
IL-8 as a Potential Therapeutic Target for Periodontitis and Its Inhibition by Caffeic Acid Phenethyl Ester In Vitro

 ,
,  , ,
, , 
Abstract
:1. Introduction
2. Results
2.1. The Impact of Proinflammatory Cytokines and the Oral Microbiota on the Severity of Periodontal Disease
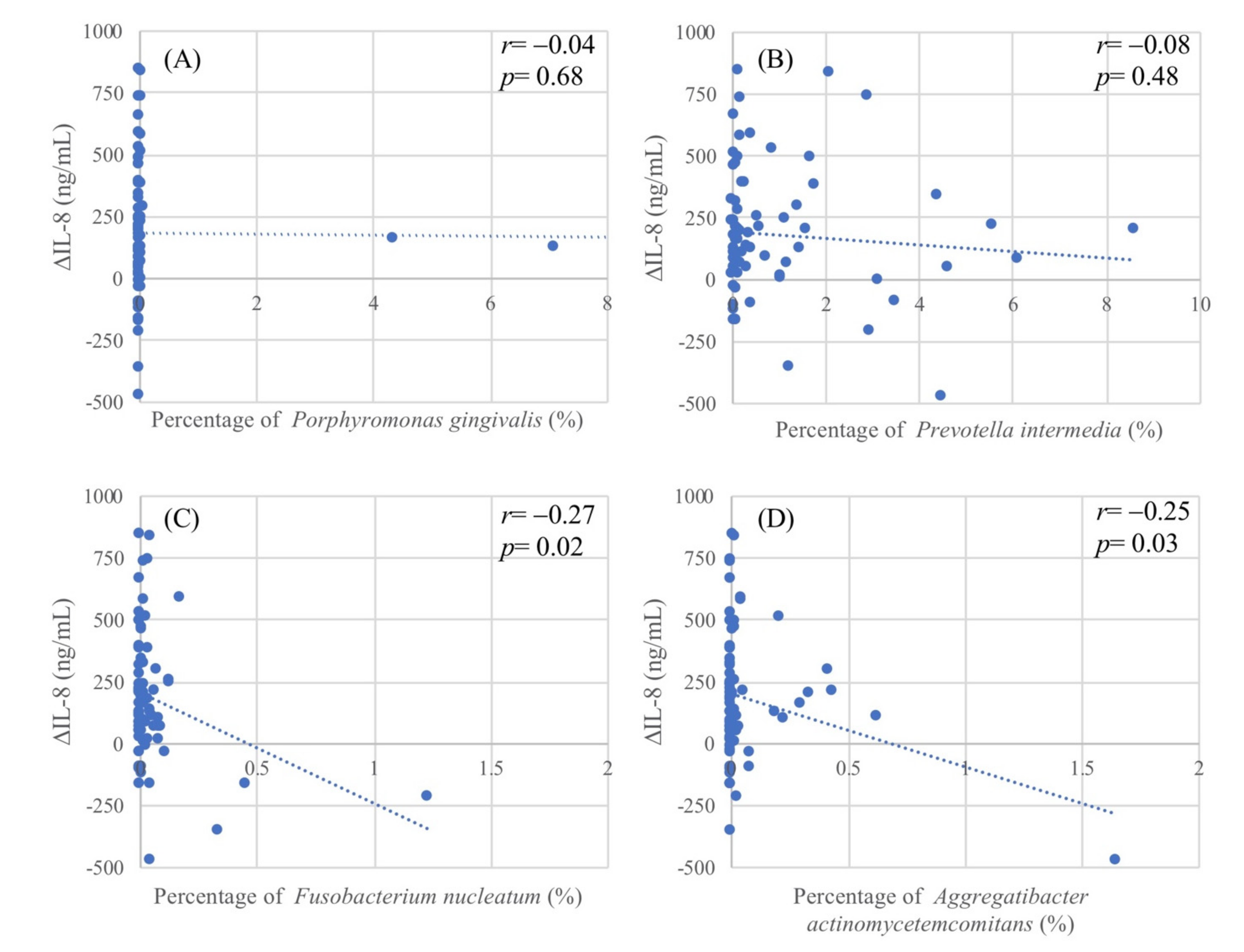
2.2. The Relationship between Oral Microbiota and Salivary Proinflammatory Cytokines
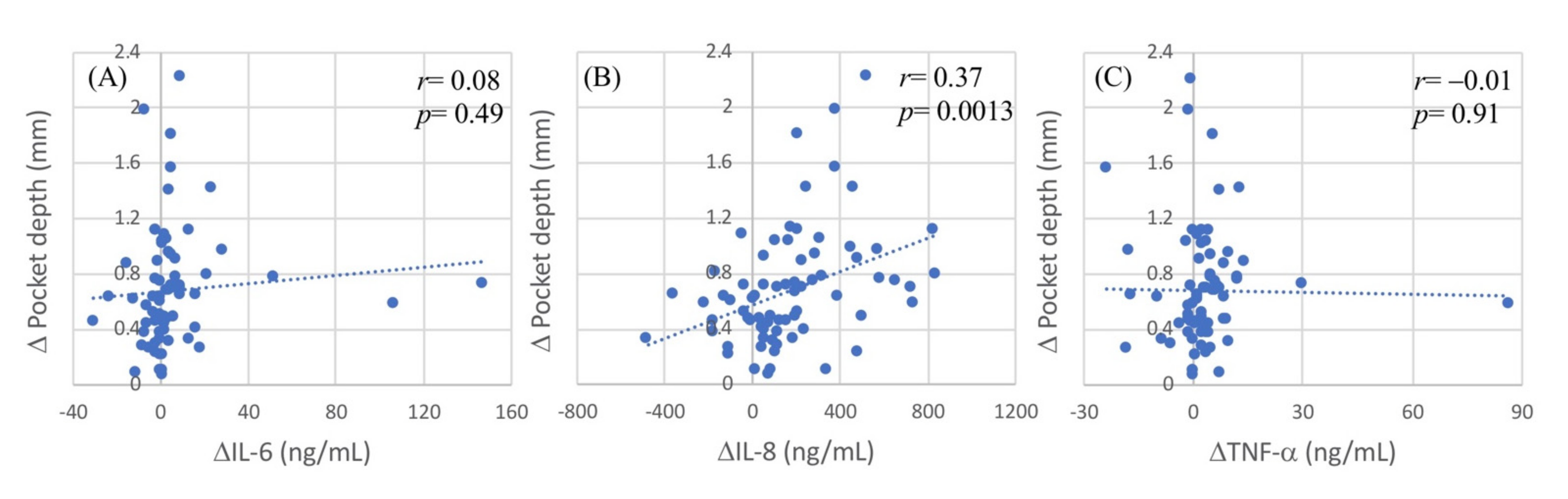
2.3. Contribution of IL-8 to the Treatment Outcome of Periodontal Disease
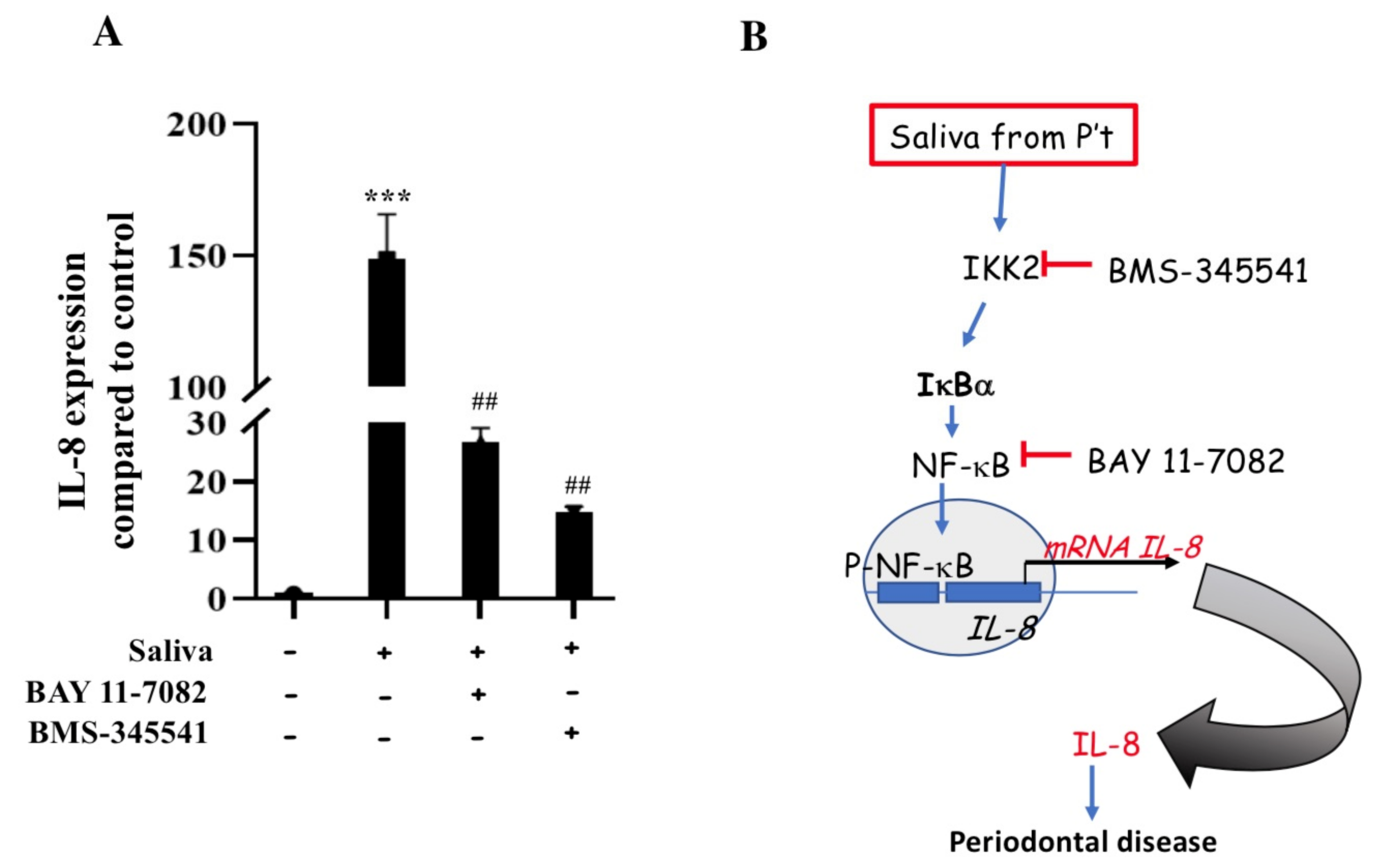
2.4. Saliva-Induced IL-8 Expression in THP-1 Cells
2.5. Induction of IL-8 Expression via the IKK2/IκBα/NF-κB Pathway in THP-1 Cells
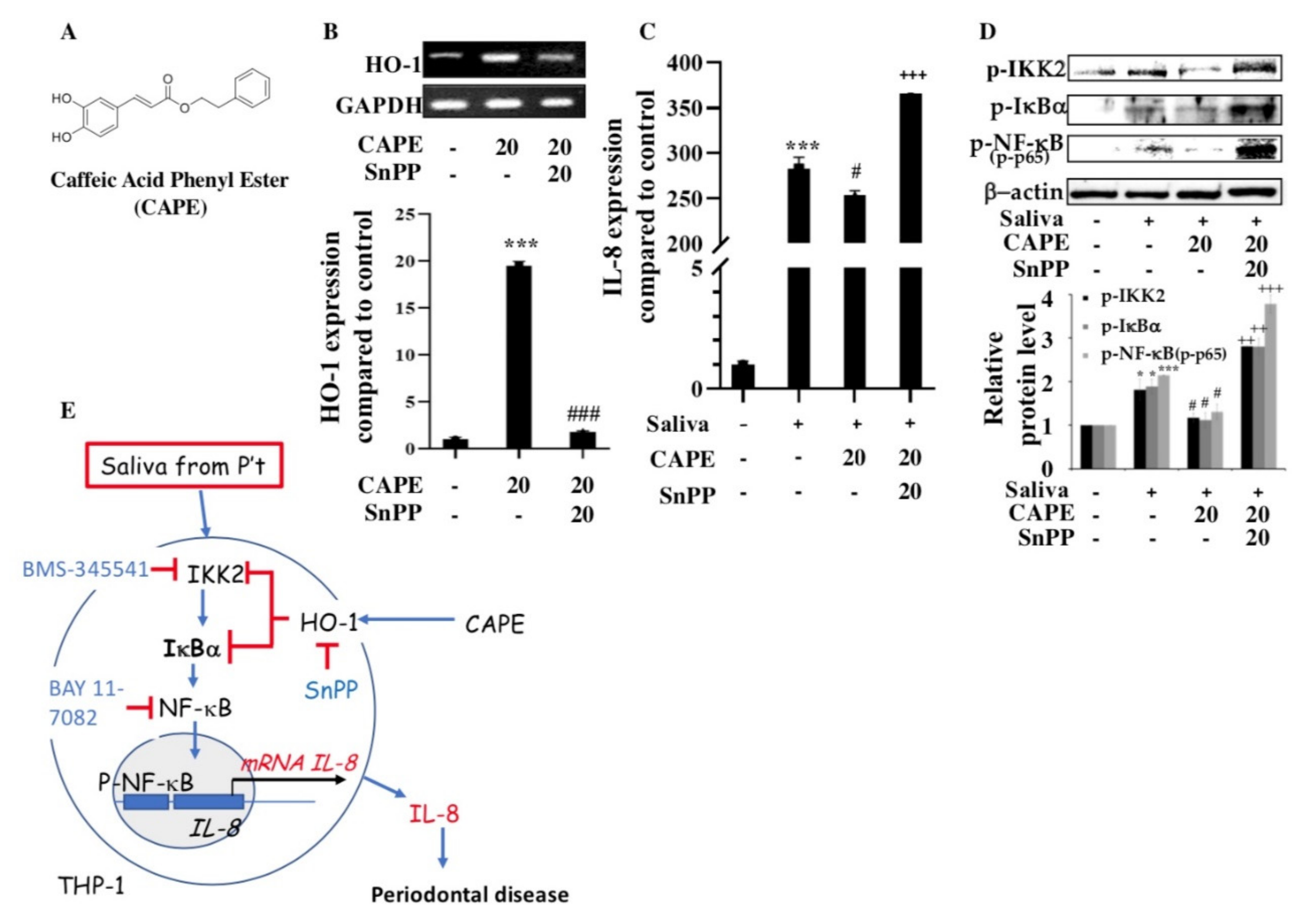
2.6. Induction of Heme Oxygenase-1 (HO-1) and Inhibition of IL-8 Expression by CAPE in THP-1 Cells
3. Discussion
4. Materials and Methods
4.1. Study Participants and Sample Collection
4.2. Cell Line and Treatment
4.3. Subgingival Specimen Collection and Sequencing of the 16S Ribosomal RNA (rRNA) Genes of the Oral Microbiota
4.4. Isolation of RNA and Reverse Transcription–PCR
4.5. Western Blotting
4.6. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Eke, P.I.; Wei, L.; Thornton-Evans, G.O.; Borrell, L.N.; Borgnakke, W.S.; Dye, B.; Genco, R.J. Risk indicators for periodontitis in us adults: Nhanes 2009 to 2012. J. Periodontol. 2016, 87, 1174–1185. [Google Scholar] [CrossRef] [Green Version]
- Petersen, P.E.; Ogawa, H. The global burden of periodontal disease: Towards integration with chronic disease prevention and control. Periodontol. 2000 2012, 60, 15–39. [Google Scholar] [CrossRef]
- Hirschfeld, J.; Higham, J.; Chatzistavrianou, D.; Blair, F.; Richards, A.; Chapple, I.L.C. Systemic disease or periodontal disease? Distinguishing causes of gingival inflammation: A guide for dental practitioners. Part 1: Immune-mediated, autoinflammatory, and hereditary lesions. Br. Dent. J. 2019, 227, 961–966. [Google Scholar] [CrossRef] [PubMed]
- Cekici, A.; Kantarci, A.; Hasturk, H.; Van Dyke, T.E. Inflammatory and immune pathways in the pathogenesis of periodontal disease. Periodontol. 2000 2014, 64, 57–80. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fine, D.H.; Mandel, I.D. Indicators of periodontal disease activity: An evaluation. J. Clin. Periodontol. 1986, 13, 533–546. [Google Scholar] [CrossRef] [PubMed]
- Bonassi, S.; Neri, M.; Puntoni, R. Validation of biomarkers as early predictors of disease. In Mutation Research-Fundamental and Molecular Mechanisms of Mutagenesis; Elsevier: Amsterdam, The Netherlands, 2001; Volume 480, pp. 349–358. [Google Scholar]
- Li, Q.; Verma, I.M. Nf-κb regulation in the immune system. Nat. Rev. Immunol. 2002, 2, 725–734. [Google Scholar] [CrossRef] [PubMed]
- Dahiya, P.; Kamal, R.; Gupta, R.; Bhardwaj, R.; Chaudhary, K.; Kaur, S. Reactive oxygen species in periodontitis. J. Indian Soc. Periodontol. 2013, 17, 411–416. [Google Scholar] [CrossRef]
- Liu, Y.C.; Lerner, U.H.; Teng, Y.T. Cytokine responses against periodontal infection: Protective and destructive roles. Periodontol. 2000 2010, 52, 163–206. [Google Scholar] [CrossRef] [PubMed]
- Kataoka, K.; Ekuni, D.; Tomofuji, T.; Irie, K.; Kunitomo, M.; Uchida, Y.; Fukuhara, D.; Morita, M. Visualization of oxidative stress induced by experimental periodontitis in keap1-dependent oxidative stress detector-luciferase mice. Int. J. Mol. Sci. 2016, 17, 1907. [Google Scholar] [CrossRef] [Green Version]
- Turkseven, S.; Kruger, A.; Mingone, C.J.; Kaminski, P.; Inaba, M.; Rodella, L.F.; Ikehara, S.; Wolin, M.S.; Abraham, N.G. Antioxidant mechanism of heme oxygenase-1 involves an increase in superoxide dismutase and catalase in experimental diabetes. Am. J. Physiol. Heart Circ. Physiol. 2005, 289, H701–H707. [Google Scholar] [CrossRef] [PubMed]
- Rathnayake, N.; Akerman, S.; Klinge, B.; Lundegren, N.; Jansson, H.; Tryselius, Y.; Sorsa, T.; Gustafsson, A. Salivary biomarkers for detection of systemic diseases. PLoS ONE 2013, 8, e61356. [Google Scholar] [CrossRef] [Green Version]
- Mostefaoui, Y.; Bart, C.; Frenette, M.; Rouabhia, M. Candida albicans and streptococcus salivarius modulate il-6, il-8, and tnf-alpha expression and secretion by engineered human oral mucosa cells. Cell Microbiol. 2004, 6, 1085–1096. [Google Scholar] [CrossRef]
- Scheres, N.; Laine, M.L.; de Vries, T.J.; Everts, V.; van Winkelhoff, A.J. Gingival and periodontal ligament fibroblasts differ in their inflammatory response to viable porphyromonas gingivalis. J. Periodontal Res. 2010, 45, 262–270. [Google Scholar] [CrossRef] [PubMed]
- Kato, H.; Taguchi, Y.; Tominaga, K.; Umeda, M.; Tanaka, A. Porphyromonas gingivalis lps inhibits osteoblastic differentiation and promotes pro-inflammatory cytokine production in human periodontal ligament stem cells. Arch. Oral Biol. 2014, 59, 167–175. [Google Scholar] [CrossRef]
- Beiler, T.F.C.S.B.; De Mello Neto, J.M.; Alves, J.C.; Hamlet, S.; Ipe, D.; Da Silva Figueredo, C.M. Impact of non-surgical periodontal treatment on salivary expression of cytokines related to bone metabolism. Odontology 2020, 108, 646–652. [Google Scholar] [CrossRef] [PubMed]
- Anjum, S.I.; Ullah, A.; Khan, K.A.; Attaullah, M.; Khan, H.; Ali, H.; Bashir, M.A.; Tahir, M.; Ansari, M.J.; Ghramh, H.A.; et al. Composition and functional properties of propolis (bee glue): A review. Saudi J. Biol. Sci. 2019, 26, 1695–1703. [Google Scholar] [CrossRef] [PubMed]
- Wagh, V.D. Propolis: A wonder bees product and its pharmacological potentials. Adv. Pharmacol. Sci. 2013, 2013, 308249. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kocot, J.; Kielczykowska, M.; Luchowska-Kocot, D.; Kurzepa, J.; Musik, I. Antioxidant potential of propolis, bee pollen, and royal jelly: Possible medical application. Oxid. Med. Cell. Longev. 2018, 2018, 7074209. [Google Scholar] [CrossRef]
- Abbasi, A.J.; Mohammadi, F.; Bayat, M.; Gema, S.M.; Ghadirian, H.; Seifi, H.; Bayat, H.; Bahrami, N. Applications of propolis in dentistry: A review. Ethiop. J. Health Sci. 2018, 28, 505–512. [Google Scholar]
- Oeckinghaus, A.; Ghosh, S. The nf-κb family of transcription factors and its regulation. Cold Spring Harb. Perspect. Biol. 2009, 1, a000034. [Google Scholar] [CrossRef] [PubMed]
- Nazir, M.A. Prevalence of periodontal disease, its association with systemic diseases and prevention. Int. J. Health Sci. 2017, 11, 72–80. [Google Scholar]
- Kornman, K.S.; Page, R.C.; Tonetti, M.S. The host response to the microbial challenge in periodontitis: Assembling the players. Periodontol. 2000 1997, 14, 33–53. [Google Scholar] [CrossRef] [PubMed]
- Milward, M.R.; Chapple, I.L.C.; Wright, H.J.; Millard, J.L.; Matthews, J.B.; Cooper, P.R. Differential activation of nf-κb and gene expression in oral epithelial cells by periodontal pathogens. Clin. Exp. Immunol. 2007, 148, 307–324. [Google Scholar] [CrossRef]
- Borilova Linhartova, P.; Kavrikova, D.; Tomandlova, M.; Poskerova, H.; Rehka, V.; Dušek, L.; Izakovicova Holla, L. Differences in interleukin-8 plasma levels between diabetic patients and healthy individuals independently on their periodontal status. Int. J. Mol. Sci. 2018, 19, 3214. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kantarci, A.; Hasturk, H.; Dyke, T.E. Host-mediated resolution of inflammation in periodontal diseases. Periodontol. 2000 2006, 40, 144–163. [Google Scholar] [CrossRef] [PubMed]
- Finoti, L.S.; Nepomuceno, R.; Pigossi, S.C.; Corbi, S.C.; Secolin, R.; Scarel-Caminaga, R.M. Association between interleukin-8 levels and chronic periodontal disease: A prisma-compliant systematic review and meta-analysis. Medicine 2017, 96, e6932. [Google Scholar] [CrossRef] [PubMed]
- Lundqvist, C.; Hammarstrom, M.L. T-cell receptor gamma delta-expressing intraepithelial lymphocytes are present in normal and chronically inflamed human gingiva. Immunology 1993, 79, 38–45. [Google Scholar] [PubMed]
- Gemmell, E.; Seymour, G.J. Gamma delta t lymphocytes in human periodontal disease tissue. J. Periodontol. 1995, 66, 780–785. [Google Scholar] [CrossRef]
- Noh, M.K.; Jung, M.; Kim, S.H.; Lee, S.R.; Park, K.H.; Kim, D.H.; Kim, H.H.; Park, Y.G. Assessment of il-6, il-8 and tnf-alpha levels in the gingival tissue of patients with periodontitis. Exp. Ther. Med. 2013, 6, 847–851. [Google Scholar] [CrossRef] [Green Version]
- Otero, J.E.; Chen, T.; Zhang, K.H.; Abu-Amer, Y. Constitutively active canonical nf-κb pathway induces severe bone loss in mice. PLoS ONE 2012, 7, e38694. [Google Scholar] [CrossRef] [Green Version]
- Park, M.H.; Hong, J.T. Roles of nf-κb in cancer and inflammatory diseases and their therapeutic approaches. Cells 2016, 5, 15. [Google Scholar] [CrossRef]
- Ruocco, M.G.; Maeda, S.; Park, J.M.; Lawrence, T.; Hsu, L.C.; Cao, Y.; Schett, G.; Wagner, E.F.; Karin, M. Iκb kinase (ikk)β, but not ikkα, is a critical mediator of osteoclast survival and is required for inflammation-induced bone loss. J. Exp. Med. 2005, 201, 1677–1687. [Google Scholar] [CrossRef] [Green Version]
- Jimi, E.; Aoki, K.; Saito, H.; D’Acquisto, F.; May, M.J.; Nakamura, I.; Sudo, T.; Kojima, T.; Okamoto, F.; Fukushima, H.; et al. Selective inhibition of nf-κb blocks osteoclastogenesis and prevents inflammatory bone destruction in vivo. Nat. Med. 2004, 10, 617–624. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Sun, W.; Wu, T.; Lu, R.; Shi, B. Caffeic acid phenethyl ester attenuates lipopolysaccharide-stimulated proinflammatory responses in human gingival fibroblasts via nf-κb and pi3k/akt signaling pathway. Eur. J. Pharmacol. 2017, 794, 61–68. [Google Scholar] [CrossRef] [PubMed]
- El-Sharkawy, H.M.; Anees, M.M.; Van Dyke, T.E. Propolis improves periodontal status and glycemic control in patients with type 2 diabetes mellitus and chronic periodontitis: A randomized clinical trial. J. Periodontol. 2016, 87, 1418–1426. [Google Scholar] [CrossRef] [PubMed]
- Ruocco, M.G.; Karin, M. Ikkβ as a target for treatment of inflammation induced bone loss. Ann. Rheum. Dis. 2005, 64 (Suppl. S4), iv81–iv85. [Google Scholar]
- Murakami, Y.; Kawata, A.; Suzuki, S.; Fujisawa, S. Radical-scavenging and pro-/anti-inflammatory activity of tetracycline and related phenolic compounds with or without visible light irradiation. In Vivo 2020, 34, 81–94. [Google Scholar] [CrossRef]
- Choe, S.H.; Choi, E.Y.; Hyeon, J.Y.; Choi, I.S.; Kim, S.J. Effect of nitric oxide-releasing derivative of indomethacin on prevotella intermedia lipopolysaccharide-induced production of proinflammatory mediators in murine macrophages. Biochem. Biophys. Res. Commun. 2017, 492, 224–230. [Google Scholar] [CrossRef] [PubMed]
- Chan, C.L.; You, H.J.; Lian, H.J.; Huang, C.H. Patients receiving comprehensive periodontal treatment have better clinical outcomes than patients receiving conventional periodontal treatment. J. Formos. Med. Assoc. 2016, 115, 152–162. [Google Scholar] [CrossRef] [Green Version]
- Chang, C.H.; Han, M.L.; Teng, N.C.; Lee, C.Y.; Huang, W.T.; Lin, C.T.; Huang, Y.K. Cigarette smoking aggravates the activity of periodontal disease by disrupting redox homeostasis- an observational study. Sci. Rep. 2018, 8, 11055. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | PI (%) | BOP (%) | PPD (Mean; mm) |
|---|---|---|---|
| Salivary proinflammatory cytokines | |||
| Interleukin-6 | 0.08 | 0.08 | 0.13 |
| Interleukin-8 | −0.14 | 0.45 *** | 0.49 *** |
| Tumor necrosis factor-α | −0.05 | 0.00 | 0.04 |
| Selected oral microbiota species | |||
| Porphyromonas gingivalis | −0.14 | −0.11 | −0.03 |
| Prevotella intermedia | −0.20 | −0.05 | −0.06 |
| Fusobacterium nucleatum | −0.04 | −0.13 | −0.08 |
| Aggregatibacter actinomycetemcomitans | −0.03 | −0.02 | −0.10 |
| Selected Oral Microbiota Species | ∆PI (%) | ∆BOP (%) | ∆PPD (Mean; mm) |
|---|---|---|---|
| Porphyromonas gingivalis | 0.01 (0.94) | −0.07 (0.55) | −0.001 (0.98) |
| Prevotella intermedia | 0.09 (0.44) | −0.19 (0.11) | −0.07 (0.57) |
| Fusobacterium nucleatum subsp. nucleatum | 0.08 (0.53) | −0.04 (0.72) | −0.02 (0.86) |
| Aggregatibacter actinomycetemcomitans | 0.05 (0.69) | −0.03 (0.80) | −0.07 (0.51) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huang, Y.-K.; Tseng, K.-F.; Tsai, P.-H.; Wang, J.-S.; Lee, C.-Y.; Shen, M.-Y. IL-8 as a Potential Therapeutic Target for Periodontitis and Its Inhibition by Caffeic Acid Phenethyl Ester In Vitro. Int. J. Mol. Sci. 2021, 22, 3641. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms22073641
Huang Y-K, Tseng K-F, Tsai P-H, Wang J-S, Lee C-Y, Shen M-Y. IL-8 as a Potential Therapeutic Target for Periodontitis and Its Inhibition by Caffeic Acid Phenethyl Ester In Vitro. International Journal of Molecular Sciences. 2021; 22(7):3641. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms22073641
Chicago/Turabian StyleHuang, Yung-Kai, Kuo-Feng Tseng, Ping-Hsuan Tsai, Jie-Sian Wang, Chang-Yu Lee, and Ming-Yi Shen. 2021. "IL-8 as a Potential Therapeutic Target for Periodontitis and Its Inhibition by Caffeic Acid Phenethyl Ester In Vitro" International Journal of Molecular Sciences 22, no. 7: 3641. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms22073641