
The Application of Mesenchymal Stromal Cells and Their Homing Capabilities to Regenerate the Intervertebral Disc

 , , , , and
, , , , and
Abstract
:1. Introduction
The Burden of Low Back Pain and Its Association with Intervertebral Disc Degeneration
2. Application of Mesenchymal Stromal Cells for IVD Repair
2.1. Preclinical Studies with MSCs
2.2. Clinical Studies with MSCs
2.3. MSC Homing into an IVD
3. Limitations of MSC-Based IVD Regeneration
4. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| ACAN | Aggrecan |
| AF | Annulus Fibrosus |
| BDI | Beck Depression Inventor |
| BMP2 | Bone Morphogenetic Protein 2 |
| CA12 | Carbonic Anhydrase 12 |
| CD | Cluster of Differentiation |
| CEP | Cartilaginous Endplate |
| CFU-F | Colony Forming Unit-Fibroblasts |
| COL1 | Collagen Type I |
| COL2 | Collagen Type II |
| CTGF | Connective Tissue Growth Factor |
| CXCR4 | C-X-C Chemokine Receptor Type 4 |
| DALY | Disability-Adjusted Life-Years |
| FGF | Fibroblast Growth Factor |
| FOX | Forkhead Box |
| GAG | Glycosaminoglycan |
| GD2 | Disialoganglioside 2 |
| GDF | Growth/Differentiation Factor |
| IDD | Intervertebral Disc Degeneration |
| IGF-1 | Insulin-Like Growth Factor 1 |
| IGF-1sR | Insulin-Like Growth Factor 1 Receptor |
| IL-1β | Interleukin-1β |
| iPSC | Induced Pluripotent Stem Cell |
| IVD | Intervertebral Disc |
| KRT | Cytokeratin |
| LBP | Low Back Pain |
| MDC | Macrophage-Derived Chemokine |
| MRI | Magnetic Resonance Imaging |
| MSC | Mesenchymal Stromal Cell |
| NP | Nucleus Pulposus |
| NSAID | Non-Steroidal Anti-Inflammatory Drug |
| ODI | Oswestry Disability Index |
| PAX | Paired Box |
| PCL | Polycaprolacton |
| PDGF-R | Platelet-Derived Growth Factor Receptor |
| PPI | Present Pain Intensity |
| SANE | Single Assessment Numeric Evaluation |
| SDF-1 | Stromal Cell-Derived Factor 1 |
| SHH | Sonic Hedgehog Signaling Molecule |
| SOX | SRY-Box Transcription Factor |
| TGF-β3 | Transforming Growth Factor β3 |
| Tie2 | Angiopoietin-1 Receptor |
| TNF-α | Tumor Necrosis Factor α |
| VAS | Visual Analogue Scale |
References
- Oichi, T.; Taniguchi, Y.; Oshima, Y.; Tanaka, S.; Saito, T. Pathomechanism of intervertebral disc degeneration. JOR Spine 2020, 3, e1076. [Google Scholar] [CrossRef] [PubMed]
- DALYs, G.B.D.; Collaborators, H. Global, regional, and national disability-adjusted life-years (DALYs) for 333 diseases and injuries and healthy life expectancy (HALE) for 195 countries and territories, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet 2017, 390, 1260–1344. [Google Scholar] [CrossRef] [Green Version]
- Hartvigsen, J.; Hancock, M.J.; Kongsted, A.; Louw, Q.; Ferreira, M.L.; Genevay, S.; Hoy, D.; Karppinen, J.; Pransky, G.; Sieper, J.; et al. What low back pain is and why we need to pay attention. Lancet 2018, 391, 2356–2367. [Google Scholar] [CrossRef] [Green Version]
- Bevan, S.; Quadrello, T.; McGee, R.; Mahdon, M.; Vavrovsky, A.; Barham, L. Fit for Work? Musculoskeletal Disorders in the European Workforce: Fit for Work Europe; Part of Lancaster University: Lancashire, UK, 2009. [Google Scholar]
- Hoy, D.; Bain, C.; Williams, G.; March, L.; Brooks, P.; Blyth, F.; Woolf, A.; Vos, T.; Buchbinder, R. A systematic review of the global prevalence of low back pain. Arthritis Rheum 2012, 64, 2028–2037. [Google Scholar] [CrossRef] [PubMed]
- Katz, J.N. Lumbar disc disorders and low-back pain: Socioeconomic factors and consequences. J. Bone Jt. Surg. Am. 2006, 88 (Suppl. 2), 21–24. [Google Scholar] [CrossRef]
- Macfarlane, G.J.; Thomas, E.; Croft, P.R.; Papageorgiou, A.C.; Jayson, M.I.; Silman, A.J. Predictors of early improvement in low back pain amongst consulters to general practice: The influence of pre-morbid and episode-related factors. Pain 1999, 80, 113–119. [Google Scholar] [CrossRef]
- Dunn, K.M.; Hestbaek, L.; Cassidy, J.D. Low back pain across the life course. Best Pract. Res. Clin. Rheumatol. 2013, 27, 591–600. [Google Scholar] [CrossRef]
- Golob, A.L.; Wipf, J.E. Low back pain. Med. Clin. N. Am. 2014, 98, 405–428. [Google Scholar] [CrossRef]
- Cheung, K.M.; Karppinen, J.; Chan, D.; Ho, D.W.; Song, Y.Q.; Sham, P.; Cheah, K.S.; Leong, J.C.; Luk, K.D. Prevalence and pattern of lumbar magnetic resonance imaging changes in a population study of one thousand forty-three individuals. Spine 2009, 34, 934–940. [Google Scholar] [CrossRef]
- White, A.A., 3rd; Panjabi, M.M. The basic kinematics of the human spine. A review of past and current knowledge. Spine 1978, 3, 12–20. [Google Scholar] [CrossRef]
- Sun, Z.; Liu, B.; Luo, Z.J. The Immune Privilege of the Intervertebral Disc: Implications for Intervertebral Disc Degeneration Treatment. Int. J. Med. Sci. 2020, 17, 685–692. [Google Scholar] [CrossRef] [Green Version]
- Cassidy, J.J.; Hiltner, A.; Baer, E. Hierarchical structure of the intervertebral disc. Connect Tissue Res. 1989, 23, 75–88. [Google Scholar] [CrossRef]
- Adams, P.; Eyre, D.R.; Muir, H. Biochemical aspects of development and ageing of human lumbar intervertebral discs. Rheumatol. Rehabil. 1977, 16, 22–29. [Google Scholar] [CrossRef] [PubMed]
- Inoue, H.; Takeda, T. Three-dimensional observation of collagen framework of lumbar intervertebral discs. Acta Orthop. Scand. 1975, 46, 949–956. [Google Scholar] [CrossRef] [Green Version]
- Sakai, D.; Andersson, G.B. Stem cell therapy for intervertebral disc regeneration: Obstacles and solutions. Nat. Rev. Rheumatol. 2015, 11, 243–256. [Google Scholar] [CrossRef]
- Urban, J.P.; Smith, S.; Fairbank, J.C. Nutrition of the intervertebral disc. Spine 2004, 29, 2700–2709. [Google Scholar] [CrossRef]
- Kurunlahti, M.; Tervonen, O.; Vanharanta, H.; Ilkko, E.; Suramo, I. Association of atherosclerosis with low back pain and the degree of disc degeneration. Spine 1999, 24, 2080–2084. [Google Scholar] [CrossRef] [PubMed]
- Johnstone, B.; Bayliss, M.T. The large proteoglycans of the human intervertebral disc. Changes in their biosynthesis and structure with age, topography, and pathology. Spine 1995, 20, 674–684. [Google Scholar] [CrossRef] [PubMed]
- Risbud, M.V.; Shapiro, I.M. Role of cytokines in intervertebral disc degeneration: Pain and disc content. Nat. Rev. Rheumatol. 2014, 10, 44–56. [Google Scholar] [CrossRef] [PubMed]
- Freemont, A.J.; Peacock, T.E.; Goupille, P.; Hoyland, J.A.; O’Brien, J.; Jayson, M.I. Nerve ingrowth into diseased intervertebral disc in chronic back pain. Lancet 1997, 350, 178–181. [Google Scholar] [CrossRef]
- Carreon, L.Y.; Ito, T.; Yamada, M.; Uchiyama, S.; Takahashi, H.E. Neovascularization induced by anulus and its inhibition by cartilage endplate. Its role in disc absorption. Spine 1997, 22, 1429–1434. [Google Scholar] [CrossRef]
- Kadow, T.; Sowa, G.; Vo, N.; Kang, J.D. Molecular basis of intervertebral disc degeneration and herniations: What are the important translational questions? Clin. Orthop. Relat. Res. 2015, 473, 1903–1912. [Google Scholar] [CrossRef] [Green Version]
- Luoma, K.; Riihimaki, H.; Luukkonen, R.; Raininko, R.; Viikari-Juntura, E.; Lamminen, A. Low back pain in relation to lumbar disc degeneration. Spine 2000, 25, 487–492. [Google Scholar] [CrossRef]
- Qaseem, A.; Wilt, T.J.; McLean, R.M.; Forciea, M.A.; Clinical Guidelines Committee of the American College of Physicians. Noninvasive Treatments for Acute, Subacute, and Chronic Low Back Pain: A Clinical Practice Guideline From the American College of Physicians. Ann. Intern. Med. 2017, 166, 514–530. [Google Scholar] [CrossRef] [Green Version]
- Vas, J.; Aranda, J.M.; Modesto, M.; Benitez-Parejo, N.; Herrera, A.; Martinez-Barquin, D.M.; Aguilar, I.; Sanchez-Araujo, M.; Rivas-Ruiz, F. Acupuncture in patients with acute low back pain: A multicentre randomised controlled clinical trial. Pain 2012, 153, 1883–1889. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.H.; Choi, T.Y.; Lee, M.S.; Lee, H.; Shin, B.C.; Lee, H. Acupuncture for acute low back pain: A systematic review. Clin. J. Pain 2013, 29, 172–185. [Google Scholar] [CrossRef] [PubMed]
- Saper, R.B.; Lemaster, C.; Delitto, A.; Sherman, K.J.; Herman, P.M.; Sadikova, E.; Stevans, J.; Keosaian, J.E.; Cerrada, C.J.; Femia, A.L.; et al. Yoga, Physical Therapy, or Education for Chronic Low Back Pain. Ann. Intern. Med. 2017, 167. [Google Scholar] [CrossRef]
- Chou, R.; Cote, P.; Randhawa, K.; Torres, P.; Yu, H.; Nordin, M.; Hurwitz, E.L.; Haldeman, S.; Cedraschi, C. The Global Spine Care Initiative: Applying evidence-based guidelines on the non-invasive management of back and neck pain to low- and middle-income communities. Eur. Spine J. 2018, 27, 851–860. [Google Scholar] [CrossRef]
- May, R.D.; Frauchiger, D.A.; Albers, C.E.; Benneker, L.M.; Kohl, S.; Gantenbein, B. Inhibitory Effects of Human Primary Intervertebral Disc Cells on Human Primary Osteoblasts in a Co-Culture System. Int. J. Mol. Sci. 2018, 19, 1195. [Google Scholar] [CrossRef] [Green Version]
- De Kunder, S.L.; Rijkers, K.; Caelers, I.; de Bie, R.A.; Koehler, P.J.; van Santbrink, H. Lumbar Interbody Fusion: A Historical Overview and a Future Perspective. Spine 2018, 43, 1161–1168. [Google Scholar] [CrossRef] [PubMed]
- Bodalia, P.N.; Balaji, V.; Kaila, R.; Wilson, L. Effectiveness and safety of recombinant human bone morphogenetic protein-2 for adults with lumbar spine pseudarthrosis following spinal fusion surgery: A systematic review. Bone Jt. Res. 2016, 5, 145–152. [Google Scholar] [CrossRef] [PubMed]
- May, R.D.; Frauchiger, D.A.; Albers, C.E.; Tekari, A.; Benneker, L.M.; Klenke, F.M.; Hofstetter, W.; Gantenbein, B. Application of Cytokines of the Bone Morphogenetic Protein (BMP) Family in Spinal Fusion—Effects on the Bone, Intervertebral Disc and Mesenchymal Stromal Cells. Curr. Stem Cell Res. Ther. 2019, 14, 618–643. [Google Scholar] [CrossRef]
- Wang, X.; Wanyan, P.; Tian, J.H.; Hu, L. Meta-analysis of randomized trials comparing fusion surgery to non-surgical treatment for discogenic chronic low back pain. J. Back Musculoskelet. Rehabil. 2015, 28, 621–627. [Google Scholar] [CrossRef]
- Harris, I.A.; Traeger, A.; Stanford, R.; Maher, C.G.; Buchbinder, R. Lumbar spine fusion: What is the evidence? Intern. Med. J. 2018, 48, 1430–1434. [Google Scholar] [CrossRef] [Green Version]
- Clouet, J.; Fusellier, M.; Camus, A.; Le Visage, C.; Guicheux, J. Intervertebral disc regeneration: From cell therapy to the development of novel bioinspired endogenous repair strategies. Adv. Drug Deliv. Rev. 2019, 146, 306–324. [Google Scholar] [CrossRef]
- Sakai, D.; Nakamura, Y.; Nakai, T.; Mishima, T.; Kato, S.; Grad, S.; Alini, M.; Risbud, M.V.; Chan, D.; Cheah, K.S.; et al. Exhaustion of nucleus pulposus progenitor cells with ageing and degeneration of the intervertebral disc. Nat. Commun. 2012, 3, 1264. [Google Scholar] [CrossRef] [Green Version]
- Takahashi, K.; Yamanaka, S. Induction of pluripotent stem cells from mouse embryonic and adult fibroblast cultures by defined factors. Cell 2006, 126, 663–676. [Google Scholar] [CrossRef] [Green Version]
- Yoshikawa, T.; Ueda, Y.; Miyazaki, K.; Koizumi, M.; Takakura, Y. Disc regeneration therapy using marrow mesenchymal cell transplantation: A report of two case studies. Spine 2010, 35, E475–E480. [Google Scholar] [CrossRef] [PubMed]
- Sheikh, H.; Zakharian, K.; De La Torre, R.P.; Facek, C.; Vasquez, A.; Chaudhry, G.R.; Svinarich, D.; Perez-Cruet, M.J. In vivo intervertebral disc regeneration using stem cell-derived chondroprogenitors. J. Neurosurg. Spine 2009, 10, 265–272. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vadala, G.; Ambrosio, L.; Russo, F.; Papalia, R.; Denaro, V. Interaction between Mesenchymal Stem Cells and Intervertebral Disc Microenvironment: From Cell Therapy to Tissue Engineering. Stem Cells Int. 2019, 2019, 2376172. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.J.; Zhuge, Y.; Velazquez, O.C. Trafficking and differentiation of mesenchymal stem cells. J. Cell Biochem. 2009, 106, 984–991. [Google Scholar] [CrossRef] [PubMed]
- Bianco, P. Mesenchymal stem cells. Annu. Rev. Cell Dev. Biol. 2014, 30, 677–704. [Google Scholar] [CrossRef]
- Pittenger, M.F.; Mackay, A.M.; Beck, S.C.; Jaiswal, R.K.; Douglas, R.; Mosca, J.D.; Moorman, M.A.; Simonetti, D.W.; Craig, S.; Marshak, D.R. Multilineage potential of adult human mesenchymal stem cells. Science 1999, 284, 143–147. [Google Scholar] [CrossRef] [Green Version]
- Caplan, A.I. Adult mesenchymal stem cells for tissue engineering versus regenerative medicine. J. Cell Physiol. 2007, 213, 341–347. [Google Scholar] [CrossRef]
- Bertolo, A.; Thiede, T.; Aebli, N.; Baur, M.; Ferguson, S.J.; Stoyanov, J.V. Human mesenchymal stem cell co-culture modulates the immunological properties of human intervertebral disc tissue fragments in vitro. Eur. Spine J. 2011, 20, 592–603. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shim, E.K.; Lee, J.S.; Kim, D.E.; Kim, S.K.; Jung, B.J.; Choi, E.Y.; Kim, C.S. Autogenous Mesenchymal Stem Cells from the Vertebral Body Enhance Intervertebral Disc Regeneration via Paracrine Interaction: An in Vitro Pilot Study. Cell Transpl. 2016, 25, 1819–1832. [Google Scholar] [CrossRef] [PubMed]
- Stoyanov, J.V.; Gantenbein-Ritter, B.; Bertolo, A.; Aebli, N.; Baur, M.; Alini, M.; Grad, S. Role of hypoxia and growth and differentiation factor-5 on differentiation of human mesenchymal stem cells towards intervertebral nucleus pulposus-like cells. Eur. Cell Mater. 2011, 21, 533–547. [Google Scholar] [CrossRef]
- Clarke, L.E.; McConnell, J.C.; Sherratt, M.J.; Derby, B.; Richardson, S.M.; Hoyland, J.A. Growth differentiation factor 6 and transforming growth factor-beta differentially mediate mesenchymal stem cell differentiation, composition, and micromechanical properties of nucleus pulposus constructs. Arthritis Res. Ther. 2014, 16, R67. [Google Scholar] [CrossRef] [Green Version]
- Berebichez-Fridman, R.; Gomez-Garcia, R.; Granados-Montiel, J.; Berebichez-Fastlicht, E.; Olivos-Meza, A.; Granados, J.; Velasquillo, C.; Ibarra, C. The Holy Grail of Orthopedic Surgery: Mesenchymal Stem Cells-Their Current Uses and Potential Applications. Stem Cells Int. 2017, 2017, 2638305. [Google Scholar] [CrossRef]
- Hodgkinson, T.; Shen, B.; Diwan, A.; Hoyland, J.A.; Richardson, S.M. Therapeutic potential of growth differentiation factors in the treatment of degenerative disc diseases. JOR Spine 2019, 2, e1045. [Google Scholar] [CrossRef] [Green Version]
- Lyu, F.J.; Cheung, K.M.; Zheng, Z.; Wang, H.; Sakai, D.; Leung, V.Y. IVD progenitor cells: A new horizon for understanding disc homeostasis and repair. Nat. Rev. Rheumatol. 2019, 15, 102–112. [Google Scholar] [CrossRef]
- Kraus, P.; Lufkin, T. Implications for a Stem Cell Regenerative Medicine Based Approach to Human Intervertebral Disk Degeneration. Front. Cell Dev. Biol. 2017, 5, 17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Loibl, M.; Wuertz-Kozak, K.; Vadala, G.; Lang, S.; Fairbank, J.; Urban, J.P. Controversies in regenerative medicine: Should intervertebral disc degeneration be treated with mesenchymal stem cells? JOR Spine 2019, 2, e1043. [Google Scholar] [CrossRef] [PubMed]
- Ma, K.; Chen, S.; Li, Z.; Deng, X.; Huang, D.; Xiong, L.; Shao, Z. Mechanisms of endogenous repair failure during intervertebral disc degeneration. Osteoarthr. Cartil. 2019, 27, 41–48. [Google Scholar] [CrossRef] [Green Version]
- Melrose, J. Strategies in regenerative medicine for intervertebral disc repair using mesenchymal stem cells and bioscaffolds. Regen. Med. 2016, 11, 705–724. [Google Scholar] [CrossRef]
- Piazza, N.; Dehghani, M.; Gaborski, T.R.; Wuertz-Kozak, K. Therapeutic Potential of Extracellular Vesicles in Degenerative Diseases of the Intervertebral Disc. Front. Bioeng. Biotechnol. 2020, 8, 311. [Google Scholar] [CrossRef]
- Richardson, S.M.; Kalamegam, G.; Pushparaj, P.N.; Matta, C.; Memic, A.; Khademhosseini, A.; Mobasheri, R.; Poletti, F.L.; Hoyland, J.A.; Mobasheri, A. Mesenchymal stem cells in regenerative medicine: Focus on articular cartilage and intervertebral disc regeneration. Methods 2016, 99, 69–80. [Google Scholar] [CrossRef] [PubMed]
- Urits, I.; Capuco, A.; Sharma, M.; Kaye, A.D.; Viswanath, O.; Cornett, E.M.; Orhurhu, V. Stem Cell Therapies for Treatment of Discogenic Low Back Pain: A Comprehensive Review. Curr. Pain Headache Rep. 2019, 23, 65. [Google Scholar] [CrossRef]
- Vadala, G.; Russo, F.; Ambrosio, L.; Papalia, R.; Denaro, V. Mesenchymal stem cells for intervertebral disc regeneration. J. Biol. Regul. Homeost. Agents 2016, 30, 173–179. [Google Scholar]
- Vadala, G.; Russo, F.; Ambrosio, L.; Loppini, M.; Denaro, V. Stem cells sources for intervertebral disc regeneration. World J. Stem Cells 2016, 8, 185–201. [Google Scholar] [CrossRef] [PubMed]
- Xia, K.; Gong, Z.; Zhu, J.; Yu, W.; Wang, Y.; Wang, J.; Xu, A.; Zhou, X.; Tao, H.; Li, F.; et al. Differentiation of Pluripotent Stem Cells into Nucleus Pulposus Progenitor Cells for Intervertebral Disc Regeneration. Curr. Stem Cell Res. Ther. 2019, 14, 57–64. [Google Scholar] [CrossRef]
- Stergar, J.; Gradisnik, L.; Velnar, T.; Maver, U. Intervertebral disc tissue engineering: A brief review. Bosn. J. Basic Med. Sci. 2019, 19, 130–137. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Frauchiger, D.A.; Heeb, S.R.; May, R.D.; Woltje, M.; Benneker, L.M.; Gantenbein, B. Differentiation of MSC and annulus fibrosus cells on genetically engineered silk fleece-membrane-composites enriched for GDF-6 or TGF-beta3. J. Orthop. Res. 2018, 36, 1324–1333. [Google Scholar] [CrossRef] [PubMed]
- Peroglio, M.; Eglin, D.; Benneker, L.M.; Alini, M.; Grad, S. Thermoreversible hyaluronan-based hydrogel supports in vitro and ex vivo disc-like differentiation of human mesenchymal stem cells. Spine J. 2013, 13, 1627–1639. [Google Scholar] [CrossRef]
- Zhang, C.; Gullbrand, S.E.; Schaer, T.P.; Boorman, S.; Elliott, D.M.; Chen, W.; Dodge, G.R.; Mauck, R.L.; Malhotra, N.R.; Smith, L.J. Combined Hydrogel and Mesenchymal Stem Cell Therapy for Moderate-Severity Disc Degeneration in Goats. Tissue Eng. Part A 2020. [Google Scholar] [CrossRef]
- Sun, B.; Lian, M.; Han, Y.; Mo, X.; Jiang, W.; Qiao, Z.; Dai, K. A 3D-Bioprinted dual growth factor-releasing intervertebral disc scaffold induces nucleus pulposus and annulus fibrosus reconstruction. Bioact. Mater. 2021, 6, 179–190. [Google Scholar] [CrossRef] [PubMed]
- Karp, J.M.; Leng Teo, G.S. Mesenchymal stem cell homing: The devil is in the details. Cell Stem Cell 2009, 4, 206–216. [Google Scholar] [CrossRef] [Green Version]
- Migliorini, F.; Rath, B.; Tingart, M.; Baroncini, A.; Quack, V.; Eschweiler, J. Autogenic mesenchymal stem cells for intervertebral disc regeneration. Int. Orthop. 2019, 43, 1027–1036. [Google Scholar] [CrossRef]
- Orozco, L.; Soler, R.; Morera, C.; Alberca, M.; Sanchez, A.; Garcia-Sancho, J. Intervertebral disc repair by autologous mesenchymal bone marrow cells: A pilot study. Transplantation 2011, 92, 822–828. [Google Scholar] [CrossRef] [Green Version]
- Noriega, D.C.; Ardura, F.; Hernandez-Ramajo, R.; Martin-Ferrero, M.A.; Sanchez-Lite, I.; Toribio, B.; Alberca, M.; Garcia, V.; Moraleda, J.M.; Sanchez, A.; et al. Intervertebral Disc Repair by Allogeneic Mesenchymal Bone Marrow Cells: A Randomized Controlled Trial. Transplantation 2017, 101, 1945–1951. [Google Scholar] [CrossRef]
- Centeno, C.; Markle, J.; Dodson, E.; Stemper, I.; Williams, C.J.; Hyzy, M.; Ichim, T.; Freeman, M. Treatment of lumbar degenerative disc disease-associated radicular pain with culture-expanded autologous mesenchymal stem cells: A pilot study on safety and efficacy. J. Transl. Med. 2017, 15, 197. [Google Scholar] [CrossRef] [Green Version]
- Comella, K.; Silbert, R.; Parlo, M. Effects of the intradiscal implantation of stromal vascular fraction plus platelet rich plasma in patients with degenerative disc disease. J. Transl. Med. 2017, 15, 12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elabd, C.; Centeno, C.J.; Schultz, J.R.; Lutz, G.; Ichim, T.; Silva, F.J. Intra-discal injection of autologous, hypoxic cultured bone marrow-derived mesenchymal stem cells in five patients with chronic lower back pain: A long-term safety and feasibility study. J. Transl. Med. 2016, 14, 253. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kumar, H.; Ha, D.H.; Lee, E.J.; Park, J.H.; Shim, J.H.; Ahn, T.K.; Kim, K.T.; Ropper, A.E.; Sohn, S.; Kim, C.H.; et al. Safety and tolerability of intradiscal implantation of combined autologous adipose-derived mesenchymal stem cells and hyaluronic acid in patients with chronic discogenic low back pain: 1-year follow-up of a phase I study. Stem Cell Res. Ther. 2017, 8, 262. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pettine, K.A.; Suzuki, R.K.; Sand, T.T.; Murphy, M.B. Autologous bone marrow concentrate intradiscal injection for the treatment of degenerative disc disease with three-year follow-up. Int. Orthop. 2017, 41, 2097–2103. [Google Scholar] [CrossRef]
- Michalek, A.J.; Buckley, M.R.; Bonassar, L.J.; Cohen, I.; Iatridis, J.C. The effects of needle puncture injury on microscale shear strain in the intervertebral disc annulus fibrosus. Spine J. 2010, 10, 1098–1105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carragee, E.J.; Don, A.S.; Hurwitz, E.L.; Cuellar, J.M.; Carrino, J.A.; Herzog, R. 2009 ISSLS Prize Winner: Does discography cause accelerated progression of degeneration changes in the lumbar disc: A ten-year matched cohort study. Spine 2009, 34, 2338–2345. [Google Scholar] [CrossRef]
- Hu, M.H.; Yang, K.C.; Chen, Y.J.; Sun, Y.H.; Lin, F.H.; Yang, S.H. Optimization of puncture injury to rat caudal disc for mimicking early degeneration of intervertebral disc. J. Orthop. Res. 2018, 36, 202–211. [Google Scholar] [CrossRef]
- Issy, A.C.; Castania, V.; Castania, M.; Salmon, C.E.; Nogueira-Barbosa, M.H.; Bel, E.D.; Defino, H.L. Experimental model of intervertebral disc degeneration by needle puncture in Wistar rats. Braz. J. Med. Biol. Res. 2013, 46, 235–244. [Google Scholar] [CrossRef]
- Vadala, G.; Sowa, G.; Hubert, M.; Gilbertson, L.G.; Denaro, V.; Kang, J.D. Mesenchymal stem cells injection in degenerated intervertebral disc: Cell leakage may induce osteophyte formation. J. Tissue Eng. Regen. Med. 2012, 6, 348–355. [Google Scholar] [CrossRef]
- Huang, Y.C.; Leung, V.Y.; Lu, W.W.; Luk, K.D. The effects of microenvironment in mesenchymal stem cell-based regeneration of intervertebral disc. Spine J. 2013, 13, 352–362. [Google Scholar] [CrossRef] [PubMed]
- Fong, E.L.; Chan, C.K.; Goodman, S.B. Stem cell homing in musculoskeletal injury. Biomaterials 2011, 32, 395–409. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, G.D.; Nolta, J.A.; Jin, Y.S.; Barr, M.L.; Yu, H.; Starnes, V.A.; Cramer, D.V. Migration of mesenchymal stem cells to heart allografts during chronic rejection. Transplantation 2003, 75, 679–685. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Li, Y.; Wang, L.; Lu, M.; Zhang, X.; Chopp, M. Therapeutic benefit of intracerebral transplantation of bone marrow stromal cells after cerebral ischemia in rats. J. Neurol. Sci. 2001, 189, 49–57. [Google Scholar] [CrossRef]
- Shafei, A.E.; Ali, M.A.; Ghanem, H.G.; Shehata, A.I.; Abdelgawad, A.A.; Handal, H.R.; Talaat, K.A.; Ashaal, A.E.; El-Shal, A.S. Mesenchymal stem cell therapy: A promising cell-based therapy for treatment of myocardial infarction. J. Gene Med. 2017, 19. [Google Scholar] [CrossRef]
- Barbash, I.M.; Chouraqui, P.; Baron, J.; Feinberg, M.S.; Etzion, S.; Tessone, A.; Miller, L.; Guetta, E.; Zipori, D.; Kedes, L.H.; et al. Systemic delivery of bone marrow-derived mesenchymal stem cells to the infarcted myocardium: Feasibility, cell migration, and body distribution. Circulation 2003, 108, 863–868. [Google Scholar] [CrossRef]
- Shahror, R.A.; Ali, A.A.A.; Wu, C.C.; Chiang, Y.H.; Chen, K.Y. Enhanced Homing of Mesenchymal Stem Cells Overexpressing Fibroblast Growth Factor 21 to Injury Site in a Mouse Model of Traumatic Brain Injury. Int. J. Mol. Sci. 2019, 20, 2624. [Google Scholar] [CrossRef] [Green Version]
- Fan, M.; Zhang, J.; Xin, H.; He, X.; Zhang, X. Current Perspectives on Role of MSC in Renal Pathophysiology. Front. Physiol. 2018, 9, 1323. [Google Scholar] [CrossRef] [Green Version]
- Shao, Y.; Zhou, F.; He, D.; Zhang, L.; Shen, J. Overexpression of CXCR7 promotes mesenchymal stem cells to repair phosgene-induced acute lung injury in rats. Biomed. Pharmacother. 2019, 109, 1233–1239. [Google Scholar] [CrossRef]
- Yao, W.; Lay, Y.E.; Kot, A.; Liu, R.; Zhang, H.; Chen, H.; Lam, K.; Lane, N.E. Improved Mobilization of Exogenous Mesenchymal Stem Cells to Bone for Fracture Healing and Sex Difference. Stem Cells 2016, 34, 2587–2600. [Google Scholar] [CrossRef] [Green Version]
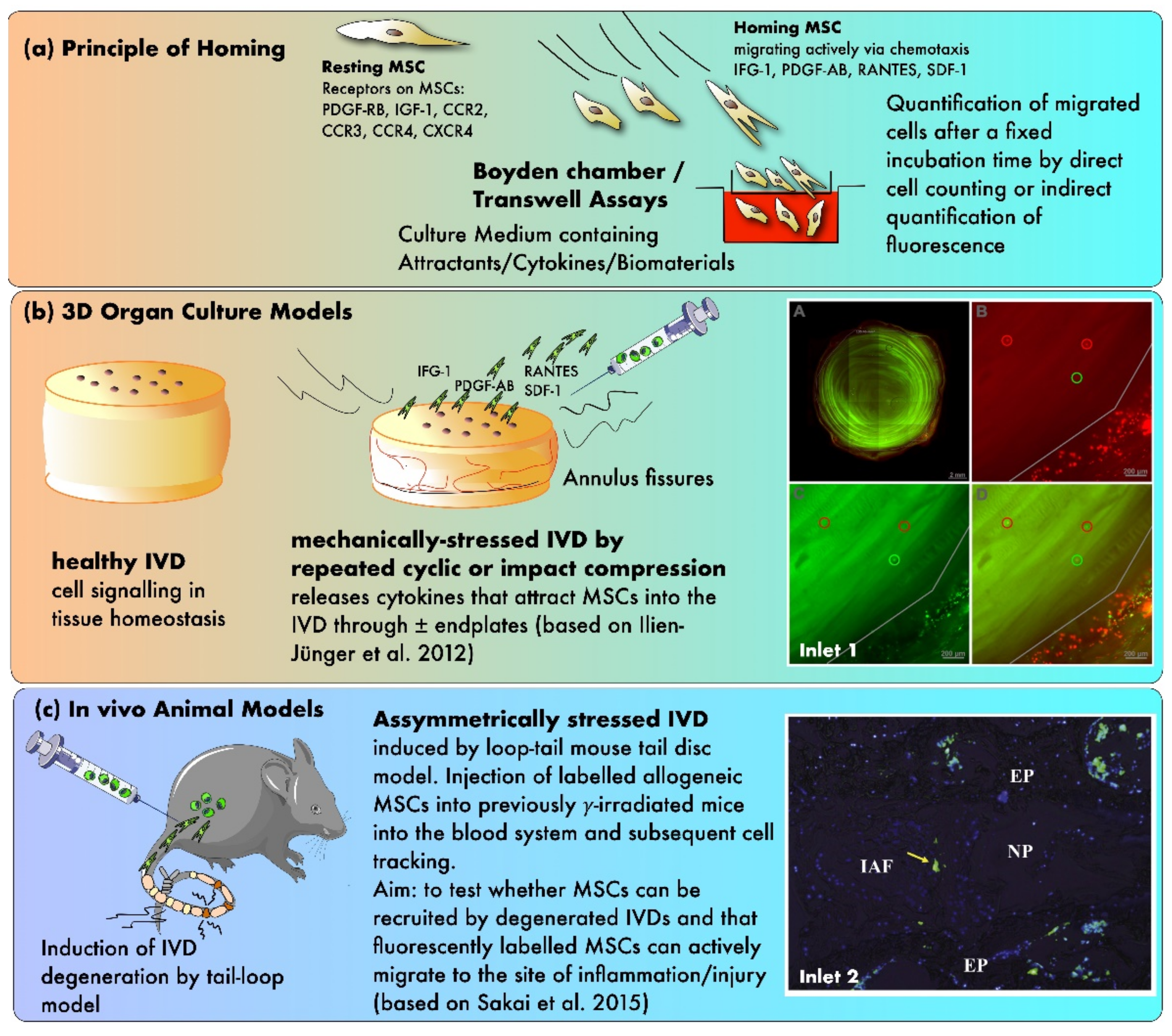
- Sakai, D.; Nishimura, K.; Tanaka, M.; Nakajima, D.; Grad, S.; Alini, M.; Kawada, H.; Ando, K.; Mochida, J. Migration of bone marrow-derived cells for endogenous repair in a new tail-looping disc degeneration model in the mouse: A pilot study. Spine J. 2015, 15, 1356–1365. [Google Scholar] [CrossRef] [Green Version]
- Illien-Junger, S.; Pattappa, G.; Peroglio, M.; Benneker, L.M.; Stoddart, M.J.; Sakai, D.; Mochida, J.; Grad, S.; Alini, M. Homing of mesenchymal stem cells in induced degenerative intervertebral discs in a whole organ culture system. Spine 2012, 37, 1865–1873. [Google Scholar] [CrossRef] [PubMed]
- Sordi, V. Mesenchymal stem cell homing capacity. Transplantation 2009, 87, S42–S45. [Google Scholar] [CrossRef]
- Ponte, A.L.; Marais, E.; Gallay, N.; Langonne, A.; Delorme, B.; Herault, O.; Charbord, P.; Domenech, J. The in vitro migration capacity of human bone marrow mesenchymal stem cells: Comparison of chemokine and growth factor chemotactic activities. Stem Cells 2007, 25, 1737–1745. [Google Scholar] [CrossRef]
- Lapidot, T.; Kollet, O. The essential roles of the chemokine SDF-1 and its receptor CXCR4 in human stem cell homing and repopulation of transplanted immune-deficient NOD/SCID and NOD/SCID/B2m(null) mice. Leukemia 2002, 16, 1992–2003. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pereira, C.L.; Goncalves, R.M.; Peroglio, M.; Pattappa, G.; D’Este, M.; Eglin, D.; Barbosa, M.A.; Alini, M.; Grad, S. The effect of hyaluronan-based delivery of stromal cell-derived factor-1 on the recruitment of MSCs in degenerating intervertebral discs. Biomaterials 2014, 35, 8144–8153. [Google Scholar] [CrossRef] [PubMed]
- Pattappa, G.; Peroglio, M.; Sakai, D.; Mochida, J.; Benneker, L.M.; Alini, M.; Grad, S. CCL5/RANTES is a key chemoattractant released by degenerative intervertebral discs in organ culture. Eur. Cell Mater. 2014, 27, 124–136. [Google Scholar] [CrossRef]
- Wangler, S.; Menzel, U.; Li, Z.; Ma, J.; Hoppe, S.; Benneker, L.M.; Alini, M.; Grad, S.; Peroglio, M. CD146/MCAM distinguishes stem cell subpopulations with distinct migration and regenerative potential in degenerative intervertebral discs. Osteoarthr. Cartil. 2019, 27, 1094–1105. [Google Scholar] [CrossRef] [PubMed]
- Tam, V.; Rogers, I.; Chan, D.; Leung, V.Y.; Cheung, K.M. A comparison of intravenous and intradiscal delivery of multipotential stem cells on the healing of injured intervertebral disk. J. Orthop. Res. 2014, 32, 819–825. [Google Scholar] [CrossRef] [Green Version]
- Cunha, C.; Almeida, C.R.; Almeida, M.I.; Silva, A.M.; Molinos, M.; Lamas, S.; Pereira, C.L.; Teixeira, G.Q.; Monteiro, A.T.; Santos, S.G.; et al. Systemic Delivery of Bone Marrow Mesenchymal Stem Cells for In Situ Intervertebral Disc Regeneration. Stem Cells Transl. Med. 2017, 6, 1029–1039. [Google Scholar] [CrossRef]
- Gruber, H.E.; Ashraf, N.; Kilburn, J.; Williams, C.; Norton, H.J.; Gordon, B.E.; Hanley, E.N., Jr. Vertebral endplate architecture and vascularization: Application of micro-computerized tomography, a vascular tracer, and immunocytochemistry in analyses of disc degeneration in the aging sand rat. Spine 2005, 30, 2593–2600. [Google Scholar] [CrossRef]
- Hassler, O. The human intervertebral disc. A micro-angiographical study on its vascular supply at various ages. Acta Orthop. Scand. 1969, 40, 765–772. [Google Scholar] [CrossRef]
- Pereira, C.L.; Teixeira, G.Q.; Ribeiro-Machado, C.; Caldeira, J.; Costa, M.; Figueiredo, F.; Fernandes, R.; Aguiar, P.; Grad, S.; Barbosa, M.A.; et al. Mesenchymal Stem/Stromal Cells seeded on cartilaginous endplates promote Intervertebral Disc Regeneration through Extracellular Matrix Remodeling. Sci. Rep. 2016, 6, 33836. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wangler, S.; Peroglio, M.; Menzel, U.; Benneker, L.M.; Haglund, L.; Sakai, D.; Alini, M.; Grad, S. Mesenchymal Stem Cell Homing Into Intervertebral Discs Enhances the Tie2-positive Progenitor Cell Population, Prevents Cell Death, and Induces a Proliferative Response. Spine 2019, 44, 1613–1622. [Google Scholar] [CrossRef]
- Violante, F.S.; Mattioli, S.; Bonfiglioli, R. Low-back pain. Handb. Clin. Neurol. 2015, 131, 397–410. [Google Scholar] [CrossRef] [PubMed]
- D’Ippolito, G.; Schiller, P.C.; Ricordi, C.; Roos, B.A.; Howard, G.A. Age-related osteogenic potential of mesenchymal stromal stem cells from human vertebral bone marrow. J. Bone Miner Res. 1999, 14, 1115–1122. [Google Scholar] [CrossRef]
- Banfi, A.; Muraglia, A.; Dozin, B.; Mastrogiacomo, M.; Cancedda, R.; Quarto, R. Proliferation kinetics and differentiation potential of ex vivo expanded human bone marrow stromal cells: Implications for their use in cell therapy. Exp. Hematol. 2000, 28, 707–715. [Google Scholar] [CrossRef]
- Mushahary, D.; Spittler, A.; Kasper, C.; Weber, V.; Charwat, V. Isolation, cultivation, and characterization of human mesenchymal stem cells. Cytometry A 2018, 93, 19–31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burdick, J.A.; Mauck, R.L.; Gerecht, S. To Serve and Protect: Hydrogels to Improve Stem Cell-Based Therapies. Cell Stem Cell 2016, 18, 13–15. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Study Design | Outcomes | References |
|---|---|---|
| Reviewing current uses and potential applications of MSCs in orthopedic surgery. | MSCs can be used for treating musculoskeletal diseases. Further research is needed to evaluate the safety and effectiveness of MSC treatment in orthopedics. | [50] |
| Reviewing current cell-based therapies for treating IDD, with an emphasis on endogenous repair strategies. | Intradiscal cell injections show promising results to reduce LBP. Endogenous repair with growth factors and chemokines has the potential to overcome hurdles of cell-based therapies. | [36] |
| Reviewing current knowledge about IDD and discussing recent advancements made with the GDF family for IVD regeneration. | GDF family members can stimulate anabolic processes when delivered to NP cells and promote NP-like differentiation when delivered to MSCs. | [51] |
| Reviewing characteristics and potency of progenitor cells in different IVD compartments. | IVD progenitor cells show a trilineage differentiation potential and express typical MSC markers. Aging and a degenerated microenvironment affect the fate of IVD progenitor cells. | [52] |
| Reviewing the successes, drawbacks, and the failures of stem cell-based regenerative medicine approaches to repair IDD. | MSC-based treatments for IDD are on the rise and many of them look promising. Nevertheless, it remains important to understand the fate and contribution of these cells and consequently to promote a safer outcome for stem cell-based approaches. | [53] |
| Researchers and clinicians discuss the pros and cons of MSC treatment for IVD regeneration. | Preclinical trials using MSCs for IVD regeneration look promising because of MSC proliferation characteristics, anabolic functionality and inflammation-modulatory properties. | [54] |
| Reviewing mechanisms of endogenous repair during IDD. | Endogenous stem/progenitor cell-based therapy is a promising approach for IDD. Biomimetic peptide biomaterials with signaling molecules can be designed to facilitate the survival and migration of IVD stem/progenitor cells. | [55] |
| Reviewing strategies for IVD repair using bioscaffolds and MSCs. | Preclinical studies with ovine and canine MSCs show impressive results for IVD repair. The authors also hypothesize that combined therapeutic approaches using biomaterial and cell-based therapies promise notable breakthroughs in IVD repair in the near future. | [56] |
| Reviewing the therapeutic potential of MSC-derived and IVD-derived extracellular vesicles for IDD. | MSC-derived extracellular vesicles promote ECM synthesis, IVD cell proliferation, and reduce inflammation and apoptosis. | [57] |
| Reviewing stem cell-based treatments, the molecular machinery and signaling pathways responsible for cartilage and IVD regeneration. | MSC-based therapies show a significant potential to revolutionize the treatment of cartilage defects and IDD. However, there are still many hurdles associated with isolating, expanding, differentiating, and preconditioning MSCs for transplantation into degenerated joints and IVDs. | [58] |
| Reviewing current stem cell therapies to treat discogenic LBP. | Preliminary animal models have shown the great potential of MSC implantation in order to restore the ECM and regenerate the IVD. | [59] |
| Reviewing different stem cell-based treatments for IDD. | The transplantation of adult stem cells has repeatedly shown to help regenerate the IVD’s ECM. However, the efficacy of adult stem cell transplantation for IDD treatment is still unclear and therefore needs further investigation. | [60] |
| Reviewing different stem cell types used as a cell-based therapy for IVD regeneration. | Adult stem cell therapy shows promise for the treatment of IDD. Recent studies have demonstrated the effectiveness of autologous MSC transplantation for IVD regeneration in reproducible animal models. | [61] |
| Reviewing characteristics of healthy and degenerated IVD microenvironments and their influence on IVD and MSC biological activity and viability. | IDD causes an aggravation of the hostile microenvironment for tissue repair and cell survival in the IVD. However, intradiscal cell therapy with MSCs has the potential to regenerate the IVD and to reverse the changes of IDD. | [41] |
| Reviewing the latest advances in repairing degenerated IVDs using MSCs, pluripotent stem cells, and NP progenitor cells. | Various animal models have shown that intradiscally transplanted MSCs generally fail to survive and engraft into the IVD niche, whereas pluripotent stem cells and NP progenitor cells can survive successfully. | [62] |
| Study | Inclusion Criteria | Number of Patients | Number of Cells Injected | Follow Up | Results | References |
|---|---|---|---|---|---|---|
| Injection of autologous BM-derived MSCs into the IVD. | (1) IDD with posterior IVD bulge, (2) radicular pain, (3) failed conservative treatment, (4) failed interventional therapy, (5) patient refuses to pursue surgical option | 33 | N/A | 6 years | Three patients reported. No serious adverse events. Improved SANE numeric pain score. 85% of patients showed reduced IVD bulge size. | [72] |
| Injection of autologous stromal vascular fraction containing adipose tissue-derived MSCs together with platelet rich plasma. | (1) Between 19 and 90 years of age, (2) LBP after failed conservative treatment for 6 months, (3) fibrous ring able to hold the cell implantation | 15 | 30–60 × 106 | 6–12 months | Significant improvement in flexion, VAS, PPI, and pain. Positive trends for ODI and BDI. No severe adverse events were observed. | [73] |
| Injection of autologous BM-derived cultured in a hypoxic environment. | (1) Between 18 and 65 years of age, (2) IDD and failed conservative treatment, (3) significantly functional disability due to pain, (4) painful annular fissures and low pressure positive discography | 5 | 15.1–51.6 × 106 | 4–6 years | No adverse events were reported. Improvement in mobility, strength, and post-stem cell treatment. | [74] |
| Injection of adipose tissue-derived MSCs combined with hyaluronic acid derivates. | (1) Between 10 and 70 years of age, (2) LBP for at least 3 months, (3) VAS ≥ 4, (4) ODI ≥ 30, (5) Pfirrmann’s grade III–IV, (6) IDD confirmed by discography | 10 | 20 × 106 (n = 5) and 40 × 106 (n = 5) | 12 months | No adverse events were observed. Improvement in VAS and ODI. Elevated IVD water content in three patients. | [75] |
| Injection of allogeneic BM-derived MSCs into the IVD compared to sham injection. | (1) IDD and remaining LBP after conservative treatment >6 months, (2) fibrous ring able to hold the cell implantation, (3) decrease in disc height >20%, (4) no spinal infection, (5) absent pregnancy in fertile women | 24 | 25 × 106 | 12 months | Procedure was feasible and safe. Improved algofunctional indices and Pfirrmann’s grade with MSC-treated patients. | [71] |
| Injection of autologous BM-derived MSCs into the IVD. | (1) Centralized chronic LBP for ≥6 months, (2) non-operative treatment for 3 months without resolution, (3) Pfirrmann’s grade 4–7, (4) Modic grade II change or less, (5) decrease in disc height <30%, (6) ODI ≥ 30/100 (7) VAS ≥ 4/10 | 26 | 5426 CFU-F | 3 years | Improvement in VAS and ODI. 40% showed improvement on Pfirrmann’s grade despite the relatively low number of CFU-F. | [76] |
| Injection of autologous BM-derived MSCs into the IVD. | (1) Decrease in disc height >50%, (2) no spinal infection, (3) stages 2, 3, and 4 of Adams, (4) LBP with IDD of one or two IVDs after conservative treatment for over 6 months, (5) No spinal infection | 10 | 10 ± 5 × 106 | 12 months | 85% of pain and disability improvement. Elevated water content but no height recovery in IVDs. | [70] |
| Transplantation of a collagen sponge containing autologous BM-derived MSCs into the IVD. | (1) IDD confirmed with MRI, (2) vacuum phenomenon, (3) IVD instability, (4) pressure and spontaneous pain at level of degenerated IVD, (5) failed conservative treatment | 2 | N/A | 2 years | Enhanced pain scores and increased water content in the IVD. | [39] |
| Species | Study Type | Cell Types | Outcomes | References |
|---|---|---|---|---|
| Human | in vitro | BM MSCs | Growth factors and chemokines such as IGF-1, PDGF-AB, RANTES, and SDF-1 showed a chemoattractive effect on MSCs. | [95] |
| Bovine IVDs and human MSCs | ex vivo | BM MSCs | An intradiscal injectable hydrogel-based on hyaluronan-poly(N-isopropylacrylamide) and supplemented with SDF-1 showed a chemoattractive effect on MSCs. | [97] |
| Bovine IVDs and human MSCs | ex vivo | BM MSCs | The concentration of RANTES was significantly elevated in the medium of induced degenerated IVDs; RANTES may be a key chemoattractant for MSCs in the IVD. | [98] |
| Bovine IVDs and human MSCs | ex vivo | BM MSCs | MSC subpopulations positive for CD146 were associated with a greater homing potential but produced a weaker regenerative response than CD146-negative MSCs. | [99] |
| Murine model with human MPSCs | in vivo | Umbilical cord blood MPSCs | Intravenously injected MSCs showed limited ability to home into a degenerated IVD, but they upregulated GAG and ACAN. | [100] |
| Murine | in vivo | BM MSCs | Intravenously injected MSCs significantly decreased IVD herniation and induced an immunomodulatory effect. | [101] |
| Murine | in vivo | BM MSCs | Only a limited number of intravenously injected MSCs migrated to a degenerated IVD. However, the more serious the injury, the more cells were recruited. | [92] |
| Bovine IVDs and human MSCs | ex vivo | BM MSCs | Greater MSC homing occurred with degenerated IVDs than healthy samples, and IGF-1-transduced MSCs significantly increased the proteoglycan synthesis. | [93] |
| Bovine IVDs and human MSCs | ex vivo | BM MSCs | MSCs seeded on the endplate’s surface of nucleotomized IVDs migrated into the NP and stimulated ECM production and growth factors. | [104] |
| Bovine and human | ex vivo | BM MSCs | Homed MSCs increased the fraction of Tie2-positive IVD cells, enhanced IVD cell proliferation, and reduced the fraction of dead cells in the IVD. | [105] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Croft, A.S.; Illien-Jünger, S.; Grad, S.; Guerrero, J.; Wangler, S.; Gantenbein, B. The Application of Mesenchymal Stromal Cells and Their Homing Capabilities to Regenerate the Intervertebral Disc. Int. J. Mol. Sci. 2021, 22, 3519. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms22073519
Croft AS, Illien-Jünger S, Grad S, Guerrero J, Wangler S, Gantenbein B. The Application of Mesenchymal Stromal Cells and Their Homing Capabilities to Regenerate the Intervertebral Disc. International Journal of Molecular Sciences. 2021; 22(7):3519. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms22073519
Chicago/Turabian StyleCroft, Andreas S., Svenja Illien-Jünger, Sibylle Grad, Julien Guerrero, Sebastian Wangler, and Benjamin Gantenbein. 2021. "The Application of Mesenchymal Stromal Cells and Their Homing Capabilities to Regenerate the Intervertebral Disc" International Journal of Molecular Sciences 22, no. 7: 3519. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms22073519