
The Role of TNF-α and Anti-TNF-α Agents during Preconception, Pregnancy, and Breastfeeding

 , and
, and
Abstract
:1. The Role of TNF-α in Pregnancy
2. Rheumatic and Gastroenterological Diseases in Pregnancy
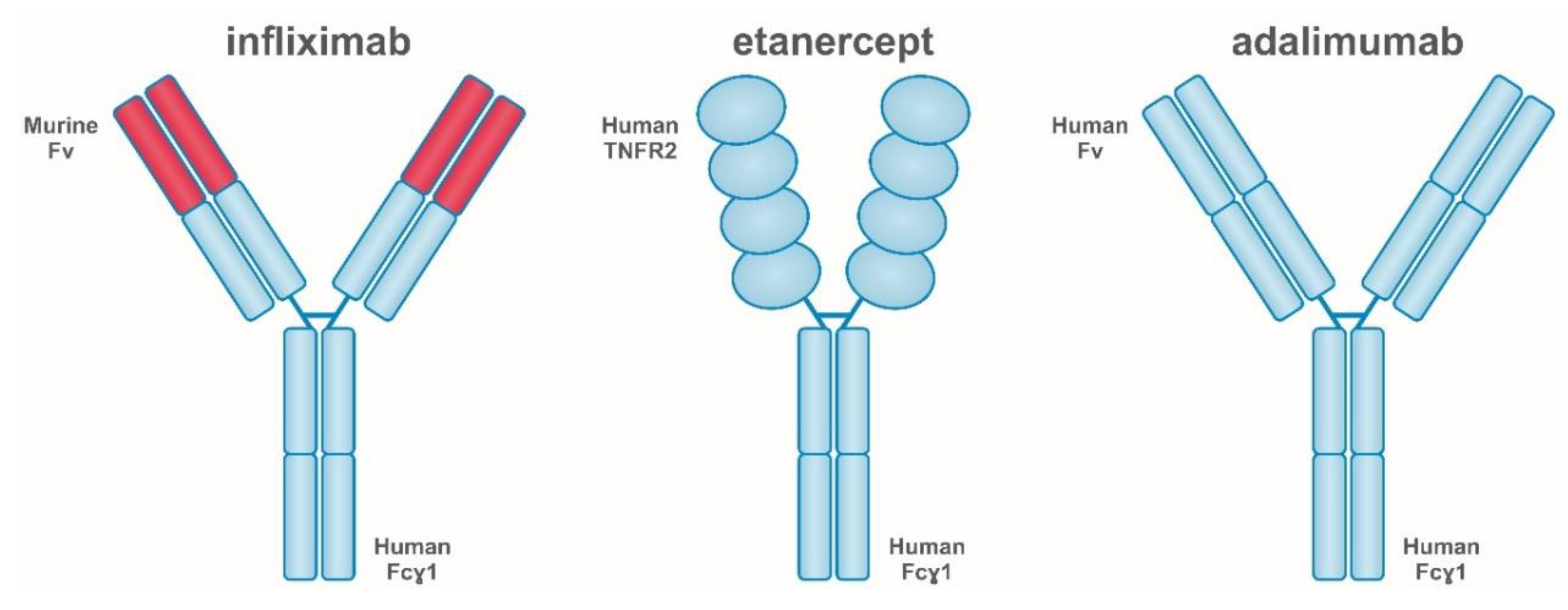
3. Anti-TNF-α Agents
4. Fertility and Biological Therapies
4.1. Men
4.2. Women
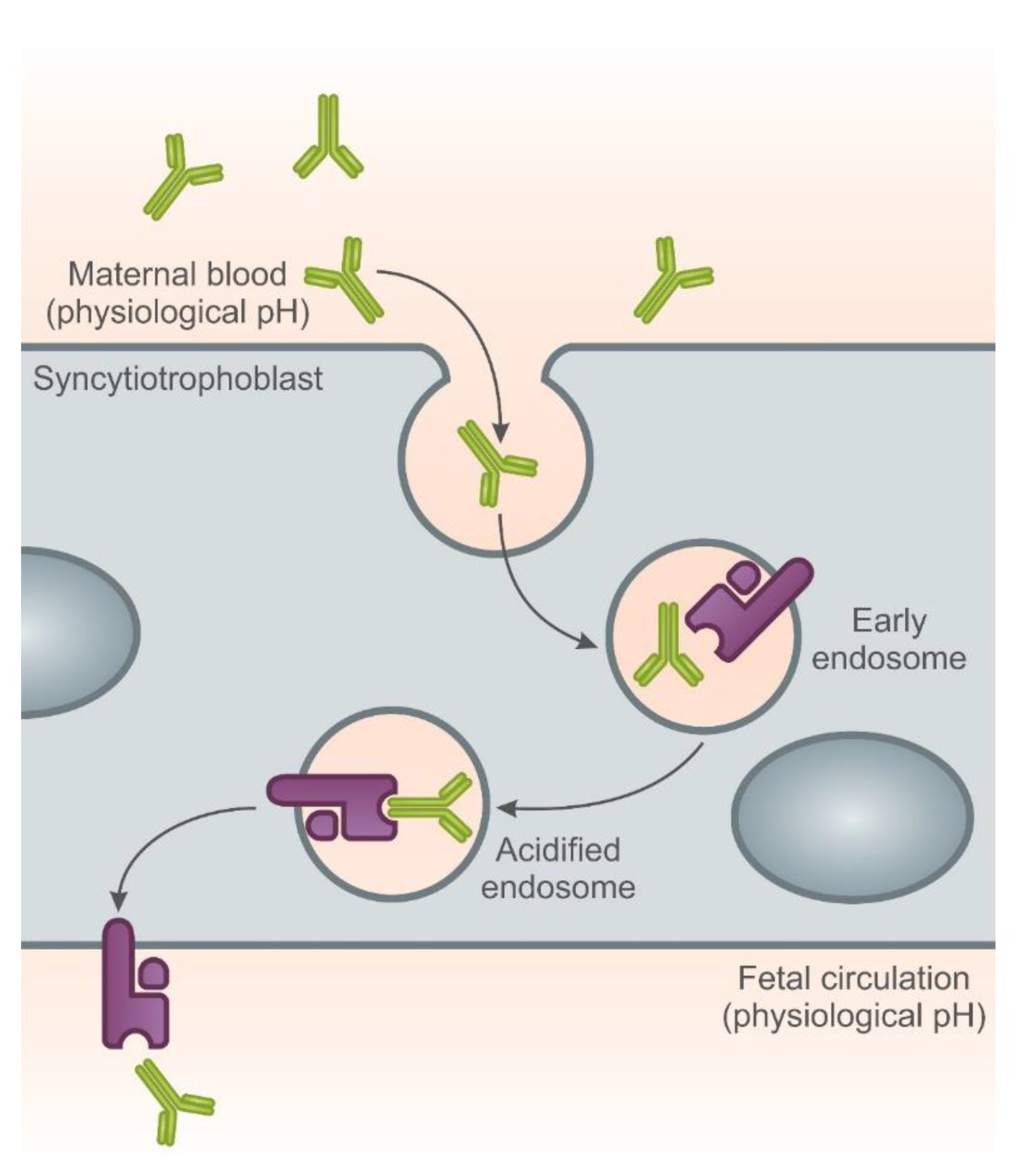
5. Placental Transfer of Biologicals and Maternal/Child Safety during Pregnancy and Breastfeeding
6. Infliximab
7. Adalimumab
8. Etanercept
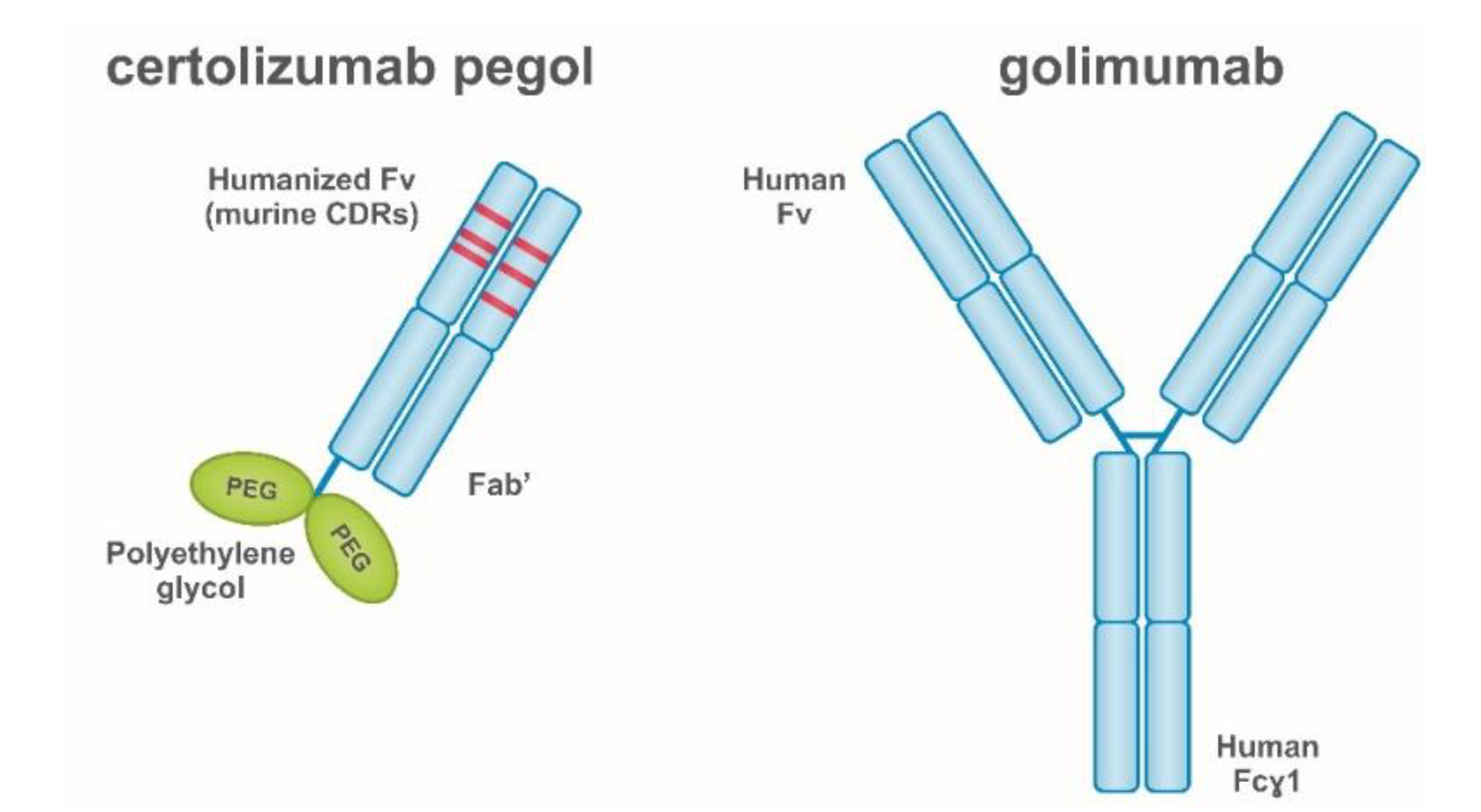
9. Certolizumab
10. Golimumab
11. Anti- TNF-α Therapy and Family Planning—Is It Safe?
12. Recommendations for the Management in Pregnancy-Planning Patients Treated with Anti-TNF-α Drugs Based on the Guidelines of Rheumatology and Gastroenterology Societies
12.1. The Period of Procreation
12.2. Pregnancy
12.3. Breastfeeding
12.4. Vaccinations
13. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| Grade | Quality of Evidence | Meaning |
|---|---|---|
| A | High | We are very confident that the true effect lies close to that of the estimate of the effect |
| B | Moderate | We are moderately confident in the effect estimate. The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different |
| C | Low | Our confidence in the effect estimate is limited. The true effect may be substantially different from the estimate of the effect |
| D | Very low | We have very little confidence in the effect estimate. The true effect is likely to be substantially different from the estimate of the effect |
| A | No. | Levels of Evidence (Treatment Benefits) |
| 1 * | Systematic review of randomized trials or n-of-1 trials | |
| 2 * | Randomized trial or observational study with dramatic effect | |
| 3 * | Non-randomized controlled cohort/follow-up study ** | |
| 4 * | Case-series, case-control studies, or historically controlled studies ** | |
| 5 * | Mechanism-based reasoning | |
| B | No. | Levels of Evidence (Common Treatment Harms) |
| 1 * | Systematic review of randomized trials, systematic review of nested case-control studies, n-of-1 trial with the patient you are raising the question about, or observational study with dramatic effect | |
| 2 * | Individual randomized trial or (exceptionally) observational study with dramatic effect | |
| 3 * | Non-randomized controlled cohort/follow-up study (post-marketing surveillance) provided there are sufficient numbers to rule out a common harm. (For long-term harms, the duration of follow-up must be sufficient) ** | |
| 4 * | Case-series, case-control, or historically controlled studies ** | |
| 5 * | Mechanism-based reasoning | |
| C | Grade | Grade of Recommendation-Meaning |
| A | Consistent level 1 studies | |
| B | Consistent level 2 or 3 studies or extrapolations from level 1 studies | |
| C | Level 4 studies or extrapolations from level 2 or 3 studies | |
| D | Level 5 evidence is troublingly inconsistent or inconclusive in studies of any level |
References
- Moreli, J.B.; Ruocco, A.M.C.; Vernini, J.M.; Rudge, M.V.; Calderon, I.M. Interleukin 10 and tumor necrosis factor-α in pregnancy: Aspects of interest in clinical obstetrics. ISRN Obstet. Gynecol. 2012, 2012, 230742. [Google Scholar] [CrossRef] [Green Version]
- Hunt, J.S.; Chen, H.L.; Miller, L. Tumor necrosis factors: Pivotal components of pregnancy? Biol. Reprod. 1996, 54, 554–562. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Babbage, S.J.; Arkwright, P.D.; Vince, G.S.; Perrey, C.; Pravica, V.; Quenby, S.; Bates, M.; Hutchinson, I.V. Cytokine promoter gene polymorphisms and idiopathic recurrent pregnancy loss. J. Reprod. Immunol. 2001, 51, 21–27. [Google Scholar] [CrossRef]
- Anim-Nyame, N.; Gamble, J.; Sooranna, S.R.; Johnson, M.R.; Steer, P.J. Microvascular permeability is related to circulating levels of tumour necrosis factor-α in pre-eclampsia. Cardiovasc. Res. 2003, 58, 162–169. [Google Scholar] [CrossRef] [Green Version]
- Demir, R.; Yaba, A.; Huppertz, B. Vasculogenesis and angiogenesis in the endometrium during menstrual cycle and implantation. Acta Histochem. 2010, 112, 203–214. [Google Scholar] [CrossRef] [PubMed]
- Saini, V.; Arora, S.; Yadav, A.; Bhattacharjee, J. Cytokines in recurrent pregnancy loss. Clin. Chim. Acta. 2011, 412, 702–708. [Google Scholar] [CrossRef] [PubMed]
- Makhseed, M.; Raghupathy, R.; Azizieh, F.; Omu, A.; Al-Shamali, E.; Ashkanani, L. Th1 and Th2 cytokine profiles in recurrent aborters with successful pregnancy and with subsequent abortions. Hum. Reprod. 2001, 16, 2219–2226. [Google Scholar] [CrossRef]
- Makhseed, M.; Raghupathy, R.; Azizieh, F.; Al-Azemi, M.M.; Hassan, N.A.; Bandar, A. Mitogen-induced cytokine responses of maternal peripheral blood lymphocytes indicate a differential Th-type bias in normal pregnancy and pregnancy failure. Am. J. Reprod. Immunol. 1999, 42, 273–281. [Google Scholar] [CrossRef]
- Raghupathy, R.; Makhseed, M.; Azizieh, F.; Omu, A.; Gupta, M.; Farhat, R. Cytokine production by maternal lymphocytes during normal human pregnancy and in unexplained recurrent spontaneous abortion. Hum. Reprod. 2000, 15, 713–718. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- del Prete, G.; de Carli, M.; Lammel, R.M.; D’Elios, M.M.; Daniel, K.C.; Giusti, B.; Abbate, R.; Romagnani, S. Th1 and Th2 T-helper cells exert opposite regulatory effects on procoagulant activity and tissue factor production by human monocytes. Blood 1995, 86, 250–257. [Google Scholar] [CrossRef] [Green Version]
- Ma, J.; Zhang, X.; He, G.; Yang, C. Association between TNF, IL1B, IL6, IL10 and IFNG polymorphisms and recurrent miscarriage: A case control study. Reprod. Biol. Endocrinol. 2017, 15, 83. [Google Scholar] [CrossRef] [Green Version]
- Wang, T.; Lu, N.; Cui, Y.; Tian, L. Polymorphisms in interleukin genes and their association with the risk of recurrent pregnancy loss. Genes Genet. Syst. 2019, 94, 109–116. [Google Scholar] [CrossRef] [Green Version]
- Zhang, M.; Xu, J.; Bao, X.; Niu, W.; Wang, L.; Du, L.; Zhang, N.; Sun, Y. Association between Genetic Polymorphisms in Interleukin Genes and Recurrent Pregnancy Loss—A Systematic Review and Meta-Analysis. PLoS ONE 2017, 12, e0169891. [Google Scholar] [CrossRef]
- Wang, Q.; Wang, C. Comparison of the expression levels of TNF-α, IL-6, hsCRP and sICAM-1 inflammatory factors, bone mineral density and nutritional status between diabetic and normal pregnant women. Cell Mol. Biol. 2020, 66, 132–137. [Google Scholar] [CrossRef]
- Finan, R.R.; Al-Irhayim, Z.; Mustafa, F.E.; Al-Zaman, I.; Mohammed, F.A.; Al-Khateeb, G.M.; Madan, S.; Issa, A.A.; Almawi, W.Y. Tumor necrosis factor-α polymorphisms in women with idiopathic recurrent miscarriage. J. Reprod. Immunol. 2010, 84, 186–192. [Google Scholar] [CrossRef] [PubMed]
- Ma, X.; Xu, L.J.; Wang, J.; Xian, M.M.; Liu, M. Association of IL-1β and IL-6 gene polymorphisms with recurrent spontaneous abortion in a Chinese Han population. Int. J. Immunogenet. 2012, 39, 15–19. [Google Scholar] [CrossRef]
- Christian, L.M.; Porter, K. Longitudinal changes in serum proinflammatory markers across pregnancy and postpartum: Effects of maternal body mass index. Cytokine 2014, 70, 134–140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pantham, P.; Aye, I.L.; Powell, T.L. Inflammation in maternal obesity and gestational diabetes mellitus. Placenta 2015, 36, 709–715. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peraçoli, J.C.; Rudge, M.V.; Peraçoli, M.T. Tumor necrosis factor-α in gestation and puerperium of women with gestational hypertension and pre-eclampsia. Am. J. Reprod. Immunol. 2007, 57, 177–185. [Google Scholar] [CrossRef] [PubMed]
- Bauer, S.; Pollheimer, J.; Hartmann, J.; Husslein, P.; Aplin, J.D.; Knöfler, M. Tumor necrosis factor-α inhibits trophoblast migration through elevation of plasminogen activator inhibitor-1 in first-trimester villous explant cultures. J. Clin. Endocrinol. Metab. 2004, 89, 812–822. [Google Scholar] [CrossRef] [PubMed]
- Leisser, C.; Saleh, L.; Haider, S.; Husslein, H.; Sonderegger, S.; Knöfler, M. Tumour necrosis factor-α impairs chorionic gonadotrophin β-subunit expression and cell fusion of human villous cytotrophoblast. Mol. Hum. Reprod. 2006, 12, 601–609. [Google Scholar] [CrossRef]
- Aldo, P.B.; Racicot, K.; Craviero, V.; Guller, S.; Romero, R.; Mor, G. Trophoblast induces monocyte differentiation into CD14+/CD16+ macrophages. Am. J. Reprod. Immunol. 2014, 72, 270–284. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ramhorst, R.; Fraccaroli, L.; Aldo, P.; Alvero, A.B.; Cardenas, I.; Leirós, C.P.; Mor, G. Modulation and recruitment of inducible regulatory T cells by first trimester trophoblast cells. Am. J. Reprod. Immunol. 2012, 67, 17–27. [Google Scholar] [CrossRef] [Green Version]
- PrabhuDas, M.; Bonney, E.; Caron, K.; Dey, S.; Erlebacher, A.; Fazleabas, A.; Fisher, S.; Golos, T.; Matzuk, M.; McCune, J.M.; et al. Immune mechanisms at the maternal-fetal interface: Perspectives and challenges. Nat. Immunol. 2015, 16, 328–334. [Google Scholar] [CrossRef]
- Catalano, P.; deMouzon, S.H. Maternal obesity and metabolic risk to the offspring: Why lifestyle interventions may have not achieved the desired outcomes. Int. J. Obes. 2015, 39, 642–649. [Google Scholar] [CrossRef] [Green Version]
- Desoye, G.; van Poppel, M. The feto-placental dialogue and diabesity. Best Pract. Res. Clin. Obstet. Gynaecol. 2015, 29, 15–23. [Google Scholar] [CrossRef] [PubMed]
- Siwetz, M.; Blaschitz, A.; El-Heliebi, A.; Hiden, U.; Desoye, G.; Huppertz, B.; Gauster, M. TNF-α alters the inflammatory secretion profile of human first trimester placenta 1ear. Lab. Investig. 2016, 96, 428–438. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jethwa, H.; Lam, S.; Smith, C.; Giles, I. Does Rheumatoid Arthritis Really Improve During Pregnancy? A Systematic Review and Metaanalysis. J. Rheumatol. 2019, 46, 245–250. [Google Scholar] [CrossRef]
- Märker-Hermann, E.; Fischer-Betz, R. Rheumatic diseases and pregnancy. Curr. Opin. Obstet. Gynecol. 2010, 22, 458–465. [Google Scholar] [CrossRef] [PubMed]
- Skomsvoll, J.F.; Ostensen, M.; Irgens, L.M.; Baste, V. Obstetrical and neonatal outcome in pregnant patients with rheumatic disease. Scand. J. Rheumatol. Suppl. 1998, 107, 109–112. [Google Scholar] [CrossRef] [PubMed]
- Bowden, A.P.; Barrett, J.H.; Fallow, W.; Silman, A.J. Women with inflammatory polyarthritis have babies of lower birth weight. J. Rheumatol. 2001, 28, 355–359. [Google Scholar] [PubMed]
- Chambers, C.D.; Johnson, D.L.; Jones, K.L. Pregnancy outcome in women exposed to anti-TNF-α medications: The OTIS rheumatoid arthritis pregnancy study. Arthritis Rheum. 2004, 50, S479. [Google Scholar]
- Eudy, A.M.; McDaniel, G.; Clowse, M.E. Pregnancy outcomes, fertility, and family planning in women with psoriatic arthritis. Obstet. Med. 2020, 13, 70–75. [Google Scholar] [CrossRef]
- Giovannopoulou, E.; Gkasdaris, G.; Kapetanakis, S.; Kontomanolis, E. Ankylosing Spondylitis and Pregnancy: A Literature Review. Curr. Rheumatol. Rev. 2017, 13, 162–169. [Google Scholar] [CrossRef]
- Østensen, M.; Husby, G. Ankylosing spondylitis and pregnancy. Rheum. Dis. Clin. N. Am. 1989, 15, 241–254. [Google Scholar]
- Østensen, M.; Fuhrer, L.; Mathieu, R.; Seitz, M.; Villiger, P.M. A prospective study of pregnant patients with rheumatoid arthritis and ankylosing spondylitis using validated clinical instruments. Ann. Rheum. Dis. 2004, 63, 1212–1217. [Google Scholar] [CrossRef] [Green Version]
- Zbinden, A.; van den Brandt, S.; Østensen, M.; Villiger, P.M.; Förger, F. Risk for adverse pregnancy outcome in axial spondyloarthritis and rheumatoid arthritis: Disease activity matters. Rheumatology 2018, 57, 1235–1242. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wright, G.C.; Kaine, J.; Deodhar, A. Understanding differences between men and women with axial spondyloarthritis. Semin. Arthritis Rheum. 2020, 50, 687–694. [Google Scholar] [CrossRef]
- van den Brandt, S.; Zbinden, A.; Baeten, D.; Villiger, P.M.; Østensen, M.; Förger, F. Risk factors for flare and treatment of disease flares during pregnancy in rheumatoid arthritis and axial spondyloarthritis patients. Arthritis Res. Ther. 2017, 19, 64. [Google Scholar] [CrossRef] [Green Version]
- Ursin, K.; Lydersen, S.; Skomsvoll, J.F.; Wallenius, M. Disease activity during and after pregnancy in women with axial spondyloarthritis: A prospective multicentre study. Rheumatology 2018, 57, 1064–1071. [Google Scholar] [CrossRef] [Green Version]
- Pedersen, N.; Bortoli, A.; Duricova, D.; D’Inca, R.; Panelli, M.R.; Gisbert, J.P.; Zoli, G.; López-Sanromán, A.; Castiglione, F.; Riegler, G.; et al. The course of inflammatory bowel disease during pregnancy and postpartum: A prospective European ECCO-EpiCom Study of 209 pregnant women. Aliment. Pharmacol. Ther. 2013, 38, 501–512. [Google Scholar] [CrossRef]
- Mahadevan, U.; Martin, C.F.; Sandler, R.; Kane, S.V.; Dubinsky, M.; Lewis, J.D.; Sandborn, W.J.; Sands, B.E. 865 PIANO: A 1000 patient prospective registry of pregnancy outcomes in women with IBD exposed toimmunomodulators and biologic therapy. Gastroenterology 2012, 142, 149. [Google Scholar] [CrossRef]
- Nasef, N.A.; Ferguson, L.R. Inflammatory bowel disease and pregnancy: Overlapping pathways. Transl. Res. 2012, 160, 65–83. [Google Scholar] [CrossRef]
- Mahadevan, U.; Sandborn, W.J.; Li, D.K.; Hakimian, S.; Kane, S.; Corley, D.A. Pregnancy outcomes in women with inflammatory bowel disease: A large community-based study from Northern California. Gastroenterology 2007, 133, 1106–1112. [Google Scholar] [CrossRef]
- Julsgaard, M.; Nørgaard, M.; Hvas, C.L.; Grosen, A.; Hasseriis, S.; Christensen, L.A. Self-reported adherence to medical treatment, breastfeeding behaviour, and disease activity during the postpartum period in women with Crohn’s disease. Scand. J. Gastroenterol. 2014, 49, 958–966. [Google Scholar] [CrossRef]
- Ujihara, M.; Ando, T.; Ishiguro, K.; Maeda, O.; Watanabe, O.; Hirayama, Y.; Morise, K.; Maeda, K.; Matsushita, M.; Miyahara, R.; et al. Importance of appropriate pharmaceutical management in pregnant women with ulcerative colitis. BMC Res. Notes 2013, 6, 210. [Google Scholar] [CrossRef] [Green Version]
- Mouyis, M.; Flint, J.D.; Giles, I.P. Safety of anti-rheumatic drugs in men trying to conceive: A systematic review and analysis of published evidence. Semin. Arthritis Rheum. 2019, 48, 911–920. [Google Scholar] [CrossRef]
- Available online: https://ec.europa.eu/health/documents/community-register/2004/200409208252/anx_8252_pl.pdf (accessed on 18 February 2021).
- Available online: https://ec.europa.eu/health/documents/community-register/2007/2007111934690/anx_34690_pl.pdf (accessed on 18 February 2021).
- Available online: https://ec.europa.eu/health/documents/community-register/2007/2007100932109/anx_32109_pl.pdf (accessed on 18 February 2021).
- Available online: https://ec.europa.eu/health/documents/community-register/2017/20170428137807/anx_137807_pl.pdf (accessed on 18 February 2021).
- Available online: https://www.ema.europa.eu/en/documents/product-information/simponi-epar-product-information_pl.pdf (accessed on 18 February 2021).
- Riccioli, A.; Starace, D.; D’Alessio, A.; Starace, G.; Padula, F.; de Cesaris, P.; Filippini, A.; Ziparo, E. TNF -a and IFN-y regulate the expression and function of the Fas system in the seminiferous epithelium. J. Immunol. 2000, 165, 743–749. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, M.W.; Xia, W.; Mruk, D.D.; Wang, C.Q.; Yan, H.H.; Siu, M.K.; Lui, W.Y.; Lee, W.M.; Cheng, C.Y. Tumor necrosis factor α reversibly disrupts the blood-testis barrier and impairs Sertoli-germ cell adhesion in the seminiferous epithelium of adult rat testes. J. Endocrinol. 2006, 190, 313–329. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Loveland, K.L.; Klein, B.; Pueschl, D.; Indumathy, S.; Bergmann, M.; Loveland, B.E.; Hedger, M.P.; Schuppe, H.C. Cytokines in Male Fertility and Reproductive Pathologies: Immunoregulation and Beyond. Front. Endocrinol. 2017, 8, 307. [Google Scholar] [CrossRef]
- Suominen, J.S.; Yanyan, W.; Kaipia, A.; Toppari, J. Tumor necrosis factor-α (TNF -a) promotes cell survival during spermatogenesis, and this effect can be blocked by infliximab, a TNF -a antagonist. Eur. J. Endocrinol. 2004, 151, 629–640. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, Y.C.; Richburg, J.H. Characterization of the role of tumor necrosis factor apoptosis inducing ligand (TRAIL) in spermatogenesis through the evaluation of trail gene-deficient mice. PLoS ONE 2014, 9, e93926. [Google Scholar] [CrossRef] [PubMed]
- O’Bryan, M.K.; Hedger, M.P. Inflammatory networks in the control of spermatogenesis: Chronic inflammation in an immunologically privileged tissue? Adv. Exp. Med. Biol. 2008, 636, 92–114. [Google Scholar] [CrossRef] [PubMed]
- Cooley, L.F.; Wren, J.; Keeter, M.K.; Lam, I.; Bennett, N.; Brannigan, R.E. Anti-TNF agents and potential effects on male fertility: Are men being counseled? BMC Urol. 2020, 20, 111. [Google Scholar] [CrossRef] [PubMed]
- Micu, M.C.; Micu, R.; Surd, S.; Girlovanu, M.; Bolboaca, S.D.; Ostensen, M. TNF -α inhibitors do not impair sperm quality in males with ankylosing spondylitis after short-term or long-term treatment. Rheumatology 2014, 53, 1250–1255. [Google Scholar] [CrossRef] [Green Version]
- Montagna, G.L.; Malesci, D.; Buono, R.; Valentini, G. Asthenoazoospermia in patients receiving anti-tumour necrosis factor α agents. Ann. Rheum. Dis. 2005, 64, 1667. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mahadevan, U.; Terdiman, J.P.; Aron, J.; Jacobsohn, S.; Turek, P. Infliximab and semen quality in men with inflammatory bowel disease. Inflamm. Bowel Dis. 2005, 11, 395–399. [Google Scholar] [CrossRef] [PubMed]
- Serghini, M.; Fekih, M.; Karoui, S.; Ben Mustapha, N.; Kallel, L.; Matri, S.; Boubaker, J.; Filali, A. Fertilité et maladies inflammatoires chroniques de l’intestin [Fertility and inflammatory bowel diseases]. Tunis. Med. 2010, 88, 623–628. [Google Scholar]
- Mahadevan, U. Fertility and pregnancy in the patient with inflammatory bowel disease. Gut 2006, 55, 1198–1206. [Google Scholar] [CrossRef] [Green Version]
- Wildi, L.M.; Haraoui, B. Reversible male infertility under treatment with an anti-TNFα agent: A case report. Ann. Rheum. Dis. 2012, 71, 473–474. [Google Scholar] [CrossRef] [PubMed]
- Semet, M.; Paci, M.; Saïas-Magnan, J.; Metzler-Guillemain, C.; Boissier, R.; Lejeune, H.; Perrin, J. The impact of drugs on male fertility: A review. Andrology 2017, 5, 640–663. [Google Scholar] [CrossRef]
- Younis, S.; Rimar, D.; Slobodin, G.; Boulman, N.; Rozenbaum, M.; Rosner, I. Effect of infliximab on male fertility: Comment on the article “Fertility in male patients with seronegative spondyloarthropathies treated with infliximab” by Saougou et al., Joint Bone Spine 2013; 80, 34–37. Jt. Bone Spine 2014, 81, 102–103. [Google Scholar] [CrossRef] [PubMed]
- Blotière, P.O.; Rudant, J.; Barré, A.; Racine, A.; Weill, A.; Peyrin-Biroulet, L.; Carbonnel, F.; Alla, F. Conditions of prescription of anti-TNF agents in newly treated patients with inflammatory bowel disease in France (2011–2013). Dig. Liver Dis. 2016, 48, 620–625. [Google Scholar] [CrossRef] [PubMed]
- Curtis, J.R.; Singh, J.A. Use of biologics in rheumatoid arthritis: Current and emerging paradigms of care. Clin. Ther. 2011, 33, 679–707. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Knowles, S.R.; Gass, C.; Macrae, F. Illness perceptions in IBD influence psychological status, sexual health and satisfaction, body image and relational functioning: A preliminary exploration using Structural Equation Modeling. J. Crohn Colitis. 2013, 7, e344–e350. [Google Scholar] [CrossRef]
- Timmer, A.; Bauer, A.; Kemptner, D.; Fürst, A.; Rogler, G. Determinants of male sexual function in inflammatory bowel disease: A survey-based cross-sectional analysis in 280 men. Inflamm. Bowel Dis. 2007, 13, 1236–1243. [Google Scholar] [CrossRef]
- Liu, Y.F.; Dong, H.; Chen, Z.; Wang, Y.U.; Tu, S.H. Impact of ankylosing spondylitis on sexual function: A systematic review and meta-analysis. Exp. Ther. Med. 2015, 9, 1501–1507. [Google Scholar] [CrossRef] [Green Version]
- Baillargeon, J.; Al Snih, S.; Raji, M.A.; Urban, R.J.; Sharma, G.; Sheffield-Moore, M.; Lopez, D.S.; Baillargeon, G.; Kuo, Y.F. Hypogonadism and the risk of rheumatic autoimmune disease. Clin. Rheumatol. 2016, 35, 2983–2987. [Google Scholar] [CrossRef] [PubMed]
- Cutolo, M.; Sulli, A.; Capellino, S.; Villaggio, B.; Montagna, P.; Pizzorni, C.; Paolino, S.; Seriolo, B.; Felli, L.; Straub, R.H. Anti-TNF and sex hormones. Ann. N. Y. Acad. Sci. 2006, 1069, 391–400. [Google Scholar] [CrossRef]
- Almeida, B.P.; Saad, C.G.; Souza, F.H.; Moraes, J.C.; Nukumizu, L.A.; Viana, V.S.; Bonfá, E.; Silva, C.A. Testicular Sertoli cell function in ankylosing spondylitis. Clin. Rheumatol. 2013, 32, 1075–1079. [Google Scholar] [CrossRef]
- Rezvani, A.; Ozaras, N. Infertility improved by etanercept in ankylosing spondylitis. Indian J. Pharmacol. 2008, 40, 276–277. [Google Scholar] [CrossRef] [PubMed]
- Sammaritano, L.R.; Bermas, B.L.; Chakravarty, E.E.; Chambers, C.; Clowse, M.E.B.; Lockshin, M.D.; Marder, W.; Guyatt, G.; Branch, D.W.; Buyon, J.; et al. 2020 American College of Rheumatology Guideline for the Management of Reproductive Health in Rheumatic and Musculoskeletal Diseases. Arthritis Care Res. 2020, 72, 461–488. [Google Scholar] [CrossRef]
- Flint, J.; Panchal, S.; Hurrell, A.; van de Venne, M.; Gayed, M.; Schreiber, K.; Arthanari, S.; Cunningham, J.; Flanders, L.; Moore, L.; et al. BSR and BHPR Standards, Guidelines and Audit Working Group. BSR and BHPR guideline on prescribing drugs in pregnancy and breastfeeding-Part I: Standard and biologic disease modifying anti-rheumatic drugs and corticosteroids. Rheumatology 2016, 55, 1693–1697. [Google Scholar] [CrossRef] [Green Version]
- Tavernier, N.; Fumery, M.; Peyrin-Biroulet, L.; Colombel, J.F.; Gower-Rousseau, C. Systematic review: Fertility in non-surgically treated inflammatory bowel disease. Aliment. Pharmacol. Ther. 2013, 38, 847–853. [Google Scholar] [CrossRef]
- Heetun, Z.S.; Byrnes, C.; Neary, P.; O’Morain, C. Review article: Reproduction in the patient with inflammatory bowel disease. Aliment. Pharmacol. Ther. 2007, 26, 513–533. [Google Scholar] [CrossRef] [PubMed]
- Palomba, S.; Sereni, G.; Falbo, A.; Beltrami, M.; Lombardini, S.; Boni, M.C.; Fornaciari, G.; Sassatelli, R.; La Sala, G.B. Inflammatory bowel diseases and human reproduction: A comprehensive evidence-based review. World J. Gastroenterol. 2014, 20, 7123–7136. [Google Scholar] [CrossRef]
- Mahadevan, U.; McConnell, R.A.; Chambers, C.D. Drug Safety and Risk of Adverse Outcomes for Pregnant Patients with Inflammatory Bowel Disease. Gastroenterology 2017, 152, 451–462.e2. [Google Scholar] [CrossRef] [PubMed]
- Ban, L.; Tata, L.J.; Humes, D.J.; Fiaschi, L.; Card, T. Decreased fertility rates in 9639 women diagnosed with inflammatory bowel disease: A United Kingdom population-based cohort study. Aliment. Pharmacol. Ther. 2015, 42, 855–866. [Google Scholar] [CrossRef]
- Cornish, J.; Tan, E.; Teare, J.; Teoh, T.G.; Rai, R.; Clark, S.K.; Tekkis, P.P. A meta-analysis on the influence of inflammatory bowel disease on pregnancy. Gut 2007, 56, 830–837. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brouwer, J.; Hazes, J.M.; Laven, J.S.; Dolhain, R.J. Fertility in women with rheumatoid arthritis: Influence of disease activity and medication. Ann. Rheum. Dis. 2015, 74, 1836–1841. [Google Scholar] [CrossRef] [PubMed]
- de Jong, P.H.; Dolhain, R.J. Fertility, Pregnancy, and Lactation in Rheumatoid Arthritis. Rheum. Dis. Clin. N. Am. 2017, 43, 227–237. [Google Scholar] [CrossRef] [PubMed]
- Schulze, H.; Esters, P.; Dignass, A. Review article: The management of Crohn’s disease and ulcerative colitis during pregnancy and lactation. Aliment. Pharmacol. Ther. 2014, 40, 991–1008. [Google Scholar] [CrossRef]
- Smeele, H.T.W.; Dolhian, R.J.E.M. Current perspectives on fertility, pregnancy and childbirth in patients with Rheumatoid Arthritis. Semin. Arthritis Rheum. 2019, 49, S32–S35. [Google Scholar] [CrossRef] [PubMed]
- Brouwer, J.; Fleurbaaij, R.; Hazes, J.M.W.; Dolhain, R.J.E.M.; Laven, J.S.E. Subfertility in Women with Rheumatoid Arthritis and the Outcome of Fertility Assessments. Arthritis Care Res. 2017, 69, 1142–1149. [Google Scholar] [CrossRef] [Green Version]
- Leach, J.L.; Sedmak, D.D.; Osborne, J.M.; Rahill, B.; Lairmore, M.D.; Anderson, C.L. Isolation from human placenta of the IgG transporter, FcRn, and localization to the syncytiotrophoblast: Implications for maternal-fetal antibody transport. J. Immunol. 1996, 157, 3317–3322. [Google Scholar]
- Roberts, D.M.; Guenthert, M.; Rodewald, R. Isolation and characterization of the Fc receptor from the fetal yolk sac of the rat. J. Cell Biol. 1990, 111 Pt 1, 1867–1876. [Google Scholar] [CrossRef] [Green Version]
- Simister, N.E.; Story, C.M. Human placental Fc receptors and the transmission of antibodies from mother to fetus. J. Reprod. Immunol. 1997, 37. [Google Scholar] [CrossRef]
- Ober, R.J.; Martinez, C.; Lai, X.; Zhou, J.; Ward, E.S. Exocytosis of IgG as mediated by the receptor, FcRn: An analysis at the single-molecule level. Proc. Natl. Acad. Sci. USA 2004, 101, 11076–11081. [Google Scholar] [CrossRef] [Green Version]
- Junghans, R.P.; Anderson, C.L. The protection receptor for IgG catabolism is the beta2-microglobulin-containing neonatal intestinal transport receptor. Proc. Natl. Acad. Sci. USA 1996, 93, 5512–5516. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ghetie, V.; Popov, S.; Borvak, J.; Radu, C.; Matesoi, D.; Medesan, C.; Ober, R.J.; Ward, E.S. Increasing the serum persistence of an IgG fragment by random mutagenesis. Nat. Biotechnol. 1997, 15, 637–640. [Google Scholar] [CrossRef]
- Mahadevan, U.; Wolf, D.C.; Dubinsky, M.; Cortot, A.; Lee, S.D.; Siegel, C.A.; Ullman, T.; Glover, S.; Valentine, J.F.; Rubin, D.T.; et al. Placental transfer of anti-tumor necrosis factor agents in pregnant patients with inflammatory bowel disease. Clin. Gastroenterol. Hepatol. 2013, 11, 286–292. [Google Scholar] [CrossRef] [Green Version]
- Julsgaard, M.; Christensen, L.A.; Gibson, P.R.; Gearry, R.B.; Fallingborg, J.; Hvas, C.L.; Bibby, B.M.; Uldbjerg, N.; Connell, W.R.; Rosella, O.; et al. Concentrations of Adalimumab and Infliximab in Mothers and Newborns, and Effects on Infection. Gastroenterology 2016, 151, 110–119. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seow, C.H.; Leung, Y.; Casteele, N.V.; Afshar, E.E.; Tanyingoh, D.; Bindra, G.; Stewart, M.J.; Beck, P.L.; Kaplan, G.G.; Ghosh, S.; et al. The effects of pregnancy on the pharmacokinetics of infliximab and adalimumab in inflammatory bowel disease. Aliment. Pharmacol. Ther. 2017, 45, 1329–1338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McConnell, R.A.; Mahadevan, U. Pregnancy and the Patient with Inflammatory Bowel Disease: Fertility, Treatment, Delivery, and Complications. Gastroenterol. Clin. North Am. 2016, 45, 285–301. [Google Scholar] [CrossRef]
- Deepak, P.; Stobaugh, D.J. Maternal and foetal adverse events with tumour necrosis factor-alpha inhibitors in inflammatory bowel disease. Aliment. Pharmacol. Ther. 2014, 40, 1035–1043. [Google Scholar] [CrossRef]
- Schnitzler, F.; Fidder, H.; Ferrante, M.; Ballet, V.; Noman, M.; van Assche, G.; Spitz, B.; Hoffman, I.; van Steen, K.; Vermeire, S.; et al. Outcome of pregnancy in women with inflammatory bowel disease treated with antitumor necrosis factor therapy. Inflamm. Bowel Dis. 2011, 17, 1846–1854. [Google Scholar] [CrossRef] [PubMed]
- Seirafi, M.; de Vroey, B.; Amiot, A.; Seksik, P.; Roblin, X.; Allez, M.; Peyrin-Biroulet, L.; Marteau, P.; Cadiot, G.; Laharie, D.; et al. Factors associated with pregnancy outcome in anti-TNF treated women with inflammatory bowel disease. Aliment. Pharmacol. Ther. 2014, 40, 363–373. [Google Scholar] [CrossRef] [PubMed]
- Shihab, Z.; Yeomans, N.D.; de Cruz, P. Anti-Tumour Necrosis Factor α Therapies and Inflammatory Bowel Disease Pregnancy Outcomes: A Meta-analysis. J. Crohns Colitis. 2016, 10, 979–988. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Narula, N.; Al-Dabbagh, R.; Dhillon, A.; Sands, B.E.; Marshall, J.K. Anti-TNFα therapies are safe during pregnancy in women with inflammatory bowel disease: A systematic review and meta-analysis. Inflamm. Bowel Dis. 2014, 20, 1862–1869. [Google Scholar] [CrossRef]
- Magro, F.; Gionchetti, P.; Eliakim, R.; Ardizzone, S.; Armuzzi, A.; Barreiro-de Acosta, M.; Burisch, J.; Gecse, K.B.; Hart, A.L.; Hindryckx, P.; et al. Third European Evidence-based Consensus on Diagnosis and Management of Ulcerative Colitis. Part 1: Definitions, Diagnosis, Extra-intestinal Manifestations, Pregnancy, Cancer Surveillance, Surgery, and Ileo-anal Pouch Disorders. J. Crohns Colitis. 2017, 11, 649–670. [Google Scholar] [CrossRef]
- Katz, J.A.; Antoni, C.; Keenan, G.F.; Smith, D.E.; Jacobs, S.J.; Lichtenstein, G.R. Outcome of pregnancy in women receiving infliximab for the treatment of Crohn’s disease and rheumatoid arthritis. Am. J. Gastroenterol. 2004, 99, 2385–2392. [Google Scholar] [CrossRef]
- van der Giessen, J.; Binyamin, D.; Belogolovski, A.; Frishman, S.; Tenenbaum-Gavish, K.; Hadar, E.; Louzoun, Y.; Peppelenbosch, M.P.; van der Woude, C.J.; Koren, O.; et al. Modulation of cytokine patterns and microbiome during pregnancy in IBD. Gut 2020, 69, 473–486. [Google Scholar] [CrossRef]
- Lichtenstein, G.R.; Feagan, B.G.; Cohen, R.D.; Salzberg, B.A.; Diamond, R.H.; Price, S.; Langholff, W.; Londhe, A.; Sandborn, W.J. Serious infection and mortality in patients with Crohn’s disease: More than 5 years of follow-up in the TREAT™ registry. Am. J. Gastroenterol. 2012, 107, 1409–1422. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luu, M.; Benzenine, E.; Doret, M.; Michiels, C.; Barkun, A.; Degand, T.; Quantin, C.; Bardou, M. Continuous Anti-TNFα Use throughout Pregnancy: Possible Complications for the Mother but Not for the Fetus. A Retrospective Cohort on the French National Health Insurance Database (EVASION). Am. J. Gastroenterol. 2018, 113, 1669–1677. [Google Scholar] [CrossRef] [PubMed]
- Truta, B.; Canner, J.; Efron, J.; Safar, B. The effect of intrauteri exposure to biologics: Two years follow up. Gastroenterology 2016, 150, S773. [Google Scholar] [CrossRef]
- Mahadevan, U.; Martin, C.F.; Chambers, C.; Kane, S.V.; Dubinsky, M.; Sandborn, W.; Sands, B.E. Achievement of developmental milestones among ofspring of women with infammatory bowel disease: The PIANO Registry. Gastroenterology 2014, 146, S-14. [Google Scholar] [CrossRef]
- Chaparro, M.; Verreth, A.; Lobaton, T.; Gravito-Soares, E.; Julsgaard, M.; Savarino, E.; Magro, F.; Biron, A.I.; Lopez-Serrano, P.; Casanova, M.J.; et al. Long-Term Safety of in Utero Exposure to Anti-TNFα Drugs for the Treatment of Inflammatory Bowel Disease: Results from the Multicenter European TEDDY Study. Am. J. Gastroenterol. 2018, 113, 396–403. [Google Scholar] [CrossRef] [PubMed]
- Gisbert, J.P.; Chaparro, M. Safety of anti-TNF agents during pregnancy and breastfeeding in women with inflammatory bowel disease. Am. J. Gastroenterol. 2013, 108, 1426–1438. [Google Scholar] [CrossRef]
- Matro, R.; Martin, C.F.; Wolf, D.; Shah, S.A.; Mahadevan, U. Exposure Concentrations of Infants Breastfed by Women Receiving Biologic Therapies for Inflammatory Bowel Diseases and Effects of Breastfeeding on Infections and Development. Gastroenterology 2018, 155, 696–704. [Google Scholar] [CrossRef] [Green Version]
- Clowse, M.E.B.; Scheuerle, A.E.; Chambers, C.; Afzali, A.; Kimball, A.B.; Cush, J.J.; Cooney, M.; Shaughnessy, L.; Vanderkelen, M.; Förger, F. Pregnancy Outcomes after Exposure to Certolizumab Pegol: Updated Results from a Pharmacovigilance Safety Database. Arthritis Rheumatol. 2018, 70, 1399–1407. [Google Scholar] [CrossRef]
- Suzuki, T.; Ishii-Watabe, A.; Tada, M.; Kobayashi, T.; Kanayasu-Toyoda, T.; Kawanishi, T.; Yamaguchi, T. Importance of neonatal FcR in regulating the serum half-life of therapeutic proteins containing the Fc domain of human IgG1: A comparative study of the affinity of monoclonal antibodies and Fc-fusion proteins to human neonatal FcR. J. Immunol. 2010, 184, 1968–1976. [Google Scholar] [CrossRef] [PubMed]
- Ben-Horin, S.; Yavzori, M.; Katz, L.; Picard, O.; Fudim, E.; Chowers, Y.; Lang, A. Adalimumab level in breast milk of a nursing mother. Clin. Gastroenterol. Hepatol. 2010, 8, 475–476. [Google Scholar] [CrossRef]
- Levy, R.A.; de Jesús, G.R.; de Jesús, N.R.; Klumb, E.M. Critical review of the current recommendations for the treatment of systemic inflammatory rheumatic diseases during pregnancy and lactation. Autoimmun. Rev. 2016, 15, 955–963. [Google Scholar] [CrossRef]
- Porter, C.; Armstrong-Fisher, S.; Kopotsha, T.; Smith, B.; Baker, T.; Kevorkian, L.; Nesbitt, A. Certolizumab pegol does not bind the neonatal Fc receptor (FcRn): Consequences for FcRn-mediated in vitro transcytosis and ex vivo human placental transfer. J. Reprod. Immunol. 2016, 116, 7–12. [Google Scholar] [CrossRef] [Green Version]
- Mariette, X.; Förger, F.; Abraham, B.; Flynn, A.D.; Moltó, A.; Flipo, R.M.; van Tubergen, A.; Shaughnessy, L.; Simpson, J.; Teil, M.; et al. Lack of placental transfer of certolizumab pegol during pregnancy: Results from CRIB, a prospective, postmarketing, pharmacokinetic study. Ann. Rheum. Dis. 2018, 77, 228–233. [Google Scholar] [CrossRef]
- Clowse, M.E.; Förger, F.; Hwang, C.; Thorp, J.; Dolhain, R.J.; van Tubergen, A.; Shaughnessy, L.; Simpson, J.; Teil, M.; Toublanc, N.; et al. Minimal to no transfer of certolizumab pegol into breast milk: Results from CRADLE, a prospective, postmarketing, multicentre, pharmacokinetic study. Ann. Rheum. Dis. 2017, 76, 1890–1896. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abhyankar, A.; Ham, M.; Moss, A.C. Meta-analysis: The impact of disease activity at conception on disease activity during pregnancy in patients with inflammatory bowel disease. Aliment. Pharmacol. Ther. 2013, 38, 460–466. [Google Scholar] [CrossRef] [Green Version]
- Reddy, D.; Murphy, S.J.; Kane, S.V.; Present, D.H.; Kornbluth, A.A. Relapses of inflammatory bowel disease during pregnancy: In-hospital management and birth outcomes. Am. J. Gastroenterol. 2008, 103, 1203–1239. [Google Scholar] [CrossRef] [PubMed]
- Korelitz, B.I. Inflammatory bowel disease and pregnancy. Gastroenterol. Clin. N. Am. 1998, 27, 213–224. [Google Scholar] [CrossRef]
- Bortoli, A.; Saibeni, S.; Tatarella, M.; Prada, A.; Beretta, L.; Rivolta, R.; Politi, P.; Ravelli, P.; Imperiali, G.; Colombo, E.; et al. Study Group for Inflammatory Bowel Diseases GSMII. Pregnancy before and after the diagnosis of inflammatory bowel diseases: Retrospective case-control study. J. Gastroenterol. Hepatol. 2007, 22, 542–549. [Google Scholar] [CrossRef]
- Torres, J.; Boyapati, R.K.; Kennedy, N.A.; Louis, E.; Colombel, J.F.; Satsangi, J. Systematic Review of Effects of Withdrawal of Immunomodulators or Biologic Agents from Patients with Inflammatory Bowel Disease. Gastroenterology 2015, 149, 1716–1730. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reinisch, W.; Sandborn, W.J.; Rutgeerts, P.; Feagan, B.G.; Rachmilewitz, D.; Hanauer, S.B.; Lichtenstein, G.R.; de Villiers, W.J.; Blank, M.; Lang, Y.; et al. Long-term infliximab maintenance therapy for ulcerative colitis: The ACT-1 and -2 extension studies. Inflamm. Bowel Dis. 2012, 18, 201–211. [Google Scholar] [CrossRef]
- Mirdamadi, K.; Salinas, T.; Vali, R.; Papadimitropoulos, M.; Piquette-Miller, M. Meta-Analysis of Pregnancy Outcomes after Exposure to TNF-α Inhibitors during Pregnancy for the Treatment of Arthritic Diseases. J. Popul. Ther. Clin. Pharmacol. 2018, 25, e53–e56. [Google Scholar] [CrossRef]
- Bröms, G.; Kieler, H.; Ekbom, A.; Gissler, M.; Hellgren, K.; Lahesmaa-Korpinen, A.M.; Pedersen, L.; Schmitt-Egenolf, M.; Sørensen, H.T.; Granath, F. Anti-TNF treatment during pregnancy and birth outcomes: A population-based study from Denmark, Finland, and Sweden. Pharmacoepidemiol. Drug Saf. 2020, 29, 316–327. [Google Scholar] [CrossRef]
- Skorpen, C.G.; Hoeltzenbein, M.; Tincani, A.; Fischer-Betz, R.; Elefant, E.; Chambers, C.; da Silva, J.; Nelson-Piercy, C.; Cetin, I.; Costedoat-Chalumeau, N.; et al. The EULAR points to consider for use of antirheumatic drugs before pregnancy, and during pregnancy and lactation. Ann. Rheum. Dis. 2016, 75, 795–810. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lau, C.S.; Chia, F.; Dans, L.; Harrison, A.; Hsieh, T.Y.; Jain, R.; Jung, S.M.; Kishimoto, M.; Kumar, A.; Leong, K.P.; et al. 2018 update of the APLAR recommendations for treatment of rheumatoid arthritis. Int. J. Rheum. Dis. 2019, 22, 357–375. [Google Scholar] [CrossRef] [Green Version]
- Doherty, G.; Katsanos, K.H.; Burisch, J.; Allez, M.; Papamichael, K.; Stallmach, A.; Mao, R.; Berset, I.P.; Gisbert, J.P.; Sebastian, S.; et al. European Crohn’s and Colitis Organisation Topical Review on Treatment Withdrawal [‘Exit Strategies’] in Inflammatory Bowel Disease. J. Crohns Colitis. 2018, 12, 17–31. [Google Scholar] [CrossRef] [Green Version]
- Puchner, A.; Gröchenig, H.P.; Sautner, J.; Helmy-Bader, Y.; Juch, H.; Reinisch, S.; Högenauer, C.; Koch, R.; Hermann, J.; Studnicka-Benke, A.; et al. Immunosuppressives and biologics during pregnancy and lactation: A consensus report issued by the Austrian Societies of Gastroenterology and Hepatology and Rheumatology and Rehabilitation. Wien. Klin. Wochenschr. 2019, 131, 29–44. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mahadevan, U.; Robinson, C.; Bernasko, N.; Boland, B.; Chambers, C.; Dubinsky, M.; Friedman, S.; Kane, S.; Manthey, J.; Sauberan, J.; et al. Inflammatory Bowel Disease in Pregnancy Clinical Care Pathway: A Report from the American Gastroenterological Association IBD Parenthood Project Working Group. Gastroenterology 2019, 156, 1508–1524. [Google Scholar] [CrossRef] [Green Version]
- Lamb, C.A.; Kennedy, N.A.; Raine, T.; Hendy, P.A.; Smith, P.J.; Limdi, J.K.; Hayee, B.; Lomer, M.C.E.; Parkes, G.C.; Selinger, C.; et al. British Society of Gastroenterology consensus guidelines on the management of inflammatory bowel disease in adults. Gut 2019, 68 (Suppl. S3). [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Restellini, S.; Biedermann, L.; Hruz, P.; Mottet, C.; Moens, A.; Ferrante, M.; Schoepfer, A.M.; on behalf of Swiss IBDnet, an official working group of the Swiss Society of Gastroenterology. Update on the Management of Inflammatory Bowel Disease during Pregnancy and Breastfeeding. Digestion 2020, 101 (Suppl. S1), 27–42. [Google Scholar] [CrossRef] [PubMed]
- Balshem, H.; Helfand, M.; Schünemann, H.J.; Oxman, A.D.; Kunz, R.; Brozek, J.; Vist, G.E.; Falck-Ytter, Y.; Meerpohl, J.; Norris, S.; et al. GRADE guidelines: 3. Rating the quality of evidence. J. Clin. Epidemiol. 2011, 64, 401–406. [Google Scholar] [CrossRef] [PubMed]
- Paul, R.P.R.; Michael, P.G. OCEBM Levels of Evidence Working Group. The Oxford 2011 levels of evidence. Oxford centre for Evidence-Based Medicine. Spine 2011, 38, 786–794. [Google Scholar]



| FDA Category | Description |
|---|---|
| A | Adequate and well-controlled studies have failed to demonstrate a risk to the fetus during the first trimester of pregnancy (and there is no evidence of risk in the later trimesters) |
| B | Animal reproduction studies have not demonstrated a fetal risk, but there are no adequate and well-controlled studies in pregnant women. Or Animal reproduction studies have shown an adverse effect, but adequate and well-controlled studies in pregnant women have failed to demonstrate a risk to the fetus during the first trimester of pregnancy (and there is no evidence of a risk in the later trimester) |
| C | Animal reproduction studies have shown an adverse effect on the fetus, there are no adequate and well-controlled studies in humans, and the benefits from the use of the drug in pregnant women may be acceptable despite its potential risks. Or There are no animal reproduction studies and no adequate and well-controlled studies in humans. |
| D | There is positive evidence of human fetal risk based on adverse reaction data from investigational or marketing experience or studies in humans, but the potential benefits from the use of the drug in pregnant women may be acceptable despite its potential risks |
| X | Studies in animal or humans have demonstrated fetal abnormalities or there is positive evidence of fetal risk based on adverse reaction reports from investigational or marketing experience or both and the risk of the use of the drug in pregnant women |
| Medical Societies Recommendations for Management of Inflammatory Diseases PRIOR TO CONCEPTION | |||||||
|---|---|---|---|---|---|---|---|
| Society | BSR/BHPR 2016 | EULAR 2016 | APLAR 2018 | ACR 2020 | ECCO 2017 | ASGHRR 2019 | AGA 2019 |
| Medication | |||||||
| Adalimumab (ADA) | Can be used | No risk of congenital defects | No clear guidelines-use in pregnancy only in patients whose disease activity cannot be otherwise controlled (Grade C) * | Can be used + | No clear guidelines | Can be used | TNFi should be continued; measure serum drug levels; monotherapy as preferred option |
| Etanercept (ETA) | Can be used | Can be used + | Can be used | ||||
| Infliximab (INF) | Can be used | Can be used + | Can be used | ||||
| Certolizumab pegol (CZP) | Can be used | Strongly recommended ++ | Can be used | ||||
| Golimumab (GOLI) | No data | Can be used + | Conditionally | ||||
| Medical Societies Recommendations for the Management of Inflammatory Diseases DURING PREGNANCY | |||||||
|---|---|---|---|---|---|---|---|
| Society | BSR 2016 | EULAR 2016 | APLAR 2018 | ACR 2020 | ECCO 2017 | ASGHRR 2019 | AGA 2019 |
| Medication | |||||||
| Adalimumab (ADA) | Can be used during I and II trimester | Use throughout first half of the pregnancy (20 weeks). Throughout pregnancy- as needed | TNFi (preferred ETA and CZP) can be used throughout pregnancy in patients with established RA, if other therapeutical options are not efficient | Conditionally +; Continue in I and II trimesters, discontinue in III trimester # | Treatment should be discontinued at latest week 30 or even earlier (20–25 week), if IBD is in remission Female patients in clinical remission-safe option for the mother and for the child is to discontinue TNFi in II trimester | Strong recommendation for use (LE2; GRB) | Maintain prepregnancy doses. Continue dosing throughout all 3 trimesters (CZP)If possible, plan the final dose before EDC according to the drug T1/2 to minimize transfer through the placenta: ADA—2–3 weeks: GOLI—4–6 weeks INF—6–10 weeks; base dosing on prepregnancy weight. Resume treatment not earlier than 24–48 ** h after delivery |
| Etanercept (ETA) | Can be used during I and II trimester | Use throughout pregnancy may be considered *. | Conditionally +; Continue in I and II trimesters, discontinue in III trimester # | Strong recommendation for use (LE2; GRB) | |||
| Infliximab (INF) | Can be used during I trimester–stop at 16 week | Use throughout first half of the pregnancy (20 weeks). Throughout pregnancy- as needed | Conditionally +; Continue in I and II trimesters, discontinue in III trimester # | Strong recommendation for use (LE2; GRB) | |||
| Certolizumab pegol (CZP) | Can be used | Use throughout pregnancy may be considered *. | Strongly recommended ++ | Strong recommendation for use (LE2; GRB) | |||
| Golimumab (GOLI) | No data | ConditionallyNo data | Conditionally + Management like ADA, ETA, INF | Conditionally limited data (LE4, G C) | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Romanowska-Próchnicka, K.; Felis-Giemza, A.; Olesińska, M.; Wojdasiewicz, P.; Paradowska-Gorycka, A.; Szukiewicz, D. The Role of TNF-α and Anti-TNF-α Agents during Preconception, Pregnancy, and Breastfeeding. Int. J. Mol. Sci. 2021, 22, 2922. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms22062922
Romanowska-Próchnicka K, Felis-Giemza A, Olesińska M, Wojdasiewicz P, Paradowska-Gorycka A, Szukiewicz D. The Role of TNF-α and Anti-TNF-α Agents during Preconception, Pregnancy, and Breastfeeding. International Journal of Molecular Sciences. 2021; 22(6):2922. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms22062922
Chicago/Turabian StyleRomanowska-Próchnicka, Katarzyna, Anna Felis-Giemza, Marzena Olesińska, Piotr Wojdasiewicz, Agnieszka Paradowska-Gorycka, and Dariusz Szukiewicz. 2021. "The Role of TNF-α and Anti-TNF-α Agents during Preconception, Pregnancy, and Breastfeeding" International Journal of Molecular Sciences 22, no. 6: 2922. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms22062922