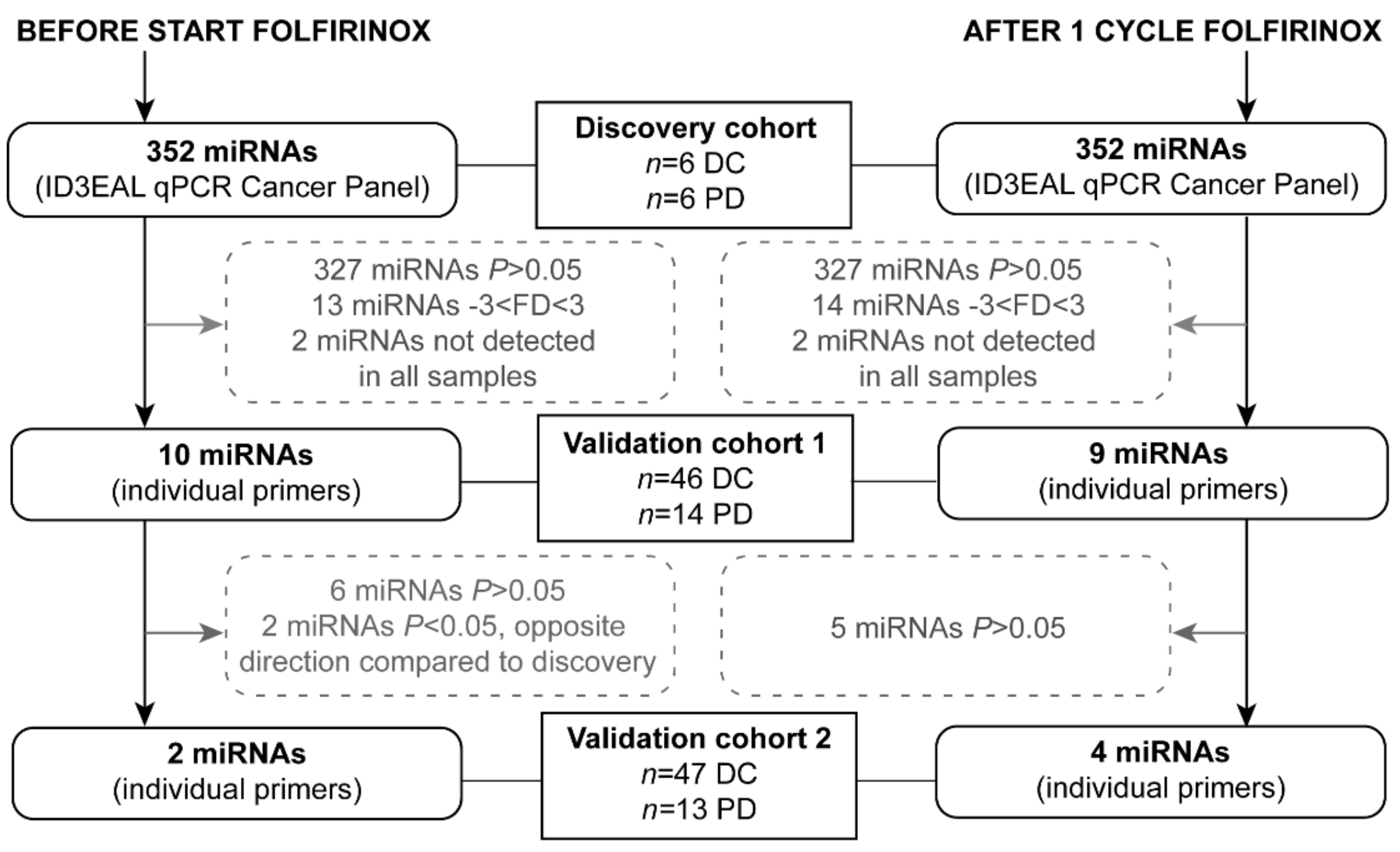
2.2. Serum miRNA Expression in the Discovery Cohort
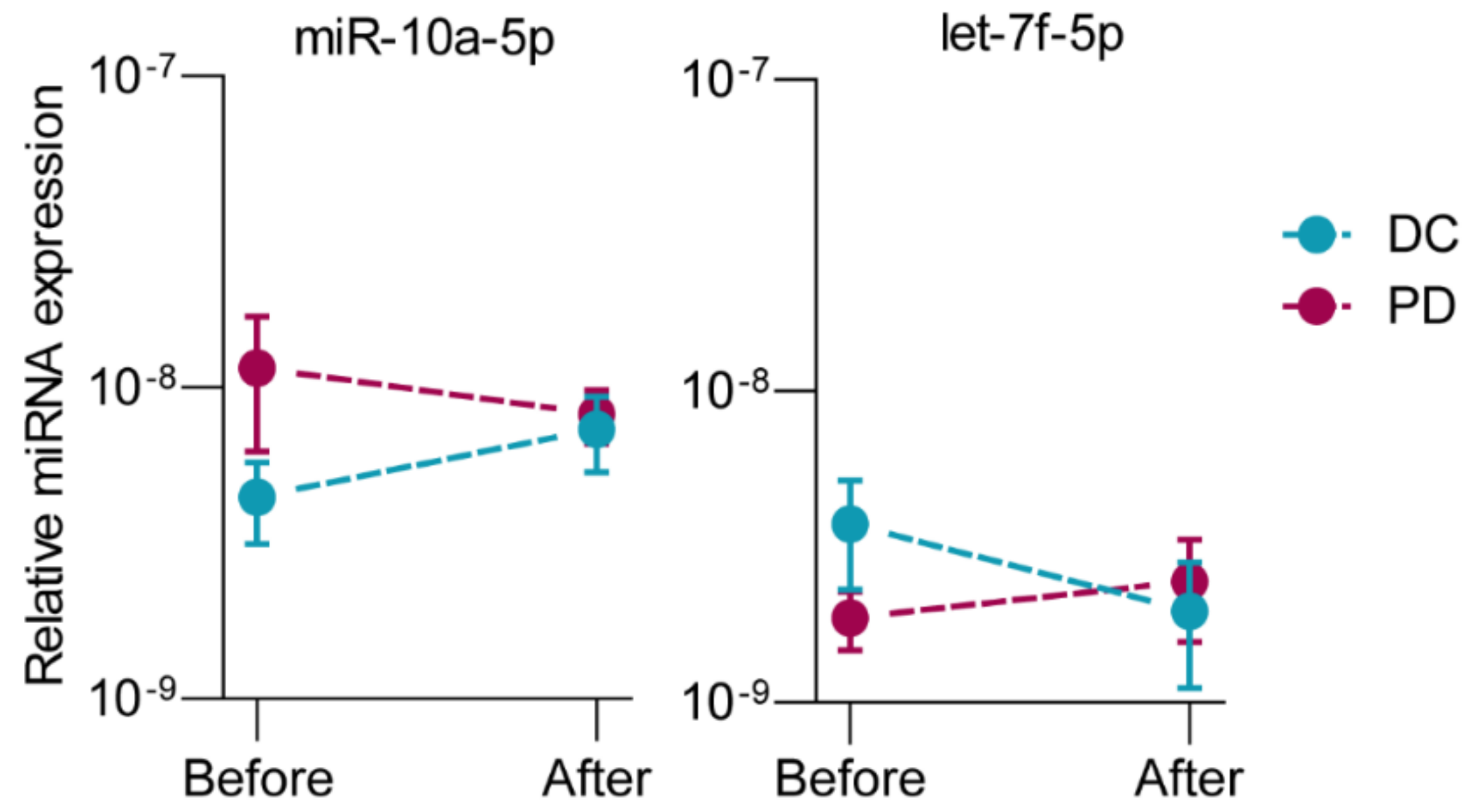
2.3. Serum miRNA Expression in the Validation Cohorts
2.4. Serum miRNA Expression between Disease Stages
2.5. Serum miRNA Expression and Overall Survival
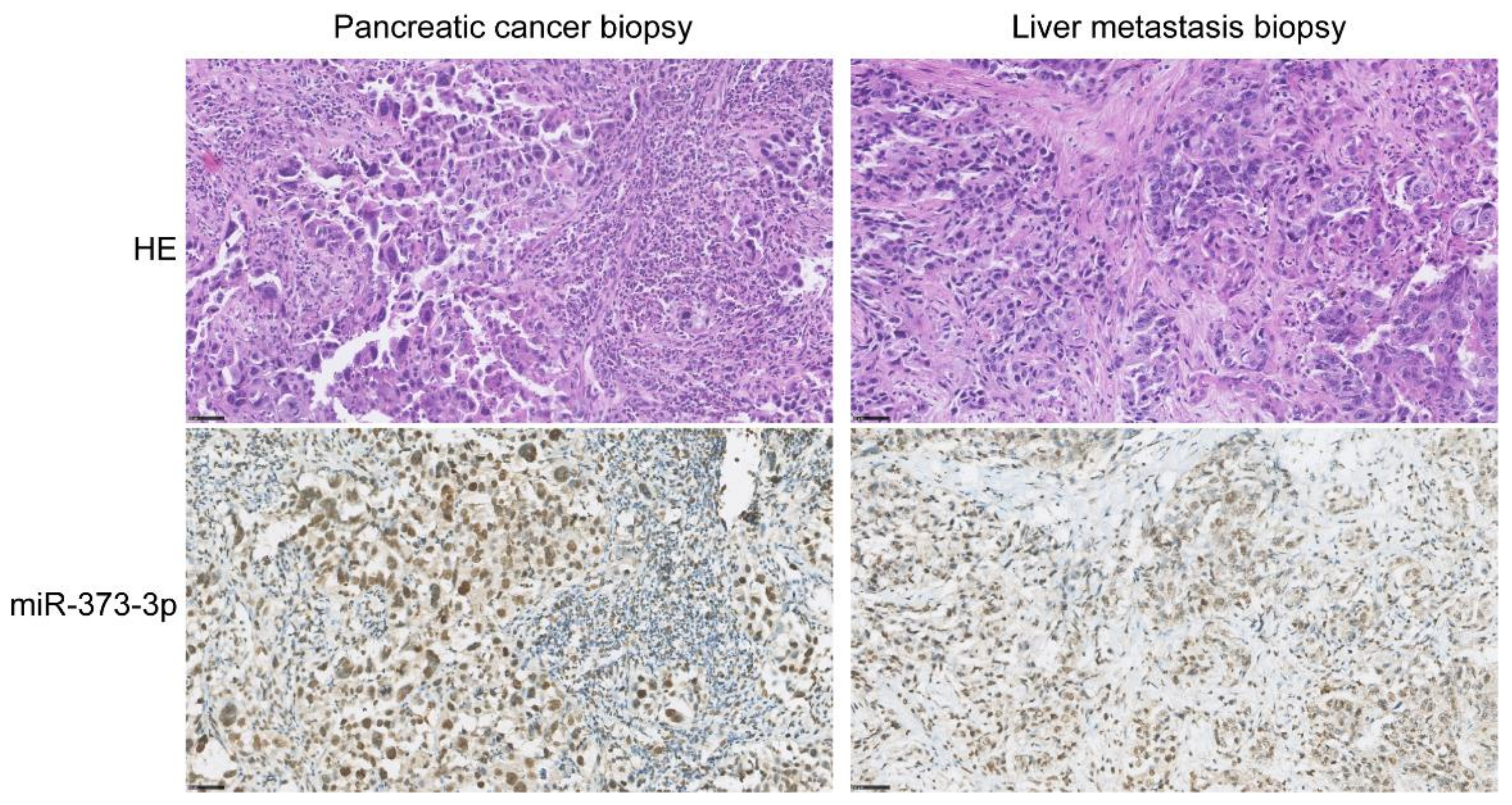
2.6. Tissue miR-373-3p Expression
3. Discussion
4. Materials and Methods
4.1. Patient Selection
4.2. Sample Collection
4.3. Serum miRNA Isolation and Quantitation
4.4. In Situ Hybridization (ISH) of Pancreatic Cancer Tissue
4.5. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ferlay, J.; Soerjomataram, I.; Dikshit, R.; Eser, S.; Mathers, C.; Rebelo, M.; Parkin, D.M.; Forman, D.; Bray, F. Cancer incidence and mortality worldwide: Sources, methods and major patterns in globocan 2012. Int. J. Cancer 2015, 136, E359–E386. [Google Scholar] [CrossRef] [PubMed]
- Rahib, L.; Smith, B.D.; Aizenberg, R.; Rosenzweig, A.B.; Fleshman, J.M.; Matrisian, L.M. Projecting cancer incidence and deaths to 2030: The unexpected burden of thyroid, liver, and pancreas cancers in the united states. Cancer Res. 2014, 74, 2913–2921. [Google Scholar] [CrossRef] [Green Version]
- Suker, M.; Beumer, B.R.; Sadot, E.; Marthey, L.; Faris, J.E.; Mellon, E.A.; El-Rayes, B.F.; Wang-Gillam, A.; Lacy, J.; Hosein, P.J.; et al. Folfirinox for locally advanced pancreatic cancer: A systematic review and patient-level meta-analysis. Lancet Oncol. 2016, 17, 801–810. [Google Scholar] [CrossRef] [Green Version]
- Conroy, T.; Desseigne, F.; Ychou, M.; Bouché, O.; Guimbaud, R.; Bécouarn, Y.; Adenis, A.; Raoul, J.L.; Gourgou-Bourgade, S.; de la Fouchardière, C.; et al. Folfirinox versus gemcitabine for metastatic pancreatic cancer. N. Engl. J. Med. 2011, 364, 1817–1825. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Conroy, T.; Hammel, P.; Hebbar, M.; Ben Abdelghani, M.; Wei, A.C.; Raoul, J.L.; Choné, L.; Francois, E.; Artru, P.; Biagi, J.J.; et al. Folfirinox or gemcitabine as adjuvant therapy for pancreatic cancer. N. Engl. J. Med. 2018, 379, 2395–2406. [Google Scholar] [CrossRef]
- Thibodeau, S.; Voutsadakis, I.A. Folfirinox chemotherapy in metastatic pancreatic cancer: A systematic review and meta-analysis of retrospective and phase ii studies. J. Clin. Med. 2018, 7, 7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xiong, G.; Feng, M.; Yang, G.; Zheng, S.; Song, X.; Cao, Z.; You, L.; Zheng, L.; Hu, Y.; Zhang, T.; et al. The underlying mechanisms of non-coding rnas in the chemoresistance of pancreatic cancer. Cancer Lett. 2017, 397, 94–102. [Google Scholar] [CrossRef]
- Neesse, A.; Michl, P.; Frese, K.K.; Feig, C.; Cook, N.; Jacobetz, M.A.; Lolkema, M.P.; Buchholz, M.; Olive, K.P.; Gress, T.M.; et al. Stromal biology and therapy in pancreatic cancer. Gut 2011, 60, 861–868. [Google Scholar] [CrossRef] [PubMed]
- Long, J.; Zhang, Y.; Yu, X.; Yang, J.; LeBrun, D.G.; Chen, C.; Yao, Q.; Li, M. Overcoming drug resistance in pancreatic cancer. Expert Opin. Ther. Targets 2011, 15, 817–828. [Google Scholar] [CrossRef] [Green Version]
- Allen, K.E.; Weiss, G.J. Resistance may not be futile: Microrna biomarkers for chemoresistance and potential therapeutics. Mol. Cancer Ther. 2010, 9, 3126–3136. [Google Scholar] [CrossRef] [Green Version]
- Si, W.; Shen, J.; Zheng, H.; Fan, W. The role and mechanisms of action of micrornas in cancer drug resistance. Clin. Epigenetics 2019, 11, 25. [Google Scholar] [CrossRef]
- Meijer, L.L.; Garajová, I.; Caparello, C.; Le Large, T.Y.S.; Frampton, A.E.; Vasile, E.; Funel, N.; Kazemier, G.; Giovannetti, E. Plasma mir-181a-5p downregulation predicts response and improved survival after folfirinox in pancreatic ductal adenocarcinoma. Ann. Surg. 2020, 271, 1137–1147. [Google Scholar] [CrossRef]
- Xue, J.; Jia, E.; Ren, N.; Lindsay, A.; Yu, H. Circulating micrornas as promising diagnostic biomarkers for pancreatic cancer: A systematic review. Oncol. Targets Ther. 2019, 12, 6665–6684. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, L.; Zhou, W.B.; Zhou, J.; Wei, Y.; Wang, H.M.; Liu, X.D.; Chen, X.C.; Wang, W.; Ye, L.; Yao, L.C.; et al. Circulating exosomal micrornas as novel potential detection biomarkers in pancreatic cancer. Oncol. Lett. 2020, 20, 1432–1440. [Google Scholar] [CrossRef]
- Daoud, A.Z.; Mulholland, E.J.; Cole, G.; McCarthy, H.O. Micrornas in pancreatic cancer: Biomarkers, prognostic, and therapeutic modulators. BMC Cancer 2019, 19, 1130. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ebrahimi, S.; Hosseini, M.; Ghasemi, F.; Shahidsales, S.; Maftouh, M.; Akbarzade, H.; Parizadeh, S.A.; Hassanian, S.M.; Avan, A. Circulating micrornas as potential diagnostic, prognostic and therapeutic targets in pancreatic cancer. Curr. Pharm Des. 2016, 22, 6444–6450. [Google Scholar] [CrossRef] [PubMed]
- Guo, S.; Fesler, A.; Wang, H.; Ju, J. Microrna based prognostic biomarkers in pancreatic cancer. Biomark Res. 2018, 6, 18. [Google Scholar] [CrossRef] [PubMed]
- Wald, P.; Liu, X.S.; Pettit, C.; Dillhoff, M.; Manilchuk, A.; Schmidt, C.; Wuthrick, E.; Chen, W.; Williams, T.M. Prognostic value of microrna expression levels in pancreatic adenocarcinoma: A review of the literature. Oncotarget 2017, 8, 73345–73361. [Google Scholar] [CrossRef] [Green Version]
- Madurantakam Royam, M.; Ramesh, R.; Shanker, R.; Sabarimurugan, S.; Kumarasamy, C.; Ramesh, N.; Gothandam, K.M.; Baxi, S.; Gupta, A.; Krishnan, S.; et al. Mirna predictors of pancreatic cancer chemotherapeutic response: A systematic review and meta-analysis. Cancers 2019, 11, 900. [Google Scholar] [CrossRef] [Green Version]
- Ohuchida, K.; Mizumoto, K.; Kayashima, T.; Fujita, H.; Moriyama, T.; Ohtsuka, T.; Ueda, J.; Nagai, E.; Hashizume, M.; Tanaka, M. Microrna expression as a predictive marker for gemcitabine response after surgical resection of pancreatic cancer. Ann. Surg. Oncol. 2011, 18, 2381–2387. [Google Scholar] [CrossRef] [Green Version]
- Kaur, G.; Dufour, J.M. Cell lines: Valuable tools or useless artifacts. Spermatogenesis 2012, 2, 1–5. [Google Scholar] [CrossRef] [Green Version]
- Nosirov, B.; Billaud, J.; Vandenbon, A.; Diez, D.; Wijaya, E.; Ishii, K.J.; Teraguchi, S.; Standley, D.M. Mapping circulating serum mirnas to their immune-related target mrnas. Adv. Appl. Bioinform. Chem. 2017, 10, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Pritchard, C.C.; Kroh, E.; Wood, B.; Arroyo, J.D.; Dougherty, K.J.; Miyaji, M.M.; Tait, J.F.; Tewari, M. Blood cell origin of circulating micrornas: A cautionary note for cancer biomarker studies. Cancer Prev. Res. 2012, 5, 492–497. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nakata, K.; Ohuchida, K.; Mizumoto, K.; Aishima, S.; Oda, Y.; Nagai, E.; Tanaka, M. Micro rna-373 is down-regulated in pancreatic cancer and inhibits cancer cell invasion. Ann. Surg. Oncol. 2014, 21 (Suppl. 4), S564–S574. [Google Scholar] [CrossRef] [PubMed]
- Hua, Y.; Chen, H.; Wang, L.; Wang, F.; Wang, P.; Ning, Z.; Li, Y.; Liu, L.; Chen, Z.; Meng, Z. Low serum mir-373 predicts poor prognosis in patients with pancreatic cancer. Cancer Biomark 2017, 20, 95–100. [Google Scholar] [CrossRef] [PubMed]
- Wei, F.; Cao, C.; Xu, X.; Wang, J. Diverse functions of mir-373 in cancer. J. Transl. Med. 2015, 13, 162. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, Y.; Wang, X. Mirdb: An online database for prediction of functional microrna targets. Nucleic Acids Res. 2020, 48, D127–D131. [Google Scholar] [CrossRef] [Green Version]
- Aylon, Y.; Michael, D.; Shmueli, A.; Yabuta, N.; Nojima, H.; Oren, M. A positive feedback loop between the p53 and lats2 tumor suppressors prevents tetraploidization. Genes Dev. 2006, 20, 2687–2700. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Voorhoeve, P.M.; le Sage, C.; Schrier, M.; Gillis, A.J.; Stoop, H.; Nagel, R.; Liu, Y.P.; van Duijse, J.; Drost, J.; Griekspoor, A.; et al. A genetic screen implicates mirna-372 and mirna-373 as oncogenes in testicular germ cell tumors. Cell 2006, 124, 1169–1181. [Google Scholar] [CrossRef] [Green Version]
- Biankin, A.V.; Waddell, N.; Kassahn, K.S.; Gingras, M.C.; Muthuswamy, L.B.; Johns, A.L.; Miller, D.K.; Wilson, P.J.; Patch, A.M.; Wu, J.; et al. Pancreatic cancer genomes reveal aberrations in axon guidance pathway genes. Nature 2012, 491, 399–405. [Google Scholar] [CrossRef]
- Zhang, J.; Zhao, C.Y.; Zhang, S.H.; Yu, D.H.; Chen, Y.; Liu, Q.H.; Shi, M.; Ni, C.R.; Zhu, M.H. Upregulation of mir-194 contributes to tumor growth and progression in pancreatic ductal adenocarcinoma. Oncol. Rep. 2014, 31, 1157–1164. [Google Scholar] [CrossRef] [Green Version]
- Meng, X.; Li, Z.; Zhou, S.; Xiao, S.; Yu, P. Mir-194 suppresses high glucose-induced non-small cell lung cancer cell progression by targeting nfat5. Thorac. Cancer 2019, 10, 1051–1059. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yin, W.; Shi, L.; Mao, Y. Mir-194 regulates nasopharyngeal carcinoma progression by modulating map3k3 expression. FEBS Open Bio. 2019, 9, 43–52. [Google Scholar] [CrossRef] [PubMed]
- Zhao, X.; Hou, Y.; Tuo, Z.; Wei, F. Application values of mir-194 and mir-29 in the diagnosis and prognosis of gastric cancer. Exp. Ther. Med. 2018, 15, 4179–4184. [Google Scholar] [CrossRef] [PubMed]
- Shi, L.; Xie, C.; Zhu, J.; Chen, X. Downregulation of serum mir-194 predicts poor prognosis in osteosarcoma patients. Ann. Diagn. Pathol. 2020, 46, 151488. [Google Scholar] [CrossRef] [PubMed]
- Basati, G.; Razavi, A.E.; Pakzad, I.; Malayeri, F.A. Circulating levels of the mirnas, mir-194, and mir-29b, as clinically useful biomarkers for colorectal cancer. Tumour. Biol. 2016, 37, 1781–1788. [Google Scholar] [CrossRef] [PubMed]
- McShane, L.M.; Altman, D.G.; Sauerbrei, W.; Taube, S.E.; Gion, M.; Clark, G.M. Statistics Subcommittee of the, N.C.I.E.W.G.o.C.D. Reporting recommendations for tumour marker prognostic studies (remark). Br. J. Cancer 2005, 93, 387–391. [Google Scholar] [CrossRef] [Green Version]
- Schwartz, L.H.; Litière, S.; de Vries, E.; Ford, R.; Gwyther, S.; Mandrekar, S.; Shankar, L.; Bogaerts, J.; Chen, A.; Dancey, J.; et al. Recist 1.1-update and clarification: From the recist committee. Eur. J. Cancer 2016, 62, 132–137. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Characteristic | Discovery Cohort (n = 12) | Validation Cohort 1 (n = 60) | Validation Cohort 2 (n = 60) | p | Total Cohort (n = 132) |
|---|---|---|---|---|---|
| Age (years), median (range) | 64 (49–78) | 66 (41–81) | 62 (49–79) | 0.601 | 64 (41–81) |
| Sex, male (%) | 7 (58.3) | 34 (56.7) | 36 (60.0) | 0.934 | 77 (58.3) |
| Stage of disease (%) (Borderline) resectable Locally advanced Metastatic | 2 (16.7) 4 (33.3) 6 (50.0) | 29 (48.3) 18 (30.0) 13 (21.7) | 31 (51.7) 23 (38.3) 6 (10.0) | 0.016 | 62 (47.0) 45 (34.1) 25 (18.9) |
| Cycles of FOLFIRINOX received, median (range) | 4 (2–12) | 8 (2–12) | 8 (1–12) | 0.087 | 8 (1–12) |
| Baseline CA19-9 (kU/L), median (IQR) | 410 (74.5–9341.0) | 147.5 (51.8–910.3) | 216.0 (51.0–845.0) | 0.315 | 190.0 (51.0–1050.0) |
| RECIST response outcome after FOLFIRINOX a (%) Disease control Progressive disease | 6 (50.0) 6 (50.0) | 46 (76.7) 14 (23.3) | 47 (78.3) 13 (21.7) | 0.108 | 99 (75.0) 33 (25.0) |
| Discovery Cohort (n = 6 DC, n = 6 PD) | Validation Cohort 1 (n = 46 DC, n = 14 PD) | Validation Cohort 2 (n = 47 DC, n = 13 PD) | Total Validation Cohort (n = 93 DC, n = 27 PD) | |||||
|---|---|---|---|---|---|---|---|---|
| miRNA | Log2 FD * | p | Log2 FD * | p | Log2 FD * | p | Log2 FD * | p |
| Before start of FOLFIRINOX | ||||||||
| hsa-let-7g-5p a | −2.34 | 0.041 | 0.27 | 0.189 | ||||
| hsa-miR-126-3p | −1.75 | 0.004 | 0.08 | 0.568 | ||||
| hsa-miR-1290 | 1.78 | 0.039 | 0.28 | 0.451 | ||||
| hsa-miR-17-3p | 2.11 | 0.038 | 0.49 | 0.048 | 0.11 | 0.752 | 0.36 | 0.134 |
| hsa-miR-194-5p a | −2.44 | 0.015 | 0.57 | 0.112 | ||||
| hsa-miR-199a-5p | −1.64 | 0.014 | −0.34 | 0.254 | ||||
| hsa-miR-200c-3p | 3.52 | 0.032 | 0.48 | 0.185 | ||||
| hsa-miR-30a-5p a | −2.64 | 0.041 | 0.41 | 0.007 | ||||
| hsa-miR-373-3p | 8.37 | <0.001 | 0.84 | 0.110 | 0.92 | 0.007 | 0.88 | 0.006 |
| hsa-miR-629-5p | −3.56 | 0.048 | 0.58 | 0.015 | ||||
| After one cycle of FOLFIRINOX | ||||||||
| hsa-let-7g-5p a | −1.66 | 0.020 | −0.09 | 0.570 | ||||
| hsa-miR-18a-5p | −1.83 | 0.007 | −0.32 | 0.027 | 0.56 | 0.016 | 0.13 | 0.361 |
| hsa-miR-19a-3p | −1.72 | 0.049 | −0.05 | 0.793 | ||||
| hsa-miR-194-5p a | −2.25 | 0.017 | −0.50 | 0.026 | −0.15 | 0.421 | −0.29 | 0.044 |
| hsa-miR-24-3p | −3.92 | 0.036 | −0.78 | 0.024 | 0.53 | 0.073 | −0.08 | 0.715 |
| hsa-miR-27a-3p | −2.22 | 0.041 | −0.95 | 0.008 | 0.45 | 0.208 | −0.20 | 0.459 |
| hsa-miR-30a-5p a | −1.78 | 0.020 | −0.16 | 0.235 | ||||
| hsa-miR-30d-5p | −3.35 | <0.001 | −0.15 | 0.205 | ||||
| hsa-miR-92b-3p | −1.94 | 0.049 | 0.16 | 0.563 | ||||
| Univariable | Multivariable | |||
|---|---|---|---|---|
| Variable | OR (95% CI) | p | OR (95% CI) | p |
| Stage of disease Resectable LAPC Metastatic | Ref 1.31 (0.58–2.95) 1.87 (0.65–5.35) | 0.521 0.245 | ||
| CA19-9 at baseline (per 100 kU/L) | 1.00 (1.00–1.01) | 0.475 | ||
| miR-17-3p relative expression over reference miRNAs (per 1 × 10−2 increase) a | 1.39 (0.91–2.13) | 0.125 | ||
| miR-373-3p relative expression over reference miRNAs (per 1 × 10−2 increase) a | 2.62 (0.90–7.63) | 0.078 | 3.99 (1.10–14.49) | 0.035 |
| miR-194-5p relative expression over reference miRNAs (per 1 × 10−2 increase) b | 0.94 (0.87–1.00) | 0.065 | 0.91 (0.83–0.99) | 0.030 |
| Univariable | Multivariable | |||
|---|---|---|---|---|
| Variable | HR (95% CI) | p | HR (95% CI) | p |
| Age (per year) | 1.01 (0.99–1.04) | 0.226 | ||
| Stage of disease Resectable LAPC Metastatic | Ref 1.00 (0.66–1.54) 2.16 (1.36–3.43) | 0.985 0.001 | Ref 1.40 (0.72–2.71) 2.51 (1.21–5.23) | 0.316 0.014 |
| CA19-9 at baseline (per 100 kU/L) | 1.00 (1.00–1.01) | 0.009 | 1.00 (1.00–1.01) | 0.116 |
| RECIST response outcome Disease control Progressive disease | Ref 3.85 (2.58–5.73) | <0.001 | Ref 4.64 (2.48–8.68) | <0.001 |
| miR-17-3p relative expression over reference miRNAs (per 1 × 10−2 increase) a | 1.30 (1.02–1.65) | 0.032 | 1.18 (0.92–1.52) | 0.192 |
| miR-373-3p relative expression over reference miRNAs (per 1 × 10−2 increase) a | 1.15 (0.96–1.38) | 0.141 | ||
| miR-194-5p relative expression over reference miRNAs (per 1 × 10−2 increase) b | 0.96 (0.90–1.02) | 0.145 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
van der Sijde, F.; Homs, M.Y.V.; van Bekkum, M.L.; van den Bosch, T.P.P.; Bosscha, K.; Besselink, M.G.; Bonsing, B.A.; de Groot, J.W.B.; Karsten, T.M.; Groot Koerkamp, B.; et al. Serum miR-373-3p and miR-194-5p Are Associated with Early Tumor Progression during FOLFIRINOX Treatment in Pancreatic Cancer Patients: A Prospective Multicenter Study. Int. J. Mol. Sci. 2021, 22, 10902. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms222010902
van der Sijde F, Homs MYV, van Bekkum ML, van den Bosch TPP, Bosscha K, Besselink MG, Bonsing BA, de Groot JWB, Karsten TM, Groot Koerkamp B, et al. Serum miR-373-3p and miR-194-5p Are Associated with Early Tumor Progression during FOLFIRINOX Treatment in Pancreatic Cancer Patients: A Prospective Multicenter Study. International Journal of Molecular Sciences. 2021; 22(20):10902. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms222010902
Chicago/Turabian Stylevan der Sijde, Fleur, Marjolein Y. V. Homs, Marlies L. van Bekkum, Thierry P. P. van den Bosch, Koop Bosscha, Marc G. Besselink, Bert A. Bonsing, Jan Willem B. de Groot, Thomas M. Karsten, Bas Groot Koerkamp, and et al. 2021. "Serum miR-373-3p and miR-194-5p Are Associated with Early Tumor Progression during FOLFIRINOX Treatment in Pancreatic Cancer Patients: A Prospective Multicenter Study" International Journal of Molecular Sciences 22, no. 20: 10902. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms222010902